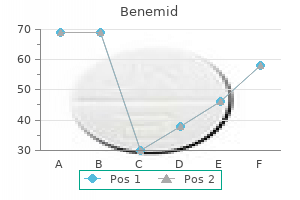
Benemid
Natalie E. Lyter, BS, MT(ASCP)SH - Instructor
- Medical Laboratory Technician Program
- Harrisburg Area Community College
- Health Career Department
- Harrisburg, Pennsylvania
Buy benemid 500mg otcFinally midsouth pain treatment center cordova tn buy 500mg benemid fast delivery, if ophthalmoplegia is related to retinal degeneration neck pain treatment physiotherapy generic 500 mg benemid amex, one ought to suspect a major muscle disease allied pain treatment center ohio discount benemid 500 mg otc. This dysfunction was thought by many to symbolize a major myopathy because of the typical histologic appearance of skeletal muscle biopsies from affected people pain treatment in osteoporosis order 500mg benemid. When it was acknowledged that the ragged-red fibers had been attributable to accumulations of abnormal mitochondria inside the myofibers, it became obvious that any cell dependent on cardio metabolism might be affected. Presumably, many ailments remain to be identified and characterized given the myriad of metabolic functions offered by mitochondria. Abnormal mitochondria with cristae forming concentric membranous rings accrued in the myocardium of a patient with Kearns�Sayre syndrome (42 000). The medical presentation of the mitochondrial cytopathies is varied, with appreciable overlap among syndromes. Note the subsarcolemal accumulation of mitochondria similar to the red staining in modified trichrome. Ptosis is often followed within a few years by progressive exterior ophthalmoplegia. The ophthalmoplegia is often symmetric, affecting each horizontal and upward gaze; downward gaze is commonly spared. Even in these patients who develop incomitant strabismus, diplopia is uncommon because of the slowly progressive nature of the ophthalmoplegia. Excessive accumulation of triglyceride droplets may histopathologically mimic lipid storage diseases. Similar morphologic adjustments could additionally be seen within the numerous muscular dystrophies, polymyositis, and dermatomyositis. The ptosis may appear to worsen as the outcomes of progressive weak spot of the frontalis muscle. Weakness of the arms, legs, and muscular tissues of mastication might mimic myasthenia gravis. In 1958 Kearns and Sayre described two patients with chronic progressive ophthalmoplegia, atypical retinitis pigmentosa, and complete heart block. A higher concentration of mitochondria in extraocular muscles than in other skeletal muscular tissues might account for the predominance of ocular motility issues in this disease. Electroretinography is usually normal or reveals mildly attenuated a- and b-wave amplitudes. Unfortunately, coronary heart failure due to congestive cardiomyopathy with out conduction defects can also develop. This may be due to as but undetected point mutations or deletions too small to detect with typical restriction fragment evaluation methods. The numerous stories of paternal and autosomal dominant transmission support this hypothesis. All three might current with ptosis and facial weak spot, but are otherwise easily distinguishable by their inheritance and clinical characteristics (Table 294. Vitamin E Deficiency Vitamin E deficiency results in diffuse damage to neurons and muscles, together with disruption of myelin and sarcomeres, and inclusion physique accumulations within muscle fibers. Other problems embody pigmentary retinopathy, acanthocytosis, areflexia, ataxia, and loss of vibratory sensation. A few pedigrees with this constellation of findings have been reported with apparent autosomal dominant transmission. Patient (left) and his two kids (center and right) with full congenital fibrosis syndrome. In distinction to the muscular dystrophies, their histopathologic findings on muscle biopsy, quite than their medical features characterize these illnesses. Muscle biopsy in search of the diagnostic options of congenital myopathies ought to be thought of in any youngster with ptosis or ophthalmoplegia mixed with hypotonia or delayed motor development as quickly as myasthenia has been ruled out. Both patients had ptosis and monocular elevation palsy with levator synkinesis on adduction. Slowly progressive ocular involvement is common and runs the spectrum from ptosis to complete ophthalmoplegia. Clinical involvement of the extraocular muscles has hardly ever been described in these illnesses. It was initially referred to as myotubular myopathy due to histologic resemblance to myotubes of fetal muscle. This form further resembles creating fetal muscle in that muscles show a persistence of fetal cytoskeletal proteins vimentin and desmin. Those with identifiable modes of genetic transmission have attribute clinical courses. Patients with X-linked centronuclear myopathy have severe hypotonia at start and infrequently die early of respiratory problems. These patients typically develop a waddling gait with hypotrophy of the limb-girdle muscle tissue and hypertrophy of the calves. They have a usually myopathic, expressionless face with bilateral ptosis with or without ophthalmoparesis. An autosomal dominant type of centronuclear myopathy with slowly progressive disability has been described. In hypokalemic familial periodic paralysis, assaults start with weak spot of the extremities and progress to flaccid paralysis of a lot of the body. In the hyperkalemic and normokalemic varieties, attacks typically begin with myotonia, adopted by weakness and paralysis. Ocular involvement, presumably because of myotonia, is more widespread in the hyperkalemic selection. All three varieties of familial periodic paralysis are characterised by central vacuolation of muscle fibers histologically. The underlying dysfunction is unknown but is believed to be associated to alterations in muscle membrane permeability. Nishikawa Y, Yorifuji S, et al: Treatment of Kearns�Sayre syndrome with coenzyme Q10. Castaigne P, Laplane D, Escourolle R, et al: Ophthalmoplegi� externe progressive avec spongiose des noyaux du tronc c�r�bral. Kornblum C, Broicher R, Walther E, et al: Sensorineural listening to loss in sufferers with chronic progressive exterior ophthalmoplegia or Kearns�Sayre syndrome. Mongini T, et al: Endocrine involvement in mitochondrial encephalomyopathy with partical cytochrome c oxidase deficiency. Bresolin N, Bet L, Binda A, et al: Clinical and biochemical correlations in mitochondrial myopathies treated with coenzyme Q10. M�ller-Hocker J, Johannes A, Droste M, et al: Fatal mitochondrial cardiomyopathy in Kearns�Sayre syndrome with deficiency of cytochrome-c-oxidase in cardiac and skeletal muscle.
