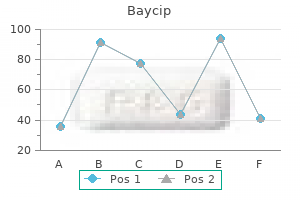
Baycip
Kwesi Hankins, RN - Department of Emergency Medicine
- Methodist Hospital
- Peoria, IL
Proven baycip 500mgNonoperative management was successful and resulted in no delayed nephrectomies in a cohort of 108 hemodynamically steady sufferers with stab wounds (Armenakas et al treatment 4th metatarsal stress fracture discount 500mg baycip free shipping. The only absolute intraoperative indication for kidney exploration is a pulsatile and expanding retroperitoneal hematoma treatment hpv order baycip 500 mg line, that suggests a life-threatening renal artery laceration medications for adhd discount baycip 500 mg with mastercard. All patients with high-grade injuries chosen for nonoperative administration should be closely noticed with serial hematocrit readings and important indicators treatment room generic baycip 500mg amex. Should bleeding persist or delayed bleeding happen, angiography with selective embolization of bleeding vessels can obviate surgical intervention. The patient ought to be periodically undergo blood strain monitoring for as a lot as a year publish harm, for the uncommon instance of acute or delayed renovascular hypertension. Delayed bleeding after discharge to house is rare and often occurs within 2 weeks submit harm. Risk elements for failure embrace renal damage grade, nonrenal stomach accidents, and penetrating accidents (Bjurlin et al. Most patients for whom conservative administration fails require only a ureteral stent or angioembolization. Although nonoperative administration for renal trauma has been increasing, latest examine shows that the rate of surgical intervention for renal trauma varies considerably among high-, medium-, and low-volume trauma facilities, with high-volume facilities intervening in solely 12. Initial observation is warranted for sufferers with renal damage and urinary extravasation (Morey et al. Such injuries usually resolve spontaneously in over 90%, unless a renal pelvis avulsion or proximal ureteral avulsion harm is current. For such sufferers, immediate intervention is required, either endoscopically or open, depending on the scientific state of affairs. When continued urinary drainage results in enlarging urinoma, fistula, an infection, or indicators of chemical peritonitis corresponding to ache, fever, ileus, urinary drainage by way of ureteral stent and/or urinoma drain are required. In extreme renal injuries with continued urinary extravasation, placement of an internal ureteral stent alone for drainage usually prevents prolonged urinary extravasation and decreases the prospect of perirenal urinoma formation. Examples include concomitant pelvic fracture urethral distraction defects, severe genital trauma prohibiting urethral entry, complete ureteral transection, and fractures prohibiting the dorsal lithotomy position. Percutaneous nephrostomy drainage with consideration for antegrade ureteral stent placement is a viable option in these situations. When the perinephric fluid assortment persists regardless of ureteral stenting or percutaneous nephrostomy drainage, placement of a percutaneous drain can facilitate healing and forestall or treat abscesses. Renal Exploration Surgical exploration of the acutely injured kidney is best by a transabdominal approach, which permits complete inspection of intra-abdominal organs and bowel. In some reported series of penetrating injuries, nonrenal organ injury has been noted to be as excessive as 94% (McAninch et al. Injuries to the nice vessels, liver, spleen, pancreas, and bowel can be recognized and stabilized, if necessary, before renal exploration. The renal vessels are isolated before exploration to provide the immediate capability to occlude them if large bleeding should ensue when Gerota fascia is opened (Scott and Selzman, 1966). An incision is remodeled the aorta in the retroperitoneum simply superior to the inferior mesenteric artery. Exposure of the anterior surface of the aorta is achieved and adopted superiorly to the left renal vein, which crosses the aorta anteriorly. The vein usually must be retracted cephalad, with a vein or-Gil Vernet retractor, to expose the left and right renal arteries beneath. The right renal vein also could be secured via this incision; but when this proves difficult, reflecting the second portion of the duodenum supplies glorious exposure to the vein. Large hematomas may prolong over the aorta and obscure the landmarks for the deliberate preliminary retroperitoneal incision. In such cases, the inferior mesenteric vein can be used as an anatomic information for an applicable incision. By making the retroperitoneal incision just medial to the inferior mesenteric vein and dissecting via the hematoma, the anterior surface of the aorta can be identified and followed superiorly to the crossing left renal vein. The kidney is then uncovered by incising the peritoneum lateral to the colon, followed by mobilization off Gerota fascia. This maneuver often requires launch of the splenic (left) or hepatic (right) attachments of the colon. Gerota fascia is then opened, and the kidney with damage is completely dissected from the encircling hematoma. Should troublesome bleeding develop, the previously isolated vessels can be quickly occluded with a vascular clamp or a vessel loop tourniquet. Some manadate that control of the renal Operative Management Indications for renal exploration or speedy angioembolization after trauma may be separated into absolute and relative (Morey et al. Absolute indications include (1) hemodynamic instability with no or transient response to resuscitation, (2) expanding/pulsatile renal hematoma (usually indicating renal artery laceration), (3) suspected renal vascular pedicle avulsion, and (4) ureteropelvic junction avulsion. More latest data counsel that sufferers with renal devascularization and urine leak even have wonderful outcomes, with only one of 18 (6%) sufferers requiring subsequent intervention during conservative management of segmental renal artery injuries (Elliott et al. Should nonviable tissue represent more than 25% in association with a parenchymal laceration, urinary extravasation, or each, the potential for complications. The argument being, that proximal vascular management avoids a possible large bleed, from launch of the tamponade effect. Thus, obtaining early vascular management earlier than opening Gerota fascia can lower renal loss, depending on the harm web site. In a comparative sequence, the whole nephrectomy fee was decreased from 56% to 18% when vascular control was obtained (McAninch and Carroll, 1982). In a series of 133 renal models by which early vessel isolation and control have been achieved earlier than opening Gerota fascia, McAninch et al. Overall, the aim of kidney exploration is to management the bleeding first, repair the kidney (when possible) and retroperitoneal drainage. Regardless of the method of vascular management, when unstable, high grade kidney trauma patients endure open retroperitoneal exploration, nephrectomy is usually the outcome. Renovascular penetrating or avulsion injuries after trauma are uncommon and often have related accidents requiring operative intervention. For main renovascular injuries in sufferers with two kidneys, immediate nephrectomy is advocated. In rare instances in which vascular repair is technically feasible, renal salvage charges are disappointingly low, exemplified by a 33% renal salvage fee for major renal artery reconstruction even in the most expert of hands (Elliott et al. Main renal artery thrombosis from blunt trauma happens most frequently secondary to deceleration injuries. The mobility of the kidney leads to stretch on the renal artery, which in turn causes the arterial intima, low in elastic fibers, to disrupt. For unilateral arterial thrombosis, revascularization rarely ends in a profitable salvage or a viable kidney. As lengthy as the contra-lateral kidney is regular, remark is often one of the best management. In contrast, for bilateral renal hilar accidents, revascularization should be tried, as as a lot as 56% of patients can doubtlessly keep away from dialysis by immediate intervention (Knudson et al. Case stories of successful renal revascularization through the use of endovascular stents during angiography provides a promising method to the issue of blunt trauma renal artery thrombosis caused by the intimal flap (Inoue et al. The great disadvantage of this approach has been the shortcoming to safely institute post-stent anticoagulation in the affected person with polytrauma.
