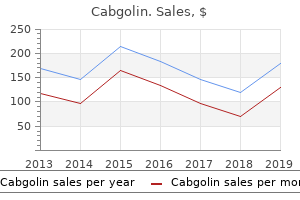
Cabgolin
Bruce D. Spiess, MD, FAHA - Professor of Anesthesiology and Emergency Medicine
- Director of VCURES
- VCU–Medical College of Virginia
- Richmond, Virginia
Order cabgolin 0.5 mg visaThe exterior genitalia are lined by keratinizing stratified squamous epithelium symptoms queasy stomach discount 0.5mg cabgolin fast delivery. In the creating embryo symptoms for mono buy cabgolin 0.5mg line, primordial germ cells from the yolk sac wall migrate to the urogenital ridge to turn into ovarian germ cells within the epithelium and stroma derived from urogenital ridge mesoderm treatment 32 for bad breath order cabgolin 0.5mg mastercard. The unfused parts of the m�llerian (paramesonephric) ducts form the fallopian tubes medications lexapro cabgolin 0.5 mg with mastercard, and the fused parts become the uterus and vagina, whereas the distal fused ducts contact the urogenital sinus to become the vestibule of the exterior genitalia. Contrast material extends into the best fallopian tube and left fallopian tube, eventually spilling out through the fimbriated ends of the fallopian tubes (oviducts) in the right adnexal and left adnexal areas, indicating regular tubal patency. These paired glands produce mucinous secretions and have ducts that empty into the vaginal orifice. The duct to a gland can become obstructed, resulting in cystic glandular enlargement with irritation and infection, producing pain and discomfort. In the best panel, the cyst with flattened transitional or squamous lining is at the far proper, with remaining adjacent normal glands on the left. This course of can develop slowly and contain progressively extra labial skin surface in ladies, particularly after menopause. Formerly known as lichen simplex chronicus, this lesion arises from mechanical irritation with rubbing or scratching pruritic pores and skin to relieve pruritus. It varieties a sharply circumscribed nodule, most commonly in the labia majora or interlabial folds. It has a histologically similar look to an intraductal papilloma of the breast. Note the overlying hyperkeratosis (which produces a grossly visible space of leukoplakia), with more regular (but atrophic) keratinizing squamous epithelium on the left. Many lesions are multicentric, and some happen in affiliation with cervical or vaginal squamous carcinoma. Note the vacuolated cells forming irregular clusters with ill-defined glandular lumens. Clear cell carcinoma typically becomes invasive before detection and is troublesome to cure. A Pap smear is obtained by scraping or brushing the floor of the cervix (and typically the vagina) to get hold of cells which are placed in a fixative solution and stained. The cervix has been opened anteriorly at post-mortem to reveal an endocervical canal leading to the lower uterine phase on the best that has an erythematous appearance extending to the cervical os, in keeping with continual irritation. The cervix has an underlying dense fibromuscular stroma that appears white on minimize part. Inflammation with cervicitis might produce submucosal gland obstruction in order that glandular cystic dilation happens. These are common lesions, generally starting from a few millimeters to 1 cm in measurement. The endocervix has underlying endocervical glands within the stroma which might be additionally lined by tall mucinous columnar cells. The uterus has been opened anteriorly here to reveal the endocervical canal and decrease uterine segment. During reproductive years, estrogen levels promote maturation with glycogen uptake of cervical and vaginal squamous epithelium, and this glycogen supplies a substrate for the traditional vaginal bacterial flora that keeps the pH low to inhibit proliferation of pathogenic organisms. Common bacterial organisms, including streptococci, staphylococci, enterococci, and coliforms, and the fungus Candida and the protozoan Trichomonas vaginalis could contribute to cervicitis and vaginitis, which usually have a clinical course marked by episodes of acute irritation that blend into