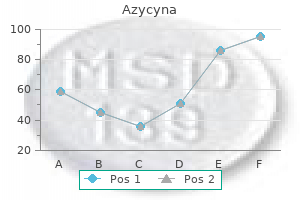
Azycyna
Jennifer M. Kalish, M.D., Ph.D. - The Children’s Hospital of Philadelphia
- Philadelphia, Pennsylvania
Cheap azycyna 250mg on-lineDobutamine stress produces greater increases in international contractility than both treadmill or bicycle stress and discount in cavity quantity is the rule in normal people antimicrobial yoga pant discount azycyna 100mg with mastercard. Cavity dilation is infrequent with dobutamine stress even within the setting of left main illness bacteria lesson plan generic 500mg azycyna otc. False optimistic research may outcome from difficulty in distinguishing ischemic wall movement abnormalities from these produced by tethering of myocardial segments to much less cell constructions such because the mitral annulus antibiotics poop discount azycyna 500mg line. As beforehand talked about antibiotics for sinus infection augmentin purchase azycyna 500mg with amex, dysynchronous contraction produced by left bundle department block and proper ventricular pacing can be confused with septal wall motion abnormalities from ischemia. Suggested guidelines for the suitable use of stress echocardiography had been printed in 2008 (see Suggested Readings). A technical panel of clinician-experts graded varied indications for stress echocardiography based on data from revealed literature. Grades assigned by the professional panel have been used to categorize indications for stress echocardiography as acceptable, uncertain, and inappropriate. Some of the indications considered applicable for stress echocardiography are proven in Table 50-3. Indications where stress echocardiography is presently thought of inappropriate are proven in Table 50-4. The excessive specificity is maintained in topic populations, similar to girls, in whom other noninvasive testing modalities might have the next price of false positives. Potential causes of both false unfavorable and false constructive stress echocardiograms are listed in Table 50-2. When stress echocardiography is being performed for diagnostic functions in a steady affected person, withdrawal of medications that would blunt the guts fee response to stress is really helpful to cut back the frequency of inadequate stress. Laboratories should have protocols in place to rapidly establish appropriate sufferers, carry out distinction injection and imaging, and monitor for any opposed effects. Restrictions in the use of distinction brokers issued in that warning have subsequently been relaxed based mostly on lately published research documenting the protection of distinction brokers. Although some false positive research could result from challenges in wall movement evaluation, a significant proportion of false optimistic studies is as a outcome of of myocardial ischemia in the absence of obstruction of epicardial coronary vessels. Women with atypical signs are a bunch in whom the excessive specificity of stress echocardiography could show helpful. The diagnostic worth of stress echocardiography is taken into account unsure in excessive threat asymptomatic people based mostly on a relative lack of data on this subset of patients. In spite of questions in regards to the utility of stress echocardiography in asymptomatic subjects, a variety of research have shown that stress echocardiography has vital prognostic value in sufferers with diabetes. Serial testing at intervals of lower than or equal to 1 year is taken into account inappropriate (Table 50-4, indication 4) in sufferers with a beforehand irregular stress imaging examine and no or secure signs. The stress echo appropriateness criteria published in 2008 and included in Table 50-3 have been drafted with out the advantage of the 2007 Perioperative Guidelines doc. Stress echocardiography in sufferers with one or more scientific predictors (diabetes mellitus, renal insufficiency, cerebrovascular disease, ischemic coronary heart illness, or history of congestive heart failure) is now thought-about optionally available and reserved for cases where affected person administration may be affected. Patients with ischemia on stress echocardiography could profit essentially the most from perioperative beta-blockade. However, the finding of in depth ischemia (5 segments) on a stress echocardiogram could identify these with triple vessel or left primary disease in whom revascularization could enhance both perioperative and long-term end result. Assessment of Myocardial Viability the utility of stress echocardiography for the evaluation of myocardial viability has been documented in numerous studies. Dobutamine echocardiography is essentially the most commonly used ultrasound modality for assessment of viability. The uncoupling of the inotropic and chronotropic results of dobutamine at low doses (10 g/kg/min) permits improvement of contractile perform in surprised or hibernating myocardium without major increases in heart price and myocardial oxygen demand. In the setting of coronary obstruction, higher doses of dobutamine produce ischemia with worsening of perform in regions that exhibited contractile reserve with low dose dobutamine. The "biphasic response" with enchancment of perform at low doses and worsening of function at larger doses of dobutamine has been proven to have a high positive predictive value for figuring out viable myocardium that may have useful recovery with revascularization. Other inotropic agents and vasodilators, similar to dipyridamole, have been efficiently used as alternatives to dobutamine for assessment of contractile reserve. Contractile reserve, although a highly specific marker for practical recovery, is a much less sensitive marker for tissue viability than perfusion imaging using single photon emission computed tomography or metabolic imaging utilizing positron emission tomography. Echocardiographic distinction perfusion agents additionally enable assessment of myocardial viability. However, no brokers are presently approved to be used in the United States for this purpose. Patients with out inducible ischemia with preserved global left ventricular systolic function are at lower threat. Those with reduced global perform, massive areas of nonviable myocardium, or ischemia are at elevated threat. Stress echocardiography may present useful information on the practical significance of multivessel disease in sufferers in whom solely the culprit vessel was revascularized. Assessment of Hemodynamics Stress echocardiography mixed with Doppler imaging is likely underutilized within the evaluation of patients with valvular heart illness. Dobutamine echocardiography could additionally be significantly helpful in sufferers with low move or low gradient aortic stenosis. Patients with low gradient aortic stenosis (which could additionally be defined by valve area <1. In the previous condition, aortic valve replacement could end in substantial improvement in left ventricular perform once the marked improve in afterload attributable to severe stenosis is relieved. Dobutamine stimulation in relatively low doses up to 20 g/kg/min could also be used to distinguish the two circumstances. The absence of contractile reserve with a marginal or no increase in ejection fraction with dobutamine is a poor prognostic sign and predicts a poor surgical consequence. In this example, the additive value of evaluation of world and regional function with echocardiography is uncertain. Bicycle train or dobutamine stress may present helpful data in individuals with complicated signs and average mitral stenosis. Both modalities of stress enable continuous or intermittent monitoring of valve hemodynamics throughout stress with bicycle train being more physiologic. The discovering of marked will increase in mitral valve gradient and pulmonary pressures coupled with signs of dyspnea indicate a person in whom the stenosis is functionally limiting. The findings of decreased ejection fraction with stress or will increase in end-systolic volume and decrease than anticipated exercise capacity identify people who will soon want surgical procedure to avoid significant postoperative left ventricular dysfunction. Assessment of train capacity, ischemic threshold, and regional and international perform with stress enables threat stratification of patients in to low, intermediate, and high risk teams (Table 50-5). Cut-off values for high-risk group are approximate values derived from obtainable research. These topics stay at low threat for no less than a quantity of years following their stress study. Provided that sufficient stress is achieved, a standard pharmacologic stress echocardiogram also identifies sufferers at low danger. Poor exercise capability, a historical past of infarction, and the presence of resting and/or stress-induced wall motion abnormalities establish patients at elevated threat.