Generic 500mg baycip fast deliveryAnother large-scale review involving 189 cases of laparoscopic pyeloplasty identified roughly 2% to 2 symptoms 6dpo buy cheap baycip 500 mg on line. The total success of open dismembered pyeloplasty has been favorable in the literature 2c19 medications baycip 500 mg on-line. Of the 111 patients with open pyeloplasty symptoms dehydration discount baycip 500mg with amex, 95 (86%) patients underwent dismembered pyeloplasty 4 medications proven 500mg baycip. Most of the printed laparoscopic pyeloplasty reports have used the traditional Andersen-Hynes dismembered approach as a outcome of most laparoscopic surgeons try to duplicate the well-established principles of open surgery (Bachmann et al. The overwhelming majority of patients in these recent collection had major laparoscopic pyeloplasties, and the mean operative instances are in the vary of 119 to 252 minutes. In experienced arms, the entire procedure can be persistently performed in lower than 3. With mean follow-up times of 14 to 26 months, the rates of surgical success (defined as sturdy medical and/or radiographic success) reach the vary of 87% to 99%; nearly all of contemporary series report success charges of greater than 95%. The safety and efficacy of laparoscopic pyeloplasty have additionally been demonstrated in the pediatric population together with sufferers youthful than 1 year (Metzelder et al. Most failures from laparoscopic pyeloplasty happen within the first 2 years, although up to 30% of failed circumstances may happen after 2 years postoperatively (Madi et al. For the sufferers who fail laparoscopic pyeloplasty, open surgery has been used as a salvage procedure, with success rates of approximately 86% (Thomas et al. However, most instances may be nicely managed with endoscopic intervention corresponding to endopyelotomy, with success charges of roughly 70% (Varkarakis et al. More data on robotic-assisted laparoscopic pyeloplasty have emerged just lately (Table 89. Like the traditional laparoscopic research, the overwhelming majority of the patients in these latest sequence had primary robotic-assisted laparoscopic pyeloplasties. With mean follow-up times of eleven to 39 months, the rates of surgical success (defined as sturdy scientific and/or radiographic success) are 94. These outcomes were much like those from the historic laparoscopic collection within the literature. The feasibility of the robotic strategy has also been demonstrated within the pediatric sufferers (Atug et al. The further reported benefits supplied by the robotic embrace better 3D magnification, increased vary of motion, and ease of dissection and suturing. However, the worth of the robot in the setting of medical pyeloplasty stays controversial and has been addressed by one recent research (Link et al. In this research comparing robotic and laparoscopic pyeloplasty in a prospective method, the mean operative time and total room time for robotic cases have been discovered to be considerably longer than laparoscopic cases by 19. Beyond value, additional issues for the robotic-assisted laparoscopic pyeloplasty embrace limited instrumentation and want for knowledgeable bedside laparoscopic help (Peschel et al. Although success rates of pyeloplasty are typically high, late failures can happen and long-term follow-up could additionally be useful in identifying these patients. A newer sequence of robotic pyeloplasties had limited radiographic follow-up (mean 12. Open conversion was necessary in 1 patient, and postoperative Special Situations of Laparoscopic and Robotic-Assisted Laparoscopic Management of Ureteropelvic Junction Obstruction Laparoscopic and Robotic-Assisted Laparoscopic Ureterocalicostomy. Ureterocalicostomy has been accomplished successfully by way of laparoscopic and robotic-assisted laparoscopic approaches. In both patients a double-J ureteral stent was first positioned into the ipsilateral ureter cystoscopically. With the affected person in a 45- to 60-degree flank position, a transperitoneal method utilizing three or 4 ports was used to gain entry to the ipsilateral renal unit laparoscopically. A round rim of the tip of the thin lower pole renal parenchyma was recognized and excised. The ureter was spatulated laterally, and end-to-end ureterocaliceal anastomosis with mucosa-to-mucosa apposition over the preplaced double-J stent was performed with free-hand intracorporeal suturing and knot-tying techniques. The basic reconstructive principles are identical to those of open ureterocalicostomy described previously, including the want to achieve tension-free, water-tight, dependent drainage. The largest sequence of ureterocalicostomies reports outcomes in seventy two procedures, 38 of which have been laparoscopic, whereas the remainder were open procedures (Srivastava, 2017). Mean follow-up was 60 months, and 82% of patients had had earlier ipsilateral renal surgical procedure. This success price is pretty similar to different "redo" pyeloplasty sequence, although it contrasts with some smaller ureterocalicostomy sequence, suggesting the significance of technical and affected person components within the choice to carry out this operation. Mean operative time was 168 minutes, and feasibility of using a robot was well demonstrated. In the collection, extraction of the caliceal stones was assisted by method of a flexible cystoscope introduced by way of a 10- to 12-mm port website. Robotic-assisted laparoscopic pyeloplasty with concomitant pyelolithotomy has also been demonstrated in eight patients, utilizing the similar instruments together with laparoscopic graspers (Atug et al. Presence of a big higher ureteral defect after the excision of ureteropelvic junction stricture may be managed laparoscopically with success. Using a four-port transperitoneal strategy, a wide-base renal pelvic flap was created and tubularized to bridge the defect, using intracorporeal freehand suturing methods. At a 2-month follow-up, excretory urography and diuretic renal scan confirmed a extensively patent higher ureter. Rather than performing tedious anatomic dissection and complicated ureteral reconstruction in such a scenario as required in typical laparoscopic pyeloplasty, a nephrotomy was created on the most dependent portion of the hydronephrotic lower pole moiety after which laparoscopically anastomosed to the bladder dome vesicostomy utilizing intracorporeal freehand suturing and knottying techniques. At the 4-month follow-up, patent calicovesicostomy was confirmed endoscopically and clinically. These variations in many cases may be carried out by way of both open or minimally invasive approaches, depending on the talent level of the surgeon. Like different flap techniques, nevertheless, its use has typically been changed by the more versatile dismembered pyeloplasty. As in different flap strategies, the Foley Y-V-plasty is particularly contraindicated when transposition of lower pole vessels is critical. In situations requiring concomitant reduction of redundant renal pelvis, this system can be of little value. In Foley Y-V-plasty, the renal pelvis and proximal ureter are first exposed, and a extensively primarily based triangular or V-shaped flap is printed with methylene blue or fine stay sutures. The incision from the apex of the flap (the stem of the Y) is then performed along the lateral side of the proximal ureter. First, the apex of the pelvic flap is approximated to the apex (inferior aspect) of the ureterotomy incision utilizing fine, absorbable suture. Interrupted method is more doubtless to reduce pursing or buckling of the suture line, in addition to native tissue ischemia. The Culp-DeWeerd spiral flap is usually finest suited for giant, readily accessible extrarenal pelves, in which the ureteral insertion is already in a dependent, oblique place. Retroperitoneal laparoscopic strategy and anterior extraperitoneal approach rely on creation of a working area utilizing guide or balloon dilation. The incision from the apex of the flap, which represents the stem of the Y, is then carried along the lateral facet of the proximal ureter properly into an area of normal caliber. The apex of the pelvic flap is then dropped at probably the most inferior aspect of the ureterotomy incision.
Syndromes - PET scan (sometimes useful for determining the stage of disease, and whether surgery is possible)
- Secondary aplastic anemia
- Loss of vision
- Viruses
- An infant younger than 2 months is constipated
- Bites, either human or insect
- Did it begin recently?
Baycip 500 mg cheapCaution is required while performing this process as a result of it entails surgery on the unhurt treatment xerosis cheap 500 mg baycip amex, contralateral ureter with the theoretical risk for changing unilateral ureteral injury into (iatrogenic) bilateral ureteral damage treatment 5th finger fracture cheap baycip 500 mg on line. For the non-acute trauma affected person daughter medicine baycip 500mg without prescription, and in an elective style treatment uti infection buy baycip 500 mg low cost, robotic ureteroneocystostomy is increasingly widespread with successful fee of around 95% (Fifer et al. Standard rules of ureteroneocystostomy embody a protracted, nontunneled, spatulated, stented anastomosis. A comparability of nonrefluxing and refluxing anastomoses in neobladders discovered a better rate of stricture resulting in renal deterioration within the nonrefluxing group (Shaaban et al. As such, we favor nontunneled anastomoses for the trauma patient, because we choose the very low risk of clinically vital reflux to the higher threat of ureteral obstruction utilizing a tunneled strategy. We choose it over ureteroureterostomy in decrease ureteral accidents because the tenuous ureteral blood provide might not survive transection. Some authors favor end-to-end repair in lower ureteral injuries when the distal stump is preserved (Paick et al. For decrease ureteral injuries, the ureteral gap may be bridged by "hitching" (suturing) the apex of the bladder to the ipsilateral psoas muscle and psoas minor tendon. The contralateral superior vesical pedicle is often divided to improve mobilzation. Nontapered distal ileal section is anastomosed to the bladder in a wide-open, and refluxing style. Delayed ureteral repairs, particularly when a very long segment of ureter is destroyed, additionally may be carried out by creation of an ileal "chimney" in much the same way that an ileal conduit is constructed to drain the urine after cystectomy. Success charges for ileal replacement of the ureter have been reported to be 81% (Boxer et al. A review of long-term complications of 99 renal items reported a 3% anastomotic stricture and 6% fistula rate (Armatys et al. Hyperchloremic metabolic acidosis occurred in 20% of sufferers, pyelonephritis in 9%, and surgical intervention in 4%. Some have successfully used the Monti procedure, by which brief segments of small or giant bowel are sewn together to make a protracted, skinny tube in ureteral reconstruction (Ali-el-Dein and Ghoneim, 2003; Bao et al. We typically favor to mix the ileal chimney with an ipsilateral Psoas bladder hitch, so as to shorten the length of the conduit and hypothetically lower the danger of metabolic and mucus problems. Ileal interposition has no position within the acute repair of ureteral injury and must be reserved only for delayed or staged repairs. There is little consensus within the literature when and tips on how to picture for silent hydronephrosis/ureteral obstruction after traumatic ureteral reconstruction. Typically a diuretic renogram or renal ultrasound with doppler imaging for ureteral jets is carried out at four to 12 weeks and at 1 year post harm. Because ureteral damage repairs typically occur within the setting of ureteral devascularization, late stenosis can occur and is often clinically silent. Rarely, acute nephrectomy is required to deal with ureteral damage after exterior trauma. Delayed nephrectomy could also be required because of poor renal perform (which can sometimes be seen after delayed recognition of an obstructing ureteral injury), severe panureteral injury when ileal ureter or other reconstruction is unimaginable, or persistent ureteral fistula (especially vascular fistula) despite earlier intervention (Ghali et al. Bladder is opened and secured to the psoas muscle to facilitate ureteral anastomosis. If the patient is unstable, the process must be delayed till a planned and staged repair. If the bladder is regular in measurement and thickness, a protracted pedicle of bladder may be incised and rotated cephalad and tubularized to bridge the hole to the injured ureter. Primary repair of a partial transection is used in the majority of ureteral accidents, up to 58% of the time in a single large sequence (Presti et al. Principles of main restore contain spatulated, watertight closure, with interrupted or working absorbable suture similar to Maxon (polyglyconate), Vicryl (polyglactin 910), or Dexon (polyglycolic acid). The ureteral damage is closed by changing a longitudinal laceration into a transverse one in order not to slender the ureteral lumen (Heineke-Mikulicz procedure) and retroperitonealize if potential. This is truly because the patient is just too unstable to tolerate the operative time required to complete the restore (Cass, 