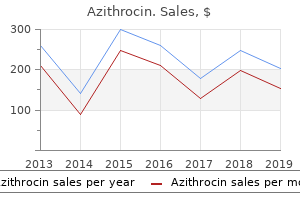
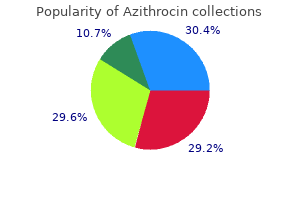
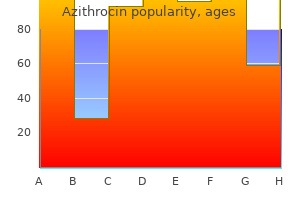
Azithrocin
Neda Zadeh, M.D. - Children’s Hospital of Orange County
- Orange, California
Azithrocin 100 mg with visaSkull fractures are greatest thought of as involving the cranial vault or the skull base infection control risk assessment purchase 100 mg azithrocin fast delivery. Cranial vault fractures are further divided into linear or depressed antibiotics alcohol purchase 100mg azithrocin with visa, and open or closed antibiotic classifications order azithrocin 250mg with amex. Basilar cranium fractures are generally linear and mostly involve the anterior cranial base and the petrous part of the temporal bone infection behind ear lobe buy generic azithrocin 250mg on line. Approximately 4% of significant head accidents embrace cranium base fractures, with most (90%) the results of closed head trauma and the remainder involving penetrating trauma. Open depressed cranium fractures could additionally be related to vital morbidity and mortality. The affected person sustained minimal brain injury from the impression as a end result of the facial and anterior frontal sinuses absorbed a lot of the energy, cushioning the brain during impact, very related to an air bag. B, Image from a preoperative sagittal T1 magnetic resonance imaging research without contrast demonstrates the tract of a nasogastric tube via the frontal lobe in a 42-year-old lady with an anterior cranial base defect (arrow). B, Computed tomography three-dimensional reconstruction also demonstrates the depressed skull fracture (arrow). Under these circumstances, the risks related to surgical procedure are increased, and elevation of the fracture fragment typically is reserved for important compromise of venous drainage. Open depressed cranial fractures could also be handled nonoperatively if medical and radiographic examination reveals no proof of dural penetration, significant intracranial hematoma, depression higher than 1 cm, frontal sinus involvement, gross beauty deformity, wound infection, pneumocephalus, or gross wound contamination. The potential house between the internal desk of the skull and the dura is the epidural house. The affected person was a 32-year-old man hit on the back of the top by a metal beam at a building website who introduced with a deteriorating level of consciousness. When a fracture extends across the bony groove of the artery, it could possibly tear and bleed. A lucid interval happens when a patient initially is rendered unconscious from a concussive head injury that causes a linear skull fracture involving the middle meningeal artery with bleeding into the potential epidural space. Because the dura is tightly adherent to the inner desk of the cranium, significant pressure is needed to push the dura off the inside desk. An arterial hemorrhage generally has sufficient pressure to strip the dura off the bone, converting the potential epidural house into a mass. The bony attachment of the dura becomes progressively stronger with age; therefore the dura of a younger patient requires much less drive to push off the bone than would be required in an older affected person. The medial part of the temporal lobe, the uncas, lies just lateral to the brainstem at the level of the third cranial nerve (oculomotor nerve), which runs alongside the tentorial edge. This may trigger a contralateral hemiparesis from direct compression of the cerebral peduncle and a decrease in stage of consciousness from the impact on the reticular activating system within the brainstem. Occasionally, as a substitute of directly compressing the ipsilateral cerebral peduncle, the herniating uncas can shift the brainstem itself into the contralateral tentorial edge, a relatively sharp rigid structure. Taking a basic view, the patient progresses from unconscious on the time of impact from a concussive harm, to awake, to unconscious once more secondary to brainstem compression-hence the term lucid interval. She was combative on presentation, pharmacologically paralyzed, and intubated in the trauma bay. Note the right frontal traumatic subarachnoid hemorrhage (small, skinny arrow) and the small amount of air (arrowhead) from the related open, linear fracture (arrow), seen in B. No prospective randomized trials have been carried out to compare surgical remedy with nonoperative administration, nor should there be. One suboptimally controlled research reported worse outcomes in a small group of sufferers who underwent emergency operations by non-neurosurgeons and attributed this mainly to the technical inadequacy of the operation. Note that the hematoma expands the subdural area and follows the contour of the mind because it generates extreme extra-axial mass impact and shift. Subdural Hematoma Deep to the epidural area, below the dura, is the subdural compartment. Anatomically, bridging veins course through the subdural house from the cerebral hemispheres to the superior sagittal sinus. After this time, the clot steadily and progressively lyses, resulting in a mixture of clot and fluid as it transitions to the subacute phase. A membrane usually surrounds these hematomas, and the collection of fluid may slowly develop in size because of repeated small bleeds or accumulation of fluid transudate from the membrane. If the quantity of shift is immediately proportional to the thickness of the extra-axial clot, the damage is likely to be simple and the brain merely compressed. However, if the quantity of shift is more than anticipated as indicated by the dimensions of the hematoma, then additional parenchymal mind harm probably is current under the clot, causing additive mass effect. There is a major increase in poor outcome among sufferers older than 60 years of age with severe head damage in general. Contusions usually involve the crests of the gyri however in additional extreme injury might lengthen into the substance of the white matter. The quantity of vitality delivered could have only been sufficient to trigger failure of small vessels, resulting in contusions. If more energy is delivered, failure of larger vessels could happen, resulting in hematomas. Alternatively, the hemorrhagic component of a contusion might proceed to bleed and coalesce right into a extra discrete hematoma. In basic, the commonest traumatic parenchymal lesions are contusions,one hundred thirty and so they tend to evolve. These delayed hemorrhages are reported to occur in as much as 7% of patients with extreme head accidents. Coup contusions happen within the brain tissue underneath the influence web site and are often associated with an acceleration harm. Contrecoup contusions are positioned away from the purpose of influence and are usually related to a deceleration injury. In trauma, the trigger of tissue damage may be any of three types of induced strains: compression, pressure, and shear. The cranium, mind, and blood vessels will tolerate compression better than tension, and pressure better than shear. These strains are induced by contact or inertia (relative to acceleration-deceleration), or both. B, Intraoperative photograph of decompressed brain reveals hemorrhagic, inflamed, and edematous brain swelling out by way of the cranial defect. Occasionally, the distribution of the hemorrhage may be hard to differentiate from an aneurysmal hemorrhage. Note the large, homogeneous areas throughout the contusions that could be categorized as hematomas. As a consequence of contact the pinnacle is ready in movement, which finally ends up in inertial damage. Inertial accidents may trigger harm by differential acceleration of the cranium and brain. In addition, acceleration-deceleration can independently produce strains within the mind itself. The two clinically related forms of acceleration are translational (when the mind moves in a straight line) and angular.