Purchase 100 mg azycyna overnight deliveryThese clinical advantages are associated with proof of lowered progression of transforming antibiotics while breastfeeding order azycyna 250 mg on line, and in some instances antimicrobial infections azycyna 100mg fast delivery, dramatic reversal of ventricular transforming throughout therapy termin 8 antimicrobial preservative cheap azycyna 500mg otc. Taken collectively antibiotics for uti for elderly order azycyna 250mg overnight delivery, these scientific observations recommend that activation of the sympathetic nervous system mediates progression of heart failure in humans primarily via stimulation of the mocyte beta-1 adrenoreceptor subtype. In response to acute reductions in the filling of the arterial vascular area, the sympathetic nervous system, renin-angiotensin aldosterone system, and other signaling systems mediate short-term homeostatic results to return arterial pressures to the traditional range. In persistent coronary heart failure, the attenuated response to the homeostatic results of neurohormonal activation results in long-term activation of those same signaling techniques. Chronic neurohormonal activation induces maladaptive changes in myocardial structure and function through proliferative signaling pathways. Neurohormonal activation is assumed to play a important role in modulating the transforming process and disease development. Arterial and cardiopulmonary baroreceptor sensitivity are decreased and arterial chemoreceptor sensitivity is increased in experimental models and patients with heart failure. These adjustments in autonomic receptor perform occur early after myocardial damage and are thought to be an important cause of elevated sympathetic activation (as mentioned above) and also withdrawal of parasympathetic tone (as evidence by decreased coronary heart price variability and post-exercise coronary heart price recovery). The direct impression of the reduction in parasympathetic signaling on ventricular remodeling is unsure, but scientific research have consistently shown that markers of decreased parasympathetic tone are strongly related to increased threat of mortality. Renin-angiotensin Aldosterone System the renin-angiotensin-aldosterone system is activated in coronary heart failure by sympathetic activation, decreased renal perfusion, and in later phases of disease by diuretic and sodium restriction remedy. Several biomarkers of activation of the renin-angiotensin aldosterone system are associated with elevated threat or mortality. These brokers also reduce the progression of ventricular remodeling in patients after myocardial infarction. These scientific observations strongly and consequent elevated spillover of norepinephrine in to the systemic circulation. Failing myocardium is hyporesponsive to elevated sympathetic exercise because of down-regulation of the number of myocardial beta-1-adrenoreceptors, and uncoupling of receptors from their second messenger signal transduction techniques (mediated partially by beta-adrenergic receptor kinase activity). In experimental fashions, the hypertrophic effects of catecholamines are mediated primarily by alpha-adrenoreceptor subtypes linked by Gq to a mitogen-activated protein kinase signaling cascade. In patients with heart failure, elevated norepinephrine ranges in blood are strongly associated with elevated risk of mortality. Inflammatory Signaling/ Nitric Oxide Signaling Activation of pro-inflammatory cytokine signaling pathways (tumor necrosis issue alpha, interleukin-1 beta, and interleukin-6) might contribute to the ventricular remodeling process and disease development. Blood and myocardial levels of tumor necrosis issue alpha are elevated in sufferers with heart failure and have been linked to the medical phenomenon of cardiac cachexia. The stimulus for activation of inflammatory mediators could also be related to increased wall stress inside the myocardium and/or activation of other neurohormonal systems. In experimental fashions, elevated myocardial exposure to tumor necrosis factor alpha is related to contractile dysfunction, ventricular dilation, and myocyte hypertrophy. Nitric oxide can alter myocyte operate immediately by activation of soluble guanylate cyclase or by nitrosylation of sarcolemmal proteins, or indirectly by alteration of autonomic signaling within the heart. Nitric oxide is also identified to act as an uncoupling agent that reduces myocardial oxygen consumption by binding to mitochondrial cytochrome c oxidase and will contribute to the abnormalities in myocardial energy stores mentioned above. Whether inflammatory signaling plays an necessary function in the development of human coronary heart failure stays uncertain. Increased blood ranges of soluble tumor necrosis issue alpha receptors are related to elevated mortality danger. It is possible that redundant cytokine signaling might limit the effectiveness of selective anticytokine agents or that the complicated nature of cytokine signaling may lead to both beneficial and detrimental results that offset one another. These peptide hormones mediate their organic effects by activation of selective membranebound receptors linked to cyclic guanosine monophosphate signaling in goal organs (brain, heart, blood vessels, kidney, and neuroendocrine tissues). The most outstanding biological results of natriuretic peptides are vasodilation, elevated renal sodium and water excretion, and suppression of sympathetic activation and aldosterone launch. In heart failure, the biological effects of natriuretic peptides are attenuated by altered myocardial synthesis, processing and release of the hormone, by increased peptide degradation with neutral endopeptidase, and by changes in postreceptor signaling in target tissues that restrict the mobile response. Another counter-regulatory signaling molecule is endothelium derived nitric oxide. Endothelial manufacturing and launch of nitric oxide is decreased, and its vasodilating effects in vascular smooth muscle are attenuated in sufferers with heart failure. In sufferers with symptomatic coronary heart failure, the end-diastolic volume and myocardial mass could additionally be 2- to 5-fold larger than regular values. The reworked ventricle continues to function as a volume driven pump, attempting to eject blood in every systole commensurate with the blood delivered in to the ventricle during the diastolic phase of the earlier cardiac cycle. The enhance in diastolic volume preserves stroke volume within the setting of lowered ejection fraction so the center can keep regular resting cardiac outputs, albeit at elevated diastolic volumes and pressures. The capability of the reworked ventricle to reply to stress is severely restricted, as intrinsic myocyte excitation contraction coupling is impaired, regular physiological mechanisms (such because the Frank-Starling mechanism and adrenergic responsiveness) Other Neurohormonal Systems Abnormalities in numerous extra autocrine, paracrine, and endocrine components have been described in experimental and clinical heart failure, however whether these elements play a causal function in progression of illness is unsure (Table 57-2). Heart failure can be characterized by increased production of counter-regulatory hormones with actions that oppose the positive inotropic, vasoconstrictive, and hypertrophic effects induced by sympathetic activation and vasoconstricting peptide hormones. Another functional consequence of ventricular dilation is distortion of the position of the papillary muscles in relation to the mitral valve leaflets, and dilation of the mitral valve annulus. The combination of those two elements results in a preload dependent practical mitral valve regurgitation. The regurgitant lesion additional limits the ability to preserve ahead stroke volume within the setting of increased afterload. Myocardial overload Underfilled arterial area Asymptomatic Left Ventricular Dysfunction Based on epidemiological observations after myocardial infarction, many years and even decades commonly elapse between the preliminary myocardial injury and the next onset of scientific symptoms of coronary heart failure. The preservation of stroke quantity associated with increased end-diastolic quantity, the slowly progressive nature of the pathological hypertrophy and transforming process, and maybe other adaptive mechanisms that enhance effectivity of oxygen extraction within the skeletal muscle circulation during exercise forestall the development of scientific symptoms. Despite the lack of symptoms, this part of the guts failure disease process is characterized by ventricular enlargement with