1983). Some have instructed that in cases of severe hemorrhagic shock, uncontrollable intraoperative bleeding, or extreme colon damage (especially those requiring colectomy), ureteral reconstruction must be delayed till the affected person is totally resuscitated and carried out as a staged repair (Velmahos et al. The four choices for harm management in ureteral accidents are (1) do nothing, however plan a reoperation when the patient is extra steady, usually within 24 hours; (2) place a ureteral stent into the proximal end of the transected ureter and exteriorize the stent to the pores and skin; (3) mobilize and exteriorize the ureter, as in a cutaneous ureterostomy; or (4) ligate the ureter and plan a staged percutaneous nephrostomy (Hirshberg et al. In most cases of deliberate staged repair, we prefer to ligate the proximal finish of the broken ureter, utilizing lengthy silk or polypropylene ties to help the dissection of the ureteral stump during the second-stage repair. We advocate percutaneous (not intraoperative or intra-abdominal) placement of a nephrostomy tube, only once the patient has been fully stabilized and in a delayed trend. Open nephrostomy placement is simply too time-consuming and has no position in these unstable sufferers. Alternatively, a single-J stent or 5-Fr pediatric feeding tube may be placed into the proximal finish of the injured ureter, with minimal to no mobilization of the proximal ureter, a nonabsorbale tie placed across the proximal ureter to secure the stent in place, the stent, and the stent end externalized by way of the stomach wall into a urostomy pouch (Ball et al. If possible, appropriate planned ureteric reconstruction should be carried out after useful and anatomic imaging. Ureteral repair of traumatic injuries ought to be carried out on the time of initial laparotomy, when possible. Immediate restore, however, will not be acceptable in unstable, advanced polytrauma patients. Injuries found after this 1-week interval, must be managed by retrograde ureteral imaging with ureteral stent placement, percutaneous nephrostomy, or both, and definitive repair delayed until a minimal of 6 weeks after harm. This putatively avoids an inflammatory part, when ureteral repairs are thought to be much less reliable. Others suggest immediate repair even when discovered weeks to months, and cite low complication charges, just like accidents which would possibly be acknowledged immediately (Ghali et al. However, delayed prognosis of ureteral injury increase the complication rate of the restore significantly (Selzman and Spirnak, 1996), from 10% to 40% in a single series (Campbell et al. Some have suggested that delaying the restore (6 or extra weeks) avoids this threat by permitting for maximal resolution of perioperative irritation. A latest report suggests that even delayed repairs have a slightly higher price of failure than instant restore (Eswara et al. Most delayed recognized ureteral accidents, are found within 6 weeks of surgery (Hatch et al. Cure charges seem equal within the early (within 1 week) and late discovery teams (Brandt et al. Another study found no difference between repairs performed instantly, within 1 month, or at three months (Li et al. Ligation of the ureter discovered intraoperatively ought to be treated by removal of the ligature and remark of the ureter for viability. If viability is in question, ureteroureterostomy or ureteral reimplantation should be carried out (Assimos et al. Even if the ureter appears wholesome, a ureteral stent must be placed at minimum, both by opening the bladder or by instant cystoscopic placement. Injuries found instantly after nonaortic surgery are largely handled in the identical means as ureteral harm after exterior trauma. Most lacerations may be handled with ureteroureterostomy, though extra maneuvers such as omental wrapping of the repair or placement of an ipsilateral nephrostomy tube have been advocated to decrease the potential for urine leakage or breakdown of the repair (Adams et al.
Baycip 500mg overnight deliveryUltrasonography is a noninvasive and comparatively inexpensive modality that can differentiate cystic versus stable renal plenty symptoms zyrtec overdose generic baycip 500 mg without a prescription, and it continues to play an essential position for such lesions medicine vs engineering buy generic baycip 500 mg. Strict ultrasonographic criteria for easy cysts have been defined and include a clean cyst wall medications and mothers milk 2014 buy 500mg baycip with visa, a round or oval shape without inside echoes medicine 0829085 generic baycip 500 mg with mastercard, and through-transmission with sturdy acoustic shadowing posteriorly. Regardless of imaging modality used, imaging ought to comment on renal mass diameter in craniocaudal, transverse, and anterioposterior dimensions; tumor morphology, including involvement of or juxtaposition to the renal hilum, vein, or amassing system; enhancement characteristics; and related options similar to retroperitoneal lymphadenopathy and presence or absence of belly metastases. As discussed earlier, growing tumor size is the strongest predictor of malignant illness and subsequent metastatic potential (Pierorazio et al. Tumor location and complexity describe the connection of the mass with the renal hilum, accumulating system, polarity, and endophytic versus exophytic location. Emerging data indicate that growing tumor complexity may correlate with risk of malignancy and aggressive histology (Kutikov et al. Molecular imaging exploits existing mobile processes and highaffinity radio-labeled molecules to improve diagnostic imaging. Sestamibi is taken up by mitochondria, that are in abundance in oncocytomas and hybrid oncocytic/chromophobe tumors, and a robust signal is suggestive of those histologies. Simple cysts are thin-walled, fluid-filled constructions with a nearly zero threat of malignancy. The danger of malignancy will increase with cyst complexity as outlined by evaluation of the wall of the lesion; its thickness and contour; the quantity, contour, and thickness of any septa; the amount, character, and location of any calcifications; the density of fluid within the lesion; the margination of the lesion; and the presence of solid parts. These are by far the most typical renal cystic lesions, and within the absence of related symptoms, no therapy or surveillance is important. In the absence of a mitigating issue similar to renal trauma or infection, surgical exploration is normally indicated in wholesome patients with Bosniak three or 4 lesions (Campbell et al. Overall, approximately 16 new instances are identified per a hundred,000 inhabitants per yr, with a male-to-female predominance of 1. This is primarily a illness of older adults, with typical presentation between 55 and 75 years of age (Pantuck et al. However, analysis of renal most cancers has elevated extra rapidly in these less than forty years of age than some other age group (Nepple et al. Compared with Americans of other races, the incidence and demise rates are about 50% decrease in Asian-American/Pacific Islanders, and 5% to 10% greater in African-Americans, for unknown reasons (Chow et al. This trend has correlated with an increased proportion of incidentally discovered and localized tumors and with improved 5-year survival rates for sufferers with this stage of illness (Kane et al. This rising mortality fee is especially troubling as a result of the proportion of superior tumors has actually decreased (Decastro and McKiernan, 2008; Siegel et al. This means that a deleterious change in tumor biology may have occurred in the course of the past a quantity of many years, maybe associated to tobacco use, dietary components and obesity, or publicity to different carcinogens (Hock et al. As many as 15% of these tumors happen in children which have obtained chemotherapy for different malignancies (Brok et al. All types of tobacco use have been implicated, and risk will increase with cumulative dose or pack-years (Cote et al. Relative danger is directly associated to duration of smoking and begins to fall after cessation, further supporting a cause-and-effect relationship (Cumberbatch et al. The proposed mechanisms are hypertension-induced renal damage and inflammation or metabolic or useful adjustments in the renal tubules that may enhance susceptibility to carcinogens (Lipworth et al. The potential position of trichloroethylene publicity has been actively investigated; some studies showed relative risks ranging from twofold to sixfold, however others have argued that inherent biases doubtless account for these results (Kelsh et al. Other potential iatrogenic causes include regular utilization of nonsteroidal anti-inflammatory drugs, which was related to a relative risk of 1. Malignant Renal Tumors 2141 and in a unifocal method (Knudson, 1971; Knudson and Strong, 1972). All of those tumor sorts are highly vascular and may result in substantial morbidity. Penetrance for all of these traits is way from full, and some, such as pheochromocytomas, are probably to be clustered only in sure families (Table ninety seven. These research demonstrated a common loss of chromosome 3 in kidney cancer, particularly the clear cell variant, and led to intensive efforts to discover a tumor suppressor gene on this area (Seizinger et al. A massive number of frequent mutations or "sizzling spots" in the gene have been recognized, and a direct correlation between genotype and phenotype has been established in some instances (McNeill et al. The identification of this tumor suppressor gene represented a serious advance in the subject and required close collaboration between urologic oncologists and molecular geneticists (Schmidt and Linehan, 2016). Knudson and Strong recognized that familial forms of most cancers could maintain the key to the identification of important regulatory components generally recognized as tumor suppressor genes (Knudson, 1971; Knudson and Strong, 1972). Their observations about the childhood tumor retinoblastoma, in which familial cases are inclined to be multifocal and early onset, led them to propose a two-hit concept of carcinogenesis. They hypothesized that a gene product that might suppress tumor improvement have to be involved and that each alleles of this "tumor suppressor gene" should be mutated or inactivated for tumorigenesis to happen. Furthermore, Knudson postulated that sufferers with familial cancers are born with one mutant allele and that every one cells in that organ or tissue are at risk, accounting for the early onset and multifocal nature of the illness. Again, molecular linkage analysis in affected households played a key role in the discovery of the involved gene, which was localized to chromosome 7q31. However, in this case, the inciting occasion is activation of a protooncogene, rather than inactivation of a tumor suppressor gene. The protein product of this gene is the receptor tyrosine kinase for hepatocyte development issue, and its activation results in mobile proliferation and other potential tumorigenic results (Vira et al. These growth components are concerned with angiogenesis, glucose transport, and autocrine and paracrine development stimulation, respectively. Affected people present with bilateral, multifocal, early onset (<40 years) renal tumors, typically together with pheochromocytomas and head and neck paragangliomas. Tumors with high-grade, coagulative necrosis, or sarcomatoid features usually tend to behave aggressively (Gill et al. An autosomal dominant sample of inheritance is attribute and genetic testing is now obtainable (see Table 97. Microphthalmia-Associated Transcription Factor�Associated Cancer Syndrome A germline missense variant (p. Side results of immune modulators can include autoimmune diseases, such as enterocolitis, hepatitis, dermatitis, or pneumonitis, as anticipated by their mechanism of action (Choueiri et al. Suboptimal results with these formidable protocols suggested immune tolerance, doubtless induced by the tumor (Amin and White, 2013; Zibelman and Plimack, 2017). Under regular situations these receptors participate within the regulation of the immune system, essentially serving an inhibitory role to prevent autoimmune diseases from growing. Another mixture strategy, pembrolizumab plus axitinib, additionally appears to be energetic in untreated patients with metastatic kidney most cancers, as it demonstrated higher general survival when compared to sunitinib monotherapy, with profit observed in all risk teams (Rini et al. However, the promiscuity of the interactions between the various ligands, receptors, downstream effectors, and inhibitors can result in a wide selection of results that might be troublesome to predict. A scientific area of interest for bevacizumab when combined with interferon-alpha was outlined shortly thereafter (Escudier et al. Analyses carried out in this landmark research included nextgeneration sequencing to evaluate the entire genome of twenty-two tumors and whole-exome sequencing of 417 extra tumors. These checkpoint inhibitors thus can activate the T cells and bolster immune responses to the malignancy. Tumor dimension has averaged between four and 8 cm in most sequence however can differ from a quantity of millimeters to giant sufficient to fill the complete stomach.
