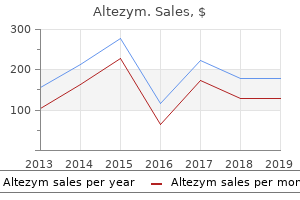
Altezym
Elias I. Traboulsi, M.D. - Cleveland Clinic Foundation
- Division of Ophthalmology
- Cleveland, Ohio
Best altezym 500 mgThe spinal twine lesion tends to be more in depth in rostral-caudal dimension than the standard vascular or demyelinative myelopathy amical 48 antimicrobial discount 100mg altezym visa. These are important points to establish antibiotics for acne weight gain order altezym 250mg with amex, as a end result of a mistaken diagnosis of intraspinal tumor or of a dural arteriovenous fistula may lead to antibiotic cream for dogs cheap altezym 250mg without a prescription an pointless operation or further irradiation antimicrobial vinegar altezym 250mg low price. Varying degrees of secondary degeneration are seen within the ascending and descending tracts. Vascular changes-necrosis of arterioles or hya line thickening of their walls and thrombotic occlusion of their lumens-are prominent in probably the most severely broken parts of the twine. Most neuropathologist& have attributed the parenchymal lesion to the blood ves sel modifications; others believe that the degree of vascular change is inadequate to clarify the necrosis (Malamud et al; Burns et al). Exceptional cases, in which a transverse myelopathy has developed within a number of hours of radiation therapy (as described by Reagan et al), are more readily explained by thrombotic occlusion of a large spinal artery. Neurologists related to cancer treatment cen ters are generally confronted with a affected person who exhib its the late growth (up to 10 to 15 years after radia tion) of a slowly progressive sensorimotor paralysis of just one limb (motor weak spot predominates) or one region of the physique. Treatment and Prevention Kagan and colleagues have determined the tolerance of the grownup human spinal wire to radiation, considering the amount of this sue irradiated, the length of the irradiation, and the total dose. It is noteworthy that in the cases reported by Sanyal and associates, the amount of radiation surpassed these limits. Forewarned with this data, radiation specialists have the impression that the incidence of this complication is reducing. Of course, if the underlying neoplasm is likely to be immi nently deadly, palliative radiation can exceed these limits. A variety of case stories remark on temporary enchancment in neurologic perform after the adminis tration of corticosteroids. This remedy ought to be tried because in some sufferers it seems to arrest the process short of complete destruction of all sensory and motor tracts. About one-third of the deadly accidents result from contact with household currents. The issue that governs the damage to the nervous system is the quantity of current, or amperage, with which the sufferer has contact, not simply the voltage, as is mostly believed. In any particular case, the period of contact with the present and the resistance offered by the skin to present (greatly decreased if the pores and skin is moist or a body part is immersed in water) are of importance. The physics of electrical accidents is rather more complex than these transient remarks indicate (for a full discussion, see the evaluations by Panse and by Winkelman). Any part of the peripheral or central nervous system could additionally be injured by electrical currents and lightning. The effects may be quick, which is understandable, however of larger curiosity are the cases of neurologic harm that occur after a delay of 1 day to 6 weeks (1 week on average) and a rarer syndrome of anterior hom cell dam age that arises after a few years. They have been attributed to vascular occlusive adjustments induced by the electric current, a mechanism proposed to underlie the same delayed effects of radia tion remedy (see earlier). However, the latent period is measured in lots of months or a few years quite than in days and the course is extra usually progressive than self-limited. Moreover, the few postmortem studies of myelopathy as a consequence of electrical damage have disclosed a widespread demyelination of lengthy tracts, to the point of tissue necrosis in some segments, and relative sparing of the grey matter, however no abnormalities of the blood vessels. The extraordinary syndrome of focal muscular atro phy occurring with a delay of weeks to years after an electric shock has been described by Panse beneath the title spinal atrophic paralysis. It happens when the path of the cur hire, often of low voltage, is from arm to arm (across the cervical cord) or from an arm to leg. When the head is one of the contact factors, the patient turns into uncon scious or suffers tinnitus, deafness, or headache for a brief period following the injury. Pain and paresthesias occur instantly within the concerned limb but these signs are transient. Mild weak spot, also unilateral, is immediate, followed in a number of weeks or months by muscle losing, most frequently taking the form of segmental muscular atrophy. A more severe and everlasting harm has been caused by inadver tent injection of anesthetic instantly into the conus medullaris (see Hamandi et al; W ilkinson et al). The patient reports leg weak spot and numbness on one facet instantly with the injection or upon awakening if sedation has been used. Although this complication is rare, it has occurred even when skilled anesthesiologists perform the procedure; misidentification of the L3-L4 spi nal interspace has been cited as the issue. Flat-tipped needles are as prone to cause harm to the conus as are ones with sharp beveled ideas. Arachnoiditis from irrita tive agents, not used to any nice extent, up to now triggered a myelopathy (see Chap. Direct strikes are often deadly; nearby strikes produce neurologic injury as described below. Topographic prominences similar to timber, hills, and towers are struck preferentially, so these should be avoided; a person caught in the open ought to curl up on the bottom, mendacity on one side with legs close together. Arborescent pink traces or burns on the pores and skin indicate the point of contact of the vitality generated by direct or close by lightning. The path via the physique can be roughly deduced from the scientific sequelae. Death is a results of ventricular fibrillation or of the consequences of intense desiccating warmth on the mind. Lightning that strikes the pinnacle is especially harmful, proving deadly in 30 p.c of cases. Rarely, unconscious ness or an agitated-confusional state might persist for per week or two. There is often a disturbance of sensorimotor func tion of a limb or all of the limbs, which may be pale and chilly or cyanotic. As a rule, these signs are additionally evanescent, but in some instances they persist, or an atrophic paralysis of a limb or part of a limb makes its look after a symptom-free interval of several months as within the case of electrical injury. There are additionally a few instances on report of recovery from generalized polyneuropathy after lightning harm, but our expertise with one case was of profound generalized axonal dam age with little restoration (see Chap. Gradually, knowledge of neuropathology superior, and one illness after one other was faraway from this class till solely the verifiably inflammatory ones remained. The spinal wire is known to be the locus of a limited number of infective and noninfective inflammatory pro cesses, some causing selective destruction of neurons, others affecting primarily white matter (tracts), and yet one more group involving the meninges and white mat ter or leading to a necrosis of both grey and white mat ter. Other special terms, qualifying myelitis, are used to indicate extra exactly the distribution of the process: if confined to gray matter, the correct expression is poliomy elitis; if to white matter, leukomyelitis. If approximately the entire cross-sectional space of the twine is involved at one or more levels, the method is claimed to be a transverse myeli this (although the time period is still used more broadly for so much of myelitides); if the lesions are a number of and widespread over a long vertical extent, the modifying adjectives d if fuse or disseminated are used and recently longitudinally intensive myelopathy has been introduced to denote a bined infl ammation of meninges and spinal cord and generally with explicit circulating autoantibodies (see Chap, 36). A transient and sometimes uneven paraparesis is understood epidural or subdural spinal abscess granuloma, as the case may be. The adjectives acute, subacute, and continual denote the tempo of evolution of myelitic symptoms-namely, extra or tively. Myelitis secondary to bacterial, fungal, parasitic, and first granulomatous ailments of the menin ges and spinal twine (Chap. Parasitic and fungal infections producing epidural granuloma, localized meningitis, or meningomyelitis and abscess, especially certain forms of schistosomiasis (Chap.