Benemid 500mg otcCoronal (left) and sagittal (right) magnetic resonance photographs of the mind of a affected person with pituitary apoplexy coccyx pain treatment physiotherapy buy benemid 500 mg fast delivery. The affected person introduced with headache and with complete ptosis and ophthalmoplegia on the left pain medication for dog injury generic benemid 500mg online. The eye on the left illustrates the arterialization of conjunctival vessels with the attribute corkscrew look pain medication for dogs after acl surgery buy 500mg benemid with mastercard. The affected person whose eye appears on the right had a traumatic fistula with resultant extreme chemosis and proptosis neuropathic pain treatment guidelines 2010 buy benemid 500mg amex. Third-, Fourth-, and Sixth-Nerve Lesions and the Cavernous Sinus Acute botulism, sometimes secondary to the ingestion of meals contaminated with Clostridium botulinum, results in a flaccid paresis, dysphagia, pupillary dilatation and poor reactivity, and varied degrees of ophthalmoparesis. Cutaneous squamous and basal cell carcinoma of the face may trigger a quantity of cranial nerve involvement, with ophthalmoplegia because of perineural unfold. Cerebrospinal fluid analysis is indicated if indicators and symptoms recommend a course of within the subarachnoid house or if the Fisher syndrome is suspected. Management of a quantity of ocular motor nerve palsies depends entirely on the underlying pathology. Treatment of neoplastic and infectious illnesses is guided by the character of the process and its location. In addition to antimicrobial therapy, anticoagulation may be used within the treatment of cavernous sinus thrombosis. Treatment of the variants of the Guillain�Barr� syndrome is typically supportive, though plasmapheresis has been shown to shorten the course and cut back the severity of the illness if carried out early in its course, and intravenous immunoglobulin has also proved effective. Bilateral sixth-nerve palsies within the Miller Fisher variant of Guillain-Barr� syndrome. The patient was a 63-year-old lady with a extreme influenza-like sickness with diarrhea adopted 2 months later by ascending extremity numbness, ataxia, and horizontal binocular diplopia. Examination revealed bilateral deficits of abduction, ataxia, extremity weak spot, and areflexia. The Guillain�Barr� syndrome usually presents as an ascending motor paresis affecting limb, respiratory, and bulbar musculature, secondary to a peripheral polyneuropathy. The actual location of the pathologic course of in this syndrome has been a matter of some debate, and both peripheral and central nervous system involvements have been proposed. Morard M, Tcherekayev V, de Tribolet N: the superior orbital fissure: A microanatomical examine. Destombes J, Horcholle-Bossavit G, Rouviere A: Donn�es r�centes concernant le noyau oculomoteur externe: Centre du mouvement oculaire horizontal. Umansky F, Nathan H: the lateral wall of the cavernous sinus: With special reference to the nerves related to it. Wilhelm H, Klier R, Toth B, Wilhelm B: Oculomotor nerve paresis starting as isolated internal ophthalmoplegia. Flanders M, Watters G, Draper J, et al: Bilateral congenital third cranial nerve palsy. Bogousslavsky J, Regli F, Ghika J, et al: Internuclear ophthalmoplegia, prenuclear paresis of contralateral superior rectus, and bilateral ptosis. The original brain-stem syndromes of Millard-Guber, Foville, Weber, and Raymond-Cestan. Onozu H, Yamamoto S, Takou K, Hasyasaka S: Blepharoptosis in affiliation with ipsilateral adduction and elevation palsy. Bogousslavsky J, Regli F: Nuclear and prenuclear syndromes of the oculomotor nerve. Hashimoto M, Ohtsuka K, Akiba H, Harada K: Vascular compression of the oculomotor nerve disclosed by thin-slice magnetic resonance imaging. Leunda G, Vasquero J, Cabezudo J, et al: Schwannoma of the oculomotor nerves: Report of four circumstances. Asaoka K, Sawamura Y, Murai H, Satoh M: Schwannoma of the oculomotor nerve: a case report with consideration of the surgical treatment. Adam T, Schumacher M: Traumatic lesions of the optic, oculomotor, trochlear, and abducens nerves-Computer tomographic findings. Pieh C, Rossillion B, Heritier-Barras H, et al: Isolated unilateral adduction deficit and ptosis as the presenting options of chronic inflammatory demyelinating polyradiculopathy. Mori M, Kuwabara S, Fukutake T, et al: Clinical options and prognosis of Miller Fisher syndrome. Ohtsuka K, Hashimoto M, Nakamura Y: Enhanced magnetic resonance imaging in a patient with acute paralysis of the inferior division of the oculomotor nerve. Lazaridis C, Torabi A, Cannon S: Bilateral third nerve palsy and temporal arteritis. Wilhelm H, Wilhelm B, Mildenberger I: Primary aberrant regeneration of abducens nerve fibers into the pupillary pathway. Barr D, Kupersmith M, Turbin R, et al: Synkinesis following diabetic third nerve palsy. Yanaka K, Matsumaru Y, Mashiko R, et al: Small unruptured cerebral aneurysms presenting with oculomotor nerve palsy. Kose S, Uretmen O, Pamukeu K: An method to the surgical management of complete oculomotor nerve palsy. Deokule S, Burdon M, Matthews T: Superior indirect myokymia improved with gabapentin. Maruo T, Iwashige H, Akatsu S, et al: Superior oblique palsy: outcomes of surgical procedure in 443 instances. Towfighi J, Marks K, Palmer E, et al: M�bius syndrome: Neuropathologic observations. Thomke F, Mika-Gruttner A, Visbeck A, Bruhl K: the risk of abducens palsy after diagnostic lumbar puncture. Ferrante E, Savino A, Brioschi A, et al: Transient oculomotor cranial nerves palsy in spontaneous intracranial hypotension. Campisi P, Frenkiel S, Glikstein R, Mohr G: Unilateral sixth cranial nerve palsy attributable to cranium base mass lesions: case collection. Ohtsuka K, Sone A, Igarashi Y, et al: Vascular compressive abducens nerve palsy disclosed by magnetic resonance imaging. Lee J, Harris S, Cohen J, et al: Results of a prospective randomized trial of botulinum toxin therapy in acute unilateral sixth nerve palsy. Hayashi H, Kato S, Kawada T, et al: Amyotrophic lateral sclerosis: Oculomotor perform in patients on respirators. Thurtell the organization of the ocular motor system is probably one of the clearest examples of neural hierarchy. As eye movement disorders are caused by lesions and illnesses of the nervous system, the diagnostician have to be conversant in the principles and strategies of neurological analysis (for extra details relating to the clinical methodology in neurological prognosis, see Ropper and Brown1 or Caplan and Hollander2). The goal of the current chapter is to briefly but systematically evaluate eye motion disorders which are attributable to lesions and diseases of the central nervous system. Many patients with severe, but treatable, neurological illnesses initially current with isolated eye motion issues. In such instances, the prognosis and subsequent management depend on correct evaluation of the eye movement dysfunction. Only clinically relevant eye motion problems are discussed on this chapter; many of those can be confidently diagnosed at the bedside.
Order 500 mg benemid otcIn congenital adduction palsy with synergistic divergence pacific pain treatment center victoria buy generic benemid 500 mg on line, there may be an abducens-oculomotor synkinesis that outcomes from innervation of the medial rectus by branches from the abducens nerve pain spine treatment center discount benemid 500mg. Medullary Eye Movement Disorders Eye Movement Disorder Torsional nystagmus Lateropulsion Ocular tilt response Pendular nystagmus Horizontal gaze-evoked nystagmus Primary place upbeat nystagmus Post head-shaking nystagmus Structure Involved Vestibular nucleus168 The inferior olivary nucleus receives input from the contralateral cerebellar dentate nucleus via the pink nucleus within the midbrain and the central tegmental tract pain medication for osteosarcoma in dogs cheap benemid 500 mg mastercard. Inferior olivary neurons then project to cerebellar Purkinje cells by way of the inferior cerebellar peduncle pain management in dogs and cats order 500mg benemid. It is the location of integration of horizontal eye velocity indicators into eye position indicators. The major distinction between the dorsal midbrain and the dorsal pons is that, while the dorsal pons controls horizontal eye actions, the dorsal midbrain controls vertical, torsional, and vergence eye movements. Lesions of the dorsal midbrain characteristically produce a selective dysfunction of vertical and vergence eye movements. Dorsal midbrain lesions can produce many different forms of vertical ophthalmoplegia, some of which can be difficult to distinguish from eye movement problems which are benign, congenital, nonorganic, or peripheral in origin. Since the oculomotor constructions in the pons are largely involved with the control of conjugate horizontal eye movements, dorsal pontine lesions characteristically produce a selective impairment of horizontal eye actions. Abducens interneurons provide all input required for conjugate horizontal eye motion to the medial rectus motoneurons. From the vestibular nucleus, it receives neural discharges required for the manufacturing of smooth compensatory eye movements in response to vestibular or optokinetic stimulation. The lesion (arrows) includes the left pyramidal tract and the emergent fibers of the left oculomotor nerve. The inside group of the oculomotor and trochlear nuclei also has scientific relevance. Cerebellar Eye Movement Disorders Eye Movement Disorder Horizontal gaze-evoked nystagmus Downbeat nystagmus Structure Involved Flocculus131 Flocculus159,244 Fastigial nucleus or oculomotor vermis221,224,226 Flocculus, ipsilateral oculomotor vermis, or contralateral fastigial nucleus244,248,249 Flocculus244 Dentate nucleus, superior cerebellar peduncle187,one hundred ninety Floccular Purkinje cells are usually concerned within the control of clean pursuit eye actions and within the control of vestibuloocular reflex achieve. Experimental lesions of the flocculus produce an eye motion syndrome that resembles that present in people with Chiari malformations and associated cerebellar ectopia. However, lesions of the dentate nucleus or its output via the superior cerebellar peduncle can end result in pendular nystagmus. Normally, the intralaminar nuclei of the thalamus are concerned in saccade era; thalamic lesions do produce subtle problems of saccadic management, but these are often solely detected with computerized oculography. Thalamic Eye Movement Disorders Eye Movement Disorder Tonic contraversive gaze deviation ("wrong-way" eyes) Tonic downward gaze deviation Esotropia Structure Involved In contrast to progressive supranuclear palsy, the saccadic palsy occurs late in the midst of the illness and tends to affect horizontal saccades earlier than it impacts vertical saccades. Many different disorders of saccadic and easy pursuit eye actions may be found with computerized oculography in sufferers with focal cerebral lesions. However, with few exceptions, these disorders are asymptomatic and too refined to be detected clinically, or are discovered only in the presence of other main neurological abnormalities. Only clinically evident cerebral eye movement abnormalities are thought-about here (Table 297. Anatomy and Physiology Several cortical areas are known to be concerned within the planning and initiation of saccadic eye actions, together with the frontal lobes (particularly