chronic irritation. The restore response to the inflamed and eroded epithelium might produce mildly atypical�appearing cells ("inflammatory" atypia) on a Pap smear. There is some extent of cervicitis in practically all girls, however the amount of irritation is minimal, and normally no significant health problems are related to it. Metaplasia is a doubtlessly reversible process in which one type of epithelium is exchanged for the traditional epithelium. Metaplasia could additionally be step one in epithelial mobile alteration resulting in dysplasia. Bacterial vaginosis contains gram-negative cocci of Gardnerella species and small curved rods of Mobiluncus species. Inflammatory cells and infectious agents corresponding to Candida albicans, trichomonads, and clue cells of bacterial vaginosis. The cytologic features of regular squamous epithelial cells can be seen at the center high and backside, with orange to pale blue, platelike squamous cells which have small pyknotic nuclei. The dysplastic cells within the heart extending to the higher proper are smaller overall with darker, extra irregular nuclei. The irritation and hemorrhage in the background are characteristic of a extra aggressive, ulcerative, and invasive lesion. There is continued expression of E6/E7 oncogenes with destabilizing influences on the cell cycle. Nevertheless, dysplasias are probably to progress over a few years, giving plenty of alternative to find early lesions with periodic Pap smear screening and to deal with with excision of the dysplastic areas. Note how the dysplastic cell nuclei are bigger and darker, and the dysplastic cells have a disorderly arrangement within the epithelium. Five-year survival charges of 80% to 90% occur when the neoplasm is more invasive but nonetheless confined to the cervix (stage Ib). Cervical carcinomas could begin appearing in the second decade, however the peak incidence is within the fifth decade. On the left, dark vulvar skin leads to the vagina and to the cervix in the heart, where an irregular tan tumor mass is infiltrating upward into the bladder. Nests of neoplastic squamous cells are invading via a chronically inflamed stroma. Most cervical carcinomas are composed of enormous pink keratinizing or nonkeratinizing squamous cells. Less than 5% are composed of small undifferentiated cells or neuroendocrine cells. The proliferative (follicular) portion of the cycle varies amongst women but tends to remain the identical for any one girl. The time from ovulation to menstruation within the secretory (luteal) portion of the cycle is a continuing 14-day interval. In this section, tubular endometrial glands lined by tall columnar cells and surrounded by a dense stroma are proliferating to construct up the quantity of functional endometrium after the earlier cycle with shedding from menstruation. The histologic adjustments after ovulation are fixed over the next 14 days to menstruation and can be utilized to date the endometrium with biopsy for diagnostic functions. Endocrine abnormalities of the pituitary or ovary can also be implicated, as could weight problems or any chronic illness state. The failure of ovulation leads to an inadequate luteal section with prolonged estrogenic stimulation with out the progestational part. This produces a persistent proliferative endometrial pattern and eventual stromal breakdown with bleeding. The biopsy sample shown right here, on what should be postovulatory day eight, shows minimal glandular development and stromal hemorrhage. These adjustments prevent successful implantation of the blastocyst, but the primary impact of contraceptive brokers is prevention of ovulation. Retained products of conception after delivery increase the danger for endometritis.
Bupleurum. Cabgolin. - Fevers, flu, the common cold, cough, fatigue, headache, ringing in the ears, liver disorders, blood disorders, stimulating the immune system, and many other uses.
- Dosing considerations for Bupleurum.
- Are there safety concerns?
- How does Bupleurum work?
- Are there any interactions with medications?