reduced ejection fraction, delicate neurohormonal activation, and decreased peak oxygen uptake throughout train compared with age-matched wholesome controls. These asymptomatic sufferers profit from treatment with angiotensin converting enzyme inhibitors to gradual onset of scientific heart failure and reduce mortality danger. It is presumed that sufferers with other forms of coronary heart failure also expertise a comparable asymptomatic interval of transforming after harm, although in the absence of a practical way to routinely identify these asymptomatic subjects, few data are available. In response to myocardial injury and/or overload, a mix of altered biomechanical signaling and neurohormonal signaling induces long-term adjustments in the structure and performance of the guts and resistance arterioles. These structural and performance modifications preserve stroke quantity in the setting of decreased contractile function but additionally lead to maladaptive alterations in myocardial loading circumstances that contribute to illness development. Substantial changes in myocardial construction and function could happen slowly over years after myocardial damage before growth of heart failure symptoms. Exercise Intolerance Exercise intolerance is the commonest presenting complaint in symptomatic patients with heart failure. The sudden dissociation between resting ejection fraction and functional capacity could additionally be partly attributable to poor correlation between resting and train cardiac operate. Chronotropic incompetence and the effects of exercise-induced mitral valve regurgitation and proper ventricular dysfunction on forward stroke volume are necessary elements which can contribute to decreased cardiac output reserve during exercise independently of resting ejection fraction.
Azycyna: 500 mg, 250 mg, 100 mg
Azycyna 500mg with visaThese agents must be ideally administered via a distally positioned infusion catheter or perfusion balloon virus hunter order 100mg azycyna amex. The extra commonly studied medicine are verapamil antibiotic z pak order azycyna 500 mg, adenosine antibiotic prescribing guidelines azycyna 100 mg fast delivery, nicardipine antibiotics names 250 mg azycyna sale, and nitroprusside. Aminophylline (50-100 mg) could be administered to reverse extreme side effects of adenosine. Fractional Flow Reserve and Coronary Flow Reserve Adenosine is the commonly used vasodilator within the U. Adenosine stimulates the A2 receptor of vascular myocytes to produce microvascular dilation. A comparability of balloon-expandable-stent implantation with balloon angioplasty in sufferers with coronary artery illness. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. Pathological correlates of late drug-eluting stent thrombosis: strut coverage as a marker of endothelialization. Effect of pretreatment with aspirin versus aspirin plus dipyridamole on frequency and type of acute problems of percutaneous transluminal coronary angioplasty. Intensive oral antiplatelet therapy for discount of ischaemic events References 1. Evaluation of anti-platelet aggregatory effects of aspirin, cilostazol and ramatroban on platelet-rich plasma and whole blood. Aspirin and dipyridamole in the prevention of restenosis after percutaneous transluminal coronary angioplasty. Glanzmann thrombasthenia: a model disease which paved the best way to highly effective therapeutic brokers. A medical trial of abciximab in elective percutaneous coronary intervention after pretreatment with clopidogrel. Relationship between activated clotting time during percutaneous intervention and subsequent bleeding issues. Low-molecular weight heparins in percutaneous coronary interventions: present ideas, issues, and views. Troponin T identifies sufferers with unstable coronary artery illness who profit from long-term antithrombotic protection. A novel point-of-care enoxaparin monitor to be used throughout percutaneous coronary intervention. Bivalirudin offers increasing profit with decreasing renal function: a metaanalysis of randomized trials. A clinical trial evaluating three antithrombotic-drug regimens after coronary-artery stenting. The role of intracoronary thrombolysis and percutaneous transluminal coronary angioplasty in evolving myocardial infarction. Treatment of noreflow in degenerated saphenous vein graft interventions: comparison of intracoronary verapamil and nitroglycerin. Reversal of "no reflow" throughout vein graft stenting utilizing excessive velocity boluses of intracoronary adenosine. Intracoronary adenosine administered during percutaneous intervention in acute myocardial infarction and discount in the incidence of "no reflow" phenomenon. Treatment of no-reflow and impaired move with the nitric oxide donor nitroprusside following percutaneous coronary interventions: preliminary human clinical experience. Effects of the nitric oxide donor nitroprusside on no-reflow phenomenon during coronary interventions for acute myocardial infarction. Treatment of slow/no-reflow phenomenon with intracoronary nitroprusside injection in main coronary intervention for acute myocardial infarction. Efficacy of intracoronary nicardipine within the treatment of no-reflow during percutaneous coronary intervention. Intragraft nicardipine prophylaxis to prevent no-reflow in triple-vessel saphenous vein graft intervention. Effect of intracoronary nicorandil administration on preventing no-reflow/ sluggish move phenomenon throughout rotational atherectomy. Prevention of no-reflow/slow-flow phenomenon during rotational atherectomy-a prospective randomized research evaluating intracoronary steady infusion of verapamil and nicorandil. Comparison of the results of nicorandil versus verapamil on the incidence of slow flow/no reflow throughout rotational atherectomy. Comparison of combination therapy of adenosine and nitroprusside with adenosine alone within the treatment of angiographic no-reflow phenomenon. Effect of combined intracoronary adenosine and nicorandil on no-reflow phenomenon during percutaneous coronary intervention. Intracoronary boluses of adenosine and sodium nitroprusside together reverses slow/no-reflow throughout angioplasty: a scientific state of affairs of ischemic preconditioning. Pharmacological choices for inducing maximal hyperaemia during research of coronary physiology. Distal myocardial protection throughout percutaneous coronary intervention with an intracoronary beta-blocker. Effects of metoprolol remedy on cardiac troponin-I levels after elective percutaneous coronary interventions. Safety of concomitant therapy with eptifibatide and enoxaparin in sufferers present process percutaneous coronary intervention: outcomes of the Coronary Revascularization Using Integrilin and Single bolus Enoxaparin Study. The right ventricular free wall and proper ventricular apex are averted because of the danger of free wall perforation and tamponade. Ultrasound steerage or a Doppler "sensible needle" is used for localizing the interior jugular vein in patients with tough anatomy. In some sufferers for whom the bioptome tends to "hang up" over the superior vena caval suture line or over the tricuspid valve annulus, an extended sheath is used to bypass the impeding structure, thereby limiting trauma and facilitating the biopsy. A versatile bioptome can then easily access the interventricular septum for biopsy. Long sheaths are inclined to clot easily and hence they should be flushed repeatedly or repeatedly between biopsies. Arterial sheaths are maintained beneath constant pressurized infusion and patients are systemically anticoagulated with heparin to scale back the chance of systemic embolization. Samples may be submitted for transmission electron microscopy, particularly if the scientific question is anthracycline cardiotoxicity, infiltrative issues. Small perforations in transplanted hearts can often be managed conservatively without want for pericardiocentesis. Additionally, biopsy specimens can be frozen for immunohistochemical studies, as C4D-staining for evaluation of humoral rejection or for detection of viruses in myocarditis. Morphologically, acute rejection is a mononuclear inflammatory response of, predominantly, lymphocytes in opposition to the myocardium. Grading of rejection is carried out based on the rules of the International Society for Heart and Lung Transplantation, which was revised in 2004 as proven in Table 45-3. The first is the anticipated yield of the procedure, given the scientific, pre-biopsy likelihood of a given disorder. Acute cellular rejection significantly contributes to mortality and morbidity after cardiac transplantation, accounting for 6.