Baycip: 500 mg
Purchase 500mg baycipLindsjo M medications blood thinners baycip 500mg fast delivery, Fellstrom B medicine daughter buy baycip 500mg low price, Ljunghall S medicine zofran discount baycip 500 mg on line, et al: Treatment of enteric hyperoxaluria with calcium-containing natural marine hydrocolloid symptoms for pneumonia buy baycip 500mg without a prescription, Lancet 2(8665):701� 704, 1989. Hugosson J, Grenabo L, Hedelin H, et al: Bacteriology of higher urinary tract stones, J Urol 143(5):965�968, 1990. Hylander E, Jarnum S, Nielsen K: Calcium treatment of enteric hyperoxaluria after jejunoileal bypass for morbid obesity, Scand J Gastroenterol 15(3):349� 352, 1980. Izzedine H, Launay-Vacher V, Deray G: Antiviral drug-induced nephrotoxicity, Am J Kidney Dis 45(5):804�817, 2005. Joly D, Rieu P, Mejean A, et al: Treatment of cystinuria, Pediatr Nephrol 13(9):945�950, 1999. Kato Y, Hou K, Saga Y, et al: Ammonium acid urate stone due to laxative abuse: a case report], Hinyokika Kiyo 50(11):799�803, 2004. Kessler T, Jansen B, Hesse A: Effect of blackcurrant-, cranberry- and plum juice consumption on risk factors related to kidney stone formation, Eur J Clin Nutr 56(10):1020�1023, 2002. Kisku S, Sen S, Karl S, et al: Bladder calculi in the augmented bladder: a follow-up study of a hundred and sixty youngsters and adolescents, J Pediatr Urol 11(2):sixty six, e1�e6, 2015. Koga S, Arakaki Y, Matsuoka M, et al: Staghorn calculi-long-term outcomes of management, Br J Urol 68(2):122�124, 1991. Ljunghall S: Incidence of upper urinary tract stones, Miner Electrolyte Metab 13(4):220�227, 1987. Mandel N, Mandel I, Fryjoff K, et al: Conversion of calcium oxalate to calcium phosphate with recurrent stone episodes, J Urol 169(6):2026�2029, 2003. Marangella M, Bianco O, Martini C, et al: Effect of animal and vegetable protein consumption on oxalate excretion in idiopathic calcium stone illness, Br J Urol 63(4):348�351, 1989. Marcus R, Madvig P, Crim M, et al: Conjugated estrogens within the therapy of postmenopausal women with hyperparathyroidism, Ann Intern Med 100(5):633�640, 1984. Meschi T, Maggiore U, Fiaccadori E, et al: the effect of fruit and veggies on urinary stone risk components, Kidney Int 66(6):2402�2410, 2004. Michelakakis H, Delis D, Anastasiadou V, et al: Ineffectiveness of captopril in reducing cystine excretion in cystinuric kids, J Inherit Metab Dis 16(6):1042�1043, 1993. Mohkam M, Karimi A, Gharib A, et al: Ceftriaxone associated nephrolithiasis: a potential examine in 284 youngsters, Pediatr Nephrol 22(5):690�694, 2007. Specific organ doses and efficient doses compared with renal stone protocol noncontrast computed tomography, Urology 83(2):282�287, 2014. Nordenvall B, Backman L, Larsson L, et al: Effects of calcium, aluminium, magnesium and cholestyramine on hyperoxaluria in sufferers with jejunoileal bypass, Acta Chir Scand 149(1):93�98, 1983. Nouvenne A, Meschi T, Prati B, et al: Effects of a low-salt diet on idiopathic hypercalciuria in calcium-oxalate stone formers: a 3-mo randomized controlled trial, Am J Clin Nutr 91(3):565�570, 2010. Ohkawa M, Tokunaga S, Nakashima T, et al: Thiazide remedy for calcium urolithiasis in patients with idiopathic hypercalciuria, Br J Urol 69(6):571� 576, 1992. Ortiz-Alvarado O, Miyaoka R, Kriedberg C, et al: Pyridoxine and dietary counseling for the administration of idiopathic hyperoxaluria in stone-forming patients, Urology 77(5):1054�1058, 2011. Polito C, La Manna A, Cioce F, et al: Clinical presentation and natural course of idiopathic hypercalciuria in youngsters, Pediatr Nephrol 15(3�4):211�214, 2000. Remien A, Kallistratos G, Burchardt P: Treatment of cystinuria with Thiola (alpha-mercaptopropionyl glycine), Eur Urol 1(5):227�228, 1975. Rivers K, Shetty S, Menon M: When and tips on how to evaluate a affected person with nephrolithiasis, Urol Clin North Am 27(2):203�213, 2000. Hyperparathyroidism and sarcoidosis, Urol Clin North Am 27(2):275�285, viii, 2000. Sakhaee K, Nicar M, Hill K, et al: Contrasting results of potassium citrate and sodium citrate therapies on urinary chemistries and crystallization of stone-forming salts, Kidney Int 24(3):348�352, 1983. Sakhaee K, Baker S, Zerwekh J, et al: Limited danger of kidney stone formation during long-term calcium citrate supplementation in nonstone forming subjects, J Urol 152(2 Pt 1):324�327, 1994. Sakhaee K: Epidemiology and medical pathophysiology of uric acid kidney stones, J Nephrol 27(3):241�245, 2014. Shavit L, Chen L, Ahmed F, et al: Selective screening for distal renal tubular acidosis in recurrent kidney stone formers: preliminary expertise and comparability Evaluation and Medical Management of Urinary Lithiasis 2068. Shuster J, Jenkins A, Logan C, et al: Soft drink consumption and urinary stone recurrence: a randomized prevention trial, J Clin Epidemiol 45(8):911�916, 1992. Siener R: Can the manipulation of urinary pH by beverages help with the prevention of stone recurrence Siener R, Bangen U, Sidhu H, et al: the role of Oxalobacter formigenes colonization in calcium oxalate stone disease, Kidney Int 83(6):1144�1149, 2013. Smith A: Evaluation of the nitroprusside take a look at for the diagnosis of cystinuria, Med J Aust 2(5):153�155, 1977. Clinical and laboratory traits of sufferers, Arch Intern Med 142(3):504�507, 1982b. Strong P, Jewell S, Rinker J, et al: Thiazide remedy and extreme hypercalcemia in a affected person with hyperparathyroidism, West J Med 154(3):338�340, 1991. Strumpf E: the weight problems epidemic within the United States: causes and extent, risks and solutions, Issue Brief (Commonw Fund) 713:1�6, 2004. Takei K, Ito H, Masai M, et al: Oral calcium supplement decreases urinary oxalate excretion in patients with enteric hyperoxaluria, Urol Int 61(3):192�195, 1998. A new genetic variant of primary hyperoxaluria, N Engl J Med 278(5):233�238, 1968. Yilmaz E, Batislam E, Kacmaz M, et al: Citrate, oxalate, sodium, and magnesium ranges in fresh juices of three several types of tomatoes: analysis in the light of the outcomes of studies on orange and lemon juices, Int J Food Sci Nutr 61(4):339�345, 2010. Zechner O, Kovarik J, Willvonseder R: Normocalcemic hyperparathyroidism, Eur Urol 7(6):327�330, 1981. Zee T, Bose N, Zee J, et al: alpha-Lipoic acid remedy prevents cystine urolithiasis in a mouse mannequin of cystinuria, Nat Med 23(3):288�290, 2017. Tefekli A, Cezayirli F: the history of urinary stones: in parallel with civilization, ScientificWorldJournal 2013:423964, 2013. Tekin A, Tekgul S, Atsu N, et al: Ureteropelvic junction obstruction and coexisting renal calculi in kids: role of metabolic abnormalities, Urology 57(3):542�545, discussion 545�546, 2001. Tosukhowong P, Yachantha C, Sasivongsbhakdi T, et al: Citraturic, alkalinizing and antioxidative results of limeade-based routine in nephrolithiasis patients, Urol Res 36(3�4):149�155, 2008. Trinchieri A, Nespoli R, Ostini F, et al: A study of dietary calcium and other vitamins in idiopathic renal calcium stone formers with low bone mineral content material, J Urol 159(3):654�657, 1998. Before the period of endourology, stones were removed by way of open stone surgical procedure, which offered high stone-free charges but was related to a excessive price of issues. More lately, in experienced arms, it has been demonstrated that laparoscopic and robotic-assisted renal stone surgical procedure may be safely used in chosen sufferers with good outcomes. In areas the place endourologic expertise is widely out there, open stone surgery is pursued only 1% of the time or less, and even in growing countries open stone surgical procedure rates have dropped dramatically from 26% to 3. Staged procedures of a given modality and combos of various modalities. The mixture of these components, availability of expertise and equipment, and familiarity of the urologist with the completely different surgical strategies in the end determines which therapy is most well-liked for a given patient.