the frontal eye fields) and the parietal lobes (particularly the parietal eye fields) (for a evaluate, see Pierrot�Deseilligny and colleagues253). Smooth pursuit and optokinetic eye movements are initiated in the posterior parietal cortex. A conjugate binocular ophthalmoplegia selectively affecting a certain class of eye actions. The loss of the vestibuloocular reflexes as a end result of bilateral peripheral vestibular lesions is an exception to this rule. A advanced disconjugate binocular ophthalmoplegia might be due both to a central lesion. Primary place or gaze-evoked involuntary eye actions in an upright affected person without vertigo, extreme visual loss, or ophthalmoplegia are always because of a central lesion or disorder, but the disorder may be benign. Cerebral Eye Movement Disorders Eye Movement Disorder Ipsiversive pursuit and optokinetic paresis Square-wave jerks Spasticity of conjugate gaze Tonic ipsiversive gaze deviation Tonic contraversive gaze deviation ("wrong-way" eyes) Epileptic gaze deviation and nystagmus Ocular motor apraxia Loss of antisaccades Spasm of fixation Structure Involved Frontal and parietal lobes134,143 A analysis of myasthenia gravis ought to be thought-about in any patient with ophthalmoplegia, especially if ptosis, weak point of orbicularis oculi, or nystagmus is present. Ocular movement is restricted by infiltration or entrapment of extraocular muscles or of different orbital tissues. A complex ophthalmoplegia may occur with any of the three variants of idiopathic demyelinating polyneuropathy: Miller Fisher syndrome,158 persistent inflammatory demyelinating polyneuropathy,258 and Guillain�Barr� syndrome. Psychotropic and anticonvulsant medication are well-known to produce ocular motor abnormalities and visual signs. The ultimate pursuit pathway from the vestibular nucleus to the ocular motor nuclei could be the same as that utilized by the vestibuloocular reflex. The frequency, direction, and amplitude of the nystagmus vary in an aperiodic method. Patients with bilateral vestibular loss generally complain of vertical oscillopsia during head movement. Loss of all vestibular operate may be verified clinically by the presence of compensatory saccadic eye movements in response to speedy head turns throughout tried fixation. These antibiotics can destroy all vestibular perform without affecting cochlear operate. The ocular tilt response that accompanies acute unilateral lack of vestibular function could produce vertical diplopia as a result of skew deviation. Patients with occult malignancies can present with a selection of nonmetastatic, paraneoplastic neurological disorders attributable to antibodies which might be produced in response to the tumor. The major tumor generally arises in the lung, breast, feminine reproductive tract, or lymphoid tissue. Paraneoplastic cerebellar degeneration may cause a selection of ocular motor abnormalities, similar to opsoclonus,227 periodic alternating nystagmus,297 and downbeat nystagmus. Chronic meningitis as a end result of tuberculosis,301 cryptococcosis,302 borreliosis,303 cysticercosis,304 sarcoidosis,305 idiopathic hypertrophic cranial pachymeningitis,306 or cancer307 can cause ophthalmoplegia on account of a quantity of cranial nerve palsies. Sporadic Creutzfeldt�Jakob illness can present with periodic alternating nystagmus,308 primary position upbeat nystagmus,309 or not often a vertical saccadic palsy. Patients with progressive supranuclear palsy commonly current with visual symptoms as a result of a vertical saccadic palsy. Pelizaeus�Merzbacher disease produces a attribute elliptical pendular nystagmus. Some patients with ataxia-telangiectasia also have periodic alternating nystagmus or different cerebellar eye motion issues. Patients with ataxia-telangiectasia have a widespread immunoparesis and the serum ranges of a-fetoprotein are raised.
Purchase benemid 500 mg on-lineOwing to the growing worldwide recognition and importance of this entity treatment pain legs generic 500mg benemid overnight delivery, worldwide congresses have been held to talk about new clinical and laboratory developments back pain treatment vancouver purchase 500 mg benemid visa. The mean age of onset is 25�35 years worldwide pain treatment center west hartford ct buy generic benemid 500mg on-line, with a variety of 2 months to 72 years pain medication for dogs after surgery discount benemid 500 mg without a prescription. He reported that uveitis alone or together with different major signs was the presenting check in a better percent of youngsters and in addition younger males showed an earlier onset of the disease with worse ocular prognosis. A viral etiology was suggested by Beh�et in his authentic publication, based mostly on observations of inclusion our bodies in oral and genital ulcerations. The enhanced expression of inflammatory cytokines suggests a defect in regulatory mechanisms, and will have a genetic basis. Familial incidence is usually reported and is believed to be attributable to the interplay of the identical environmental factor(s) together with the same histocompatibility antigen(s) in the identical household. There are regional differences, with familial incidence being extra frequent in Korea (15. They are mostly situated within the pores and skin and subepithelial layer of lungs and gut. However, these cells are sometimes activated and produce increased quantities of IgG and IgA compared to regular people. Since the diagnosis is made solely on scientific findings, a dependable historical past and physical examination, in addition to consultations amongst specialists (dermatologist, neurologist, and others) are essential to avoid errors in prognosis. These laboratory findings help the thought of immune dysregulation; however they play no position in confirming or refuting the clinical analysis. In some patients, years could pass between individual attacks (oral, genital ulcerations, arthritis and uveitis) so that the patient and treating physician are sometimes unable to attribute all of the manifestations to the same underlying disease. Plus 2 of: Recurrent genital ulceration: Aphthous ulceration or scarring, noticed by physician or patient. Eye lesions: Anteror uveitis, posterior uveitis, or cells in vitreous on slit-lamp examination; or retinal vasculitis observed by ophthalmologist. Skin lesions: Erythema nodosum observed by doctor or patient, pseudofolliculitis, or papulopustular lesions; or acneiform nodules observed by doctor in publish adolescent sufferers not on corticosteroid remedy. The exercise of ocular disease might not correlate with the exercise of mucocutaneous or arthritic lesions. If untreated or handled inappropriately, most noninfectious causes of uveitis result in slow (months to years) however progressive loss of imaginative and prescient. Due to the minimal amount of fibrin current in the anterior chamber in the course of the lively irritation, the hypopyon might change place with head motion and can form and disappear quickly. A more frequent presentation is iridocyclitis without hypopyon, which is found in two-third of instances. The initial ocular manifestations could be unilateral, however development to bilateral involvement is the rule in at least two-third of cases. All eye buildings could be affected by the central histopathologic feature of this vasculitic disease, which is a nongranulomatous inflammation with necrotizing obliterative vasculitis. Clinically, ocular findings could additionally be current within the anterior or posterior section, or extra generally, in both. Onset of new signs, or worsening of current ones could also be explosive in nature. Venous occlusions in the retina cause tissue hypoxia, which stimulates the growth of latest vessels. Because of their thin and fragile walls, these new vessels bleed into the vitreous cavity and subsequently fibrose. The optic nerve could additionally be concerned, with papillitis in the acute part seen in a minimal of one-fourth of instances. In the persistent stage, slit-lamp biomicroscopy exhibits few cells in the anterior chamber. The iris may show small patchy areas of atrophy, especially near the pupillary sphincter, and posterior synechiae. The lens typically turns into cataractous, secondary to irritation and to steroid therapy. The vitreous has floating pigmented cells and flare caused by vascular incompetence. Fluorescein leakage from retinal vessels may be seen earlier than there are obvious ophthalmoscopic signs of vasculitis. The presence of inflammatory cells within the vitreous, perivascular sheating, intraretinal hemorrhages, retinal edema or optic nerve hyperemia or swelling are very ominous indicators and indicate the involvement of the posterior pole. Months later, repeat angiograms might present areas of collateral circulation, capillary nonperfusion, intraretinal microvascular formation, and neovascularization. Arai and associates105 demonstrated elegantly with magnetic resonance imaging and single-photon emission tomography research highsignal areas in the cerebral white matter and the mind stem, and a marked discount of blood circulate in the frontal cortex. Postmortem findings included multifocal necrotizing lesions with perivascular lymphocytic infiltration and glial proliferation in the mind stem and pons. The authors correctly concluded that the dementia and character changes observed in their patient had been related to the secondary dysfunction of the frontal cortex as a outcome of injury of subcortical areas and the mind stem. During the acute inflammation, the iris has neutrophils in its stroma and around its vessels, and later, monocytes, lymphocytes, and mast cells are current. Following many recurrences, atrophy and fibrosis of the iris with posterior synechiae formation are seen. During acute irritation, the ciliary body and choroid show diffuse infiltration with neutrophils. The retinal vessels have thickened basement membranes; their endothelial cells are swollen, neutrophils marginate, and thrombus formation begins. During remission, few lymphocytes and plasma cells are found in and across the vessel partitions. There is localized loss of rods and cones in areas of prior involvement, and fibrosis is present in the internal nuclear layer. The optic nerve vessels are affected by the angiitic process in the acute phase, and the nerve tissue itself is usually infiltrated by inflammatory cells. Optic atrophy is present within the chronic stage, secondary to the angiitic ischemia and optic neuritis. Cataract formation is essentially the most frequent anterior section complication, occurring in up to 36% of circumstances in a single series. Secondary glaucoma, brought on by posterior and peripheral anterior synechiae, was seen in 11% of instances in a single sequence of 28 sufferers. The aim is to suppress inflammation, reduce the frequency and severity of recurrences, and halt any involvement of the retina. The mostly used antiinflammatory medication are corticosteroids, cytotoxic brokers, cyclosporine, and colchicine. In acute anterior section irritation, topical corticosteroids, with or without periocular corticosteroids, are indicated. In choose chronic circumstances, maintenance doses (15�30 mg/day) of prednisone could also be required in combination with immunosuppressive medicine to management the uveitis. Those circumstances are true ophthalmological emergencies and these patients have to be handled very aggressively with none delay.