Purchase azycyna 500mg on lineFamilial restrictive cardiomyopathy is extraordinarily uncommon within the absence of the above secondary causes bacteria prokaryotes 250mg azycyna overnight delivery. Loeys-Dietz syndrome is an autosomal dominant condition with a attribute triad of arterial tortuosity/aneurysm infection 4 weeks after c section discount 500 mg azycyna with visa, hypertelorism antibiotic resistance join the fight generic azycyna 500mg visa, and bifid uvula or cleft palate antibiotics for uti co amoxiclav effective 500 mg azycyna. There is critical overlap with Marfan syndrome, and the administration is analogous when it comes to cardiovascular manifestation. Early, elective, surgical intervention ought to be considered in patients with significant aneurysmal dilation of the aorta. Some clinicians have argued for much earlier surgical intervention for the dilated aorta on this situation, in contrast with Marfan syndrome, since there appears to be a much greater danger of rupture and dissection at earlier ages and smaller aortic sizes. However, figuring out wrongdoer genes have been tough because of variable penetrance and the frequent nature of the dysfunction. Aortic stenosis and infective endocarditis play a significant function in morbidity and mortality from bicuspid aortic valve. Most patients will ultimately develop signs associated to stenosis of the aortic valve, requiring surgical intervention. Serial echocardiography is really helpful in all patients with bicuspid aortic valve. Ehlers-Danlos Syndrome Ehlers-Danlos syndrome is a bunch of disorders that have an result on connective tissue growth due to defects in collagen and connective tissue biosynthesis. Cardiac manifestations include spontaneous rupture of medium to giant sized arteries including the aorta. Frequently, extracardiac shows embody hyperextensible pores and skin and hypermobile joints. To date, 11 types of the disorder have been acknowledged, however collagen defects have been described in solely 6 varieties. Although all forms of Ehlers-Danlos syndrome affect the joints and the pores and skin, scientific options range by kind. Extreme caution must be taken if surgical intervention is required as a outcome of weakened connective tissue constructions. It is a comparatively frequent finding in the basic population and the most common explanation for isolated mitral regurgitation requiring surgical restore. It can be related to other syndromic entities, such as Marfan syndrome, Ehlers-Danlos syndrome, osteogenesis imperfecta, and different collagen-related problems. Recently, mutations in the filamin A gene have been recognized in households with X-linked myxomatous valvular dystrophy. Two-dimensional images may clearly show the abnormal displacement of the valvular leaflets relative to the encompassing constructions. It affects males extra generally and incessantly is undiagnosed till adulthood as a outcome of a functionally regular valve. Bicuspid aortic valve is fashioned by two functional leaflets with two full fissures. It is related to many different cardiac disorders together with coarctation of the aorta Williams Syndrome Williams syndrome is a contiguous gene-deletion syndrome in which de novo chromosomal microdeletions of chromosome 7q. The medical spectrum varies relying on the deletion size with larger deletions related to extra severe phenotypes. Characteristic cardiovascular abnormalities embody supravalvular aortic stenosis typically at the facet of pulmonary artery stenosis. Other manifestations involve childish hypercalcemia, skeletal and renal abnormalities, mild psychological retardation, and elfin faces. The prognosis of the cardiovascular manifestations is finished by echocardiography to search for supravalvular aortic stenosis. Early detection is essential to stop nephrocalcinosis and further kidney injury from hypercalcemia with the suitable food regimen and medicine. Surgical intervention for supraaortic valvular stenosis is dependent upon the severity and the gradient across the stenosis. Genetic testing and counseling are acceptable for the relaxation of the family members. Sudden cardiac death is normally triggered by physical/emotional stress, bradyarrhythmia, electrolyte imbalance, and drugs. However, Jervell and Lange-Nielsen syndrome is associated with attribute sensorineural hearing loss and transmitted in an autosomal recessive sample. This syndrome is often extra malignant than the autosomal dominant kind and is related to a significantly larger danger of sudden cardiac demise. In addition, screening relations of sufferers with recognized mutations can assist in identifying members at risk. An implantable cardioverter-defibrillator stays the therapy of alternative in sufferers with high risk options. High danger options embrace a survivor of cardiac arrest, an extremely Noonan Syndrome Noonan syndrome is a genetic disorder with a variable medical phenotype together with typical facial dysmorphia with epicanthian folds, low set ears, webbed neck, and chest deformity. These individuals also have developmental delays, quick stature, cryptorchidism, and bleeding diathesis. Noonan syndrome is a genetically heterogeneous disorder, and more than three genes have been implicated in the pathogenesis. Genetic testing is indicated in borderline circumstances, particularly in neonates and adults the place the facial and skeletal features is probably not apparent, and in the prenatal diagnosis of a attainable transmission of the mutation from a Noonan affected mother or father. On an electrophysiology examine, people with the syndrome will often have inducible ventricular fibrillation. In people with recurrent syncope or aborted sudden cardiac dying, an implantable cardioverterdefibrillator remains the primary line of therapy. The analysis is often instructed by the historical past of an exercise or stress-induced syncope in a child. Genetic screening in the rest of the family members for the genes implicated is recommended. Brugada Syndrome Brugada syndrome is one other disorder that performs a big role in sudden cardiac dying in a structurally regular heart. Brugada syndrome is inherited in an autosomal dominant pattern with variable penetrance, contributing to the heterogeneity of the disorder. Three different sorts of Brugada syndrome have been described, depending on the manifestation on the electrocardiogram. Electrocardiogram manifestations could additionally be transient and may be unmasked by medications, namely, sodium channel blockers. Pharmacological therapy together with quinidine has been described as a potential tool. However, an implantable cardioverter-defibrillator must be considered in patients with Familial Atrial Fibrillation Atrial fibrillation is a comparatively widespread arrhythmia affecting close to two million individuals in the United States. In some studies, a household historical past of atrial fibrillation has demonstrated genetic susceptibilities.