Discount 500 mg baycip with mastercardEconomics of Metabolic Evaluation There is no doubt that the prices associated with the remedy of nephrolithiasis are substantial treatment rosacea cheap baycip 500 mg amex. Estimations of the annual medical expenditures for stone disease within the United States for 2000 have been $2 medicine man movie baycip 500mg line. With the rising incidence of stone illness treatment naive definition discount baycip 500 mg visa, it solely could be concluded that the nationwide well being care expenditure for urolithiasis will proceed to rise medicine 360 cheap 500mg baycip fast delivery. With these figures in thoughts, prudence would dictate that medical prevention could help curb runaway prices and forestall long-term sequelae of recurrent nephrolithiasis. However, office visits, serum research, and 24-hour urine studies have their very own costs. Is there a break-even point at which the prices of a metabolic evaluation, pharmacologic prophylaxis, and continued office visits are lower than the expense of surgical administration Chandhoke (2002) in contrast the value of medical prophylaxis with the price of clinically managing recurrent stone episodes. Additionally, he decided the stone recurrence rate without prophylaxis (stone frequency) at which these two remedy approaches became cost-equivalent. This review performed a price survey in 10 international locations to examine costs of medical prophylaxis and managing recurrent acute stone episodes. Not surprisingly, the costs of medical prophylaxis and managing an acute stone episode varied considerably from country to nation. The stone frequency at which costs of these management options became equivalent ranged from 0. Researchers on the University of Texas, Southwestern Medical Center have created a decision tree model to evaluate the cost-effectiveness and stone recurrence rates of frequent management methods in stone formers (Lotan et al. They evaluated 4 common medical methods: dietary measures alone (conservative), empirical drug remedy, or directed drug therapy based mostly on simple or complete metabolic evaluation. The model made cheap assumptions concerning prices for evaluation, medications, emergency therapy, and surgery for stone recurrence. A evaluate of the literature guided estimations of stone recurrence and risk reduction from varied medical therapies. They discovered that first-time stone formers had been finest treated with a conservative strategy as a end result of it was the least costly and it yielded a stone formation price of zero. For recurrent stone formers, conservative therapy was less costly than drug remedies but it was associated with the next stone recurrence price (0. Directed medical therapies had been extra pricey than conservative treatment ($885 to $1187 vs. The authors went on to examine the expense of the straightforward medical analysis and associated administration as described earlier in this chapter and famous it to be extra pricey than empirical therapy but additionally more practical. Importantly, a complete evaluation with attendant remedy supplied no benefit in value or efficacy over empirical therapy or modified easy metabolic analysis and management. In distinction, however, recurrent stone formers should be treated medically after a simplified analysis, because of the excessive recurrence price of stone formation. In some instances, a stone analysis may be extra practical to get hold of than a 24-hour urine assortment, and in other instances it can function a useful adjunct to serum and urine metabolic evaluation. They also recommend repeating stone evaluation within the occasion further stones are available, notably if not responding to remedy as stones are identified to range in composition from occasion to event. Because most stones are a mixture of a couple of component, the relative ratios or predominance of any explicit molecule may have predictive value (Table ninety two. In an evaluation of almost 1400 patients who had both stone analysis and a whole metabolic analysis, Pak et al. As expected, a really sturdy association was discovered between infection stones and an infection and between cystine stones and cystinuria. They additionally identified the potential for calcium oxalate stone formers to convert to calcium phosphate stone formers (Parks et al. Although the precise mechanism for this alteration stays unclear, acidification defects from prior shock wave lithotripsy and citrate supplementation have been postulated to be contributing factors (Parks et al. The two most generally recommended and utilized methods are x-ray diffraction or Fourier-transform infrared spectroscopy (Gilad et al. Inaccuracies in struvite and calcium phosphate have been recognized as particularly difficult (Krambeck, 2010b). One potential cause is the heterogeneity and lack of quality-control standards and best-practice policies for testing. An evaluation of stone evaluation laboratories across Europe recognized solely 56% as meeting quality necessities (Siener et al. Once the stone is destroyed, the opportunity to evaluate the microstructure and different compositions relative to each other is misplaced. There is increasing recognition that such information may present extra useful info than previously acknowledged. Gross morphologic analysis of stones has been advised to assist elucidate the etiology of stone formation, and a morphologic classification system has been previously described by Daudon et al. This system, which features 6 main forms of stones and 22 subtypes, has proved superior to stone composition alone in predicting the chance of stone recurrence. Notably, the speed of such stones elevated significantly over three a long time and was associated with youthful age of onset, greater serum ionized calcium ranges, and increased serum osteoclasts providing potential perception into the rising prevalence of stone disease (Letavernier et al. Different data can be obtained from the results of stone evaluation, evaluation of serum chemistries, and outcomes of 24-hour urine testing. There can be growing interest and investigation in utilizing endoscopic appearances of the renal papillae as a way to classify sufferers (Almeras et al. On the top proper picture, the plaque demonstrates several small cylindrical empty areas indicative of peritubular calcification within the papillary interstitium over which stones can form. On the bottom proper determine, a extra dense mineral accumulation has shaped by way of accretion and layering forming a ductal plug of calcium phosphate over which a stone could develop. The scientific rationale and physiologic processes by which these abnormalities result in stone formation may be present in Chapter ninety one. Evaluation and Medical Management of Urinary Lithiasis 2047 General Recommendations for Stone Formers Certain conservative recommendations must be made for all patients whatever the underlying cause of their stone disease. The results counsel that preventive measures centered on these components might substantially lower the burden of kidney stone disease. Fluid Recommendations Low urine quantity is maybe crucial risk factor for kidney stone formation. Increased fluid consumption is a strong software in stopping stone recurrence for all stone sorts and sure does so by way of a decrease in urinary supersaturation of stone elements (Pak et al. In a randomized controlled trial of idiopathic calcium oxalate stone formers, Borghi et al. High fluid intake has additionally been found to be protecting in relation to stone formation in several giant prospective observational studies. Furthermore, researchers on the University of Chicago demonstrated that failure to improve urine output was one of three very sturdy predictors of relapse for patients adopted in a devoted stone clinic (Strauss et al. Therefore, a mainstay of conservative administration for kidney stone prevention is elevated fluid consumption to obtain a urine output of no less than 2. The financial influence of accelerating fluid consumption to decrease stones has also been considered.
San-Qi Ginseng (Panax Pseudoginseng). Baycip. - Dosing considerations for Panax Pseudoginseng.
- How does Panax Pseudoginseng work?
- Are there safety concerns?
- Bleeding, improving blood flow, pain, swelling, high cholesterol levels, chest pain (angina), high blood pressure, dizziness, sore throat, prostate cancer, and other conditions.