- What is Bupleurum?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96640
Cabgolin: 0.5 mg
Purchase cabgolin 0.5mg otcIn distinction symptoms 12 dpo proven 0.5 mg cabgolin, many naturally occurring globular protein antigens possess just one copy of every epitope per molecule hb treatment cheap cabgolin 0.5mg fast delivery. These weak indicators may be enough to maintain the B cells alive treatment impetigo cheap 0.5 mg cabgolin free shipping, induce modifications in chemokine receptor expression symptoms 3 dpo buy cabgolin 0.5 mg with visa, and promote antigen endocytosis (Table 12. After specific B cells recognize antigens, the following steps in humoral immune responses are very completely different in T-dependent and T-independent responses. We will next describe the activation of B cells by protein antigens and helper T cells. Protein antigens are additionally internalized, processed, and offered to helper T cells. With multivalent T-independent antigens, along with the adjustments listed above, the B cells proliferate and differentiate into IgM antibody-secreting plasma cells. The Sequence of Events During T Cell-Dependent Antibody Responses Protein antigens are independently acknowledged by specific B and T lymphocytes in peripheral lymphoid organs, and the two activated cell sorts interact with one another to initiate humoral immune responses. The activated helper T cells and activated B cells migrate toward one another and work together on the edges of the follicles, where the initial antibody response develops. Some of the activated T and B cells migrate back into follicles to type germinal facilities, where extra specialized antibody responses are induced. Initial Activation and Migration of Helper B Cells and T Cells the contemporaneous activation of particular B and T cells by a protein antigen induces modifications that convey them into proximity to improve the likelihood of the antigenspecific B and T cells colocalizing and interacting with one another. The frequency of naive B cells or T cells specific for a given epitope of an antigen is as little as 1 in 105 to 1 in 106 lymphocytes, and the precise B and T cells have to find one another and physically interact to generate robust antibody responses. This is accomplished partially by regulated movement of the cells following antigen recognition. These classic experimental studies have been among the first to reveal the importance of interactions between two totally different cell populations in the immune system. The activated lymphocytes migrate towards one another and interact on the interface of T and B cell zones. B, the initial T-dependent B cell proliferation and differentiation ends in the formation of an extrafollicular focus, by which B cells proliferate, can undergo isotype switching, and differentiate into plasma cells (mostly short-lived). Some of the T cells which are activated in the extracellular focus develop into follicular helper T cells and migrate again into the follicles, together with some activated B cells, to kind a germinal center. The late events in B cell responses occur in germinal facilities and embody somatic mutation and the number of high-affinity cells (affinity maturation), extra isotype switching, reminiscence B cell era, and the era of long-lived plasma cells, described in later figures. The internet result of these changes is that antigenactivated T and B lymphocytes are drawn towards one another. Protein antigens are internalized by the B cell and presented in a kind that could be recognized by helper T cells, and this represents the following step within the process of T-dependent B cell activation. Antigen-activated helper T cells and B cells move towards each other in response to chemokine signals and make contact adjacent to the sting of primary follicles. The antibodies which may be finally secreted are often particular for conformational determinants of the native antigen as a end result of membrane Ig on B cells is capable of binding conformational epitopes of proteins, and the identical Ig is secreted by plasma cells derived from those B cells. This feature of B cell antigen recognition determines the nice specificity of the antibody response and is independent of the reality that helper T cells recognize solely linear epitopes of processed peptides. The principles outlined here for T-B cell collaboration help to explain a phenomenon that is named the hapten-carrier impact. If, nevertheless, haptens are coupled to proteins, which function carriers, the conjugates are in a position to induce antibody responses against the haptens. Analysis of antibody responses to hapten-carrier conjugates offered among the earliest demonstrations