Buy cheap azycyna 250 mgOf note bacteria kits for science fair discount azycyna 250 mg with amex, when the amount stays constant and the strain changes infection under the skin generic 250mg azycyna with mastercard, these are the isovolumic phases with contraction that happen while pressure goes up and relaxation while stress is going down antibiotic resistant sinus infection cheap azycyna 100mg. Similarly virus transmission azycyna 250mg low price, when volume is decreasing, this represents ventricular ejection, and, when volume is increasing, it represents filling. Pressure-volume loops present essential perception in to the pathophysiology of varied conditions. Ejection fraction: Amount of blood ejected in a heartbeat expressed as a proportion of complete volume. Compliance: the compliance of the left ventricle is a operate of the change in quantity in relation to change in stress, dV/dP. In any given illness state, the pressure-volume loops may evolve in response to decompensation associated with superior disease state or might change in response to remedy or loading conditions. In order to perceive and assess adjustments in pressure-volume loops, consideration must be given to the next key components: 1. A typical instance is the consideration of acute versus chronic aortic regurgitation. As disease processes advance, there often is decompensation, which finally ends up in coronary heart failure and maybe enlargement of chambers. An instance of this could be the administration of a diuretic in congestive heart failure from dilated cardiomyopathy, which might end in decreased end-diastolic stress as nicely as decrease in preload. Of note are the isovolumic phases, by which quantity stays fixed while stress changes. Similarly, ventricular ejection occurs when quantity is reducing, and ventricular filling happens when volume is increasing. Point 4 marks the beginning of ventricular filling and also marks the opening of the mitral valve. In subsequent figures, the strong blue loop represents regular and the pathologic states might be displayed in different colours and in dashed strains. Systolic dysfunction happens, for example, in idiopathic dilated cardiomyopathy, ischemic cardiomyopathy, or alcoholic cardiomyopathy. This usually results in a small stiff ventricle and leads to decreased end-diastolic quantity and elevated end-diastolic strain with decreased stroke quantity. Examples of quantity overload are circumstances of continual aortic regurgitation and continual mitral regurgitation; pressure overload is seen in individuals with hypertension and aortic stenosis. Diastolic dysfunction is seen in individuals with hypertensive coronary heart disease and in those of superior age, for example. Systolic Dysfunction Conditions similar to dilated cardiomyopathy may represent continual systolic dysfunction. These adjustments end in dilatation of the left ventricle with elevated diastolic volumes. Principally, the pressure-volume loop reveals elevated finish diastolic and end systolic volumes, leading to shift of the whole curve to the proper. Vasodilators will usually end in afterload reduction and vasoconstrictors will end in will increase in afterload. Examples of elevated inotropy are seen after administration of digoxin or dobutamine. Key Changes in Pressure Volume Loops in Various Conditions Some key changes are represented in a tabular trend in Table 39-1. Note that in superior illness states, the Table 39-1 Key components of the pressurevolume loop in varied conditions. Interventions might cause shifts in the current pressure-volume loops in accordance with their respective mechanisms of action. The usefulness of those agents as a half of a preparatory pharmacologic strategy earlier than arrival to the cardiac catheterization lab is unsure. Use of oral beta-blockers is beneficial inside 24 hours unless contraindicated whereas intravenous beta-blockade is simply really helpful in hypertensive patients. Morphine also has peripheral venous and arterial vasodilatory effect, probably reducing symptoms from pulmonary edema. One ought to exercise caution when prescribing excessive doses of morphine, given its potential results on reducing blood pressure and enhancing respiratory despair. Metoprolol was proven to decrease the speed of reinfarction and ventricular fibrillation but there were elevated episodes of cardiogenic shock in high risk patients. The absolute reduction in arrhythmia-related deaths was just like absolutely the increase in cardiogenic shock-related deaths with no overall mortality distinction. Nitroglycerin Nitroglycerin administration (sublingual or intravenous) causes peripheral arterial and venous vasodilation as well as endothelium-independent coronary artery dilatation. The efficacy of fibrinolytic brokers in lysing the thrombus diminishes as time passes, with greatest efficacy being within the first hour (Am Heart J 1999;137:34�8). Mortality benefit was greatest when administered throughout the first hour, declining in profit by 1. Fibrinolytics almost utterly lose their beneficial effects inside 12 hours after symptom onset. A meta-analysis reveals that if fibrinolytics can be administered to the suitable sufferers within the prehospital setting, time to remedy is decreased by 1 hour and mortality is lowered by 17%2. Selection of the perfect reperfusion strategy varies depending on the medical situation, patient traits, and the capabilities of the medical facility. Relationship between 30-day mortality and time from study enrollment to first balloon inflation (intention to deal with evaluation: patients assigned to angioplasty in whom angioplasty was not carried out are additionally shown). Fibrinolytic Agents All fibrinolytic brokers are direct or indirect plasminogen activators. Streptokinase is an oblique activator whereas alteplase, reteplase, and tenecteplase are direct activators. In the arm with abciximab and fibrinolytic, a decreased dose of heparin was used, unlike the full-dose in the fibrinolytic arm. Both studies showed a lower reinfarction fee and fewer refractory ischemia within the abciximab plus half-dose fibrinolytic arm; nonetheless, the 30-day or 1-year mortality was comparable in each arms. The combined major endpoint of 90-day occasion fee (death, shock, or congestive heart failure) was greater (18. Administration of clopidogrel or ticlodipine was on the discretion of the investigator. There was no distinction in the major endpoint of dying, heart failure, or resuscitated ventricular fibrillation by 90 days between the three groups (9. There was no difference within the components of the first endpoint together with mortality, coronary heart failure, cardiogenic shock, or ventricular fibrillation. Both the composite endpoint and each element of the composite endpoint (30-day mortality, in-hospital reinfarction, or in-hospital recurrent ischemia) were decreased in the enoxaparin group. The danger of noncerebral major bleeding was increased considerably solely among patients >75 years of age (7. For prior remedy with enoxaparin, if the final subcutaneous dose was administered within the prior eight hours, no extra enoxaparin should be given; if the last subcutaneous dose was administered no much less than eight to 12 hours earlier, an intravenous dose of 0.