Buy discount azithrocin 500mgThe timing of stroke could be difficult to gauge as a result of anesthesia renders physical/neurologic examination ineffective in the course of the 4- to 6-hour procedure/recovery infection of the prostate buy discount azithrocin 100 mg. Respiratory failure could additionally be the result of a selection of causes antibiotic resistance jokes azithrocin 250mg with mastercard, some of which can not directly involve the lungs or the respiratory muscle tissue virus zero air sterilizer order azithrocin 500 mg on-line. Common causes of hypoxemic and hypercapnic respiratory failure are listed in Box 36 antibiotics for acne nodules order azithrocin 250mg mastercard. Hypoxemic Respiratory Failure Basic Mechanisms the five fundamental mechanisms of hypoxemia are listed in Box 36. Most of the abnormalities improve with the administration of supplemental oxygen, apart from a shunt abnormality by which the Pao2 continues to be low regardless of the administration of high levels of supplemental oxygen. Type 1 is hypoxemic respiratory failure (oxygenation failure), and sort 2 is hypercapnic failure (ventilatory failure) with or with out hypoxemic respiratory failure. The respiratory failure could be acute or persistent in nature, associated to the onset and duration of the failure. Hypercapnic Respiratory Failure Hypercapnic respiratory failure may end up from a big selection of disorders as listed in Box 36. However, these sufferers might have acute exacerbations or comorbid conditions that cause them to decompensate into acute-on-chronic respiratory failure. Disorders that improve the respiratory load (such as a circumferential chest burn eschar or flail chest) or impair function of the respiratory muscle tissue (such as kyphoscoliosis) also result in hypoventilation. The patient with respiratory misery might manifest gasping air flow, nasal flaring, or use of the accessory muscles of respiration. Intercostal retractions may be seen, and the affected person might exhibit paradoxical respiratory movement. Typically sufferers with acute respiratory failure, whether type 1 or type 2, have altered coronary heart fee and blood pressure. The majority demonstrate a sympathetic response with tachycardia and hypertension, however sufferers may be hypotensive and bradycardic. Patients with acute respiratory failure are normally in misery and sometimes appear apprehensive. Hypercapnic sufferers may show indicators of a respiratory encephalopathy, together with somnolence, coma, asterixis, seizures, tremors, or myoclonic jerks. Although the administration of acute respiratory failure is complex and reviewed elsewhere on this textbook, a substantial quantity of effort has targeted using noninvasive air flow or high-flow nasal cannula to keep away from the use of intubation and invasive ventilatory help. Among the primary benefits of the uniform definition could be improved communication and enhanced clinical trial design. The scientific manifestations of respiratory distress could additionally be subtle and nonspecific or may be apparent to even the untrained observer. Other frequently encountered scientific risk components embody a number of emergency transfusions; aspiration harm; near-drowning; pancreatitis; trauma. Most of the reported circumstances are related to surgical procedures: thyroidectomy,forty four septorhinoplasty,45 tonsillectomy/adenoidectomy,forty six mandibular open reduction and inner fixation,forty seven or cryosurgery for a tracheal obstruction. Clinical manifestations of hypoxemia and respiratory misery may be delayed as a lot as 6 hours. Pathologic Manifestations Type 1 alveolar epithelial cells compose the most important gas trade surface of the alveolus and are integral to the upkeep of the permeability barrier function of the alveolar membrane. Incidence and mortality of acute lung harm and the acute respiratory distress syndrome in three Australian states. These dependent areas of injury encompass regions of alveolar flooding from the gravitational accumulation of lung water, areas of lung injury, and regular lung areas. The relatively normal ventral (nondependent) lung has been referred to as the "baby lung," and the injured (dependent) lung has been referred to as the "sponge lung. A weaning protocol was used as soon as the affected person was receiving a lowered amount of ventilatory help. The trial was terminated after 861 patients had been enrolled after the determination of a big (22% relative reduction) lower in mortality fee associated with the use of low Vts (39. There is an enhanced ability to recruit alveoli when the affected person is in the inclined position in contrast with the supine place related to stabilization of the anterior chest wall. It is possible that if this affiliation is cause and effect that it might be associated to delayed implementation of lungprotective ventilatory support. There was no distinction in the development of shock or the need for renal substitute remedy between the two fluid administration strategies. Prophylactic methods to forestall stress-related mucosal illness and gastrointestinal bleeding using H2-blockers, proton pump inhibitors, or presumably early enteral vitamin should happen in all sufferers until in any other case contraindicated. The group that acquired a recruitment maneuver did have a greater decrease in blood pressure during the maneuver. The worse outcome within the experimental group was doubtlessly because of an unfavorable balance between the possibly constructive impact of lowering driving strain and negative effects of accelerating overdistention and hemodynamic impairment. Inhaled Vasodilator Therapy Inhaled vasodilators, like nitric oxide or prostacyclin, are bronchial and vascular smooth muscle dilators that additionally lower platelet adherence and aggregation. Food and Drug Administration, is dear, could have an result on platelet operate, and could also be related to an increase incidence of acute kidney harm. For patients with high cardiac output needs, adequate move may be ensured by utilizing large-bore catheters or central cannulation methods. Our goal is to work towards early extubation, if possible, so that we are ready to cut back sedation and allow the affected person to participate in rehabilitation and mobilization. To date, none of these approaches has been demonstrated to supply significant benefit in well-conducted, prospective, randomized managed, multicenter scientific trials. These approaches have included the early administration of high-dose corticosteroids, prostaglandin E1, nonsteroidal antiinflammatory medication, antiendotoxin, and anticytokine remedy. Preliminary research have suggested that microparticles released from mesenchymal stem cells could also be instrumental in lung safety and repair that could be liable for this useful impact. Patients with septic shock, an outlined want for corticosteroid remedy, disseminated fungal infection, or undrained abscess had been excluded. An increase in the white blood cell rely and glucose stage associated to steroid administration occurred, along with a lower in physique temperature. No difference was measured within the main efficacy endpoint 60-day mortality rate, and no vital difference in 180-day outcome occurred between the two groups. In truth, there was extra pneumonia and septic shock within the placebo group than within the steroid-treated group. Unfortunately, the use of steroids was related to more neuropathy and myopathy, however you will need to note that 30% of the steroid-treated patients had been receiving neuromuscular blocking drugs. Of interest was the statement that the macrolide-treated sufferers had a 23% mortality price in contrast with a 36% mortality fee for nonmacrolide antibiotic regimens. This data will likely affect and direct future administration as we transfer additional alongside the path of precision management of medical conditions. In years to come, scientists might probably modify the genetic make-up or the biologic response of a prone individual by inserting chosen genes or modifying the transcription or operate of varied regulatory proteins.