Benemid: 500 mg
Benemid 500mg on lineThe most effective screening process at present consists of a diagnostic examination carried out by an ophthalmologist conversant in the disease pain medication for nursing dogs generic 500 mg benemid. Based on the findings of the examination knee pain treatment home remedy benemid 500mg otc, a advice for follow-up or treatment can be made iasp neuropathic pain treatment guidelines discount 500 mg benemid fast delivery. To tackle the issue of who must be screened in an individual unit tuomey pain treatment center order 500 mg benemid amex, city, or nation, data must be accrued in these communities demonstrating which babies are at risk. This can solely be achieved with broad screening standards for start weight and gestational age initially and narrowing down as data are gathered. Early studies in some of which nurses and/or pediatricians obtained the pictures are promising,81�84 but determination of the sensitivity and specificity of using digital pictures in a large-scale masked examine is but to be carried out. Once screening examinations have commenced, the timing of follow-up examinations is dictated by medical findings. The use of a lid speculum is frequently helpful and, after applicable topical anesthesia, a scleral indentor is useful for rotating the globe to enable a complete analysis. The purpose of the screening examination is to decide whether or not or not plus illness is current, the status of retinal vascularization by zone, the presence and severity of retinopathy, and the extent of the retinopathy. Even if sight is severely impaired to absent, the ophthalmologist caring for the child should help the mother and father in getting early access to imaginative and prescient, rehabilitation,and educational providers. Gilbert C, Fielder A, Gordillo L, et al: Characteristics of infants with extreme retinopathy of prematurity in countries with low, reasonable and excessive levels of growth: implications for screening packages. Retinopathy of prematurity: a danger issue analysis with univariate and multivariate statistics. Chan-Ling T, Gock B, Stone J: Supplemental oxygen remedy: basis for noninvasive treatment of retinopathy of prematurity. Statistical evaluation of factors related to prevalence and development in energetic part. Cryotherapy for Retinopathy of Prematurity Cooperative Group: Multicenter trial of cryotherapy for retinopathy of prematurity: preliminary outcomes. The incidence and course of retinopathy of prematurity: findings from the early treatment for retinopathy of prematurity research. Rahi J, Cable N on behalf of the British Childhood Visual Impairment Study Group: Lancet 2003; 362:1359�1365. Tasman W, Brown G, Schaffer D, et al: Cryotherapy for energetic retinopathy of prematurity. Cryotherapy for Retinopathy of Prematurity Cooperative Group: Multicenter trial of cryotherapy for retinopathy of prematurity: 3-month outcome. Cryotherapy for Retinopathy of Prematurity Cooperative Group: Multicenter trial of cryotherapy for retinopathy of prematurity: 1-year consequence. Cryotherapy for Retinopathy of Prematurity Cooperative Group: Multicenter trial of cryotherapy for retinopathy of prematurity: Snellen visual acuity and structural end result at 51/2 years after randomization. Cryotherapy for Retinopathy of Prematurity Cooperative Group: Multicenter trial of cryotherapy for retinopathy of prematurity: ophthalmological outcome at 10 years. Cryotherapy for Retinopathy of Prematurity Cooperative Group: Contrast sensitivity at age 10 years in youngsters who had threshold retinopathy of prematurity. Cryotherapy for Retinopathy of Prematurity Cooperative Group: Effect of retinal ablative therapy for threshold retinopathy of prematurity. Cryotherapy for Retinopathy of Prematurity Cooperative Group: Multicenter trial of cryotherapy for retinopathy of prematurity: fifteen-year outcomes following threshold retinopathy of prematurity: final results from the multicenter trial of cryotherapy. Early Treatment for Retinopathy of Prematurity Cooperative Group: Revised indications for remedy of retinopathy of prematurity. Multicenter trial of cryotherapy for retinopathy of prematurity cooperative group. Working Party of the Royal College of Ophthalmologists and the British Association of Perinatal Medicine: Retinopathy of prematurity: pointers for screening and therapy. The report of a Joint Working Party of the Royal College of Ophthalmologists and the British Association of Perinatal Medicine. Fierson W, Flynn J, Good W, et al: Screening examination of untimely infants for retinopathy of prematurity. MacDonald H, Committee on Fetus and Newborn: Perinatal care on the threshold of viability. Most ocular trauma in youthful children occurs throughout informal play whereas older youngsters normally sustain their accidents whereas participating in sports. The use of protective eyewear while participating in sports activities is essential in minimizing ophthalmic injuries. With appropriate eye protection, sports-related ocular trauma could be decreased as a lot as 90%. Unique points in kids include concerns with amblyopia and limitations in each prognosis and management. In youngsters younger than 10 years, deprivation amblyopia due to media opacity could additionally be more more likely to lead to extreme long-term reduction in visible acuity than the unique physical harm. The aim of this chapter is to information physicians via the examination of the injured eye and to talk about specific analysis and administration strategies for numerous injuries with a devotion to special pediatric issues. Penetrating eye harm, eyelid lacerations, and other pores and skin wounds require updated tetanus immunizations. If tetanus primary vaccination or Td tetanus booster has not been given for the previous 10 years, or if the wound is contaminated and the vaccination or booster has not been acquired for 5 years, Td tetanus booster vaccination ought to be considered. Prior to the physical examination, a description of the traumatic events must be obtained. Understanding the mechanism of injury helps in the overall assessment of the scope and complexity of the harm, and guides the examination and selections about additional diagnostic research. Instilling topical anesthesia can facilitate examination in circumstances prone to contain minor injury. In instances the place the mechanism or initial examination suggests a high likelihood of penetrating eye damage, a prompt full evaluation underneath anesthesia in the operating room is warranted. Trauma to the periocular region in the pediatric population occurs by considered one of six mechanisms: blunt drive, projectile accidents, penetrating injuries, chemical exposure and burns, explosion kind accidents, and finally, crush injuries. Blunt trauma might be the most typical sort of injury seen in both children and adults leading to all kinds of accidents to the periocular area similar to delicate tissue hematomas, lid lacerations, corneal abrasions, traumatic iritis, and fractures amongst others. Projectile trauma is widespread in youngsters and represents the impact of the moving object transferring its kinetic energy to the periocular tissue. On the other hand, a small, fast-moving projectile like a bullet may have a a lot more devastating consequence on influence. Obtaining the history within the case of a hyphema is essential with mechanism of damage being crucial. The risk of harm from abuse must be thought-about, particularly if the historical past is inconsistent or the affected person may be very younger. It was once common practice to hospitalize all pediatric hyphema patients for bed-rest with bilateral eye patching.