Purchase 100 mg altezym with amexThere is little proof that such circumstances characterize a reactivation of a virus or the presence of another infectious agent antibiotics for uti cause yeast infection discount altezym 500mg otc. This declare has been confirmed in a number of followup stud ies bacterial infection symptoms generic altezym 250 mg line, though again the profit has been marginal infection 6 weeks after c-section buy altezym 250 mg low cost. Guanidine hydrochloride and injections of cobra venom antibiotic cement spacer generic altezym 500mg, gangliosides, interferons, high-dose intravenous cyclophosphamide, and thyro tropin-releasing hormone are however a few of an extended list of agents that were said to arrest the disease course of, however these claims have been discredited. An attempt could be made to reduce the spasticity with drugs, corresponding to baclofen or tizanidine, or by subarach noid infusions of baclofen via an implanted lumbar pump. Initial intrathecal check doses are given to predict a response to the pump infusions of baclofen, but this take a look at may fail; consequently, in extreme instances it could be advisable to pro ceed with a constant infusion for a quantity of days. Some diploma of improved comfort from a reduction in the excessive rigid ity is usually essentially the most that can be anticipated. Partial reduction from spasticity may be afforded by method of benzo diazepines or sometimes dantrolene. These approaches are best suited for instances of primary lateral sclerosis, which may be expected to progress slowly and for a long interval. Physical remedy is invaluable, for instance, for avoiding con tractures of the fingers and shoulders. We sometimes carry out pulmonary perform tests every few months after the first yr or so of illness. Our experience has been that the very important capability in cubic centimeters can be estimated by multiply ing the highest number to which a patient can count with one deep breath by 100. Thus, the flexibility to count to 25 with a full effort in a single breath corresponds to a vital capability of approximately 2. Almost always, a sea soned pulmonary technologist can find solutions to these issues. With noninvasive respiratory help, it might be potential to defer trache ostomy for months or years. We broach this subject early sufficient in the midst of the illness to permit ample time for discussion and reflection. In follow, most sufferers elect to not endure tracheostomy and full air flow. As oro pharyngeal palsy progresses, food should be minimize into small items and dry meals, such as toast ought to be prevented; milk shakes and preparations of the same consis tency are perfect at this stage. Speech therapists are capable of instructing sufferers methods to adapt to declining bulbar function and on the similar time minimizing aspiration. Although we adopt a neutral position in discus sions with sufferers relating to mechanical air flow, we are likely to urge sufferers to undergo placement of a feeding tube at the acceptable time. This presumably increases survival and improves quality of life by stopping dehydration and recurrent aspiration. Laparoscopic and radiologic technologies for the location of a gastrostomy tube render the procedure swift and almost painless. Some patients have tubes inserted as outpatients after which start gastric feeding within a day or two. Other gadgets, often guided by the bodily and occupational therapist, may be of great assistance to the affected person and family because the illness progresses. These include a mechanized mattress and structural accommoda tions in the home that facilitate entry of a wheelchair and the secure use of the bath or bathe as nicely as thick-handled utensils. Ambulation aids, beginning with simple canes (first one, then two) followed by a walker (preferably with basket and seat) and then a wheelchair (manual or elec tric) are of worth in sustaining a sense of independence and assuring safety. They are presented right here as a end result of they fall throughout the class of system degenerations and are usu ally inherited. Further clinical analyses, nevertheless, indicated the inadequacy of this slim grouping for the massive group of spinal muscular atrophies. Brandt, in his examine of 112 Danish sufferers, discovered that in about one-third the weak spot was present at delivery, and in ninety seven the onset was within the first yr of life; in 9 patients, the disease was not recognized till after the primary year of life. In 1956, Walton, and later Wohlfart and colleagues and Kugelberg and Welander (see below), recognized milder forms of spinal muscular atrophy in which the onset was between 2 and 1 7 years and strolling was nonetheless attainable in grownup life. Byers and Banker, in a study of fifty two sufferers, subdivided them into three groups on the idea of age of onset; in a single group the illness was acknowledged at birth or in the first month or two of life; in a second, between 6 and 12 months; and in a third, after the first yr. In their last group, it was common for the affected person to survive into adolescence and grownup life. More recently, the designations Characteristically the toddler, often born normally, is famous from birth to be unnaturally weak and limp ("floppy"). Some mothers report that fetal movement in utero had been less than anticipated or lacking altogether. In severe cases, arthrogryposis on the ankles and wrists or dislocation of the hips is famous at delivery (arthrogryposis and its differential prognosis is discussed in Chap. The muscle weakness in these kids is generalized from the beginning, and dying comes early, normally throughout the first 12 months. Other infants appear to develop usually for several months earlier than the weak point becomes obvious. In these, the and shoulder-girdle muscular tissues are at first disproportionately affected, while the fingers and palms, toes and ft, and cranial muscle tissue retain mobility. Volume of muscle is diminished but is tough to consider within the toddler because of the coverings of adipose tissue. Perception of tactile and painful stimuli is undiminished, and emotional and social development measures up to age. As the months cross, the weak spot and hypotonia progress steadily and spread to all of the skeletal muscles besides the ocular ones. Respiratory transfer ments turn into paradoxical (abdominal protrusion with chest retraction). Their posture is attribute: position" with exterior rotation and abduction at hips and flexion at hips and knees. If the effects of gravity are arms kidnapped and flexed on the elbow, legs in the "frog the age of onset (see Table 39-7). Familial spinal muscular atrophy that begins in infancy and child hood is inherited mainly as an autosomal recessive trait. Until late within the sickness, these chil dren seem bright-eyed, alert, and responsive. Infants in whom the disease becomes apparent solely after a quantity of months of life have a less-rapid decline than these affected in utero or at delivery. Some of the former turn out to be able to sit and creep and even to stroll with sup port; those with later onset could survive for a number of years and even into adolescence or early grownup life, as already talked about. Motor unit poten tials are diminished in quantity and, within the more slowly evolving cases, some are larger than regular (giant or polyphasic potentials reflecting reinnervation). Motor nerve conduction velocities are regular or fall in the low normal vary (these are normally slower in infants than in adults). Electrophysiologic studies performed within the first few months of life may give ambiguous outcomes. Although affected siblings demonstrate very related clinical patterns of illness, the identical mutation could give rise to very different phenotypes in different households, in order that further modifying posttranscriptional or nonge netic attributes have to be enjoying a job.