Cheap 100 mg azithrocin amexIn addition infection hacked buy 100 mg azithrocin overnight delivery, a big selection of viral infections (rubella; coxsackievirus kind B; mumps; Epstein-Barr virus; cytomegalovirus; and hepatitis A antibiotic resistance among bacteria azithrocin 250 mg amex, B antibiotics for uti in hospital cheap azithrocin 100mg line, and C); Mycoplasma pneumoniae; and parasites corresponding to A antimicrobial bit in mouthwashes purchase azithrocin 100 mg fast delivery. Of patients with acute pancreatitis, solely roughly 5% develop pancreatic infections; nevertheless, the best mortality price from pancreatitis occurs in these patients. Patients with extensive necrosis, those who are very unwell, and those with early infection have the very best mortality charges. Clinically, this could be very troublesome to decide whether patients with necrotizing pancreatitis have superimposed an infection because sterile pancreatic necrosis might trigger leukocytosis and fever even in the absence of an infection, and roughly 50% of contaminated sufferers might not present early clinical signs of infection. Fungal infection of necrotic pancreatic tissue is being reported with elevated frequency. Antibiotics that penetrate into pancreatic tissue include the carbapenems, especially imipenem, fluoroquinolones, piperacillin, advanced generation cephalosporins, and metronidazole. Some patients could have little or no diarrhea however current with poisonous megacolon, colonic perforation, peritonitis, or even septic shock without other localizing symptoms. Oral metronidazole stays the first-line remedy for gentle to average disease; empiric remedy with oral metronidazole ought to be began while testing for C. Oral vancomycin must be administered to those with severe an infection or unresponsiveness to or intolerance of metronidazole. First recurrence may be treated with metronidazole, vancomycin, or fidaxomicin but subsequent recurrences should be handled with fidaxomicin or vancomycin. The use of fecal microbial transplantation in recurrent or extreme disease corresponding to poisonous megacolon has yielded favorable results with excessive success rates. A number of surgical procedures, including diverting ileostomy, cecostomy, colostomy, and subtotal colectomy, have been performed to manage toxic megacolon. Subtotal colectomy is taken into account the process of alternative for the administration of fulminant poisonous megacolon. These infections spread Clostridium difficile Colitis Clostridium difficile colitis is the commonest and costly well being care�associated infection in the United States. Potentially life-threatening infections of the top and neck may contain three cervical areas. The submandibular house may be affected by an infection involving the flora of the mouth and tongue. Manifestations of this an infection embody swelling and upward displacement of the tongue and submandibular swelling. The lateral pharyngeal area consists of an anterior and a posterior compartment divided by the styloid course of. The anterior compartment is composed of musculature, and the posterior compartment has nerves and blood vessels. Infection in the anterior compartment causes soft tissue swelling that ends in unilateral trismus brought on by irritation of the interior pterygoid muscle, induration and swelling alongside the angle of the jaw, bulging of the palatine tonsil into the posterior pharynx, and systemic toxicity. Patients might current with unilateral neck or jaw ache along with ear pain and dysphagia. Pain might worsen when the head is turned due to compression of contaminated tissue. Dental an infection, higher respiratory tract infection, pharyngitis, and otitis media with mastoiditis could all trigger lateral pharyngeal house infection. When infection occurs on this house, patients mostly present with signs of sepsis without localizing indicators on the neck. Generally signs and signs are associated to issues from involvement of the neurovascular constructions. The carotid sheath is dense and not simply penetrated; thus typically arterial erosion is normally a complication of infections of longer period (1�3 weeks). The retropharyngeal house accommodates an space that extends from the bottom of the cranium to the diaphragm and therefore is a portal for neck infections to extend into the chest. Infections of the retropharyngeal area or prevertebral area may spread because of extension by way of this space. Retropharyngeal space abscesses are comparatively uncommon and are most frequently seen in young youngsters. These abscesses often result from odontogenic an infection, penetrating trauma, or peritonsillar abscess. Patients often present with fever, pharyngitis, odynophagia, dysphagia, trismus, drooling, and a muffled voice that has been described as "hot potato" in high quality. The commonest signs of retropharyngeal area an infection in adults are fever, dysphagia, pharyngeal ache, dyspnea, noisy respiration, and stiff neck. Any deep neck infection has the potential to unfold to the mediastinum through the retropharyngeal house. Other potential issues of infection of the oral cavity are aspiration pneumonia and lung abscess. Because most of those infections originate from an odontogenic focus, the microbiology reflects polymicrobial oral flora and generally consists of Bacteroides spp. Complications include hematogenous dissemination with sepsis syndrome, airway obstruction, necrotizing pneumonia or empyema, osteomyelitis of the mandible or maxilla, mediastinitis, or intracranial extension and cavernous sinus thrombosis. When sufferers have dyspnea, stridor, or an incapability to handle secretions, a man-made airway should be established. Airway obstruction is more than likely to happen in infections of the submandibular 860 Pa rt 4 Critical Care Infectious Disease house. Patients with peritonsillar abscess ought to endure incision and drainage to prevent spontaneous rupture, aspiration pneumonia, airway obstruction, or dissection of infection into the lateral retropharyngeal space. Surgical drainage is very important for infections involving the retropharyngeal and lateral pharyngeal house. Mediastinitis Acute mediastinitis is an an infection of mediastinal structures that can develop from direct extension of pharyngeal and neck infections (descending necrotizing mediastinitis), from esophageal trauma or rupture, or as a complication of cardiothoracic surgical procedures. Patients with postcardiothoracic mediastinitis will generally have proof of local or deep sternal wound infection. Plain movies might present mediastinal widening; mediastinal air-fluid levels; and subcutaneous, mediastinal, or pericardial air. Treatment requires surgical drainage and d�bridement along with antibiotic remedy. Most cases arise from the pharynx and peritonsillar tissues with unfold by way of the lateral pharyngeal area leading to inside jugular thrombophlebitis and metastatic problems. Because that is an endovascular an infection antibiotics must be given for an extended interval of up to 6 weeks. When the patient is afebrile and neck ache has resolved, remedy may be de-escalated to an oral routine. Use of anticoagulation is controversial and is usually warranted in circumstances with retrograde cavernous sinus thrombosis. Infection is transmitted to people by a wide selection of ticks but most incessantly by the canine tick, Dermacentor variabilis.
Trusted azithrocin 500 mgWith extra cardiac arrest survivors being uncovered to therapeutic hypothermia bacteria without cell wall order azithrocin 500 mg with amex, practitioners should now achieve a traditional core temperature virus update discount azithrocin 250 mg line, defined as near-normal temperature or core temperature greater than 36�C antibiotics for uti no alcohol buy generic azithrocin 250mg online, earlier than trying to decide brain dying antibiotics for sinus infection pregnancy order azithrocin 250mg on line. Patients should have normal blood strain, outlined as systolic blood pressure equal to or higher than 100 mm Hg, as the neurologic examination is usually dependable at this degree of blood stress. Irreversibility from neurologic damage is recognized by the extent of the damage, the devastation in neurologic findings, and the dearth of enchancment. Determination of Brain Death the most typical causes of mind demise within the adult population are traumatic mind injury, aneurysmal subarachnoid hemorrhage, hypoxic-ischemic damage, and fulminant hepatic failure. Therefore the clinical analysis, when contemplating accepted guidelines, is the most unequivocal in neurology. In general, most jurisdictions require that the determination of brain demise be made by a licensed physician, which in most of the instances should be an attending physician who has expertise within the assessment of comatose patients and the legal necessities 1002 Pa rt 6 Neurologic Disease within the Critically Ill the foramen magnum. This is easily achieved by introducing noxious stimulation by way of pathways mediated by cranial nerves. When doubtful, the neurologic examination of a comatose patient turns into equivocal, and in these circumstances, extra observation or a confirmatory check may be warranted. Absence of Brainstem Reflexes All segments of the brainstem ought to be examined in the scientific examination. Constricted pupils might imply drug intoxication or lesions at the stage of the pons inflicting de-efferentation from sympathetic fibers and unopposed activation of parasympathetic centers situated in the rostral area of the midbrain (EdingerWestphal nucleus). The oculocephalic reflex is examined by briskly rotating the top aspect to side and vertically. Vertical oculocephalic movements are important for the dedication of mind death as injuries in the lateral portions of the pons may manifest with bilateral palsies of horizontal eye movements however would spare the vertical eye actions. The oculovestibular or cold-caloric reflex is tested by irrigating every ear with 50 mL of iced water and observing the response for as much as 1 minute. The tracheal reflex (cranial nerve X) is tested by analyzing the cough response to tracheal stimulation provided by suctioning. Additional cranial nerve reflexes such because the "jaw jerk" (cranial nerve V) may be assessed for completeness and to observe established tips. Deviations from accepted guidelines during clinical examination of comatose sufferers presumed to be mind dead could also be related to false-positive results, so a radical examination of all segments of the brainstem is required. The patient had a bilateral transtentorial uncal herniation (double arrow, for right-sided uncus); note that the horn of the best lateral ventricle has been pushed toward the midline. The scientific differentiation of motor responses might require expertise and particular training in neurology or neurosurgery. More complex movements which were referred to as mind death�associated reflexes (Lazarus sign, spinal man, spinal reflexes, or spinal automatisms) have been described in patients who in any other case meet all other mind dying criteria. Poor compliance occurred mainly during testing of ache above the foramen magnum and the jaw jerk, as nicely as documenting absence of spontaneous respirations in mind death examination. If the affected person stays hemodynamically secure and with oxygen saturation more than 95%, the patient is disconnected from the ventilator and