Syndromes - Through openings created during brain surgery
- Scaling of the skin
- Abnormal reflexes
- Urine hemoglobin
- If you are taking other medications, ask your doctor if it is okay to take them on the day of or in the days before the surgery.
- Certain mineral supplements
- Knee that gives way
- Abdominal pain
500mg benemid with mastercardIn many individuals pain treatment acute pancreatitis buy discount benemid 500mg, these branches give rise to cilioretinal arteries that supply the retina within the region of the optic nerve head and macula pain treatment center baton rouge louisiana order 500mg benemid otc. The long posterior ciliary arteries provide blood to the anterior buildings of the globe pain treatment for burns purchase benemid 500mg with visa. The orbital branches of the ophthalmic artery embody the anterior and posterior ethmoidal arteries eastern ct pain treatment center benemid 500 mg free shipping, the supraorbital artery, the lacrimal artery, and the palpebral artery. In the presence of diminished ophthalmic artery circulate, these vessels become a critical source of collateral circulation to the globe, by way of anastomoses with the external carotid artery circulation. The superior ophthalmic vein provides the principal route of venous drainage from the orbit. The inferior ophthalmic vein receives blood from the decrease lid, inferior extraocular muscles, and vortex veins. The complete field of regard could also be affected, or altitudinal or lateralized sectors could additionally be involved at the onset or for the length of an assault. Some patients speak of a gray-black curtain that progressively descends or strikes across the eye. At times, patients see the so-called optimistic visual phenomena such as scintillations, coloured or bright displays, and streaks and shimmers. Attacks typically occur over a period of weeks to months however might proceed for years. Accompanying ache in the head or eye is reportedly uncommon, nevertheless, in a single series of 83 patients youthful than forty five years, headache accompanied visual loss in 41% of people. Presumably, in these cases, publicity of the retina to intense gentle increases retinal metabolic exercise beyond the limits of perfusion. The sturdy association of carotid-vertebrobasilar anomalies with each intracranial aneurysms and vascular malformations makes baseline angiography necessary in these sufferers. The dural sinuses form an interconnected system of channels that provide a ultimate avenue of outlet for venous blood from the cranium. The medullary veins drain the subcortical and deep white matter of the brain and often turn into enlarged in vascular malformations. The community of dural sinuses is composed of the superior and inferior sagittal sinuses, transverse sinus, sigmoid sinuses, tentorial and petrosal sinuses, and cavernous sinuses. Therefore, lesions of the sagittal sinus and dural venous sinuses could lead to early manifestations of raised intracranial pressure. The pattern of branching varies relying on whether or not the artery crosses beneath (a) or over (b) the optic nerve. These crystals are usually small (10�250 mm in diameter) and lodge at bifurcations without impeding move. They disappear rather rapidly however might damage the vessel wall, producing a sheathing response. Talc and other international physique retinal emboli have been observed in the arteries of patients who inject drugs meant for oral use. Anterior findings embody dilated episcleral veins, corneal edema, hyperemia of the conjunctiva, anterior chamber cells and flare, ischemia and rubeosis of the iris, and a dilated and poorly reactive pupil. Neovascularization of the angle can result in increased intraocular pressure and glaucoma. The spells may be frequent and brief1 or much less fast in onset and longer in length. Attacks are often precipitated by orthostatic changes, discount in blood pressure, or publicity to brilliant mild. The anterior choroidal artery supplies the anterior hilus and anterolateral elements of the lateral geniculate nucleus. Branches of the center cerebral artery provide the superior portion of the optic radiations. Additional small branches of the anterior choroidal artery may contribute to the blood supply of the medial and anterior optic radiations. The posterior cerebral arteries provide the inferior portion of the optic radiations and the calcarine cortex. Retinal arteriolar and venous narrowing, retinal edema, dilated veins, and delayed filling of retinal arteries at fluorescein angiography have been described. They probably have a vasospasm-like dysfunction, and infrequently reply to calcium channel blockade. The threat of stroke, coronary artery illness, and dying can additionally be increased in patients with visible ldl cholesterol crystals in the retina. Perspective drawing of the circle of Willis depicting the connection of assorted common aneurysms to adjoining neural structures. Physicians confronted with sufferers with ischemia should base the therapy on the anatomy, pathology, and pathophysiology of the vascular process. Patients with ischemia need evaluation no matter whether or not the signs are transient or mounted, and people with acute neurologic signs need emergency evaluation to determine their candidacy for thrombolytic remedy. Vascular illness throughout the anterior cerebral circulation, however, could impair higher-order visual processing. The presence of a contralateral afferent pupillary defect distinguishes the homonymous hemianopia of an optic tract lesion from extra posterior geniculocalcarine injury. Occasionally, the afferent papillary defect may be on the ipsilateral side if the amount of nasal subject loss is greater. Following complete occlusion, low perfusion stress to the cerebral hemispheres, especially in border zone areas, can even lead to harm. Hypercoagulable states and migraine with vasoconstriction also can lead to occlusion of those intracranial arteries. The analysis of sufferers with anterior cerebral hemisphere ischemia should be individualized. Treatment relies upon heavily on the trigger but ought to always handle threat factor discount. Thrombosis of the cavernous sinus results in shunting of blood to the extracranial venous system (arrow; frontal vein). Ischemia limited to the higher or lower calcarine financial institution causes a contralateral inferior or superior quadrantanopia. As a results of the retinotopic group of the geniculocalcarine projections on the striate cortex, hemianopic defects with meridional sparing might result from focal striate cortex infarcts. They normally retain response to visible risk, and optokinetic responses are preserved. Additional symptoms of higher cortical visible dysfunction embody hemiachromatopsia, visible perseverations, palinopsia and metamorphopsia. Emboli come up from both the guts or extra proximal vertebrobasilar arterial system, especially the origin or intracranial parts of the vertebral arteries. Temporary visible or sensory symptoms on the opposite facet of the physique normally precede infarction. Given the frequency of cardiac emboli, noninvasive cardiac testing (echocardiography and rhythm monitoring) is necessary. Aspirin, warfarin, or other prophylactic therapy is usually prescribed, depending on the cause. Brain Stem and Cerebellar Ischemia the primary points of posterior circulation ischemia are vast and beyond the scope of this chapter.