- What is Panax Pseudoginseng?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96872
Order 500mg baycip mastercardMazdak H symptoms quad strain generic baycip 500 mg overnight delivery, Meshki I symptoms ear infection generic baycip 500 mg without a prescription, Ghassami F: Effect of mitomycin C on anterior urethral stricture recurrence after inner urethrotomy symptoms knee sprain buy baycip 500 mg amex, Eur Urol fifty one:1089�1092 medications prescribed for ptsd purchase baycip 500mg free shipping, 2007. Accurate radiological localization of the membranous urethra and distal sphincters in regular male subjects, J Urol 122:607�611, 1979a. Indications for transsphincter urethroplasty in patients with primary bulbous strictures, J Urol 122:612�618, 1979b. Memmelaar J: Use of bladder mucosa in a one stage restore of hypospadias, J Urol fifty eight:68�73, 1947. Meuli M, Briner J, Hanimann B, et al: Lichen sclerosus et atrophicus inflicting phimosis in boys: a potential research with 5-year follow-up after full circumcision, J Urol 152:987�989, 1994. Milroy E, Allen A: Long-term results of UroLume urethral stent for recurrent urethral strictures, J Urol one hundred fifty five:904, 1996. Milroy E: Treatment of sphincter strictures utilizing everlasting UroLume stent, J Urol 150:1729�1733, 1993. Report of three instances with description of corrective operation, J Urol ninety three:230�232, 1965. Orticochea M: the musculo-cutaneous flap technique: an immediate and heroic substitute for the strategy of delay, Br J Plast Surg 25:106�110, 1972. Ozgok Y, Seckin B, Demirci S, et al: Surgical remedy of urethral diverticula in men, Scand J Urol Nephrol 28:207, 1994. Pansadoro V, Emiliozzi P: Internal urethrotomy within the administration of anterior urethral strictures: long-term followup, J Urol 156:73�75, 1996. Pavlica P, Barozzi L, Menchi I: Imaging of male urethra, Eur Radiol thirteen:1583� 1596, 2003. Important technical concerns and new applications, J Pediatr Surg 17:796�811, 1982. Pe�a A, Hong A: the posterior sagittal trans-sphincteric approach, Acta Chir Iugosl fifty one:11�21, 2004. Perovic S, Scepanovic D, Sremcevic D, et al: Epispadias surgery-Belgrade expertise, Br J Urol 70:674�677, 1992. Ponten B: the fasciocutaneous flap: its use in delicate tissue defects of the lower leg, Br J Plast Surg 34:215�220, 1981. Ramsey G: Appendix B: requirements of care: the hormonal and surgical intercourse reassignment of gender dysphoric persons. Rehman J, Samadi D, Ricciardi R Jr, et al: Early endoscopic realignment as major remedy for complete posterior urethral disruptions, J Endourol 12:283�289, 1998. Rotariu P, Yohannes P, Alexianu M, et al: Reconstruction of rabbit urethra with Surgisis small intestinal submucosa, J Endourol 16:617�620, 2002. Rousseau H, Puel J, Joffre F, et al: Self-expanding endovascular prosthesis: an experimental examine, Am J Radiol 164:709, 1987. Tuffanelli D: Do some patients with morphea and lichen sclerosus et atrophicus have a Borrelia an infection Vanni A, Buckley J, Zinman L: Contemporary management of rectourethral fistulas: 10-year expertise, J Urol 181:421�422, 2009. Walzer Y, Bear R, Colapinto V, et al: Localized amyloidosis of urethra, Urology 21:406�407, 1983. Weinberg G, Williot P, Leonard M: the utility of buccal mucosa graft in salvage urethroplasty, Can J Urol 9:1641�1645, 2002. Wessells H: Cost-effective approach to quick bulbar urethral strictures supports single inside urethrotomy earlier than urethroplasty, J Urol 181:954�955, 2009. Yachia D, Beyar M: Temporarily implanted urethral coil stent for the treatment of recurrent urethral stricture: a preliminary report, J Urol 146:1001�1004, 1991. Schreiter F, Noll F: Mesh graft urethroplasty using split thickness skin graft or foreskin, J Urol 142:1223�1226, 1989. Sigwart U, Puel J, Miarkovitch V, et al: Intravascular stents to stop occlusion and restenosis after transluminal angioplasty, N Engl J Med 316:701, 1987. St�hmer A: Balanitis xerotica obliterans (post operationem) und ihre beziehungem zur Kraurosis glandis et preaeputii, Penis Arch Derm Syph (Berlin) 156:613�623, 1928. Knowledge of scrotal wall anatomy allows safer access into the scrotum for widespread scrotal procedures, facilitates identification of surgical planes during surgical debridement, and permits for multilayer closures. The scrotal pores and skin is rugated because of its underlying attachment to the dartos muscle, deeply pigmented, and hair-bearing. In contrast with different components of the physique, the scrotum is elastic and highlytemperature regulated to allow spermatogenesis. Scrotal Contents Scrotal contents are maintained of their place inside the scrotal cavity by the spermatic twine and gubernacular attachments. The testicle is intimately encased by the tunica albuginea, and guarded by the layers of tunica vaginalis, inside and exterior spermatic fascia (separated by a layer of cremasteric muscle), and in the end coated by the dartos layer and scrotal pores and skin. The epididymis originates from the efferent ducts of the rete testis in mediastinum testis. It is positioned along the posterolateral facet of the testis, with its head (caput) positioned superiorly, the physique (corpus) alongside the longitudinal axis of the testis, and the tail (cauda) on the inferior testicular pole. Two nonfunctional, vestigial buildings could also be encountered within the scrotum: the appendix testis over the upper pole of the testis and the appendix epididymis attached to the head of the epididymis. Although nearly all of the blood supply (~84%) to the epididymis comes from the superior epididymal artery, the superior epididymal artery may be sacrificed to gain additional testicular mobilization throughout vasectomy reversal because of the vascular anastomoses between the superior and inferior epididymal artery (Strittmatter and Konrad, 1989). Understanding the blood supply to the epididymides is essential within the surgical remedy of epididymal illness. Cranially, thin-caliber anastomoses are often current within the spermatic cord between the testicular artery and the deferential artery roughly 10 cm above the testis (Strittmatter and Konrad, 1989). At the extent of the cauda of the epididymis, anastomoses type between the testicular artery, deferential artery, and cremasteric artery. This redundancy of blood supply to the testis permits viability of the testis if one or two of the arteries are injured or ligated. Three teams of converging autonomic nerve fibers contribute to the autonomic innervation of the testes: (1) superior spermatic nerves, from the renal and mesenteric plexi, which comply with the testicular artery, (2) middle spermatic nerves, from the superior hypogastric plexus, which journey adjoining to the vas as it enters the interior spermatic ring, and (3) inferior spermatic nerves, which originate from the inferior hypogastric plexus (Patel, 2017). The inferior spermatic nerve fibers fuse with the middle spermatic nerve fibers at the prostate-vesical junction, run inside the spermatic wire along the vas deferens, and ultimately penetrate the epididymis and testis (Sosa et al. In addition to the sensory fibers contained within the autonomic spermatic nerves, afferent fibers of these nerves are additionally necessary in the endocrine control of the testis. The scrotum is also innervated by somatic nerves, including ilioinguinal and genitofemoral nerves. The genital branch of the genital femoral nerve is positioned on the inferolateral side of the spermatic cord and innervates the anterolateral scrotal pores and skin, the tunica vaginalis, and the cremaster muscular tissues (Ducic and Dellon, 2004; Zorn et al. In distinction, the ilioinguinal nerve sits on the anterior of the cremasteric muscular tissues and innervates the anterior scrotal skin (Wijsmuller et al. An understanding of the course of these nerves is necessary in scrotal denervation procedures, that are mentioned later on this chapter. Vasculature the scrotum is very vascularized, with blood provide provided anteriorly from the superficial external pudendal artery and deep exterior pudendal artery, and posteriorly from the posterior scrotal artery. Venous drainage follows the arterial provide draining into the external pudendal vein and posterior scrotal vein, which empty into the nice saphenous vein and to the internal iliac veins, respectively.