Discount altezym 100mg lineExcessive sweating of the soles and dorsal elements of the feet and of the volar surfaces of the hands and fingers is a typical manifestation of alcohol-induced dietary neuropathy bacteria 400x magnification cheap 100 mg altezym with visa. Postural hypotension is typically associ ated bacteria definition 250 mg altezym overnight delivery, all symptoms indicative of involvement of the peripheral sympathetic nerve fibers antibiotic resistance lesson plan generic altezym 500 mg free shipping. Sensory loss or impairment might involve all of the modalities antimicrobial activity of plant extract altezym 250 mg amex, though one may be affected out of propor tion to the others, normally pain and temperature. The mildest neuro pathic indicators are thinness and tenderness of the leg mus numerous. In reality, many sufferers are asymptomatic and evi cles, loss or despair of the Achilles reflexes and maybe of the patellar reflexes and at times, a patchy blunting of pain and touch sensation over the toes and shins. Most patients, nevertheless, are symptomatic and have weak point, paresthesias, and ache as the standard complaints. The symptoms are insidious in onset and slowly progres sive, but often they appear to evolve or to worsen rapidly over a matter of days. The preliminary symptoms are often referred to the distal portions of the limbs and progress proximally In patients with impairment of superficial sensation. Pain and dysesthesias may be outstanding in patients with either severe or slight degrees of motor, reflex, and sensory loss. Usually some aspect of motor incapacity is part of the chief grievance, but in about one-third of the patients the principle complaints are pain and paresthe sias. The discomfort takes several types: a dull, constant ache in the toes or legs; sharp and lancinating pains, momentary in length, like these of tabes dor salis; sensations of cramping or tightness in the muscle tissue of the toes and calves; or band-like emotions around the legs. Once the stimulus is perceived, however, it has a painful and diffuse, unpleasant high quality (hyperpathia). The most pronounced adjustments are noticed within the distal parts of the longest and largest myelinated fibers within the crural and, to a lesser extent, brachial nerves. In the most advanced situations of neuropathy, hoarseness and weak spot of the voice and dysphagia because of degeneration of the vagus nerves could also be added to the scientific image. The vagus and phremc nerves and paravertebral sympathetic trunks could also be affected in superior cases. Anterior hom and dorsal root ganglion cells undergo chromatolysis, indicating axonal injury. In the remaining patients, the motor-reflex-sensory indicators occurred in various combinations. Stasis edema and pigmentation, glossiness, and skinny ness of the pores and skin of the decrease legs and toes are common findings in sufferers with any severe type of neopathy. Repeated trauma to insensitive elements and super imposed an infection are thought to be answerable for the neuropathic arthropathy, as mentioned in Chaps. Nevertheless, a quantity of research in birds and humans do indeed point out that uncomplicated thiamine deficiency could lead to peripheral nerve disease. Findings of nerve conduction studies include mild to average degrees of slowing of motor and sensory conduction and a marked discount in the amplitudes of sensory action potentials; the motor conduction velocies in distal segments of the nerves may be reduced, whereas conduction in proximal segments is normal. The data introduced extra lately by Koike and colleagues, ostensibly in favor of the existence of a real alcoholic neuropathy, in our view current no con vincing assist of a direct toxic impact of alcohol. If persistent vomiting or different gastrointestinal compl ca tions stop the affected person from consuming, parenteral feeding turns into necessary; the nutritional vitamins may be given intramus cularly or added to intravenous fluids. Aching of the limbs may be associated to their immobility, during which case they should be moved passively on frequent occa sions. Aspirin or acetaminophen is usually sufficient to control hyperpathia and allodynia; often codeine or methadone must be added. Some of our sufferers with severe burning ache (similar to causalgia) within the ft had prior to now been helped briefly by blocking the lumbar sympathetic ganglia or by epidural injection of analgesics. Adrenergic-blocking medicine has been of little value and mexiletine, in our expertise, of unsure profit. The regeneration of peripheral nerves, which may take many months, might be of little avail if the muscle tissue have been allowed to bear contracture and the joints to turn into fastened. In instances of severe paralysis, molded splints ought to be applied to the arms, arms, legs, and toes in periods of relaxation. Pressure on the heels and elbows can be avoided by padding the splints and by turning the affected person frequently or by asking the affected person to accomplish that. In the mildest cases there may be a considerable restoration of motor function in a quantity of weeks. In severe forms of the disease, many months might pass earlier than the patient is in a position to stroll unaided. The sensory features and ache particularly may be slower to recuperate, having taken over a 12 months in considered one of our recently noticed patients. The slowness of restoration creates a special downside for the alcoholic patient, in whom the great hazard to continued recovery is the resumption of consuming and inadequate food plan. Serum creatine phosphate was regular in these individuals, however carnitine was reduced. The oral administration of 200 mg of riboflavin and 4 g of carnitine per day relieved the signs. Since 1940, it has diminished greatly because of the overall follow of enriching bread with niacin. Nevertheless, among the vegetarian, maize eating folks of underdeveloped international locations, and among the black population of South Africa, pellagra continues to be a typical illness (Bomb et al; Shah et al; Ronthal and Adler). In developed nations, pellagra is virtually confined to alcoholics (Ishii and Nishihara; Spivak and Jackson; Serdaru et al). In the past, there have been claims that glossitis, cheilosis, and neuropathy were attributable to riboflavin deficiency, however its results were by no means isolated. It is a component of general malnutrition, mak ing it troublesome to separate the cause of numerous problems. Antozzi and coworkers reported that a metabolic dysfunction just like the Reye syndrome can be caused by riboflavin deficiency and is correctable by administration of riboflavin alone. The affected infants of their research have been hypoglycemic, hypotonic, and episodically weak and unresponsive. Generally, 15 mg per day in divided doses is used for alternative, but restoration of a normal food regimen is paramount. Antozzi and colleagues also recorded instances of disease in older kids and adults, manifesting as a kind of lipid storage polymyopathy as a end result of either In its fully developed form, pellagra affects the pores and skin, alimentary tract, and hematopoietic and nervous sys tems. Pellagra might not solely produce mental impairment but occasionally end result from it, by virtue of anorexia and refusal of food. The dermatologic characteristic, often the facet that permits one to make a assured prognosis, is a scaly dermatitis in sun-exposed areas, adopted by hyperpig mentation of these areas. Diarrhea and glossitis or different forms of mucous membrane disorder may be accompani ments (hence the alliterative triad dementia-dermatitis diarrhea; the "3 Ds"). Signs of peripheral neuropathy are relatively much less widespread and are indistinguishable from these of neuropathic beriberi. However, in the pathologic material offered by Hauw and associates, these chro matolytic adjustments had been most pronounced within the brainstem nuclei (upper reticular and pontine) and not in the Betz cells.