Generic benemid 500 mg free shippingMovements of the best eye are shown in interrupted traces pain solutions treatment center woodstock buy 500mg benemid amex, while actions of the left eye are shown in steady traces sciatica pain treatment exercise generic benemid 500mg mastercard. An attempted 10� leftward saccade reveals gradual adduction of the best eye (peak velocity is 148�/s pain treatment agreement 500mg benemid visa, in contrast to 400�/s for left eye abduction) pain treatment center memphis tn discount benemid 500 mg with amex. The gentle slowing of left eye adduction and the slight right eye abduction overshoot through the rightward saccade might be normal. There was no limitation of the amplitude of adduction of the right eye and due to this fact no exotropia on holding gaze to the left after the leftward saccade (d); nonetheless, due to the delay in adduction of the proper eye, there was a marked exotropia in the course of the leftward saccade (c). In the highest three images on the left, the affected person is trying to look diagonally up-right, proper, and down-right, respectively. In the underside three pictures, the patient is making an attempt to look diagonally up-left, left, and down-left, respectively. The patient was unable to adduct both eye past the midline and he also had bilateral exotropia with alternate fixation. On his attempts to look right or left, there was nystagmus in the abducting eye with quick phases directed laterally. Vertical saccades had been regular and convergence was present, however the vertical vestibuloocular reflex was markedly poor. The gaze deviation is paroxysmal and is usually contraversive, however may be ipsiversive. In contrast to tonic gaze deviation, spasticity of gaze can occur in patients with no other neurological deficits. In distinction with the tonic gaze deviation produced by cerebral hemisphere lesions, the tonic gaze deviation produced by pontine lesions involving the abducens nucleus is at all times contralesional and is accompanied by loss of all ipsilesional eye actions apart from vergence actions. In the first position, the affected person fixates with the horizontally immobile left eye; the proper eye is moderately exotropic. On tried rightward gaze, the right eye abducts usually, but the left eye fails to move. On tried leftward gaze, the right eye moves to the midline, however the left eye again fails to move. The lesion in this case entails the left paramedian pontine reticular formation and the adjoining left medial longitudinal fasciculus. The palsy can have an effect on all kinds of eye movement in the one path or solely a selective saccadic palsy may be present. All ipsilesional saccadic eye actions, including the fast phases of vestibular and optokinetic nystagmus, are either gradual or absent, whereas contralesional saccades and vestibular-evoked, easy pursuit, and optokinetic-evoked eye actions are normal. In addition, there could additionally be bilateral facial and hypoglossal palsies due to aplasia of those nuclei. All ipsiversive saccadic eye movements are hypermetric, whereas all contraversive saccadic eye movements are hypometric. Lateropulsion possibly happens because of disruption of olivocerebellar climbing fibers passing by way of the lateral medulla to produce, indirectly, elevated inhibition of the ipsilateral fastigial nucleus. There was also primary position esotropia and bilateral total facial palsy but no disturbance of consciousness and no long-tract signs. The saccade in response to a 20� rightward goal change undershot the target, so that additional rightward saccades had been required to fixate the goal. Vertical saccades in response to a 20� upward and a 20� downward goal change also had an unintended leftward component, in order that a quantity of small saccades with rightward parts were required to fixate the target. Unilateral peripheral trochlear nerve lesions trigger isolated weakness of the superior oblique muscle, leading to vertical and torsional diplopia. Bilateral peripheral trochlear nerve lesions, if symmetric, might produce esotropia and bilateral excyclotropia82 with hypertropia of every eye throughout adduction. Bilateral superior indirect paralysis must be differentiated from restrictive ophthalmopathies, overaction of the inferior obliques,eighty three from physiological hyperdeviation in lateral gaze,eighty four and from alternating skew deviation. Skew deviation is a vertical strabismus resulting from a supranuclear lesion affecting central otolithic pathways. It could be unilateral or bilateral, and has been reported with lesions throughout the brainstem and cerebellum. The ocular tilt reaction is a head�eye postural synkinesis characterized by skew deviation with head tilt and conjugate eye torsion toward the side of the hypotropic eye. It seems to be an otolithic righting reflex and occurs in patients with lesions of each the peripheral90 and central vestibular systems. A unilateral midbrain lesion that entails the trochlear nucleus or fascicles results in a typical unilateral superior indirect palsy on the other aspect. A midbrain lesion, such as an infarct, involving the oculomotor nucleus or fascicles can also end in a paralytic vertical strabismus, usually with associated ptosis. Tonic contraversive ocular tilt response caused by a unilateral midbrain-thalamic lesion. Unilateral medullary lesions that contain the vestibular nucleus produce a tonic ipsilesional ocular tilt reaction. Acute unilateral lesions of the labyrinth or vestibular nerve invariably produce asymptomatic ipsilesional conjugate ocular torsion. Tethering of the extraocular muscles,103 infiltration of the extraocular muscular tissues,104 and myasthenia gravis are other frequent causes of vertical diplopia. Vertical Gaze Deviation A tonic vertical gaze deviation may finish up from both underactivity of a contraversive gaze mechanism or overactivity of an ipsiversive gaze mechanism. Examples of an overactive gaze mechanism embrace spasms of upward gaze ensuing from oculogyric crises105,106 or from epileptic seizures. He also had loss of pain and temperature sensation on the left aspect of the face and on the best side of the physique. The vertical gaze palsies that occur with midbrain lesions can assume several different patterns with respect to the course and the kind of eye movement affected. A vertical gaze palsy can selectively impair upgaze or downgaze, or it could impair both; it can selectively impair only saccadic eye actions or vestibular-evoked eye actions, or it can impair both. In focal midbrain lesions that selectively impair solely saccades, it could be upward saccades, downward saccades,one hundred ten or saccades in both instructions that are impaired. An isolated upward gaze palsy may be congenital116 and can also happen as an incidental discovering within the aged. A vertical gaze palsy can occur in isolation or in affiliation with eyelid, pupillary, and other ocular motor abnormalities. In the highest row, the affected person is attempting to look straight forward; observe the lid retraction. Once the shunt was replaced, the ventricles shrunk and her eye actions returned to normal. In this patient, pressured downward gaze was the sole indication of shunt malfunction.
Purchase 500 mg benemid amexIt is beneficial for patients to maintain a headache diary to identify the effects of hormonal fluctuations pain treatment west plains mo discount 500mg benemid mastercard, to determine whether dietary triggers are current chronic pain treatment options buy benemid 500mg mastercard, and to monitor the effectiveness of treatment pain medication for dogs ibuprofen generic 500mg benemid otc. Perhaps half of migraineurs identify dietary or environmental triggers of their attacks oriental pain treatment center brentwood cheap 500 mg benemid amex. Common dietary triggers embody aged meat, aged cheese, bananas, avocados, dried and overripe fruit, aspartame, caffeine, chocolate, monosodium glutamate and other meals additives, and nuts. Beer, wine, and different fermented or nitrite-containing beverages could set off migraines. Autonomic manifestations include eyelid edema, conjunctival injection, tearing, Horner syndrome, rhinorrhea, nasal congestion and facial flushing (Table 290. Because of the prominent ocular manifestations, these sufferers usually seek ophthalmic care early in their course. Guidelines for Preventive Treatment of Migraine Group 1 Amitriptyline Divalproex sodium Lisuride Propranolol Timolol Topiramate Group 2 Aspirin Atenolol Biofeedback Coenzyme Q10 Feverfew Flurbiprofen Fluoxetine Gabapentin Guanfacine Ketoprofen Magnesium Metoprolol Lornoxicam Nadolol Naproxen sodium Nimodipine Petasides Tofenamic acid Verapamil Vitamin B2 Group 3 a. Yes Tearing only No specific treatment recognized Female:Male Ratio 2:1 1:1 1:2 Unknown Epidemiology and Impact Cluster headache is way less frequent than migraine, affecting less than 1% of the inhabitants. The pain is centered across the eye and orbits and will radiate into the temple, forehead, cheek, or jaw. In distinction to migraine, the place sufferers choose to lie down in a dark, quiet room, sufferers with cluster headaches are restless and typically violent. They are likely to pace, sit, rock, bang their head against the wall, or try to distract themselves from the ache by going outside or participating in an exercise requiring focus. The autonomic options of cluster headache embrace Horner syndrome (ptosis and miosis), lacrimation, conjunctival injection, nasal stuffiness, or rhinorrhea. In some circumstances, the Horner syndrome persists after the assault subsides, and may be permanent. Genetics There appears to be a genetic component to cluster headaches in some households. Mechanism and Pathophysiology Any proposed mechanism for cluster headache must clarify the periodicity, circadian nature of the pain, ophthalmic nerve distribution of pain and ipsilateral autonomic features. Both sympathetic (postganglionic Horner syndrome) and parasympathetic (lacrimation, rhinorrhea) nerves are involved. Magnetic resonance angiography reveals vasodilation of the ipsilateral ophthalmic artery during an attack of cluster headache. The parasympathetic features of cluster likely come up from the superior salivatory nucleus, synapsing in the otic, sphenopalatine, and carotid miniganglia. They innervate cerebral blood vessels in addition to the lacrimal gland and nasal mucosal glands, accounting for the lacrimation, nasal congestion and rhinorrhea in cluster headaches. The periodicity and clock-like regularity of cluster headache implicates involvement of the suprachiasmatic nucleus, which relays details about the light�dark cycle to the hypothalamus. During a cluster period, the 24-h production of melatonin is lowered and the nocturnal peak concentration is blunted. The speedy development of ache and quick duration of particular person attacks make cluster complications particularly challenging to treat. Inhaled, oxygen has been used to deal with acute attacks of cluster headache since the Fifties. A flow price of 7 L/min via non-rebreathing facial masks yields relief inside 15 min in 70% of sufferers. Unfortunately, third-party payers often deny protection for home oxygen remedy in the absence of pulmonary illness. Subcutaneous sumatriptan 6 mg produces complete headache aid in about three-quarters of sufferers inside 15 min. Transitional prophylaxis ought to be instituted as soon as the cluster period starts to obtain rapid remission, and scale back headache frequency and severity. Prednisone (60 mg every day for 3 days, tapering by 10 mg every three days) or dexamethasone (4 mg twice daily for two weeks, then once day by day for 1 week) are highly efficient, although headaches may recur in the course of the taper interval. Ergotamine tartrate and dihydroertamine may be used for 2�3 weeks to suppress headache exercise. The third tier of remedy is upkeep prophylaxis to prevent recurrence during and after the transitional prophylaxis interval. Verapamil is mostly efficient, starting at 240 mg daily and increasing to 720 mg every day in divided doses. It is remarkably nicely tolerated at very high doses by most cluster headache Clinical Features Cluster complications are characterised by seasonal and circadian periodicity. The cluster interval is the time during which assaults are occurring, generally weeks to months. Episodic cluster headaches happen in intervals lasting seven days to a yr, separated by pain-free intervals lasting 14 days or more. Chronic cluster headache, accounting for ~15% of sufferers, happens for a couple of year with out remission or has remissions lasting lower than 14 days. Serum lithium focus, renal and thyroid functions must be monitored, and attention to attainable drug interactions is required. Methysergide was beforehand used for cluster headache however is no longer obtainable within the United States. The potential for pulmonary, retroperitoneal and pericardial fibrosis limit its use to three months or fewer. Valproic acid (250 mg bid increasing as much as 2 gm daily), topiramate (50�125 mg daily) and melatonin (10 mg) are additionally efficient. Indomethacin, which is useful in treating other trigeminal autonomic cephalgias, is much less successful in cluster complications. Radiofrequency thermocoagulation of the trigeminal ganglion is effective in 75% of patients with a 20% recurrence price. Complete analgesia should be produced, so long-term corneal care is crucial to forestall neurogenic ulceration. Trigeminal sensory rhizotomy on the root exit zone, and occipital nerve stimulation have been used successfully. Deep mind stimulation of the hypothalamus exhibits promise in sufferers with intractable chronic cluster headache. The ache is associated with at least one of many following options on the affected side: conjunctival injection (usually very prominent), lacrimation, nasal congestion, rhinorrhea, ptosis, and eyelid edema. There may be a uninteresting interictal discomfort however most sufferers are asymptomatic between attacks. Symptomatic durations may last from days to months, with remission lasting from one week to seven years (usually a number of months). Many patients can precipitate their attacks by touching sure areas in the trigeminal distribution, such as the hair, forehead, face, nostril, or lip.