Inositol Niacinate (Inositol Nicotinate). Azycyna. - What is Inositol Nicotinate?
- How does Inositol Nicotinate work?
- Blood disorders of the brain, migraine headaches, a disorder of fibrous connective tissue deposits in the skin and organs (scleroderma), sleeplessness (insomnia), lowering blood pressure, restless leg syndrome, acne, skin inflammation (dermatitis), inflammation of the tongue (exfoliative glossitis), psoriasis, schizophrenia, and other conditions.
- Are there safety concerns?
- Dosing considerations for Inositol Nicotinate.
- Are there any interactions with medications?
- What other names is Inositol Nicotinate known by?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96724
Best 500 mg azycynaThe primary pulmonary artery phase (arrow) is smaller in caliber than the aortic arch segment (Ao) antimicrobial keratolytic purchase 100mg azycyna with mastercard, and concave towards the best antibiotic resistance mutation cheap azycyna 250 mg without prescription. The moguls along the left heart border are the aortic arch phase (arrow 1) antimicrobial prophylaxis cheap 500 mg azycyna with visa, primary pulmonary artery section (arrow 2) antibiotics jaundice buy 100mg azycyna, and left atrial appendage phase (arrow 3). Left atrial enlargement is demonstrated by the convexity of the left atrial appendage segment away from the center, and the double density (arrowheads) considered via the cardiac silhouette. Left atrial hypertension is indicated by the indistinctness of the decrease lobe vessels, and the dilated higher lobe vessels. The upper left heart border (arrowheads) is occupied by a continuous, sharp density, representing the left aspect of the left-sided ascending aorta in corrected transposition of the good arteries. No pulmonary artery phase is seen as a end result of it lies over the mediastinum, to the right of the left heart border. The left atrial appendage segment (arrow 3) is flat, and the contour of the left ventricular segment is rounded, indicating left atrial and left ventricular enlargement. The left ventricular contour (arrow 4) extends farther toward the left (appears extra rounded), and the cardiac silhouette seems enlarged, all reflecting left ventricular dilatation. The major pulmonary artery phase (arrow 2) is greater in caliber than the aortic arch phase (arrow 1). Notice the dilated hilar proper pulmonary artery (arrow 3) seen by way of the rotated coronary heart. Pulmonary venous hypertension leads to a collection of radiographic modifications, reflecting increasing severity of the abnormality. The first signs of left atrial hypertension end result from the dilatation of the pulmonary venules and rising separation of the cells of the venular wall, increasing the scale of the interspaces between the cells, allowing passage of water from the vascular compartment in to the perivascular sheaths surrounding these buildings. When this occurs, the fluid-filled pulmonary veins are not surrounded by air-filled lungs (causing sharp vascular edges). If the method elevating left atrial strain continues, the venular stress rises and more fluid leaves the vascular area to enter the interstitial house, and the vessels turn out to be much less and less obvious. As pulmonary venous stress continues to rise and the parenchyma turns into more edematous, resistance to decrease lobe pulmonary blood circulate increases. However, finally, the left atrial myocardium can now not hypertrophy to keep perform at regular chamber measurement, and the atrium begins to dilate. The earliest radiographic signal of left atrial enlargement is posterior displacement of the left bronchus, greatest seen in the lateral chest movie. The interstitial infiltrates have turn into denser (while still retaining their not sharp edges), indicating progression to alveolar pulmonary edema. Furthermore, elevated higher lobe arterial circulate leads to elevated higher lobe venous return to the center; thus both the higher lobe arteries and veins enlarge. Dilatation of the upper lobe arteries in left-to-right shunts and the upper lobe arteries and veins may be difficult to differentiate (as one might ask, "Is a person vascular structure an artery or vein However, when the upper lobe arteries are enlarged in elevated circumstances associated with elevated pulmonary blood move, the principle and hilar pulmonary arteries are enlarged, the lower lobe vessels are dilated, and all pulmonary vessels remain sharp. Upper lobe enlargement associated with pulmonary venous hypertension is all the time associated with absence of sharpness of the lower lobe veins, and relying upon the underlying disease, it might or will not be related to dilatation of the principle or hilar pulmonary arteries. The nature of these infiltrates may be very useful for differentiating these lesions from the typical infiltrates of pneumonia. All the alveolar areas are crammed, so the infiltrate is dense, with sharp edges defining the anatomic distribution. The nearly homogeneous density and anatomic distribution (right middle lobe) of this infiltrate characterize it as pneumonia. As intrathoracic strain gradients change (patient lying on back, upright, proper or left facet down), the distribution in the lungs adjustments, and the infiltrates change their distribution (so called "fleeting infiltrates"). If the reason for the left atrial hypertension is resolved, then this progression from lower lobe indistinctness (mild) to redistribution (moderate), to alveolar infiltrates (severe) radiographic abnormality reverses, and a traditional chest movie is to be expected. Chronic gentle left atrial hypertension often goes on to a sample of interstitial fibrosis. Right coronary heart dilation causes cardiac rotation, which will change the looks of the mid left coronary heart border within the area of the anticipated left atrial appendage section. In a traditional coronary heart, the right ventricular outflow tract is medial to the projection of the left atrial appendage and left ventricular contour. When the right heart dilates, clockwise rotation of the heart rotates the left atrial appendage posteriorly and brings the outflow tract to the left. The dilated right ventricular outflow tract then turns into left heart border-forming. This modifications the looks of the left heart border and gives the look of a convex (away from the guts, i. Clockwise cardiac rotation affects the relationship of the projection of the left bronchus to the projection of the left heart border. Under normal circumstances, the projection of the left bronchus crosses the projection of the left coronary heart border. In truth, we outline the left atrial appendage segment of the left coronary heart border as that portion beneath the projection of the left bronchus, and above the curvature of the left ventricular contour. However, the relation between the projection of the left bronchus and altered left coronary heart border changes. The differential analysis of left atrial appendage phase enlargement is given in Table 46-3. The superior mediastinum on the level of the Ao may be very slender, reflecting the leftward rotation of the superior vena cava over the spine. Furthermore, discover how the left bronchus appears to run parallel to the upper left coronary heart border. The proper ventricular outflow has rotated toward the left to occupy a portion of the left heart border. Global changes to the looks of the left ventricular contour result in elevated roundness in the contour. In the normal coronary heart, the left ventricular portion of the left heart border takes a nearly vertical orientation. Congestive coronary heart failure Left Ventricular Contour the bottom portion of the left coronary heart border is the left ventricular contour. The ascending aortic phase (arrow) is enlarged, extending over the hilar proper pulmonary artery. The dilated ascending aorta (arrowheads) begins to fill the retrosternal area from behind. Overall heart size could not enhance, however the form of the left coronary heart border is altered. Such international change may be present in people with left ventricular quantity loading (dilatation), left ventricular pressure loading (hypertrophy), and abnormalities of left ventricular compliance. Certainly, when the left heart border approaches the lateral left chest wall, we will all agree that the ventricle is dilated. If, in lateral view, this level is contained by the posterior facet of the decrease heart border, then the left ventricle is dilated. Certainly, if the left ventricle is in fact dilated, then hypertrophy could be "lost" in the enlarged contour. Only an abnormality along a heart border-forming portion of the left ventricle might be apparent. Thus, an abnormality located posterior or anterior to the left ventricular contour is probably not identified.