oxygenation is preserved by putting a catheter through the endotracheal tube and near the extent of the carina delivering O2 at 1. During the next eight to 10 minutes, the practitioner ought to look rigorously for respiratory movements (abdominal or chest excursions and may embody a short gasp). If this is the case, the test can be repeated later using a T-piece, steady positive airway strain with 10 cm H2O, and O2 with 1. Potential problems during apnea take a look at embrace hemodynamic decompensation, hypoxia and hypercarbia, and rigidity pneumothorax. Pitfalls within the analysis of brain death could additionally be related to circumstances involving interference with the suitable medical diagnosis of mind dying such as sufferers with (1) facial trauma (inability to appropriately examine cranial nerve responses or to elicit sensory/motor responses from stimulation above the level of the foramen magnum), (2) preexisting pupillary abnormalities, (3) toxic ranges of anesthetics, sedatives, tricyclic antidepressants, anticholinergics, antiepileptics, or neuromuscular blocking brokers, and (4) severe chronic respiratory acidosis (chronic obstructive pulmonary illness, severe weight problems, or sleep apnea syndrome). Confirmatory Testing the role of confirmatory testing in mind demise differs amongst jurisdictions. The essential level about confirmatory testing is that these tests ought to by no means exchange the scientific examination and may never be ordered earlier than makes an attempt to complete a thorough neurologic examination. Origins of Confirmatory Testing in Brain Death In the earlier years of refining the medical image of mind death, there was a desire to show absence of mind perform with info completely different from scientific knowledge. Families must be informed in regards to the unlikely event of meaningful restoration and in these circumstances, if the patient is a candidate for organ donation, donation after circulatory Rappaport et al. If neither of those options is current, the supplier should wait at least one other 24 hours earlier than a second reassessment. A recent study confirmed that prognostication after cardiac arrest occurs on the premise of inadequate medical data, which can lead to early withdrawals on the premise of self-fulfilling prophecies of doom. The establishment of a known cause and presence of coma, the absence of brainstem reflexes, and apnea help the analysis of brain demise. Most jurisdictions require that the dedication of brain demise be made by a licensed doctor, which generally ought to be an attending physician who has experience within the assessment of comatose patients and the legal requirements applicable to the jurisdiction of follow. When unsure, an additional period of statement or a confirmatory test must be carried out to help the dedication of mind demise. Key Points � the medical examination of brain useless sufferers is probably the most unequivocal in neurology. Prognostication in comatose survivors of cardiac arrest: An advisory statement from the European Resuscitation Council and the European Society of Intensive Care Medicine. Evidence-based guideline replace: figuring out mind dying in adults: report of the Quality Standards Subcommittee of the American Academy of Neurology. Evidence-based guideline replace: determining mind death in adults: Report of the Quality Standards Subcommittee of the American Academy of Neurology. Ad Hoc Committee of the Harvard Medical School to Examine the Definition of Brain Death. Statement issued by the honorary secretary of the Conference of Medical Royal Colleges and their Faculties in the United Kingdom on eleven October 1976. Practice parameter: Prediction of outcome in comatose survivors after cardiopulmonary resuscitation (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Brain dying worldwide: accepted reality but no international consensus in diagnostic standards. Efficacy of a T-piece system and a continuous constructive airway pressure system for apnea testing in the prognosis of brain death. Apnea testing during brain demise evaluation: a evaluate of clinical apply and published literature. Diagnostique electro-sous-cortico-graphique de la mort du systeme nerveux central au cours de sure comas. Usefulness of venous oxygen saturation in the jugular bulb for the diagnosis of brain demise: report of 118 sufferers. Brief evaluation: the position of ancillary tests within the neurological determination of death. Estimated supply of organ donors after circulatory dedication of dying: a population-based cohort research. Hypothermia for neuroprotection after cardiac arrest: systematic evaluation and individual patient information meta-analysis. Outcome following postanoxic status epilepticus in sufferers with targeted temperature management after cardiac arrest. Extracorporeal membrane oxygenation to support cardiopulmonary resuscitation in adults. The challenges with mind demise willpower in adult sufferers on extracorporeal membrane oxygenation.
Azithrocin: 500 mg, 250 mg, 100 mg
Order 250mg azithrocinAcute left ventricular dysfunction during unsuccessful weaning from mechanical ventilation antibiotic x 14547a 500mg azithrocin amex. A prospective research of indexes predicting the outcome of trials of weaning from mechanical air flow antibiotics long term effects buy azithrocin 250mg with visa. Evidence-based pointers for weaning and discontinuing ventilatory help: a collective task 26 virus vih cheap azithrocin 100mg with amex. External work output and force technology during synchronized intermittent mechanical ventilation antibiotics for nasal sinus infection buy azithrocin 250mg amex. Regulation of inspiratory neuromuscular output throughout synchronized intermittent mechanical air flow. Effect of mechanical ventilator weaning protocols on respiratory outcomes in infants and children: a randomized controlled trial. A prospective, managed trial of a protocol-based technique to discontinue mechanical air flow. A randomized, controlled trial of protocol-directed versus physician-directed weaning from mechanical ventilation. Protocol weaning of mechanical air flow in medical and surgical sufferers by respiratory care practitioners and nurses: effect on weaning time and incidence of ventilator-associated pneumonia. A randomized, controlled trial of the function of weaning predictors in clinical choice making. Pressure-time product throughout steady optimistic airway strain, pressure assist air flow, and T-piece throughout weaning from mechanical air flow. He required intubation and mechanical air flow and was given intravenous broad-spectrum antibiotics and steroids. Direct measurements of labor of respiration present that weaningfailure patients consistently make higher, not weaker, inspiratory efforts than do weaning-success patients. Given this, clinicians should all the time additionally think of cardiac efficiency as a possible contributor to weaning failure. Weaning trials should be carried out several occasions per day, as opposed to one, as proof supports earlier liberation from the mechanical ventilator. Weaning with intermittent necessary ventilation has constantly been proved to be an inferior methodology. Breathing trials performed as quickly as per day are equally as efficient as multiple trials per day. Rather, causes for failure should be sought and corrected, and one other breathing trial ought to be carried out, understanding the literature helps this. Patients who require reintubation have larger severity of sickness scores, are older, and have an extended period of mechanical air flow than successfully extubated sufferers. Reintubated patients have a a lot higher mortality price than successfully extubated sufferers. Excessive secretions (16%�28% of reintubations) and inability to tolerate an additional respiratory load (28%�37% of reintubations) are the most typical causes of reintubation. Which of the next is true regarding weaning predictor checks and weaning trials Weaning trials performed as part of a protocol have constantly proven benefit by decreasing mechanical ventilator days. This means that a big barrier to extubation is lack of clinician recognition of readiness to wean. The utility of low levels of help can markedly scale back work of respiratory and overcome resistance. Although commonplace, protocolized weaning has not been shown to improve outcome above and beyond ordinary care. Reasons for failure must be sought and corrected, and the affected person ought to be noticed by the treating clinician during a weaning trial; liberation from the ventilator should be custom-made to the individual patient. The proportion of sufferers with pulmonary emboli was considerably lower with dalteparin (24 sufferers, 1. In addition, patient-related factors might embrace genetic and bought thrombophilia and hormone substitute therapy and oral contraceptive remedy. Deep Venous Thrombosis It is estimated that as many as 95% of clinically important pulmonary emboli originate from the deep veins of the decrease extremity. The proximal deep veins of the leg are the most typical sites of origin of clots that embolize to the pulmonary circulation. The thrombi kind within the valve pockets of calf veins and extend to the proximal veins. In roughly 50% of sufferers, venous outflow obstruction decreases within 3 months by lysis and recanalization. Clots that proceed to propagate have a higher risk to break apart and lead to embolization. The strongest risk factors had been hip and leg fractures, main common surgery, hip or knee replacement, major trauma, and spinal wire damage. Factor V Leiden mutation is current in up to 5% of the traditional population and is the commonest cause of familial thromboembolism. The time period main pulmonary thromboembolism has been used to describe any pulmonary thromboembolus that ends in a hemodynamically important occasion. TxA2 is produced by endothelial cells, and even in higher portions by platelets in response to platelet aggregation. The functional status of the cardiopulmonary system is essential within the initial hemodynamic presentation and is a significant determinant of short- and long-term outcome. Ventilation-perfusion mismatch and low mixed venous oxygen levels are the prevalent causes of hypoxemia. Endothelial damage could outcome from hypoxic publicity and additional lead to pulmonary vasoconstriction. Only 58 sufferers (3%) had systolic blood pressures of 90 mm Hg or lower on presentation. Sudden unexplained onset of dyspnea was the commonest symptom and was present in 80% of the sufferers. Tachypnea and tachycardia had been present in 88% and 63% of the sufferers, respectively. Accentuated second heart sound was noted in 67%, and S3 or S4 gallop was current in 47%. Retrosternal nonpleuritic chest pain might mimic the ache skilled with a myocardial infarction and characterize demand ischemia of the right ventricle. If pulmonary infarction happens as the end result of distal embolization, then hemoptysis may happen. In addition, sufferers appear weak, pale, diaphoretic, oliguric, and develop altered mental standing. The patient could additionally be hypoxemic and require high-flow oxygen or pressing intubation and mechanical air flow. History and bodily examination in acute pulmonary embolism in sufferers with out pre-existing cardiac or pulmonary illness. An increase in minute ventilation, useless space, or a rise in supplemental oxygen could also be clues to an embolic occasion.