Baycip 500 mg with mastercardRenal papilla in a calcium oxalate stoneformer (A) where a quantity of Randall plaques (arrows) appeared as irregular white areas beneath the urothelium; the plaque web site missing a urothelial layer (arrowhead) may be the web site the place the stone was attached to papilla medicine woman buy 500 mg baycip visa. Renal papilla in a non�stone former (B) the place no distinct sites of Randall plaques were famous on papilla but a nodular-appearing construction (arrowhead) was famous alongside the papilla medications made from animals generic 500mg baycip otc. Three layers separate the filtered blood from the Bowman house: a single layer of endothelial cells medicine zolpidem generic baycip 500 mg with amex, a thin glomerular basement membrane medicine engineering order 500mg baycip mastercard, and a layer of podocytes on the other side of that basement membrane. The proximal and distal convoluted tubules and the loop of Henle are lined by a single layer of cubical epithelial cells. The cells lining the amassing ducts are cubical to columnar and are extra resistant to injury than these of the renal tubules. The calyces, pelvis, ureters, bladder, and urethra are lined by transitional epithelium, the urothelium, which may change and give rise to a transitional cell carcinoma of the urinary tract or urothelial carcinoma. The medullary areas are pyramidal, more centrally positioned, and separated by segments of cortex, the columns of Bertin. Both kidney shadows are clearly visible and can be assessed with regard to their place and morphology. The psoas muscle line may be appreciated; it disappears with retroperitoneal effusions. In gray-scale ultrasonography, the renal cortices of newborn kidneys are isoechoic or hyperechoic to the liver and splenic parenchyma, due to the presence of loops of Henle and proportionately higher quantity of glomeruli in the cortex than in adults (Hricak et al. However, renal cortices and pyramids are often hypoechoic to the liver, spleen, and renal sinus. Compared with renal size, cortical thickness, or parenchymal thickness, cortical echogenicity correlates strongly with severity of pathologic modifications in renal parenchyma, such as glomerular sclerosis, tubular atrophy, interstitial fibrosis, and irritation (r = zero. However, this correlation coefficient is still low with subsequent poor predictive value of renal echogenicity. In Quaia E, editor: Radiological imaging of the kidney (medical radiology/diagnostic imaging), New York, 2011, Springer, pp 17�78. T1-weighted sequences show the renal cortex a lot brighter than the renal medulla, whereas the cortex is slightly less intense than the medulla on T2-weighted sequences. The renal pelvis containing fats seems hyperintense on T1- and T2-weighted sequences. Renal cortex and medulla carry out totally different physiologic functions and are affected by completely different pathophysiologic processes. Therefore assessment of the degree of separation between these two compartments by imaging research is necessary. Renal ultrasonography and Doppler interrogation in a 65-year-old affected person with poorly controlled hypertension. Chapter eighty four Surgical, Radiologic, and Endoscopic Anatomy of the Kidney and Ureter 1869 with persistent kidney disease and acute kidney injury, with out clear correlation with the level of serum creatinine (Semelka et al. Studies using custom-made imaging software have demonstrated a high correlation between measurements of renal and cortical volumes and renal operate (Coulam et al. Of all congenital anomalies encountered in newborns, 20% to 30% have an effect on the kidneys and ureters (Schedl, 2007). Radiologically, renal malrotation is identified because the renal pelvis seems to arise centrally instead of its medial origin from the kidney. Some calyces are located medial to the renal pelvis, a trademark of rotational anomalies. Arrest or exaggeration of normal ascent of the kidneys provides rise to renal ectopia and is usually related to malrotation. Despite the ureteral size being applicable for the kidney place, the impaired drainage leads to urinary stasis and increased chances of an infection and stone formation. A kidney could cross the midline and fuse with the other kidney (crossed-fused ectopia). The ureter from the ectopic decrease kidney crosses the midline and normally inserts into the bladder in its regular position. It is often positioned low within the abdomen due to its arrest by the origin of the inferior mesenteric artery. Renal arteries give branches to the adrenal glands, renal pelves, and proximal ureters. Therefore occlusion or damage to a segmental department causes segmental renal infarction. Nevertheless, the world provided by every segmental artery could be independently surgically resected. The anterior division supplies roughly the anterior two-thirds of the kidney, and the posterior division provides the posterior one-third of the kidney. Typically, the anterior division divides into 4 anterior segmental branches: apical, higher, center, and lower. The posterior segmental artery represents the first and most fixed department, which separates from the renal artery earlier than it enters the renal hilum. A small apical segmental branch might originate from this posterior department, however it arises most commonly from the anterior division. The posterior segmental artery from the posterior division passes posterior to the renal pelvis while the others pass anterior to the renal pelvis. In 25% to 40% of kidneys, anatomic variations in the renal vasculature have been reported. Supernumerary renal arteries are the most typical variation, with reports of as a lot as five arteries, especially on the left side. The primary renal artery could manifest early branching after originating from the belly aorta and before coming into the renal hilum. These prehilar arterial branches should be detected in sufferers present process evaluation for donor nephrectomy. An accessory renal artery may come up from the aorta, between T11 and L4, and terminate within the kidney. Rarely, it might also originate from the iliac arteries or superior mesenteric artery. Accessory renal arteries are seen in 25% to 28% of sufferers and are thought-about the only arterial supply to a selected portion of the renal parenchyma, generally the decrease and occasionally the upper pole of the kidney. Multiple renal arteries that arise from the aorta or iliac arteries are frequently seen in horseshoe and pelvic kidneys. There is a longitudinal avascular aircraft (line of Brodel) between the posterior and anterior segmental arteries just posterior to the lateral facet of the kidney by way of which incision results in significantly much less blood loss. However, this airplane could have varied areas that necessitate its delineation earlier than incision either by preoperative angiography or intraoperative segmental arterial injection of methylene blue. For example, during percutaneous entry into the kidney, posterior calyces alongside the road of Brodel are most well-liked. Furthermore, during anatrophic nephrolithotomy (Boyce procedure), an incision is made through this avascular plane.
Buy generic baycip 500mg on-lineOncologic occasions were uncommon medicine 6mp medication generic 500mg baycip otc, as anticipated for small renal masses symptoms uterine cancer cheap baycip 500 mg with visa, and related in both groups medicine to help you sleep buy 500 mg baycip. This trial had substantial flaws and most thought leaders in the area have most well-liked to dismiss the first findings of the research 911 treatment center discount 500mg baycip. Controversy has arisen relating to the routine want for many of these practices (Lam et al. An extraperitoneal flank incision could also be applicable in elderly patients or patients of poor surgical risk, but exposure may be limiting, significantly for big tumors or these with contentious hilar anatomy (Diblasio et al. In actuality, many of those sufferers are actually managed with a minimally invasive approach in this period. Morbidly overweight sufferers, these with a historical past of previous abdominal surgical procedure, and people with large tumor size may also be considered for minimally invasive renal surgery, though number of sufferers should be even handed and surgical expertise and experience should also be taken into consideration (Campbell et al. Partial Nephrectomy Nephron-sparing surgery for the treatment of renal tumors was first described by Czerny in 1890, however this approach was occasionally used until the Nineteen Eighties (reviewed in Herr, 2005). Laparoscopic radical nephrectomy (a retroperitoneal strategy is illustrated) supplies wonderful oncologic outcomes and rapid recovery but predisposes sufferers to continual kidney illness. Patients not meeting these standards should be thought of for partial nephrectomy if feasible. Margin width appears to be immaterial as lengthy as the ultimate margins are adverse; that is significantly related when the tumor is situated throughout the hilum and preservation of renal operate is at a premium (Bensalah et al. A functioning renal remnant of no much less than 20% to 30% of 1 kidney is important to keep away from end-stage renal failure, although this presumes good functional standing of the remaining parenchyma (Uzzo and a Please additionally discuss with Table ninety seven. Renal transplantation may be an choice for a few of these sufferers after an acceptable cancer-free interval. Essential steps in traditional partial nephrectomy as illustrated with open method. Nevertheless, this strategy should only be used when really necessary-upfront surgical procedure should be prioritized every time feasible (Dey et al. Nevertheless, most such complications are readily manageable with conservative measures (Campbell et al. The quality of the parenchyma is for the most half nonmodifiable, basically setting the ceiling for functional restoration after any intervention. Stated one other means, as lengthy as prolonged warm ischemia is avoided, most nephrons will recover from the ischemic insult (Kallingal et al. Precise excision of the tumor with a small rim of regular parenchyma along with careful reconstruction of the kidney to minimize devascularization is paramount and could be facilitated by a brief ischemic interval to allow for a cold subject (Bahler et al. The quality and amount of preserved parenchyma are the primary determinants of renal perform after partial nephrectomy, with ischemic damage playing a secondary role so long as restricted warm ischemia or hypothermia is used. Prolonged warm ischemia, nonetheless, can lead to irreversible lack of nephron operate. However, different strategies and views, such as the concept of segmental arterial clamping (Desai et al. These protocols ought to help reduce costs, radiographic publicity, and patient inconvenience whereas still permitting for detection of most clinically relevant recurrences (Donat et al. Development of proteinuria correlated directly with the size of follow-up and inversely with the quantity of remaining renal tissue. Efforts to ameliorate the damaging effects of renal hyperfiltration have centered on dietary and pharmacologic interventions, primarily the use of angiotensin-converting enzyme inhibitors along with a low-protein food plan (Goldfarb, 1995; Novick and Schreiber, 1995). The fundamental idea is captured within the latter side of the adage, "hold your mates shut, and your enemies closer. A current advice has been to standardize recording of the resection technique (enucleation versus standard resection, versus enucleoresection, which is a hybrid of the other two) based on visual inspection of the ultimate gross pathologic specimen. Beyond Chapter ninety seven this overriding principle, the Guidelines state that "the extent of normal parenchyma eliminated must be decided by surgeon discretion considering the medical situation; tumor characteristics including development pattern, and interface with normal tissue" (Campbell et al. Both can be administered percutaneously and thus supply the potential for decreased morbidity (Campbell et al. Overall survival is primarily determined by age and common well being standing, not method to administration. Tumor dimension is one other necessary think about affected person selection because success rates seem to be highest for tumors smaller than 2. Established stipulations for profitable cryosurgery embrace speedy freezing, gradual thawing, and a repetition of the freeze-thaw cycle. The mechanism of motion consists of instant membrane and cellular injury adopted by microcirculatory failure and ischemia (Zondervan et al. Intracellular ice irreversibly disrupts cellular organelles and the cell membrane, and delayed microcirculatory occlusion ultimately leads to cellular anoxia. Complete and reliable tissue necrosis with cryoablation is constantly achieved solely at temperatures of -19. Risk ratios with 95% confidence intervals are proven for each research and for the general evaluation. Thus, to ensure full cell kill, the iceball should extend nicely beyond the visible margins of the focused tumor. In follow, we routinely prolong the iceball approximately 1 cm beyond the sting of the tumor, as decided by real-time imaging (Gill et al. The availability of sophisticated ultrasonography and introduction of finer cryoprobes that enable for more correct and less traumatic probe placement have contributed to improved efficacy and security of visceral cryosurgery (Sterrett et al. Further details about methods required to obtain optimum outcomes with cryoablation can be found in Chapter 103. Clinical experience after major renal cryoablative therapy suggests successful local control in about 80% to 90% of patients, although many studies present solely limited follow-up (Campbell et al. However, only a minority of studies have included routine post-therapy biopsies to present histologic affirmation of oncologic standing (Gill et al. Other findings that counsel local recurrence embody a progressive enhance in measurement of an ablated neoplasm, new nodularity in or across the handled zone, failure of the treated lesion to regress over time, or satellite tv for pc or port site lesions (Donat et al. If these features are found, biopsy and possible retreatment should be considered. Most native recurrences could be salvaged with repeat ablation, although some sufferers with progressive disease ultimately require standard surgical procedure. Complications related to cryoablation can include renal fracture, hemorrhage, adjoining organ injury, ileus, and wound infection, although major morbidity is decidedly uncommon presuming good patient selection (Sidana et al. These results are observed at tissue temperatures above 41�C however improve immediately with increasing temperature and period of remedy. Temperatures in excess of 100�C are sometimes obtained on the suggestions of the probes, although this quickly dissipates additional away from the tip. Multiple probes or tines are thus sometimes required to achieve adequate heating of the entire region of interest, and thermosensors can be used to monitor progress, no much less than in areas of concern (Chang et al. Rather, therapy is primarily based on empirical outcomes from previous probe alignments, supplemented by knowledge from strategically positioned thermoprobes when necessary (see Chapter 103). Again, most native recurrences can be salvaged with repeat ablation, and cancer-specific survival remains excessive (Campbell et al.