Generic azycyna 100mg without a prescriptionPacking usually entails the use of continuous gauze (eg antimicrobial growth promoters discount 100 mg azycyna with amex, Kerlex) within a sterile plastic bag or glove antibiotics for hotspots on dogs cheap 100mg azycyna amex. Transurethral Foley catheter placement and prophylactic antibiotic use should be thought of to prevent urinary retention and infection bacteria 400x discount azycyna 100mg otc, respectively infection movies cheap azycyna 500 mg with mastercard. This silicon balloon is positioned inside the uterus either manually or under ultrasound steerage. Surveillance of persistent bleeding is feasible because the balloon catheter drains in to a set bag. After bleeding has slowed, the balloon may be steadily deflated and subsequently eliminated. Tamponade balloons can be utilized in isolation for postpartum hemorrhage control or in conjunction with other procedures (ie, surgery or selective arterial embolization). When bleeding continues regardless of conservative therapy, surgical management by way of laparotomy must be thought of. Interventions include arterial ligation, uterine compression sutures, and hysterectomy. The goal of arterial ligation is to lower uterine perfusion and subsequent bleeding. Success rates have diversified from 40% to 95% in published literature depending upon which arteries are ligated. It is beneficial that a tamponade balloon be placed with the suture placement to guarantee enough hemorrhage control. Compression sutures are greatest used for circumstances of uterine atony managed by bimanual therapeutic massage and focal invasive placentation with want for future fertility. Also, help from other surgical specialties may be essential and a delay in session ought to be avoided. Nonobstetrical Services Nonobstetrical services which might be significantly helpful in postpartum hemorrhage administration embody interventional radiology, the pharmacy, and an intensive care staff. Selective arterial embolization has gained success and recognition for postpartum hemorrhage management. The technique entails pelvic angiography to visualize the bleeding vessels and placement of Gelfoam (gelatin) pledgets in to the vessels for occlusion. Reported disadvantages include postembolization fever, infection, ischemic pain, and tissue necrosis. Unfortunately, a lack of speedy availability may limit its usefulness in some amenities. In addition to interventional radiology, one other nonobstetrical service that may be crucial in profitable postpartum hemorrhage management is the pharmacy. Unfortunately, the half-life of the agent is relatively brief (2 hours) so repeated dosing could also be needed in some circumstances. Hemostatic brokers include fibrin sealants (eg, Tisseal), hemostatic matrices (eg, Floseal), and Gelfoam. These brokers are notably useful in situations of consumptive coagulopathy related to diffuse low-volume bleeding. The patient who endures a severe postpartum hemorrhage is at danger of a number of comorbidities as noted in the following part. General Complication Assessment Once a postpartum hemorrhage has efficiently been treated, the affected person is still at risk for complications associated to the blood loss, the therapy, or both. It is necessary for the obstetrician to critically assess the patient for basic organ system problems. These problems include hypoperfusion accidents to the mind, coronary heart, and kidneys, infection, persistent coagulopathy, acute lung damage due to large transfusion necessities, and pituitary necrosis. By being conscious of those potential complications, the doctor can be positive that proper posthemorrhage care and session can be found in a timely fashion in order that additional morbidity can be prevented. Variations in the incidence of postpartum hemorrhage throughout hospitals in California. Increased plasma and platelet to purple blood cell ratios improves end result in 466 massively transfused civilian trauma patients. Predefined large transfusion protocols are related to a discount in organ failure and postinjury issues. How we deal with: management of life-threatening major postpartum hemorrhage with a standardized large transfusion protocol. Looped uterine sutures and tamponade balloon take a look at (looped us-tb test) for surgical administration of huge obstetric hemorrhage (Correspondence, 2009). The B-Lynch surgical approach for control of large postpartum haemorrhage: a substitute for hysterectomy Compressive uterine sutures to deal with postpartum bleeding secondary to uterine atony. Pelvic embolization for intractable postpartum hemorrhage: long-term follow-up and implications for fertility. By understanding the pathophysiology and occasions that result in these doubtlessly catastrophic medical situations, we will respond extra quickly and infrequently prevent them from becoming important conditions. Rapid, decisive, and educated motion on the a part of the obstetrician can usually avert an adverse end result. The finest type of therapy is geared toward correcting the underlying pathophysiologic downside, as nicely as treating the acquired or inherent clotting downside. This chapter outlines a practical strategy to these sufferers with these issues. It is characterized by accelerated formation of fibrin clots with simultaneous breakdown of these identical clots. Normally, our body is in a constant stability between fibrin technology and fibrinolysis. Following placental separation after a vaginal supply, fibrinogen is activated to become a fibrin mesh, which covers the old placental site. This, together with uterine contraction, prevents extreme blood loss within the quick postpartum interval. The genesis of this fibrin mesh results in a 10% reduction in the concentration of clotable fibrinogen following a traditional vaginal supply. In severe cases, the placenta partially detaches from the wall of the uterus and a retroplacental clot types. It is necessary to observe that the concentration of clotable fibrinogen is usually tremendously elevated throughout a traditional being pregnant. A concentration that may be "labeled" as normal by your laboratory might, certainly, be abnormally low for a pregnant patient. The clinician must depend on the general clinical image, as a outcome of a "baseline" fibrinogen focus is often not available. If, nonetheless, an unsuspected demise is found and it appears that the fetus expired some time beforehand, a coagulation profile is indicated.