Syndromes - Muscle soreness
- Heart defibrillator or pacemaker
- Discomfort
- Blood clots that form in the device
- Loss of appetite
- Putting ice over the painful area two to four times a day, and after activities
- Bladder filling
- Acts out social encounters through play activities
- Angiomyolipoma, a noncancerous tumor
Cheap azithrocin 250 mg overnight deliveryShould the electrocardiogram be used to guide remedy for sufferers with left bundle-branch block and suspected myocardial infarction Utility of left bundle branch block as a diagnostic criterion for acute myocardial infarction antibiotic names medicine order 250 mg azithrocin with visa. Prevalence of acute myocardial infarction in patients with presumably new left bundle branch block antibiotics nausea cure generic 100 mg azithrocin fast delivery. Electrocardiographic diagnosis of evolving acute myocardial infarction within the presence of left bundle-branch block antibiotics for uti staph generic azithrocin 100 mg without prescription. Indications for fibrinolytic remedy in suspected acute myocardial infarction: Collaborative overview of early mortality and main morbidity outcomes from all randomised trials of greater than one thousand sufferers treatment for dogs coughing and gagging purchase 100 mg azithrocin free shipping. Comparison of the prognostic effect of left versus right versus no bundle branch block on presenting electrocardiogram in acute myocardial infarction sufferers treated with primary angioplasty within the major angioplasty in myocardial infarction trials. Treatment and outcomes of left bundle-branch block sufferers with myocardial infarction who current with out chest ache. Appearance of abnormal Q waves early in the midst of acute myocardial infarction: implications for efficacy of thrombolytic remedy. Electrocardiographic prognosis of acute myocardial infarction: current concepts for the clinician. Clinical worth of 12-lead electrocardiogram after profitable reperfusion remedy for acute myocardial infarction. Prognostic worth of cardiac troponin in sufferers with chronic kidney illness with out suspected acute coronary syndrome. Cardiac troponin I elevation in acute pulmonary embolism is associated with proper ventricular dysfunction. Importance of cardiac troponins I and T in risk stratification of patients with acute pulmonary embolism. Clinical usefulness and prognostic value of elevated cardiac troponin I ranges in acute pulmonary embolism. Heart failure and demise after myocardial infarction locally: the rising function of mitral regurgitation. A community-wide evaluation of the utilization of pulmonary artery catheters in patients with acute myocardial infarction. Outcome of sufferers sustaining acute ischemic mitral regurgitation during myocardial infarction. Early revascularisation and 1-year survival in 14-day survivors of acute myocardial infarction: a potential cohort study. Beneficial effects of instant stenting after thrombolysis in acute myocardial infarction. Randomized comparability of percutaneous transluminal coronary angioplasty and medical remedy in secure survivors of acute myocardial infarction with single vessel illness: a examine of the Arbeitsgemeinschaft Leitende Kardiologische Krankenhausarzte. Effect of supersaturated oxygen delivery on infarct dimension after percutaneous coronary intervention in acute myocardial infarction. Cardiovascular safety of non-steroidal anti-inflammatory drugs: network meta-analysis. Long-term cardiovascular danger of nonsteroidal anti-inflammatory drug use in accordance with time passed after first-time myocardial infarction. Inhibition of clinical advantages of aspirin on first myocardial infarction by nonsteroidal anti-inflammatory medicine. Nitroglycerin-induced severe hypotension and bradycardia in patients with acute myocardial infarction. Intravenous nitroglycerin remedy to limit myocardial infarct size, growth, and complications. Effects of lisinopril and transdermal glyceryl trinitrate singly and collectively on 6-week mortality and ventricular operate after acute myocardial infarction. A randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58,050 patients with suspected acute myocardial infarction. Comparison between the consequences of nitroprusside and nitroglycerin on ischemic damage during acute myocardial infarction. Effect of short-term infusion of sodium nitroprusside on mortality price in acute ninety six. Consequences of reocclusion after profitable reperfusion remedy in acute myocardial infarction. Left ventricular perform at three months after successful thrombolysis: impact of reocclusion without reinfarction on ejection fraction, regional operate, and remodeling. Long-term implications of reocclusion on left ventricular size and function after successful thrombolysis for first anterior myocardial infarction. Effects of aspirin on coronary reocclusion and recurrent ischemia after thrombolysis: a meta-analysis. Aspirin versus Coumadin in the prevention of reocclusion and recurrent ischemia after successful thrombolysis: a potential placebo managed angiographic research. Addition of clopidogrel to aspirin, in forty five,852 patients with acute myocardial infarction: randomised placebo controlled trial. Embolic potential, prevention and management of mural thrombus complicating anterior myocardial infarction: a meta-analysis. Comparison of frequency of left ventricular thrombi in patients with anterior wall versus nonanterior wall acute myocardial infarction handled with antithrombotic and antiplatelet therapy with or without coronary revascularization. Left ventricular thrombus in anterior acute myocardial infarction after thrombolysis. Incidence and pure history of left ventricular thrombus following anterior wall acute myocardial infarction. Comparison of high-dose with low-dose subcutaneous heparin to forestall left ventricular mural thrombosis in patients with acute transmural anterior myocardial infarction. A comparability between heparin, and low-dose aspirin as adjunctive remedy with tissue plasminogen activator for acute myocardial infarction. Aspirin, heparin, and fibrinolytic remedy in suspected acute myocardial infarction. A factorial randomised trial of alteplase versus streptokinase and heparin versus no heparin among 12,490 sufferers with acute myocardial infarction. In-hospital mortality and medical course of 20,891 patients with suspected acute myocardial infarction randomised between alteplase and streptokinase with or with out heparin. A randomised comparison of streptokinase vs tissue plasminogen activator vs anistreplase and of aspirin plus heparin vs aspirin alone among 41,299 cases of suspected acute myocardial infarction. Overview of randomized trials of intravenous heparin in patients with acute myocardial infarction handled with thrombolytic remedy. Angiographic and clinical outcomes in sufferers receiving low-molecular-weight 132. Impact of bivalirudin remedy in high-risk patients with acute myocardial infarction. Heparin-induced thrombocytopenia in patients handled with low-molecular-weight heparin or unfractionated heparin. Prevalence of whole coronary occlusion through the early hours of transmural myocardial infarction. Ten-year follow-up of the first megatrial testing thrombolytic therapy in sufferers with acute myocardial infarction.