Baycip 500 mg visaEven with light method symptoms kidney disease purchase baycip 500 mg otc, extravasation during retrograde urethrography is feasible in patients in whom the urethra is markedly infected medications hyperkalemia baycip 500 mg without a prescription. Real-time ultrasound analysis of the urethra after it has been full of a lubricating jelly or saline has been described by Morey and McAninch (1996a symptoms 4 days after conception baycip 500 mg with amex, 1996b) treatment 4s syndrome generic baycip 500 mg overnight delivery. Morey and McAninch (1996a, 1996b) believed that ultrasonography of the bulbous urethra probably more accurately determines the size of the stricture, which might be necessary in contemplating an anastomotic repair. Finally, during contrast-enhanced urethrography, a couple of projection could also be necessary to visualize the stricture. Series of radiographs demonstrating the usefulness of the mix of contrast enhancement with endoscopy. In some sufferers, the urethra proximal to a narrow area could remain confusing with regard to its potential for continued constriction after reconstruction. Decision Making Once the stricture and patient specifics have been evaluated, the next step in the decision-making algorithm is figuring out if remedy is to be palliative or healing. The evaluation and decision-making algorithm in urethral stricture surgery is based upon several major factors. First, the surgeon ought to have a good understanding of the function of radiologic and endoscopic evaluations to totally characterize the anatomy of the stricture. Second, he or she ought to be acquainted with the out there strategies and their makes use of and limitations. Last, affected person and surgeon should agree upon a desired consequence of any intervention and perceive the long-term goals and expectations. In the past, an idea often identified as the reconstructive ladder was used as a treatment guideline for urethral strictures. That idea was based mostly on the principle that the simplest procedure ought to all the time be tried first, and typically repeated after failure, earlier than moving on to more complex approaches. The patient and the physician should have an excellent understanding of the goal of therapy before the therapy choice is made. Treatment options ought to be discussed with the affected person, with care taken to emphasize the anticipated consequence with regard to potential treatment. Some sufferers might prefer stricture administration and choose to have periodic dilations within the office, at home, or in the hospital quite than bear technically detailed open surgical procedure. Many surgical procedures at present have short-term and midterm results approaching long-term success charges of more than 90% to 95% for a lot of strictures. Dilation Urethral dilation is the oldest and simplest remedy of urethral stricture illness, and for a affected person with an epithelial stricture without spongiofibrosis, it may be healing. If bleeding occurs during dilation, the stricture has been torn quite than stretched, possibly further injuring the involved area. The least traumatic technique to stretch the urethra is to use gentle strategies over a quantity of therapy classes. In addition, the literature is unclear concerning the aim of inner urethrotomy. In many cases, inner urethrotomy has been reported as profitable although it has been related to eventual stricture recurrence. The variables related to success of internal urethrotomy have been verified by different research (Heyns et al. Many studies have shown that the success of reconstruction is diminished by multiple prior urethral dilations and inside urethrotomy (Albers et al. Numerous analyses have sought to compare the price effectiveness of the practice of inside urethrotomy initially before consideration of open reconstruction. The analyses differ in methodology and in findings (Rourke and Jordan, 2005; Wessells, 2009; Wright et al. Several methods have been employed to oppose the method of wound contraction and to forestall stricture recurrence. One method is to depart an indwelling Foley catheter for six weeks after urethrotomy in the hope that the urethra will mould around the catheter as it heals. However, studies have shown that the failure rate of long-term catheterization after inner urethrotomy is similar to that seen with 3 to 7 days of catheterization, and even 6 weeks is inadequate time to oppose the forces of wound contraction. Another method used to oppose the forces of wound contraction after inside urethrotomy is home self-catheterization or residence urethral obturation. After inside urethrotomy, sufferers generally have an indwelling catheter placed for three to 5 days. When the catheter is removed, the patient is started on a urethral obturation regimen. Most regimens require extra frequent catheterizations early within the recovery period, with a tapering schedule through the next 3 to 6 months. Anecdotally, many surgeons have reported an improved remedy rate with self-catheterization combined with internal urethrotomy. However, it has been our experience that the stricture inevitably recurs when the affected person stops self-obturation, regardless of how lengthy it has been used. Colchicine, because it binds tubulin, has been used along with inner urethrotomy (Carney et al. Initial findings in a nonrandomized examine also recommend that, maybe by pharmacologically blocking tubulin and probably wound contracture, the outcomes of inside urethrotomy may be higher. Mitomycin C with its antifibroblast and anticollagen activity when injected submucosally has been shown to lower the chance of recurrence after a urethrotomy (Mazdak et al. These catheters could also be attached to a filiform tip or handed over a guidewire or could include an integral coud� tip. For preliminary dilation, we favor the use of balloons positioned over wires which have been handed through the stricture under endoscopic control. Dilation can be curative and, within the literature, in accurately chosen sufferers, has short-term and midterm efficacy rates equal to inner urethrotomy. Selection standards are discussed in the following part on inside urethrotomy. Internal Urethrotomy Internal urethrotomy refers to any process that opens the stricture by incising it transurethrally. The urethrotomy procedure includes incision via the scar to wholesome tissue to enable the scar to expand (release of scar contracture) and the lumen to heal enlarged. The aim is for the resultant larger luminal caliber to be maintained after healing. In healing by secondary intention, epithelialization progresses from the wound edges. In an effort to aid epithelialization, nature invokes the forces of wound contraction, to not be confused with scar contraction. Wound contraction closes the wound defect and limits the size of the world that requires epithelialization, hastening the therapeutic of the floor defect. However, in the case of inner urethrotomy, wound contraction merely tries to reapproximate the edges of the scar, placing a race into effect.
References - Weisfeldt ML, Scully HE, Frederiksen J, et al: Hemodynamic determinants of maximum negative dP/dt and periods of diastole, Am J Physiol 227:613-621, 1974.
- Fabri M, Stenger S, Shin DM, et al. Vitamin D is required for IFN-c-mediated antimicrobial activity of human macrophages. Sci Transl Med 2011; 3: 104ra102.
- Camargo CA Jr., Stampfer MJ, Glynn RJ, et al: Prospective study of moderate alcohol consumption and risk of peripheral arterial disease in U.S. male physicians, Circulation 95:577, 1997.
- Gattinoni L, et al. A trial of goal-oriented hemodynamic therapy in critically ill patients. SvO2 Collaborative Group. N Engl J Med. 1995;333:1025-1032.
|