Cheap 100mg azycyna otcThese could impair blood provide to the cells or have an effect on metabolic processes within the cells antibiotics for pink eye purchase 100 mg azycyna with visa. Infectious illnesses cause cell harm through the actions of microorganisms (living organisms too small to be seen with the bare eye) similar to bacteria and viruses most effective antibiotics for sinus infection purchase azycyna 100mg with amex. Some genetic defects or inborn errors of metabolism can lead to antibiotic injection for uti cheap 100 mg azycyna visa irregular metabolic processes infection limited mobile al discount azycyna 100 mg without prescription. Altered metabolism results in accumulation of poisonous middleman compounds contained in the cells that in the end destroy them. In basic, the preliminary cell damage causes an alteration in a metabolic response, which ends up in a loss of perform of the cell. If the factor inflicting the damage is eliminated rapidly, the cell may have the ability to recuperate and return to its normal state, and the harm is alleged to be reversible. As the amount of harm will increase, detectable morphologic or structural modifications occur within the nucleus and the cell as nicely. Generally these contain cellular swelling and rupture if the cell membrane is affected or accumulations of lipid inside the cell if metabolic derangements are current. The cells undergo lysis or dissolution, releasing destructive lysosomal enzymes in to the tissue, which trigger irritation (swelling, redness, and pain) in addition to damage to nearby cells and reduced function (see chapter 2). If a massive number of cells have died, irritation may be in depth, inflicting the destruction of further cells. The enzymes released from the lifeless cells can diffuse in to the blood, providing helpful clues in blood exams that indicate the type of cells broken. The areas of white chalky deposits represent calcium soap formation at sites of lipid breakdown. Brain cells die quickly (4 to 5 minutes) when deprived of oxygen, whereas heart muscle can survive for roughly 30 minutes. Formerly death of the physique (somatic death) was assumed to happen when heart action and respiration ceased. Now because cardiac and respiratory operate may be maintained artificially, the analysis of demise is more complicated. Pathophysiology is the research of the structural and functional modifications related to illness processes. The allocation of sources for well being care and the moral issues related to new applied sciences are issues. The dialogue of illness processes includes such matters as occurrence, prognosis, or the identification of a disease; etiology or the reason for disease; pathologic changes within the tissues or organs, or signs and symptoms of illness; and prognosis, or the possible outcomes. Metaplasia often occurs as an adaptive change, replacing the normal cell with a extra resistant cell. Prepare an applicable record of six terms that you could use to describe this disease, and define each of the terms. Describe briefly three particular pathophysiologic results of insufficient health care or lack of well being care. Match the significant data above to the appropriate time period: prognosis, medical historical past, etiology, prognosis, benign neoplasm, iatrogenic, indicators, complication, therapy, most cancers, examination of living tissue. Describe how adjustments in capillary change have an effect on the tissues and the blood components. Associated with these mechanical limitations are physique secretions similar to saliva or tears that comprise enzymes or chemicals that inactivate or destroy potentially damaging material. The second line of defense consists of the nonspecific processes of phagocytosis and irritation. Phagocytosis is the method by which neutrophils (a leukocyte) and macrophages, the "vulture cells," randomly engulf and destroy micro organism, cell particles, or foreign matter. Inflammation includes a sequence of events intended to restrict the consequences of harm or a dangerous agent in the body. Interferons are nonspecific brokers that shield uninfected cells towards viruses (see chapter 4). The third line of defense, the immune system, is the specific defense mechanism in the body (see chapter 3). It offers safety by stimulating the production of distinctive antibodies or sensitized lymphocytes following publicity to particular substances. In current years a lot effort has been expended on research on the immune system in an effort to enhance understanding of the process of the immune response and to create ways to strengthen this protection mechanism. Precapillary sphincters composed of clean muscle prohibit blood move by way of some channels. Movement of fluid, electrolytes, oxygen, and nutrients out of the capillary at the arteriolar finish is based on the web hydrostatic stress. The net hydrostatic pressure is based on the distinction between the hydrostatic strain inside the capillary (essentially arterial pressure) as compared with the hydrostatic strain of the interstitial fluid in the tissues in addition to the relative osmotic pressures within the blood and interstitial fluid. Differences in concentrations of dissolved substances within the blood and interstitial fluid promote diffusion of electrolytes, glucose, oxygen, and different nutrients throughout the capillary membrane. Blood cells and plasma proteins (albumin, globulin, and fibrinogen) normally stay inside the capillary. At the venous finish of the capillary hydrostatic strain is decreased because of the earlier motion of fluid in to the interstitial fluid house, and osmotic stress within the vessels is comparatively high as a outcome of plasma proteins remain within the capillaries. This arrangement facilitates the motion of fluid, carbon dioxide, and other wastes in to the blood. Excess fluid and any proteins are recovered from the interstitial space by the use of the lymphatic system and eventually returned to the final circulation. Inflammation is a traditional protection mechanism within the body and is meant to localize and take away an injurious agent, whatever it might be. You have in all probability observed the inflammatory process resulting from a reduce, an allergic reaction, an insect bite, an an infection, or a small burn in your body. The basic indicators and signs of irritation function a warning of a problem, which may be hidden throughout the body. With infection, microorganisms such as a micro organism, viruses, or fungi are at all times present on the site, causing the irritation. This microbe can be identified and appropriate treatment instituted to cut back the an infection, following which, the inflammation will subside. The root word is often a body part or tissue; for instance, pancreatitis, appendicitis, laryngitis, or ileitis. Cells stay in blood A Chemotaxis = Blood Cell A = Albumin G = Globulin F = Fibrinogen B = Bradykinin H = Histamine 6. Inflammation may develop immediately and final solely a brief while; it may have a delayed onset. The severity of the inflammation varies with the specific trigger and period of publicity.
References - Agrawal A, Hila A, Tutuian R, et al: Clinical relevance of the nutcracker esophagus: Suggested revision of criteria for diagnosis. J Clin Gastroenterol 40:504, 2006.
- Dyamenahalli U, McCrindle BW, McDonald C, et al: Pulmonary atresia with intact ventricular septum: Management of, and outcomes for, a cohort of 210 consecutive patients. Cardiol Young 2004; 14:299-308.
- Ghanayem NS, Berger S, Tweddell JS: Medical management of the failing Fontan, Pediatr Cardiol 28:465-471, 2007.
- Kobashi KC, Leach GE, Chon J, et al: Continued multicenter followup of cadaveric prolapse repair with sling, J Urol 168:2063n2068, 2002.
- Meyers MA: Distribution of intra-abdominal malignant seeding: Dependency on dynamics of flow of ascitic fluid. AJR 1973; 119:198-206.
- Simpson RHW: Salivary gland tumours. In Recent Advances in Histopathology, number 17, Anthony PP et al (Eds). London, Churchill Livingstone, pp 167, 1997.
- Ebert TJ, Messana LD, Uhrich TD, et al. Absence of renal and hepatic toxicity after 1.
|