Discount 250mg altezym mastercardCiliary physique paralysis with loss of accommodation and blurring of imaginative and prescient but with preserved gentle reaction often appears within the second or third week (the opposite of the Argyll Robertson reaction) treatment for dogs broken toe buy generic altezym 500mg. The cranial nerve indicators might clear with out additional involvement of the nervous system antibiotics keflex discount altezym 250mg, or a delayed sensorimotor polyneuropathy may develop between the fifth and eighth weeks of the disease virus updates purchase altezym 500mg line. At the outset antibiotic 2 hours late order altezym 500mg mastercard, a single dose of antitoxin (3,000 to 6,000 U of tetanus immune human globulin) must be given together with a 10-day course of penicillin (1. Immediate surgical remedy of the wound (excision or debridement) is imperative, and the tissue around the wound should be infiltrated with antitoxin. Survival is decided by expert and fixed nursing in an intensive care unit and may be essential for weeks. The benzodiazepines are probably the most helpful medication for both sedation and muscle relaxation; diazepam one hundred twenty mg / d or more could be given in frequent divided doses if ventilatory support is on the market; alternatively midazolam or propofol can be utilized in a steady intravenous infusion. Short-acting barbiturates and chlorpromazine may be helpful, as could additionally be morphine. The early oropharyngeal signs, the ciliary paralysis with relatively retained pupillary response to light, and subacute evolution of a delayed symmetrical sensorimotor peripheral neuropathy distinguish diphtheria from other types of polyneuropathy. The long latency between the preliminary infection and the involvement of the nervous system has no clear explanation. In experimental animals, Waksman and colleagues demonstrated that the toxin reaches the Schwann cells in essentially the most vascular parts of the peripheral nervous system inside 24 to forty eight h of an infection but its metabolic effect on cell membranes extends over a interval of weeks. The toxin produces demyelination within the proximal parts of spinal nerves, in dorsal root ganglia, and in spinal roots. The cardiac musculature and the conducting system of the center undergo mild focal necrosis. The supply of diphtheritic an infection could also be extrafaucial-a penetrating wound, pores and skin ulcer, or infection of the umbilicus in the neonate. The systemic and neurologic complications of faucial diphtheria may also be observed within the extrafaucial form of the illness (wound infection) after an analogous latent period. It is probable, subsequently, that the toxin reaches neural websites by way of the bloodstream; but in addition, some action is exerted locally, as evidenced by palatal paralysis in faucial cases and by initial weak point and sensory impairment within the neighborhood of the infected wound. It is generally agreed that the administration of antitoxin within forty eight h of the earliest symptoms of the first diphtheritic an infection lessens the incidence and severity of the peripheral nerve complications. Botu lism Botulism is a rare type of food-borne illness caused by the exotoxin of Clostridium botulinu m. Outbreaks of poisoning are most often brought on by ingested bacte ria contained in home-preserved than in commercially canned merchandise, and vegetables and home-cured ham are incriminated extra commonly than are different food products. Although the illness is ubiquitous, five western states (California, Washington, Colorado, New Mexico, and Oregon) account for more than half of all reported outbreaks in the United States. These are a results of absorption of the toxin formed by germination of ingested spores (rather than ingestion of preformed toxin), an necessary source of which is con taminated natural (raw) honey. It is now well established on the idea of observations in each animals and people that the first website of motion of toxin is at a neuromuscular junction, more particularly on the presynaptic membrane. The toxin interferes with the release of acetylcholine from peripheral motor nerves on the neuromuscular synapse. The physiologic defect is just like the one that characterizes the myasthenic syndrome of Lambert-Eaton (see Chap. As a rule, blurred vision and diplopia are the initial neural symptoms; their affiliation with ptosis, strabismus, and extraocular muscle palsies, notably of the sixth nerve, could at first suggest a prognosis of myasthenia gravis. In botulism, nonetheless, accommodation is misplaced and the pupils are often unreactive to light. Other signs of bulbar involvement-nasality of voice, hoarseness, dysarthria, dysphagia, and an incapability to phonate comply with in fast succession. These, in tum, are followed by progressive weak spot of the muscular tissues of the face, neck, trunk, and limbs, and by respiratory insufficiency. These signs and signs evolve rapidly, over 2 to four days as a rule, and could additionally be mistaken for those of the Guillain-Barre syndrome. Severe constipation is attribute of botulism, maybe because of paresis of smooth muscle of the gut. Consciousness is retained all through the sickness unless extreme degrees of anoxia develop on account of respiratory failure. In the past, the mortality was greater than 60 p.c, nevertheless it has declined significantly in recent a long time, with improvements in the intensive care of acute respiratory failure and the effectiveness of C. In patients who get well, improvement begins inside a number of weeks, first in ocular motion, then in other cranial nerve features. This antitoxin could be obtained from the Centers for Disease Control and Prevention, Atlanta, Georgia. An preliminary dose of 10,000 U is given intravenously after intradermal testing for sensitivity to horse serum, adopted by day by day doses of 50,000 U intramuscularly till enchancment begins. Guanidine hydrochloride (50 mg/kg) has been considerably useful in reversing the weakness of limb and extraocular muscles. The therapeutic injection of small portions of botulinum toxm into a muscle affected by dystonia or spasticity will weaken or paralyze it for weeks to months (see Chap. Mild symptoms of botulism can happen with relatively giant doses, primarily affecting the oropharyngeal and ciliary muscular tissues. Ergot is used therapeutically to control postpartum hemorrhage attributable to uterine atony; considered one of its alkaloids, ergotamine, is used within the remedy of migraine (see Chap. Chronic and repeated use of the drug is the usual cause of ergotism; acute overdosage in the postpartum state or within the remedy of migraine could cause an alarming rise in blood stress. Two kinds of ergotism are recognized: gangrenous, which is attributable to a vasospastic, occlusive process within the small arteries of the extremities, and convulsive, or neurogenic, ergotism. The latter is characterised by fasciculations, myoclonus, and spasms of muscles, adopted by seizures. In nonfatal circumstances, a tabes-like neurologic syndrome might develop, with lack of knee and ankle jerks, ataxia, and impairment of deep and superficial sensation. Lathyrism Lathyrism is a neurologic syndrome characterised by the relatively acute onset of pain, paresthesia, and weakness within the decrease extremities, progressing to a everlasting spastic paraplegia. Most of them trigger solely transient gastrointestinal symptoms but some elaborate toxins that can be deadly. The most necessary of those toxins are the cyclopeptides, that are contained in several species of Amanita phalloides and m uscaria and account for greater than ninety percent of fatal mushroom poisonings. Symptoms of poisoning with Amanita often appear between 10 and 14 h after ingestion and consist of nausea, vomiting, colicky pain, and diarrhea, followed by irritability, restlessness, ataxia, hallucinations, con vulsions, and coma. Other important mushroom toxins are methylhydra zine (contained within the Gyromitra species) and muscarine (Inocybe and Clitocybe species). The former provides rise to a medical image much like that caused by the cyclo peptides. The symptoms of muscarine poisoning, which appear inside 30 to 60 min of ingestion, are primarily these of parasympathetic stimulation-miosis, lacrima tion, salivation, nausea, vomiting, diarrhea, perspiration, bradycardia, and hypotension. If vomiting has not occurred, it ought to be induced with ipecac, following which activated charcoal must be administered orally so as to bind what toxm stays in the gastrointestinal tract. A local poison control heart could assist determine the toxic mushroom and its toxin. Even extra essential, the gathering and ingestion of subject varieties of mushrooms must be left to those completely sure of their identification.