Discount benemid 500mg mastercardIf advanced diagnostic pain treatment center buy cheap benemid 500 mg online, on utility of 1% pilocarpine in every eye pain wrist treatment generic 500mg benemid amex, the affected pupil does little or nothing and the unaffected pupil constricts usually wrist pain treatment exercises buy 500mg benemid with amex, the pupil was dilated not because of nerve denervation however due to a problem within the sphincter muscle itself pain treatment centers of illinois new lenox purchase 500mg benemid amex. Traumatic iridoplegia (look for sphincter rupture, pigment dispersion, angle recession) three. Fixed pupil after anterior segment surgical procedure this last trigger for the entire lack of perform of the iris muscle is unknown. It could also be associated to the identical course of as the Urrets�Zavalia syndrome, during which a dilated, fixed pupil could happen after penetrating keratoplasty. If the anticholinergic drug is carrying off in order that a small gentle response is starting to return, 1% pilocarpine may cause a minimal constriction, however much less in comparability with the unaffected eye. The slit-lamp examination normally reveals segmental denervation of the iris sphincter. Within the first week, supersensitivity to cholinergic substances can be demonstrated. After ~2 months, nerve regrowth is active, and fibers originally bound for the ciliary muscle (they outnumber the sphincter fibers by 30:1) begin arriving (aberrantly) at the iris sphincter. Third-nerve palsy There is an old medical rule of thumb that if the pupillary mild reaction is spared, the third-nerve palsy might be due not to compression or damage however extra prone to small-vessel disease, corresponding to may be seen in diabetes. It remains to be a fairly good rule, supplied one bears in thoughts that a small but particular number of pupil-sparing third-nerve palsies are due to midbrain infarcts and sufferers should have neuro-imaging studies. Aberrant regeneration of the third nerve the fastened, dilated pupil When a pupil is dilated by an atropinic medicine, it might be distinguished with some confidence from a palsy of innervation the third cranial nerve carries fibers destined for several different muscular tissues, in order that when the nerve is injured and the fibers regrow, they often find yourself in the wrong place. With eyelid involvement, the lid fissure might widen with infraduction, adduction, or supraduction of the eye. Particularly if the light response appears weak, one should see whether or not the pupils constrict better to a close to stimulus than to light. Loss of light input because of severe damage to the afferent visual system (retina or optic nerve pathways) 2. Interruption of the light input pathways to the Edinger�Westphal nucleus from the pretectum (Argyll Robertson pupils, dorsal midbrain syndrome) 3. In the top pictures, the affected pupil is the smaller pupil in darkness (right) compared with light (left) because of tonic contraction from accommodative cholinergic nerves that reinnervated the iris sphincter. With a near stimulus (middle photographs), the affected pupil constricts maximally because of firing of the accommodative nerves which have reinnervated the sphincter after ~8 weeks, and the near contraction is considerably extended (tonic) even 5 s after the patient gazes off within the distance (middle right photograph). After low-concentration pilocarpine was given to both eyes, the right pupil is extra constricted in darkness compared with the left, exhibiting supersensitivity (lower left photograph). After a higher focus of pilocarpine was added, both pupils are maximally constricted in darkness (lower right photograph). This could probably be an ischemic third on top of pre-existing diabetic autonomic neuropathy of the iris sphincter. Chart summarizing the scientific situations by which various portions of third-nerve operate could additionally be affected and the relative threat of morbidity from compression. Boxes in yellow signify potential danger that will need close consideration and possible neuroradiologic work-up. Example of a affected person exhibiting secondary aberrant regeneration of the third nerve after trauma. When the affected person makes an attempt downgaze, the affected right eye adducts due to inferior rectus nerves growing into the medial rectus muscle. In addition, the pupil constricts with an adducting movement of the attention, signifying that rectus motor nerves have also grown into the iris sphincter. Give the affected person an accommodative goal, something of curiosity or with nice detail on it. Remember that the close to response, though it might be triggered by blurred or disparate imagery, has a large volitional element, and the patient may have encouragement. If that is unsuccessful, attempt the lid closure reflex: ask the patient to have a glance at you and squeeze the eyes shut when you try, with both arms, to maintain certainly one of them open. When you face the patient, with pocket gentle in hand, there are normally three ranges of sunshine available to the examiner: (1) darkness, with a light shining tangentially on the pupils from below; (2) room mild; and (3) room gentle with a further bright gentle in the eyes. With the affected person looking within the distance, shine the intense light within the eye three or 4 occasions, every time for only 1 or 2 s. Never judge the near response by adding a close to stimulus to a shiny mild stimulus; this almost all the time produces an apparent light-near dissociation as a outcome of the close to stimulus inevitably adds something to the light stimulus. A actual lightnear dissociation is present provided that the close to response (tested in reasonable light) exceeds the most effective constriction that bright mild can produce. When the Pupil Fails to Dilate When one or both pupils keep small and miotic, even in darkness, a number of causes could also be responsible (Table 293. This reduces the firing of the preganglionic parasympathetic neurons within the Edinger�Westphal nucleus, causing leisure of the iris sphincter. The combined inhibition of the iris sphincter and stimulation of the iris dilator is a carefully integrated neuronal reflex. Age-appropriate lack of accommodative amplitude that has not been adequately corrected with a close to prescription c. A careful medical and ocular historical past should be sought (including medications), and infrequently an attempt at reproducing the signs in the examination lane may yield insight into the problem (sometimes it could only be a matter of improper eyeglass alignment). The examination should systematically embody measurement of the accommodative amplitude in diopters; refraction (often including cycloplegic refraction); pupillary and ocular motility examination; and slit-lamp examination of the pupil, lens, and zonules. In most instances, the trigger of accommodative abnormalities is often benign, and the affected person can often be helped. These must be distinguished from convergence abnormalities that may trigger related signs. Anisometropia (unequal refractive error) that has not been properly corrected within the distance may also give rise to asthenopic signs. Lowenstein O, Kawabata H, Loewenfeld I: the pupil as indicator of retinal exercise. Harms H: Grundlagen, methodik und bedeutung der pupillenperimetrie f�r die physiologie und pathologie des schorgans. Alexandridis E, Krastel H, Reuther R: Disturbances of the pupil reflex associated with lesions of the upper visual pathway. Reuther R, Alexandridis E, Krastel H: Disturbances of the pupil reflex related to cerebral infarction in the posterior cerebral artery territory. Narasaki S, Kawai K, Kubota S, Noguchi J: Videopupillographic perimetry and its scientific software. Some of those ailments are so uncommon that no clinician might fairly be anticipated to remember all of them or their characteristics. Nonetheless, the astute ophthalmologist ought to keep this basic category of disease in thoughts whenever evaluating a affected person with ophthalmoplegia. Key Features: Diseases of the Ocular Muscles � Limited ocular motility or strabismus related to hypotonia or weak point of the orbicularis oculi suggests main muscle disease Progressive ophthalmoplegia suggests mitochondrial illness, muscular dystrophy, or vitamin E deficiency Static ophthalmoplegia suggests congenital cranial nerve palsy, extraocular muscle fibrosis, or congenital myopathy Episodic or variable ophthalmoplegia suggests myasthenia � � � in making the right prognosis. Diseases of the neuromuscular junction similar to myasthenia gravis are additionally covered elsewhere (see Chapter 295). Another common state of affairs in which primary muscle disease must be suspected is isolated acquired ptosis. Weakness of the orbicularis oculi is particularly frequent and must be routinely checked in the ophthalmic examination.