of how antigen presentation by B lymphocytes contributes to the development of humoral immune responses. There are three necessary traits of anti-hapten antibody responses to hapten-protein conjugates. First, such responses require each hapten-specific B cells and protein (carrier)-specific helper T cells. In responses to hapten-carrier conjugates, the hapten (the B cell epitope) is recognized by a specific B cell, the conjugate is endocytosed, the carrier protein is processed in the B cell, and peptides from the service (the T cell epitopes) are presented to the helper T cell. Helper T Cell-Dependent Antibody Responses to Protein Antigens 259 molecules which may be similar to those that had been involved within the initial activation of naive T cells by dendritic cells. All of those options of antibody responses to haptenprotein conjugates could be defined by the antigenpresenting capabilities of B lymphocytes. Hapten-specific B cells bind the antigen by way of the hapten determinant, endocytose the hapten-carrier conjugate, digest the protein element, and present peptides derived from the service protein to carrier-specific helper T lymphocytes. Thus, the 2 cooperating lymphocytes acknowledge completely different epitopes of the identical antigen. The hapten is responsible for environment friendly internalization of the carrier protein into the B cell, which explains why hapten and provider should be bodily linked. The hapten-carrier effect is the premise for the development of conjugate vaccines in opposition to encapsulated micro organism; these vaccines comprise carbohydrate epitopes acknowledged by B cells hooked up to proteins acknowledged by T cells, discussed later in this chapter. T cell-derived cytokines are essential for germinal center reactions, described later. After the preliminary interplay of B cells with helper T cells at the interface between the follicle and the T cell zone, subsequent activation of B cells by helper T cells can happen at two totally different places, one outdoors the follicles in an extrafollicular focus and the opposite in the germinal centers of follicles. The small quantity of antibody produced in these foci could contribute to the formation of immune complexes (containing antigen, antibody, and maybe complement) which might be trapped by follicular dendritic cells in lymphoid follicles. Follicular dendritic cells then launch chemokines, perhaps in response to the immune complexes, which attract a few (often only one or two) activated B cells from the extrafollicular focus into the follicle to provoke the germinal middle response. The extrafollicular response also helps to generate follicular helper T cells (T follicular helper [Tfh] cells) that migrate into the follicle and are required for germinal heart formation. Extrafollicular B Cell Activation B cell activation within the extrafollicular focus provides an early antibody response to protein antigens and units up the subsequent germinal center reaction. Extrafollicular foci of T-dependent B cell activation generate low-affinity antibodies that can circulate and restrict the unfold of an infection. Similar the Germinal Center Reaction the attribute events of helper T cell�dependent antibody responses, together with affinity maturation, isotype switching, and generation of long-lived plasma cells and memory B cells, occur primarily in organized constructions referred to as germinal facilities which would possibly be created inside lymphoid follicles during T-dependent immune responses. The complicated strategy of genetic diversification of activated B cells and survival of the fittest that occurs in these websites is known as the germinal middle reaction. Germinal centers develop roughly 4 to 7 days after the initiation of a T-dependent B cell response. At Helper T Cell-Dependent Antibody Responses to Protein Antigens 261 this time, a few of the B cells which are activated in extrafollicular foci migrate again into the follicle and start to proliferate rapidly, forming a distinct area of the follicle. This area was named the germinal heart by morphologists because of the assumption that new cells were generated ("germinated") there, lengthy earlier than its useful significance was understood. Each fully fashioned germinal center incorporates cells derived from just one or a number of antigen-specific B cell clones. The doubling time of these proliferating germinal middle B cells is estimated to be 6 to 12 hours, so that within 5 days, a single lymphocyte could give rise to as many as 5000 progeny. The progeny of the proliferating B cells within the germinal heart undergo differentiation and selection processes within the gentle zone, described later.