100 mg altezym for saleA tendency to cramp and ache has additionally been famous in a number of the congenital myopathies and in some fami lies with Duchenne and Becker dystrophies antimicrobial toilet seats generic altezym 500mg visa. A patient of ours with this condition had many years of persistent diarrhea antibiotics for uti and yeast infection discount altezym 100 mg otc, alopecia virus removal mac cheap 500mg altezym with visa, and steady bacteria energy source discount altezym 250mg with mastercard, extremely painful calf cramps that had the gross seem ance of fasciculations. The explanation for the disorder is obscure but is ten tatively presumed to be autoimmune. Glucocorticoids, particularly in excessive doses over short periods, have been tried with some success; dantrolene has also been used and we had the impression that plasma exchange might have been helpful in one case. Under these cir cumstances, stimulation of a muscle via its nerve at high frequencies (15 to 20 times per second) reproduces spasms, and hyperventilation and ischemia enhance the tendency. Indeed, the Trousseau sign-carpal spasms with occlusion of the blood supply to the arm-takes advantage of the latter phenomenon. Hypocalcemic tetany is attributable to an unstable depolarization of the axonal membrane of the nerve fiber. During the primary movements after a period of inactivity, a muscle or group of muscle tissue could turn into painful and tender, notably after expo sure to chilly, dampness, or minor trauma, but usually for no cause that can be discerned. Tender areas, as much as a quantity of centimeters in diameter, may be palpated inside the muscle tissue ("fibrositic nodules" by experts), and energetic contraction or passive stretching of the concerned muscular tissues increases the pain-points said to be of diagnostic value, but disputed. Often, symptoms corresponding to mental and physical fatigue, insomnia, and headache are related and lift the suspicion of an anxiety state or depression. These are particu larly distinguished in conditions that are accompanied by cramp and biochemical contracture (phosphorylase and phosphofructokinase deficiency). Muscle weakness that imposes persistent irregular postures on the limbs might trigger stretch injury to muscle tissue and tendons. In all these situations, clinical examine will usually disclose the source or sources of the ache. Diffuse muscle pain, which merges with malaise, is a frequent expression of a giant variety of systemic infections-for instance, influenza, brucellosis, dengue, Colorado tick fever, measles, malaria, relapsing fever, rheumatic fever (in which it was known as "growing pains"), salmonellosis, toxoplasmosis, trichinosis, tularemia, and Weil disease. When the ache is intense, particularly whether it is localized to one aspect of the lower chest and abdomen, the most likely diagnostic chance is epidemic myal gia (also designated as In a quantity of cases the condition clears up in a number of weeks; native heat and therapeutic massage and local injections of anesthetics or steroids are found to give comfort while symptoms are current, however most often it becomes a chronic situation. The continual type of fibromyalgia presents far higher issues, usually disabling the affected person and causing a change in accustomed habits and employment as dis cussed in Chap. It has become one of many prime diag Bornholm disease brought on by Coxsackievirus infection). Those now normally use are simi lar to the one proposed by a committee of the American College of Rheumatology. The foundation for analysis is the presence of widespread pain, including focal areas of pain (trigger points) that might be produced by strain in Poliomyelitis may be accompanied by intense pain at the onset of neurologic involvement, and later the paralyzed muscular tissues might ache. This is true also of the Guillain-Barre syndrome, during which the pain might precede weak spot by several days. Mild muscle ache is a frequent but not a needed accompaniment of polymyositis and dermatomyositis. In the previous, comparable pains were related to instances of irritable bowel or irritable bladder syndromes, dysmenorrhea, persistent headache, and cold intolerance. Depending on how broad a definition one allows for the widespread pain and painful trigger points, most or all sufferers in our experience manifest lots of the similar complaints as these with the chronic fatigue syndrome, which is mentioned in Chap. This topic is mentioned briefly in different sections of this book in relation to back and extremity pain (see Chap. The muscular soreness could also be diffuse or asymmetrical, notably in the proximal arms and shoulders. The periarticular tissues and their muscular attachments are affected primarily and could additionally be tender, however nonetheless, have pointed out that in the majority of sufferers, formal evaluation by modem standards fails to verify the presence of despair, and that when despair coex ists with the muscular complaints, the two are discordant temporally and in severity. While we acknowledge that antidepressants usually give disappointing outcomes and that in our apply there have been a quantity of patients with fibromyalgia who appeared to be psychologically sound that is tough to interpret, as a outcome of tender ness in these regions may be present in wholesome individu als. The sedimentation fee is elevated in the majority of patients, and a 48-h trial of prednisone, by completely alle viating muscle ache, confirms the analysis. Fibromyalgia remains a problematic illness, outlined largely by a pattern of ache that justifies its name. This condition is a favourite sickness with physiotherapists, who claim that their bodily measures are useful, as they might be. Rarely, a similar syndrome is the forerunner of what proves, after some days, with the onset of neurologic indicators, to be a radiculitis, brachial neuritis, or outbreak of herpes zoster (see Goldenberg). In each reported collection, such as that of Serratrice and coworkers, half of the instances with diffuse myalgia are of this unsure kind. Muscle or tendinous rupture is often brought on by a violent pressure attended by an audible snap after which a bulge, which seems when the muscle contracts. A very focal weakening in contractile energy and gentle discom fort are often famous by the patient. Often, the affected person observes that aching ache happens not on the time of exercise however some hours or even a day or two later, resembling the discomfort following the excessive use of unconditioned muscles. In a couple of situations an elevated sedimentation price or other laboratory aids might clarify the prognosis, and muscle biopsy could reveal a nonspecific interstitial nodular myositis or the giant cell arteritis related to polymyalgia rheumatica. A few people go on to have the options of the previously described fibromyalgic syndrome. However, this cluster of symptoms most often happens with out rationalization, and one can solely suspect an obscure infec tion or a refined aberration of muscle metabolism, pres ently unimaginable to reveal. Tumors of muscle embody desmoid tumor (a benign huge progress of fibrous tissue noticed most often in parturient ladies and after surgery), recurrence and metastasis), rhabdomyosarcoma and (a highly malignant tumor with sturdy liability to local liposarcoma, angioma. A particular type of occurs in patients with sophisticated and poorly controlled diabetes mellitus (Banker and Chester). Usually it involves the anterior thigh, and occasionally other muscle tissue of the decrease limb. The signs are the sudden onset of pain and swelling of the thigh, with or without the formation of a tender, palpable mass. Extensive infarction of muscle is due to the occlusion of many medium-sized muscular arteries and arterioles, more than likely the end result of embolization of ath eromatous materials from eroded plaques within the aorta or iliac arteries. Recognition of this complication and immo bilization of the limb are of prime practical importance, as one hundred twenty mg (Walton; Taylor et a! It have to be distinguished from the syndromes of painful legs and shifting toes, and from the stressed leg syndrome mentioned in Chap. Before dismissing imprecise muscle aches as an extreme somatic concern, hypothyroidism, hyperparathyroidism, and renal tubular acidosis, hypophosphatemia, hypogly cemia, and the intrinsic phosphorylase or phosphofructo kinase defects must be considered. Patients with these latter ailments typically complain of soreness, stiffness, and lameness after strenuous muscular effort. The pretibial, or compartment syndrome, additionally well recognized, follows direct trauma or extreme activ ity (marching, exercising of unconditioned muscles) or ischemic infarction due to arterial occlusion. There is swelling of the extensor hallucis longus, extensor digi torum longus, and anterior tibial muscles.