Buy cheap azithrocin 100mg onlineThe mechanically ventilated rabbit shows several areas of disrupted myofibrils (short thick arrows) virus xbox one azithrocin 100mg cheap, the mitochondria are swollen (long thick arrow) and have irregular cristae antibiotic definition discount azithrocin 500mg without prescription, and the intermyofibril area accommodates lipid droplets (long thin arrow) antibiotics for acne in pregnancy azithrocin 250mg overnight delivery, indicating decreased lipid uptake by the mitochondria bacterial infection symptoms purchase 100 mg azithrocin free shipping. Prolonged mechanical air flow was associated with reduction in myofiber cross-sectional space. D, Number of days of mechanical air flow; H, number of hours of mechanical air flow. Rapidly progressive diaphragmatic weak point and injury during mechanical air flow in humans. Of concern, nevertheless, is the report that administration of the antioxidant N-acetylcysteine to critically sick patients with severe sepsis worsened sepsis-induced organ failure. Unfortunately, when progress hormone has been administered to sufferers requiring extended mechanical air flow, the period of mechanical ventilation was not decreased nor was muscle energy increased. No distinction was famous between the muscle fibers of the 2 teams of patients with respect to cross-sectional area, most drive per unit area, calcium sensitivity of force generation, and price constant of redevelopment of drive. The muscular tissues of the sufferers had decrease contractile pressure, and will increase in inducible nitric oxide synthase expression (messenger ribonucleic acid and protein) and activity. Immunohistochemical studies revealed the generation of peroxynitrite (a extremely reactive oxidant formed by the reaction of nitric oxide with superoxide anion). Exposure of management muscles to the quantity of peroxynitrite present in sufferers brought on an irreversible lower in force era. These information recommend that sepsis decreases muscle force through the manufacturing of nitric oxide and its toxic by-products. Production of nitric oxide in sepsis could additionally be protective and never solely deleterious. This finding contrasts with the statement that nitric oxide synthase inhibitors stop muscle dysfunction in septic rats. B, A sample of gastrocnemius muscle obtained from a rat injected 12 hours earlier with regular saline solution. The strip was stimulated for 3 minutes (50 Hz, 300-msec duration) and then immersed for 90 minutes in Krebs resolution containing a fluorescent probe, Procion orange 14 (0. Critical illness polyneuropathy has been thought of one of the manifestations of multiple-organ failure syndrome. Animal models of important illness myopathy suggest that medical denervation with paralytic brokers trigger an upregulation of glucocorticoid receptors within the muscle. In the previous few years it has turn out to be more and more obvious that important illness neuropathy and myopathy often coexist. After phrenic nerve stimulation, muscle depolarization produces compound motor motion potentials that are adopted by the equivalent falls in airway stress (dashed line) and esophageal strain (solid line). A paper on the tempo of recovery from diaphragmatic fatigue and its sudden dividends. Approximately 50% to 60% of sufferers experience full restoration (ability to breathe spontaneously and to walk independently) over a interval of two weeks to 6 months or longer. Until lately, there was little doubt that metabolic acidosis may decrease muscle contractility. They noticed a fall in maximal diaphragm power with respiratory acidosis (-18%, P < 0. In contrast to what could be anticipated if acidosis brought on lower in contractility, Degroot et al. There are contrasting reviews on the effect of acute respiratory acidosis on respiratory muscle contractility. The myelin surrounding the disintegrating axons collapses around the axonal particles to form ovoids of myelin (seen higher on the lateral parts of A). B, Amid muscle fibers that are normal in measurement and shape are atrophic ones that seem small and which have developed contours with acute angles. These findings are consistent with denervation atrophy secondary to axonal degeneration, so-called crucial sickness polyneuropathy. Some investigators report no change in diaphragmatic contractility151,153 (but lower in drive of the adductor pollicis)151 when acute respiratory acidosis causes a decrease in pH to about 7. A single myosin heavy chain isoform is usually expressed inside an adult skeletal muscle fiber. Slower velocity of relaxation permits fusion of repetitive twitches at decrease frequencies of stimulation as in contrast with quick relaxations. Compared with the traditional construction, the affected person developed in depth lack of thick (myosin) myofilaments and relative preservation of skinny (actin) filaments. M, M-line fashioned by myosin filaments and M-line proteins; Z, Z-disk shaped by a lattice of filaments that be a part of the actin filaments of one sarcomere with the actin filaments of the adjacent sarcomere. Myopathy with thick filament (myosin) loss following prolonged paralysis with vecuronium throughout steroid treatment. For a given Edi throughout hypercapnia, the stress output of the diaphragm was decreased. Respiratory muscle operate could additionally be impaired by decreased levels of phosphate,159 calcium,160 magnesium,161 and potassium. Correction of hypophosphatemia was accompanied by a big enhance in twitch Pdi-from 9. Changes in serum phosphorus focus and modifications in twitch Pdi had been nicely correlated (r = 0. These results strongly recommend that hypophosphatemia can impair the contractile properties of the diaphragm throughout acute respiratory failure. The same investigators assessed the effects of hypocalcemia on diaphragmatic function in 12 anesthetized canine. Over the two hours of remark, a progressive discount in diaphragmatic drive production paralleled the progressive discount in ionized serum calcium. Severe hypokalemia may be brought on by a quantity of issues, together with posthypercapnic alkalosis, 163 renal tubular acidosis, primary hyperaldosteronism, gastrointestinal potassium losses, use of diuretics, thyrotoxic periodic paralysis, familial hypokalemic paralysis, 2-adrenergic agonists, and licorice ingestion. Hypokalemiaassociated respiratory muscle weakness can outcome in respiratory failure and demise. This incapability to maintain adequate ventilation is attributable to insufficient oxygen delivery to the respiratory muscle tissue. Compared with nonventilated patients, ventilated patients have been weaned from an intraaortic balloon pump extra often, and their survival was greater. Hemodynamic situations much less excessive than shock, which could nonetheless have an result on respiratory muscle performance, are failed makes an attempt of spontaneous respiration throughout weaning from mechanical air flow. Immediately earlier than the trial, mixed oxygen venous saturation was not different between the 2 teams. Although the calculated oxygen demand was similar within the two teams, the manner by which it was met differed.
Buy generic azithrocin 500 mgTonic seizures are episodes of tonic extension of the arms treatment for dogs with gastroenteritis azithrocin 500 mg on-line, legs antibiotics yeast infection prevention purchase 250 mg azithrocin, and trunk; they have to be distinguished from extensor posturing and from tetanic spasms antibiotic resistance pbs buy 250 mg azithrocin. They may start as generalized or treating dogs for dry skin discount azithrocin 250mg otc, more commonly, occur because the manifestation of unfold of a focal seizure (focal to bilateral tonic-clonic). Without impairment of consciousness (aura continua, with autonomic, sensory, visible, olfactory, gustatory, emotional/ psychic/experiential, or auditory symptoms) b. Although the endogenous ligands of these channels are glutamate and aspartate, the channels are named for artificial compounds that potently activate them. Multiple neurobiochemical modifications occur that contribute to the refractoriness of seizures. The most important change is probably the elevation of the extracellular potassium focus. Patients with cerebral edema, glial scarring, 1034 Pa rt 6 Neurologic Disease within the Critically Ill or alien tissue lesions have extracellular space abnormalities that impair the potassium buffering capability of glial cells. To meet this demand, cerebral blood move initially increases threefold or higher. This accentuates the demand for local catabolism to assist ion pumps (in a vain attempt to restore the internal milieu in the course of the flood of sodium and calcium). When focal seizures generalize, subcortical structures start to play an lively function in the medical phenomena observed. Spread of the electrical activity into the substantia nigra and other subcortical areas appears to be necessary before a tonic-clonic convulsion happens. The hippocampus, which is likely one of the most important areas for reminiscence function, contains the most susceptible neurons, but the cerebral cortex can additionally be vulnerable. Epinephrine and cortisol release prompts additional elevations of systemic arterial pressure and also produces hyperglycemia. Respiration turns into ineffective; both airway obstruction and diaphragmatic contraction impede air motion. Ventilatory failure impairs carbon dioxide excretion whereas carbon dioxide manufacturing will increase markedly, including a respiratory element to the acidosis. Core temperature may continue to climb, however, probably reflecting hypothalamic dysfunction. The initial hyperglycemia diminishes; after an hour or more, hepatic gluconeogenesis might fail, and hypoglycemia develops. Aspiration of oral or gastric contents generally produces chemical pneumonitis, with bacterial pneumonia often following. Although clonic motor exercise in these patients stays visible, it could be tough to determine whether or not a