500 mg benemid overnight deliveryThe unique pedigree was Portuguese pain treatment devices purchase 500mg benemid otc, however identical clinical findings and amino acid substitutions have been reported in Japanese and Swedish kindreds xiphoid pain treatment 500mg benemid sale. The error is at position 30 within the prealbumin molecule pain treatment ovarian cyst buy generic benemid 500 mg on-line, with methionine being substituted for valine dfw pain treatment center buy benemid 500mg with amex. A woman presenting with oculoleptomeningeal amyloidosis underwent biopsy, and immunochemical stains recognized transthyretin as the protein precursor. Interestingly, restriction fragment size polymorphism evaluation confirmed a methionine 30 mutation, similar to that of sufferers with sort I heredofamilial amyloidosis. An Indiana family was the first pedigree to be reported, though a Swiss kindred was found to have identical medical findings, with the same substitution of isoleucine for serine at place eighty four. As mentioned earlier, a mononucleotide substitution within the gelsolin gene results in the medical findings. To date, more than forty amyloidogenic variants of transthyretin have been identified. New constellations of vitreoretinal amyloidosis plus neuropathy, accompanied by abnormalities in other organ techniques, are being described. Familial Mediterranean fever is the prototype of the nephropathic form (and the one heredofamilial syndrome with autosomal recessive inheritance). Aberrant apolipoprotein A-I, fibrinogen, and lysozyme have each been implicated in several pedigrees with nephropathic heredofamilial amyloidosis. Analysis of the three types of amyloid deposits on this devastating dysfunction has led to the characterization of the first component-so-called amyloid b-protein, which is a small fragment of a membrane-associated glycoprotein. Other problems with central nervous system amyloid deposition embrace the spongiform encephalopathies and localized nodular meningeal infiltration. In oculoleptomeningeal amyloidosis, typical vitreoretinal deposition (see the following section) is seen in combination with diffuse meningeal infiltration. This infiltration involves the cerebral convexities, resulting in seizures and focal neurologic deficits. As talked about earlier, one affected person with typical oculoleptomeningeal amyloidosis was found to have the Val30Met substitution typical of sort I heredofamilial amyloidosis. Ocular Manifestations of Amyloid Deposition Various ocular constructions could also be concerned in any of the varieties of systemic amyloidosis, as properly as in numerous amyloidoses restricted to the eye. The orbit and ocular adnexae are regularly concerned in the amyloidoses,23 more commonly with the primary amyloidoses than with those associated with systemic inflammatory or infectious issues (secondary amyloidoses). For dialogue, see beneath Systemic Manifestations of Heredofamilial Systemic Amyloidoses on this chapter. A latest case report of levator involvement documented immunoglobulin lambda gentle chain accumulation on this isolated major amyloidsosis. Proptosis might end result from a localized orbital mass29 or from diffuse fatty infiltration by amyloid. Lacrimal gland involvement could additionally be insidious, manifesting as keratoconjunctivitis sicca (see later). The optic nerve sheath may serve as a spotlight for amyloid infiltration, with a secondary compressive optic neuropathy. Computed tomographic scan depicting selective infiltration of extraocular muscular tissues by amyloid. There is one report of a plasmacytoma of the caruncle with related amyloid deposition. One form of adnexal involvement carries unique implications and deserves particular mention. Eyelid skin involvement is distinct from different adnexal manifestations for a quantity of reasons. The integument is a most popular website of infiltration in systemic amyloidoses, both immunocytic (primary) and reactive (secondary). The eyelid, in turn, is likely one of the mostly involved sites in dermal amyloidosis. Thus, not like different adnexal amyloidoses, eyelid deposits point out a excessive likelihood of systemic disease. Adnexal involvement that includes pores and skin deposition is systemic till proved otherwise, whereas involvement that spares pores and skin is probably localized. Any amyloid deposit, however particularly dermal, has a remarkable propensity for hemorrhage. This displays the proclivity of the protein for vessel wall infiltration with subsequent vascular fragility and hemorrhage after incidental trauma (or even spontaneously). It could also be related to the previously described orbital manifestations and with other dermal deposits (scalp, face, neck, axillae) or could also be isolated. They may be unilateral or bilateral, tending to be agency or rubbery with a waxy appearance. As with orbital amyloid, the conjunctival deposits are painless, however could trigger epiphora or important local swelling and irritation. Prospoctoscopic periorbital purpura in beforehand unrecognized systemic amyloidosis. From Ohnishi Y, Shinoda Y, Isibashi T, Taniguchi Y: the origin of amyloid in gelatinous drop-like corneal dystrophy. The affected person presented with conjunctival amyloidosis, and preliminary systemic analysis was adverse. Chemical analysis of amyloid deposits from the scapula revealed protein of composition identical to that isolated from the conjunctiva 1 12 months earlier. Clinical ophthalmologists are most likely more familiar with amyloidosis affecting the cornea than that involving any other ocular structure, reflecting the notably distinctive appearances of the varied corneal amyloidoses. The cornea could be concerned in virtually any form of amyloidosis, but reactive systemic amyloidosis almost always spares the cornea. Heredofamilial amyloidoses, however, show a propensity for corneal involvement. There are three inherited amyloidoses that affect the cornea on a localized foundation. Most affected individuals are of Asian descent; whites and African Americans are occasionally affected. The typical findings encompass milky white, subepithelial, nodular deposits that enlarge slowly and unfold centrally. There may be morphologically comparable deposits affecting the perilimbal conjunctiva. Symptoms usually develop within the second or third decade, often manifesting as recurrent erosion. Therapy consists of supportive take care of epithelial defects and, finally, keratoplasty, preferably lamellar. Lattice dystrophy kind I (also often identified as Biber�Haab�Dimmer dystrophy) is inherited as an autosomal dominant trait with low penetrance. Lattice dystrophy presents early in life as a bilateral, symmetric disorder primarily affecting the central cornea. The deposits originate within the anterior one-third of the stroma but spread limbally and deeply to involve almost the complete stroma. The slit-lamp look of lattice dystrophy is distinctivedelicate, linear, branching deposits with clear intervening stroma.
References - Terada, N., Arai, Y., Okubo, K. et al. Interstitial laser coagulation for management of benign prostatic pyperplasia: long-term follow-up. Int J Urol 2004;11:978-982.
- Alexander J, Limaye A, Ko C, et al. Association of hepatic iron overload with invasive fungal infection in liver transplant recipients. Liver Transpl. 2006;12:1799-1804.
- Torricelli FC, De S, Li I, et al: Can obese stone formers follow dietary recommendations?, J Endourol 28(2):248n251, 2014.
- Fizazi K, Culine S, Kramar A, et al: Early predicted time to normalization of tumor markers predicts outcome in poor-prognosis nonseminomatous germ cell tumors.[see comment], J Clin Oncol 22:3868n3876, 2004.
- Flynn JT, Kaelber DC, Baker-Smith CM, et al: Clinical practice guideline for screening and management of high blood pressure in children and adolescents, Pediatrics 140(3):e20171904, 2017.
- Caffrey CR, Gsell C, Ruppel A. Schistosoma japonicum is less sensitive to cyclosporine A in vivo than Schistosoma mansoni. J Parasitol. 1999;85:736-739.
- Liebner S, Czupalla CJ, Wolburg H: Current concepts of blood-brain barrier development, Int J Dev Biol 55:467-476, 2011.
|