Discount altezym 100 mg with visaMost reports attribute this syndrome to infil In yet different instances infection 8 weeks after c section altezym 250mg lowest price, the neuropa tration of neural by malignant plasma cells rather than to hyperviscosity antibiotic vs probiotic purchase altezym 500mg line. The polyneuropathy best antibiotic for uti least side effects purchase 250 mg altezym with mastercard, when present top antibiotics for acne purchase altezym 250 mg, evolves over months or longer and could additionally be asymmetrical, significantly on the onset, however turns into bilateral, primarily sensory, and distal. The pattern in our patients has been very slowly progressive, and initially limited to the feet and legs with sensory ataxia and lack of knee and ankle jerks. In a case recorded by Rowland and colleagues, the polyneuropathy was purely motor and simulated motor neuron illness. As mentioned within the part on vasculitic neuropathies, cryoglobulin, a serum protein that precipitates on cooling, is usually of the IgG or IgM kind and most often polyclonal. While cryoglobulinemia might happen with none obvious associated situation (essen tial cryoglobulinemia), it additionally accompanies all kinds of disorders corresponding to multiple myeloma, lymphoma, con nective tissue disease, continual infection, and notably, hepatitis C. Peripheral neuropathy occurs in a small proportion both of the important and symptomatic instances. Occasionally the neuropathy evolves over a interval of some days and remits quickly. More usually it takes the type of a distal symmetrical sensorimotor loss, which develops insidiously (76 % of the cases within the sequence reported by Gemignani et al) in affiliation with the Raynaud phenomenon and purpuric eruptions of the pores and skin. Later, weak point and wasting develop, more in the legs than within the arms, and roughly in the identical distribution because the vascular changes. In some cases there could also be a mononeuropa thy multiplex with severe denervation within the territory of the involved nerves (9 % of the series reported by Gemignani et al; see also Garda-Bragado et al). As remarked earlier, detection of cryoglobulin requires particular handling of the blood sample. The speci males ought to be carried to the laboratory in a shower of heat water to forestall precipitation of the protein. Any of the paraproteinemic states could also be associated with an amyloid polyneuropathy, a topic accorded a separate part later within the chapter. The pathology of the cryoglobulinemic and macro globulinemic neuropathies has been incompletely studied and the mechanisms by which these problems trigger neuropathy are unsure. One presumes that some com ponent of the paraprotein acts as an antineural antibody or that deposition of the protein is in some way poisonous to the nerves or to the endoneuria! In our most totally autopsied case, there was widespread distal axonal degeneration of nonspecific kind with out amyloid deposition or inflammatory cells; but in different reported cases, amyloid has been found in the nerve and the neuropathy has been attributed directly to it. Immune thy of cryoglobulinemia is a result of the intravascular deposition of cryoglobulins, inflicting a more acute vas culitic mononeuropathy multiplex, as discussed earlier (Chad et al). We have used plasma trade and added immunosuppression in the vasculitic number of this illness. In addition, there are quite a few sporadic situations of a peripheral neuropathy brought on by amyloid deposition. As within the familial variety, the guts, kidneys, and gasoline trointestinal tract may be concerned. This acquired kind of amyloid illness has additionally been called main systemic amyloidosis to distinguish it from the variability associated with continual diseases. The time period is deceptive in that typically the amyloid is derived from a circulating para protein, however the proportion of "benign" and malignant plasma cell sources of the protein varies from one report to another. For instance, in the giant sequence collected by Kyle and Bayrd, only 26 percent of patients with primary amyloidosis had a malignant plasma cell dyscrasia. This agrees with our own expertise, however other series have found rates of myeloma as excessive as 75 p.c. In any case, ninety p.c of main amyloidosis is the outcome of a monoclonal protein in the blood (rarely polyclonal). Macrophage enzymes cleave the bigger immunoglobulin molecules and the sunshine chains mixture to form amy loid deposits in tissue, or the plasma cells may produce mild chains instantly ("light chain illness"). Lambda mild chain predominates in the idiopathic number of amyloi dosis and kappa light chain is extra frequent in myeloma. In a number of instances, the light chain is found solely in the urine (as Bence Jones protein). In contrast, familial amyloidosis, a 3rd selection, is almost invariably associ ated with neuropathy but is related to a parapro tein in solely a small proportion of circumstances and the amount of immunoglobulin is small (see "Inherited [Familial Amyloidosis] Amyloid Neuropathies" later). In our medical material, nearly all of the patients have had peripheral neuropathy, but this will likely replicate a referral bias as in different sequence, lower than one-third were so affected (Kyle et al). The neuropathic signs and signs are similar to these of hereditary amyloid poly neuropathy discussed additional on, however the progress of the disease is considerably more fast. The preliminary syndrome is primarily sensory-numb ness, paresthesias, and very often, acral pain-signs that are primarily attribute of involvement of small diameter sensory fibers (loss of ache and thermal sensa tion). It is the painful facet and the autonomic features discussed later that distinguish this illness from the other paraproteinemic neuropathies and indeed, from most other polyneuropathies. Weakness follows, initially limited to the toes but turning into more extensive as the disease progresses and finally spreads to the palms and arms. Only later is there lack of mainly giant fibers that mediate sensations of contact, pressure, and pro prioception. Twenty-five percent of sufferers have carpal tunnel syndrome from infiltration of the flexor retinacu lum. Exceptionally, patterns other than the painful and sensory predominant polyneuropathy have been associ ated with amyloidosis; preferential involvement of motor nerves, lumbar roots, plexopathy, and amyloidomas involving single nerves (sciatic, facial, trigeminal) have been reported. Autonomic involvement can be severe in amyloid neu ropathy (familial or primary) and may become evident early in the midst of the sickness; a number of of our patients introduced with disturbances of gastrointestinal motil ity such as episodic diarrhea and orthostatic dizziness or erectile dysfunction and bladder disturbances. The pupils may show a sluggish response to gentle, or there could also be a reduction in sweating. An infiltrative amyloid myopathy additionally occurs as a uncommon complication of the illness; it pres ents as an enlargement and induration of many muscles, particularly those of the tongue (macroglossia), pharynx, and larynx. Progression of the sickness is comparatively rapid, the mean survival being 12 to 24 months. Death is a results of the renal, cardiac, or gastrointestinal results of amyloid deposits, the manifestations of that are already evident in more than half of the sufferers who present with neuropathy. Analysis of the serum and urine, searching for an abnormal paraprotein, is probably the most useful screening take a look at for amyloid neuropathy. Next in value is a microscopic exami nation of a biopsy of the stomach fats pad, gingiva, or rectal mucosa for deposition of amyloid in tissue or blood vessels. Biopsy of the sural nerve or of the concerned viscera has a high diagnostic yield; muscle tissue offers variable outcomes. The liver biopsy is positive in just about all instances of main amyloid and the kidney exhibits amyloid infiltration in 85 %. In a number of of our patients with a medical syndrome typical of amyloid neuropathy but in whom amyloid was absent in the sural nerve, the diagnosis was established only after sequential biopsy of quite a few sites (fat pad, kidney, liver). If the sural nerve is severely depopulated of nerve fibers, the quantity of congophilic staining and the attribute amyloid birefringence could also be meager and yield a spuriously unfavorable outcome. It can also be crucial to make positive the accuracy of congophilic staining by comparison with positive and negative control tissue from the same laboratory. Lachmann and colleagues (2002) emphasised that 10 p.c of sufferers who appear by all the standard crite ria to have primary amyloidosis might be found to have a genetic sort. Attempts at immunomodulation, immunosup pression (which might help the renal disease), or removing of amyloid by plasma change have been marginally effective.