subsequent further decline in alertness reflects a seizure or some other process. Thus any affected person who manifests these findings and who has a possible purpose for seizures. Many kinds of abnormal actions occur in patients with extreme metabolic disturbances or anoxic brain injury. During therapeutic cooling for sufferers in a coma after cardiac arrest, seizures may be difficult to detect clinically, especially when neuromuscular junction blockade is used. Consciousness is straight away lost, and after several seconds the tonic phase offers method to clonic (rhythmic) extension of the extremities, with flexion occurring throughout each transient leisure. Although clonic motor activity is essentially the most easily recognized form, the seizure will take on the practical characteristics of the adjacent functional tissue. This could, sadly, result in both diagnostic obscuration and iatrogenic issues. Beyond attempting to defend the affected person from hurt, little or no may be done with enough rapidity to influence the course of the seizure. This is the most effective time to collect proof of a focal onset, which implies structural brain disease. The postictal examination is similarly useful; language, motor, sensory, or reflex abnormalities after an apparently generalized convulsion also needs to be considered as proof of focal illness. A complete record of potentially epileptogenic medicine is beyond the scope of this chapter; the medicines of any affected person who has a seizures ought to be reviewed with this risk in mind. Although ethanol withdrawal is the most typical offender, discontinuing any hypnosedative agent. The bodily examination should be carried out with special emphasis on the factors mentioned earlier for the postictal examination. In addition, evidence of heart problems (as a source for cerebral emboli) and systemic an infection ought to be sought. In addition to routine biochemical research, screening for drugs of abuse must be performed on patients with unexplained seizures. Cocaine has emerged as a prominent reason for seizures in many city hospitals44 and newer proconvulsant artificial substances should still be suspected within the presence of unfavorable outcomes of a toxicology display. Hyperparathyroidism has been linked anecdotally to seizures, with the inference that parathormone is neurotoxic. Similarly, hypomagnesemia has an unwarranted popularity as a cause of seizures, particularly in the malnourished alcoholic affected person. In particular, phases of the electrographic development could also be sufficiently temporary to be overlooked. Partially treating status epilepticus may dissociate the medical and electrographic features. The preliminary high-frequency discharge becomes progressively much less nicely fashioned over minutes; this pattern implies that neuronal activity is less synchronous. Such a patient may need prophylaxis against delirium tremens with benzodiazepines, however the seizures themselves seldom require treatment. It is now apparent that initiating antiseizure drug remedy after the primary unprovoked. Although the standard objective of chronic antiseizure drug treatment is to administer the smallest dose of a tolerated single agent that utterly controls seizures, such an method is commonly impossible in the important care environment. Calculations of the unbound concentration primarily based on the serum albumin concentration are unreliable. Hepatic dysfunction will mandate a lower within the upkeep dose; if the serum albumin may be very low, the loading dose could be lowered as well. This allergy may be manifested solely as fever, but more commonly it includes a rash and eosinophilia. The first panel illustrates the onset of the seizure; the following panels show its evolution. Montage: longitudinal bipolar; channels 1 to four, left temporal; and channels 5 to 8, left parasagittal. Valproate must be avoided in settings by which liver illness or hyperammonemia may be problematic but is in any other case a helpful drug out there each orally and intravenously.

100 mg azithrocin otcSevere hyperphosphatemia and hypocalcemia following the rectal administration of a phosphate-containing Fleet pediatric enema bacterial nucleoid cheap azithrocin 250mg without prescription. Identifying risk components for development to crucial care admission and death amongst individuals with acute pancreatitis: a record linkage analysis of Scottish healthcare databases bacteria description buy azithrocin 100 mg with amex. Hypocalcemia in sufferers with acute pancreatitis: a putative function for systemic endotoxin publicity infection 3 english patch 250mg azithrocin free shipping. Soft tissue calcium and magnesium content in acute pancreatitis in the dog: calcium accumulation antimicrobial effect of chlorhexidine gluconate order azithrocin 250mg free shipping, a mechanism for hypocalcemia in acute pancreatitis. Depression of serum calcium by elevated plasma free fatty acids within the rat: a mechanism for hypocalcemia in acute pancreatitis. Intraperitoneal free fatty acids induce extreme hypocalcemia in rats: a model for the hypocalcemia of pancreatitis. Functional magnesium deficiency in critically ill sufferers identified using a magnesium-loading take a look at. Is plasma calcium concentration implicated in the development of critical sickness polyneuropathy and myopathy Parathyroid hormone and parathyroid hormone-related protein in the investigation of hypercalcaemia in two hospital populations. Parathyroid hormone-related protein, bone metastases and hypercalcaemia of malignancy. Hypercalcemia related to elevated serum calcitriol ranges in three patients with lymphoma. Calcitriol manufacturing in hypercalcemic and normocalcemic sufferers with non-Hodgkin lymphoma. Case report: delayed hypercalcemia after rhabdomyolysis-induced acute renal failure. The pathophysiology of altered calcium metabolism in rhabdomyolysis-induced acute renal failure. Interactions of parathyroid hormone, 25-hydroxycholecalciferol, and 1,25-dihydroxycholecalciferol. Successful remedy of immobilization hypercalcemia utilizing calcitonin and etidronate. Ventricular fibrillation in hypercalcaemic disaster because of main hyperparathyroidism. Calcium free hemodialysis: expertise within the therapy of 33 sufferers with extreme hypercalcemia. Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: a pooled analysis of two randomized, managed clinical trials. Physiological and pathophysiological position of magnesium within the cardiovascular system: implications in hypertension. Effects of dietary vitamin D on magnesium absorption and bone mineral contents in pigs on regular magnesium intakes. Hypomagnesemia in critically unwell cancer sufferers: a potential research of predictive components. Proton pump inhibitors and hypomagnesemia within the common inhabitants: a population-based cohort study. Proton-pump inhibitor-induced hypomagnesemia: Current analysis and proposed mechanisms. High incidence of hypophosphatemia in surgical intensive care patients: efficacy of phosphorus therapy on myocardial function. Pathophysiologic and clinical correlates of hypophosphatemia and the connection with sepsis and consequence in postoperative sufferers after hepatectomy. Hypophosphatemia induced by mechanical ventilation in patients with chronic obstructive pulmonary disease. Severe hypophosphatemia throughout hematopoietic reconstitution after allogeneic peripheral blood stem cell transplantation. A new graduated dosing routine for phosphorus replacement in patients receiving nutrition support. Fatal hyperphosphatemia following Fleet Phospho-Soda in a affected person with colonic ileus. Hyperphosphatemic hypocalcemic coma caused by hypertonic sodium phosphate (fleet) enema intoxication. Spurious hyperphosphatemia as a result of sample contamination with heparinized saline from an indwelling catheter. Metastatic calcification of the cardiac conduction system with heart block: an under-reported entity in persistent renal failure sufferers. Which of the next statements regarding the remedy of lactic acidosis with sodium bicarbonate is most accurate Treatment of lactic acidosis with sodium bicarbonate will trigger a rise in carbon dioxide era, which may lower intracellular pH. By raising extracellular pH, bicarbonate administration will scale back ionized calcium (answer a incorrect). By inflicting systemic alkalinization, bicarbonate administration is more doubtless to cause a rise in lactate technology rate (answer d incorrect). The affected person was admitted with sepsis from a urinary supply and has been intubated and receiving pressors (norepinephrine and dopamine) for the past 3 days. On examination his vital signs are within normal limits and he appears to be comfy and in no distress. Urinary electrolytes include the following: urinary sodium 87 mEq/L, urinary potassium 35 mEq/L, and urinary chloride one hundred ten mEq/L. Which of the following is the most probably explanation for the elevated potassium stage There are varied causes for hyperkalemia in critically sick sufferers, including excessive potassium load, translocation of potassium across mobile membrane, and incapability to eliminate excess stability. Pseudohyperkalemia is the more than likely explanation due to normal laboratory findings the day earlier than without change in scientific status. Pseudohyperkalemia has a number of possible causes, including hemolysis and fist clenching with a tourniquet in place throughout phlebotomy (answer d correct). A 3% sodium chloride (NaCl) infusion is began at eighty mL/h and after 6 hours the sodium degree is 122 mmol/L. Stop the 3% NaCl, begin 5% dextrose in water (D5W) and desmopressin to decrease the sodium level. Patients with acute symptomatic hyponatremia have to be treated with an infusion of 3% saline resolution to quickly improve the plasma sodium focus and stop cerebral edema. The sodium aim is 6 mmol/L in the first 24 hours as a more fast rise is unnecessary and can induce osmotic demyelination syndrome.
Buy 100 mg azithrocin visaCompeting threat of cardiac standing and renal function during hospitalization for acute decompensated coronary heart failure virus removal tool kaspersky buy generic azithrocin 100mg line. It is cleared from the serum by the kidneys virus ny cheap 250 mg azithrocin overnight delivery, so ranges are larger in patients with coexisting renal disease antibiotics yellow urine 100mg azithrocin free shipping. Most latest knowledge from the United States within the Medicare inhabitants present a 1-year mortality of 29 polysorbate 80 antimicrobial azithrocin 100 mg on line. In the groups with essentially the most severe chronic coronary heart failure-patients awaiting cardiac transplantation-1-year mortality was 75% with 2-year mortality of 92%. Hospital mortality stays 40% to 50% even with aggressive supportive remedy and emergency revascularization methods. Several clinical factors have been shown to identify patients with a poorer prognosis. Hypothetical mechanisms of troponin launch in continual heart failure include ischemia, cytokine activation, oxidative stress, and apoptosis. The capability of troponin elevation to predict mortality additionally was impartial of different variables and was true even in sufferers with nonischemic etiologies of heart failure. Kidney illness aggravates the tendency to volume overload and coronary heart failure decompensation, and coronary heart failure often worsens renal operate. A meta-analysis of 16 giant studies of coronary heart failure patients revealed that 29% of coronary heart failure patients had average to severe impairment of renal operate. Any degree of renal impairment had an roughly 50% increased relative mortality danger. It is the cause of greater than 1 million hospitalizations yearly within the United States. It is defined as either the model new onset of sudden, extreme heart failure symptoms or a gradual worsening of a continual coronary heart failure syndrome that has progressed in severity to require urgent and intensive therapy. Although in-hospital mortality and size of stay have been lowered, the prognosis remains poor, with 30% mortality at 1 yr after hospitalization and 50% mortality at 5 years. This prognosis is affected by the high incidence of significant comorbid circumstances as nicely as end-organ issues, including renal dysfunction, hepatic congestion, and thromboembolic circumstances. Acute coronary heart failure requires urgent and simultaneous initiation of diagnostic testing and therapeutic interventions. Several completely different schemes are used to classify acute coronary heart failure; these allow the clinician to assess the etiology and optimize preliminary diagnostic and therapeutic methods. Blood stress on presentation can typically quickly differentiate the etiology, as acute heart failure with hypertension is taken into account a hypertensive emergency, mandating pressing blood pressure reducing. Acute heart failure with normal blood pressures suggests coronary artery disease as an etiology. Hypotension might indicate cardiogenic shock or advanced extreme chronic coronary heart failure. Another strategy to the initial evaluation is to evaluate for the chance of acute coronary ischemia as the etiology of acute coronary heart failure to assess the necessity for and timing of revascularization methods. Acute worsening or decompensation of continual heart failure signs, both within the setting of identified continual cardiovascular sickness or de novo. This is the most common presentation of acute heart failure requiring admission to hospital, occurring in approximately 70% of sufferers with acute heart failure. Acute pulmonary edema related to elevated blood pressure, usually within the setting of chronic severe hypertension and chronic kidney disease. Pulmonary edema (syndromes 2 and 3) accounts for roughly 25% of acute coronary heart failure admissions. This is probably the most severe presentation of acute coronary heart failure and is associated with high in-hospital mortality charges. High cardiac output coronary heart failure in the setting of sepsis, hyperthyroidism, or cardiac arrhythmia. This is the least frequent presentation, occurring in a small proportion of sufferers. Acute proper ventricular failure, occurring with acute proper ventricular myocardial infarction, huge pulmonary embolism, or cardiac tamponade. This presentation could also be extra refined, marked by fatigue, dyspnea, hypotension, tachycardia, and signs of systemic venous congestion. Symptoms of acute coronary heart failure include severe shortness of breath, orthopnea, wheezing, and symptoms of hypoxemia including restlessness and confusion. Symptoms of tissue hypoperfusion, similar to fatigue, weak spot, psychological status adjustments, nausea, and anorexia, may be delicate however are important to acknowledge as they may herald impending cardiogenic shock. Physical examination typically reveals pulmonary rales and wheezes, an S3 gallop, and elevation of jugular venous strain. A low cardiac output is reliably predicted by a low "proportional pulse strain," which is calculated by the coronary heart beat stress (systolic blood stress minus diastolic blood pressure) divided by systolic blood strain. Peripheral edema and ascites may indicate concomitant right ventricular failure of longer length. History and doctor examination will not be delicate or specific for the analysis of acute heart failure and is supplemented by urgent laboratory and radiologic testing. Complete blood cell count, electrolytes, renal and liver operate, thyroid profile, and cardiac biomarkers (troponin I or troponin T) are routinely tested. Natriuretic peptide levels help in the diagnosis of coronary heart failure in sufferers presenting with dyspnea, and could be adopted serially to assess effectiveness of remedy. An arterial line is useful in managing sufferers with hypotension or cardiogenic shock. It is crucial to consider left ventricular dimension and function, proper ventricular function, valve operate, and the presence of pericardial effusion. Doppler echocardiography affords assessment of ventricular filling pressures, right ventricular systolic pressure, cardiac output, and the severity of valve lesions. Initial management is focused on offering adequate oxygenation and ventilation, optimizing blood stress, stabilizing cardiac rhythm, treating myocardial ischemia when present, and reversing end-organ dysfunction. Patients with pulmonary edema often require ventilatory help with noninvasive constructive airway pressure air flow or endotracheal intubation. Noninvasive air flow improves oxygenation and pulmonary compliance and decreases work of breathing. No distinction among these therapies was famous within the major endpoint of dying at 7 days or in the secondary endpoint of death plus endotracheal intubation at 7 days. Noninvasive air flow did lead to extra fast improvement in dyspnea, tachycardia, hypercapnia, and acidosis. There are few controlled trial information to arrive at evidence-based tips for the therapy of acute heart failure. Many recommendations are based mostly on small research, expertise, statement, and consensus of opinion. However, an analysis of registry knowledge concluded that use of morphine was related to increased want for endotracheal intubation and better hospital mortality. Intravenous loop diuretics, similar to furosemide, supply rapid and effective symptom aid and are nearly all the time first-line therapy. Intravenous vasodilators are very helpful, especially in patients with extreme hypertension; intravenous nitroglycerin and intravenous nitroprusside are used mostly. A, From the pleural line, one repetition of the pleural line, a horizontal line (A line), parallel to the pleural line, is seen, indicating normal lung with no pulmonary edema.
References - Gonzales-Ulloa M, Castillo A, Stevens E, et al. Preliminary study of the total restoration of the facial skin. Plast Reconstr Surg 1954;13:151.
- Philbin DM, Levine FH, Emerson CW, et al: Plasma vasopressin levels and urinary flow during cardiopulmonary bypass in patients with valvular heart disease: Effect of pulsatile flow, J Thorac Cardiovasc Surg 78:779-783, 1979.
- Bhatia-Gaur R, Donjacour AA, Sciavolini PJ, et al: Roles for Nkx3.1 in prostate development and cancer, Genes Dev 13(8):966n977, 1999.
- World Health Organization. Rapid Implementation of the Xpert MTB/RIF diagnostic test. (WHO/HTM/TB/2011.
- Lue TF: Impotence: a patientis goal directed approach to treatment, World J Urol 8:67n74, 1990.
- Shaheen NJ, Sharma P, Overholt BF, et al: Radiofrequency ablation in Barrett's esophagus with dysplasia. N Engl J Med 360:2277, 2009.
|