Order altezym 250 mg free shippingThe correspondence between mathematical mod els of the electrical properties of the membrane and the scientific options of the myotonic and periodic paralyses is quite outstanding oral antibiotics for acne uk generic altezym 250mg. During the traditional action potential in all neural and muscular tissue antimicrobial soap purchase altezym 500 mg otc, membrane depolarization is terminated by two occasions: the depolarization-induced inactivation of the sodium channel (which ends the inward sodium current) and the subsequent motion of the outward potassium present antibiotics you can give dogs generic 250 mg altezym amex. Because of its large size virus attacking children buy altezym 500 mg visa, excitation of the muscle fiber involves depolarization that propagates not solely alongside the cell floor but additionally radially into the middle of the muscle cell via the transverse tubules (T tubules). The tubules are very narrow structures whose inside areas are in continuity with the extracellular space. When the repolar izing outward potassium current is activated, potassium ions flood into the tubules from the muscle cytoplasm. By itself, this tubular K accumulation would depolarize the muscle membrane and prolong excitation. The first clues to the significance of the chloride chan nel in this electrical stabilizing course of had been obtained by Bryant who performed in vitro research of myotonic goat muscle and found a reduced chloride conductance in the transverse tubular system. Subsequent research of muscle from sufferers with myotonia congenita by Lipicky and Bryant (1971) demonstrated a similarly low chloride conductance. As indicated, an important event for regular repolar ization of an excitable membrane is the rapid inactiva tion of the inward sodium current. This means of speedy, complete sodium channel inactivation is impaired by the sodium channel mutations implicated in hyperkalemic periodic paralysis. The mutations trigger imperfect inac tivation of the channel and lead to aberrant and early reopenings. The downside becomes self-reinforcing as a result of, because the membrane fails to repolarize totally, its elec trolytic inactivation becomes increasingly less efficient. These features are evident in hyperkalemic muscle in vitro (Cannon) and could be recapitulated in computer simulations of aber rant channels. The historical past of the illness is difficult to trace, but the first unmistakable account was probably that of Hartwig in 1874, adopted by the accounts of Westphal (1885) and Oppenheim (1891). In 1937, Aitken and associates described the prevalence of low serum potas sium throughout attacks of paralysis and reversal of the paralysis by the administration of potassium, thus setting the stage for subsequent differentiation from the hyper kalemic forms of periodic paralysis. The traditional sample of inheritance is autosomal domi nant with lowered penetrance in ladies (male-to-female ratio of 3 or 4:1). Fontaine and coworkers (1990, 1994) localized the mutation to a area containing the gene that encodes the alpha subunit of the calcium channel of skeletal muscle and the gene has now been determined. The subunit, which is a half of the dihydropyridine recep tor advanced, is situated in the transverse tubular system. This area is believed to act each as a voltage sensor that controls calcium release from the sarcoplasmic reticulum, thus mediating muscle excitation-<:ontraction coupling, and as a calcium-conducting pore. The typical attack comes on in the course of the second half of the night or the early morning hours, after a day of unusually strenuous train; a meal rich in carbohydrates favors its growth. However, diurnal assaults additionally happen, especially after a nap that follows a big meal. The assault evolves over minutes to several hours; at its peak, it might render the patient so helpless as to be unable to name for assistance. Once established, the weak point lasts a few hours if gentle or several days if extreme. The legs are often weakened earlier than the arms, but exceptionally the order is reversed. The muscles most probably to escape are these of the eyes, face, tongue, phar ynx, larynx, diaphragm, and sphincters, however every so often even these could also be concerned. When the attack is at its peak, tendon reflexes are lowered or abolished and cuta neous reflexes can also disappear. As the assault subsides, energy typically returns first to the muscular tissues that had been last to be affected. Attacks of paralysis tend to happen every few weeks and tend to reduce in frequency with advancing age. Rarely, death might happen from respiratory paralysis or derangements of the conducting system of the center. During middle grownup life, numerous sufferers have developed a extreme, slowly progressive proximal myopathy, with vacuolated and degenerated fibers and myopathic action potentials, in some instances long after attacks of periodic paralysis had ceased. Diagnosis at a time when the affected person is regular may be facilitated by provocative tests. There are pathologic adjustments in myofibrils and mitochondria as properly, and focal increases in muscle glycogen. Electron microscopic research have shown that the vacu oles arise as a outcome of proliferation and degeneration of membranous organelles within the sarcoplasmic reticu lum and transverse tubules (A. The fall in serum K is related to little or no enhance in urinary K excretion. Presumably, giant portions of K enter the muscle fibers throughout an attack but this explanation will not be full. Some episodes happen with near-normal ranges of K, and weak spot persists for a time after the serum stage has been restored. Although the shifts in K are of undoubted importance within the pathogenesis of muscle weak point, the marked sensitivity to small reductions of serum K means that other components are operative and that the autumn in K could also be a secondary phenomenon. A decline in power precedes the loss of motor unit potentials and the failure of propagation of action potentials over the surface of the fiber. The polarization potentials of muscle fibers measured by intracellular recordings are initially regular regardless of the failure of impulse propagation by the sarcolemma. One would anticipate the muscle fiber to be hyperpolarized as K strikes into it, nevertheless it actually becomes depolarized. If this approach fails, a low-carbohydrate, low-salt, high-K diet mixed with a slow-release K preparation could additionally be efficient. For the late-progressive polymyopathy that follows many severe assaults of periodic paralysis, Dalakas and Engel report profitable restoration of power by the long-term administration of dichlorphenamide. Other types of secondary hypokale mic weakness have been observed in patients affected by chronic renal and adrenal insufficiency or problems brought on by a loss of potassium, as occurs with extreme use of diuretics or laxatives (the most typical cause in practice). Rarely, as already famous, main aldosteron ism is produced by the persistent ingestion of licorice; this is due to its content material of glycyrrhizic acid, a potent mineralo corticoid (Conn et al, 1968). The muscle fibers of patients with major aldoste ronism show necrosis and vacuolation. Ultrastructurally, the necrotic areas are characterised by dissolution of myofilaments with degenerative vacuoles; nonnecrotic fibers include membrane-bound vacuoles and present dila tation of the sarcoplasmic reticulum and abnormalities of the transverse tubular system, suggesting that vulner ability of the latter structures could additionally be responsible for the muscle fiber necrosis (Atsurni et al). It is characterised by rapidly rising physique temperature, extreme muscular rigidity, and a high mortality price. Since the unique report by Denborough and Lovell in 1960, as larger experience was gained with this entity, it proved in some circumstances to be a metabolic myopathy inherited as a dominant trait, rendering the individual vulnerable to any unstable anesthetic agent, notably halothane, and to the muscle relaxant succi nylcholine. The basic cause in a big proportion of instances is an aberration in a element of the ryanodine calcium channel. Malignant hyperthermia has been esti mated to happen roughly as quickly as in the course of each 50,000 administrations of basic anesthesia. The full scientific picture is hanging however anesthesiolo gists have turn out to be adept at detecting its earliest stages and aborting the process. As halothane or a similar inhalational anesthesia is induced, or succinylcholine is given for mus cular rest, the jaw muscle tissue unexpectedly turn into tense rather than relaxed and shortly rigidity extends to the entire muscular tissues.
Altezym: 500 mg, 250 mg, 100 mg
Buy altezym 250mg lineDyck and colleagues (1975) studied fifty three sufferers in whom the neuropathy progressed for more than 6 months antibiotic resistance google scholar buy 100 mg altezym overnight delivery. The scientific course was monophasic and slowly pro gressive in about one-third antibiotic with out a prescription order 500mg altezym overnight delivery, stepwise and progressive in another third garlic antibiotics for acne discount altezym 100mg overnight delivery, and relapsing in the remaining third virus protection for windows xp buy altezym 100mg visa. Weakness of the limbs, particularly of the proximal leg muscular tissues, or numbness, paresthesias, and dysesthesias of the hands and feet were the initial signs. In 45 of the 53 sufferers, the signs have been these of a mixed sensorimotor polyneuropathy with weakness of the shoulder, higher arm, and thigh muscle tissue in addition to motor and sensory loss within the distal components of the limbs. Not emphasized of their sequence is the widespread incidence of a cerebellar-like tremor in cases of lengthy standing. In the collection reported by McCombe et al (1987b) comprising 92 patients, two major subgroups had been acknowledged: relapsing (corresponding to the relapsing and stepwise progressive circumstances of Dyck et al [1975]) and nonrelapsing ones. Chronic symmetric sensorimotor loss and areflexia coupled with nerve conduction findings of demyelination basically defines the illness. Elevated spinal fluid pro tein concentration is so frequent that it may be added as (1975), and Hughes and their associates. The typical findings in nerve conduction research are of multifocal conduction block as described in Chap. In the early phases of the disease, demyelinating features have to be carefully sought by testing a quantity of nerves at several sites alongside their programs. Its frequency as a explanation for acquired poly neuropathy is unknown, however we see several new instances every year. These symptom atic inflammatory polyneuropathies respond to corti costeroids, albeit unpredictably; and to treatment of the underlying illness. In sural nerve biopsy material, half are found to have interstitial and perivascular infiltrates of infl ammatory cells, although one expects that nearly all nerves would show these modifications if a adequate quantity might be sampled. Some specimens show only demyelination, or in circumstances of lengthy standing, severe depletion of all nerve fibers. The lack of myelinated fibers is variable and many of the remaining fibers are seen to be undergoing wallerian degeneration or present modifications of segmental demyelination or demyelination-remyelination. The few sufficient post-mortem studies have proven solely minimal or patchy irritation and a considerable diploma of axonal injury, most likely reflecting the long duration of illness before examination. More than half of our patients have responded to this remedy, albeit for under a quantity of weeks or months, after which the infusions must be repeated to keep medical improvement. A need to spare patients the unwanted aspect effects of indefinite prednisone administration (see later) makes this mode of therapy a reasonable various, in some circumstances for almost 10 years without unwell effects. Patients who require treatment at such quick inter vals as to be impractical have benefited from the addition of small doses of prednisone or of an immunosuppressive drug as described beneath. Rare cases of nephrotic syndrome, aseptic meningitis, serum illness, thrombotic venous, or arterial occlusion, together with stroke and hypotension, have been reported, significantly if the infusion is merely too speedy. In a potential double-blinded trial, Dyck and colleagues (1986a) found that plasma exchange administered twice weekly for three weeks had a helpful effect on each neurologic incapacity and nerve conduction. The effects of plasma exchanges in most patients subside in 10 to 21 days, or even much less; in some, the response lasts longer as found by Dyck and colleagues (1986a) and within the sequence reported by Hahn and colleagues (1996a). For these causes we prefer to try plasma exchange or immune globulin earlier than committing a affected person to long-term treatment with prednisone. These therapies can be supplemented by small doses of prednisone when frequent infusions or exchanges turn out to be impractical. It has been our experience that in about one-third of circumstances, Mg and plasma trade stop to have profit after repeated use for 1 or more years. Corticosteroids have been formerly the mainstay of ther apy, however many sufferers turn out to be dependent on the medica tion and correspondingly endure unwanted effects. Our strategy has been to use corticosteroids as an adjunct to one of many beforehand talked about therapies, but other facilities use them first. Attempts to withdraw the steroids more quickly have led to additional cycles of relapse. A number of sufferers may have no response to corti costeroids throughout the first 1 or 2 months however will improve if therapy is sustained. Barohn and colleagues (1989) have found that the earliest improvement happens solely after 2 months of remedy and is maximal at approxi mately 6 months. Long remissions final ing several years have been reported with using pulses of orally administered high-dose or daily cortico steroids, for instance, by Eftimov and colleagues, who used dexamethasone 40 mg per day for 4 days, repeated for six cycles, or daily prednisolone, 60 mg for six weeks. High-dose cyclophosphamide has confirmed useful in several cases beneath our care, though it has typically failed (see Brannagan et al and the evaluate by Brannagan that lists the applicable medical trials). Individual stories of successful therapy by autologous stem cell transplantation after high-dose chemotherapy have appeared however 1 affected person relapsed after 5 years (Vermuelen and van Oers). It has been acknowledged that sufferers with discrete relapses have a better prognosis than those with a progressive course. In fewer than 10 % of patients has the illness finally remitted; additionally, unexplained remission happens occasionally. The 5-year followup of 38 patients by Kuwahara and colleagues offers a figure of 49 percent with full or partial remission, far higher than in our series. The latter has as its primary function a block of combined nerve conduction at focal sites in a limited number of nerves as described earlier. In multifocal motor neuropa thy, solely blocks in motor nerve conduction are evident. They usually begin with an acute or subacute motor mononeuropathy, manifest, for example, as weak point of the wrist or foot-drop, and are often joined insidiously by another focal motor palsy. The process is painless, not like vasculitic mononeuritis mul tiplex, includes the nerve incompletely, and, in its usual type, is unaccompanied by any sensory signs similar to paresthesias or numbness. Usually, the tendon reflex is misplaced or muted in an affected area, but for unexplained causes, some sufferers have a quantity of brisk reflexes. This conforms to what has been known as Lewis-Sumner syndrome based mostly on the outline by these authors and their colleagues of subacute, painless asymmetric, distal a number of mononeuropathies. The ulnar and median nerves were involved in their sufferers and there was motor conduction block and sensory slowing in affected nerves. Curiously, 2 of their 5 original sufferers had optic neuritis, a function not reported subsequently. Some authoritative clinicians favor the early addition of rituximab in treat ment-resistant instances or when the frequency of infusions is unsustainable and if that fails, cyclophosphamide. Other immune-modulating medication have been tried in small collection with various results. In all types of uremic polyneuropathies, pathologic changes are most intense in the distal segments of the happens in different acquired demyelinating polyneuropa the purpose for uremic polyneuropathy is unknown. In distinction, the transplanted kidney successfully eliminates substances of wide-ranging molecular weights, which might account for the almost invariable enchancment of neuropathy after transplantation. As described originally by Asbury and associates (1963), the neuropathy takes the form of a ache less, progressive, symmetrical sensorimotor paralysis of the legs and then of the arms. In some patients, the syndrome begins with burning dysesthesias of the ft or with sensations of creeping, crawling, and itching of the legs and thighs, which tend to be worse at evening and are relieved by motion (comparable to "stressed legs" syn drome described in Chap. Thus this disease, although subacute in its evo lution as described earlier in the chapter, turns into a frequent explanation for persistent polyneuropathy.
References - Bagley, D.H., Grasso, M. Ureteroscopic laser treatment of upper urinary tract neoplasms. World J Urol 2010;28: 143-149.
- Calhoun BC, Gomes F, Robert ME, et al. Sampling error in the standard evaluation of endoscopic colonic biopsies. Am J Surg Pathol. 2003;27(2):254-257.
- Roehrborn, C., Issa, M., Bruskewitz, R. et al. Transurethral needle ablation for benign prostatic hyperplasia: 12-month results of a prospective, multicenter U.S. study. Urology 1998;51:415-421.
- Nikolic SD, Tamura K, Tamura T, et al: Diastolic viscous properties of the intact canine left ventricle, Circ Res 67:352-359, 1990.
- Bodizs R, Kis T, Lazar AS, et al. Prediction of general mental ability based on neural oscillation measures of sleep. J Sleep Res 2005;14(3):285-92.
- Coe FL, Evan AP, Lingeman JE, et al: Plaque and deposits in nine human stone diseases, Urol Res 38(4):239n247, 2010.
- Ross SS, Kardos S, Krill A, et al: Observation of infants with SFU grades 3-4 hydronephrosis: worsening drainage with serial diuresis renography indicates surgical intervention and helps prevent loss of renal function, J Pediatr Urol 7(3):266n271, 2011.
|