0.5 mg cabgolin otcThis is normally an incidental discovering symptoms irritable bowel syndrome buy cabgolin 0.5mg line, however a nuchal wire might intervene with descent by way of the birth canal throughout delivery and will increase the risk for umbilical twine trauma or constriction of the blood flowing via the cord medications zocor order cabgolin 0.5 mg with mastercard. The cause of the demise on this case is the marked twisting symptoms bipolar generic 0.5 mg cabgolin visa, or torsion bad medicine cheap 0.5 mg cabgolin, of the umbilical cord. Torsion could end result from increased fetal movement, which abnormally lengthens the twine, permitting the fetus to rotate more freely. This represents the consequence of extensive, diffuse fibrin deposition, related to a condition often recognized as maternal floor infarction, and typically referred to as a "gitterinfarkt. The quantity of fibrin on this condition is far higher than the scattered, small deposits of intervillous fibrin regularly observed within a term placenta. This situation is rare, however it has a tendency to recur in subsequent pregnancies. Some instances could also be related to maternal coagulopathies, similar to antiphospholipid syndrome. Syncytial knots might increase in quantity in the placenta during the first week after demise. A clue to this prevalence is greenish staining of fetal skin or fetal surface of the placenta as proven right here. Evidence of fetal misery, followed by observation of greenish staining to the fetal or placental surfaces, should raise suspicion for meconium spillage. Orange-brown balls of meconium (shaped like a rugby ball) and numerous flattened squames or desquamated fetal skin cells which are discovered in the amnionic fluid are proven here inside alveoli. Meconium is an irritant that leads to respiratory distress and chemical pneumonitis. At start, tracheal suction and lung lavage could also be useful to help take away the meconium. It is difficult to decide how far these cells prolong in the skin, so recurrences are frequent after extensive excision. At the best the epithelium is convoluted and the cells are shorter, crowded, and with nuclei exhibiting hyperchromatism. Cervical adenocarcinomas are much less common than squamous carcinomas, accounting for 15% of cervical malignancies. Called sarcoma botryoides, it is a uncommon form of embryonal rhabdomyosarcoma, discovered most frequently in toddler girls and ladies younger than age 5. They arise from preexisting leiomyomata and have an identical microscopic appearance, with low mitotic depend. Note the two pale granulomas here, together with a big Langhans big cell on the higher proper. Disseminated Mycobacterium tuberculosis infections may involve the female genital tract, including the fallopian tube. The giant epithelial cells have plentiful clear cytoplasm that resembles hypersecretory gestational endometrium. Note the ample fibrous stroma between the smaller cystic areas lined by numerous epithelia, together with serous, mucinous, and transitional (Brenner). Note the massive lipid-laden Leydig cells with distinct borders, and corpus albicans at the left. Patients have masculinization with hirsutism, voice adjustments, and clitoral enlargement. These tumors are normally grossly stable, without the prominent skin and hair of a mature teratoma. Lower genital tract, brain, lung, liver, kidney, and gastrointestinal tract are the most common websites for metastases, and this defines the next stage. Even metastases can reply to chemotherapy, and the treatment fee can still approach 75%. Despite the invasion, most of these lesions are self-limited and could be eliminated by curettage after pregnancy. There is continuous thrombosis and fibrosis with shrinkage of vessels, together with hyalinization of the decidual plate, which is eventually shed because the endometrium regenerates. The placenta separates throughout supply above the decidua basalis and beneath the Nitabuch fibrin membrane. This vascular hyperplasia in the terminal chorionic villi is most likely going attributable to extended low-grade hypoxia with uteroplacental abnormalities. This incidental discovering has no scientific significance and have to be distinguished from amnion nodosum. These nodules symbolize foci of precipitated fetal cells and vernix caseosa along with overgrowth of the amniotic epithelium and embedded desquamated fetal pores and skin cells to produce the small nodules. There is an increased incidence of premature delivery, oligohydramnios, abruptio placentae, and intrauterine fetal demise related to this situation. Macromastia may occur unilaterally or bilaterally with increased sensitivity to hormonal stimulation and could additionally be referred to as juvenile hypertrophy when it happens on the time of puberty. Rarely, a supernumerary breast could produce a subcutaneous mass anyplace from the axilla to the perineum. There is one suspicious density, however, which might be a carcinoma or just an space of pronounced sclerosis with fibrocystic changes. A mammogram is a useful screening tool to discover such lesions and to determine the necessity for additional workup. Women of their 30s start to have some involution of lobules and adjacent stroma, and the breast tissue turns into extra radiolucent from an elevated composition of adipose tissue replacing fibrous stroma and lobules. During the normal menstrual cycle, after ovulation under the affect of estrogen and rising progesterone levels, lobular acini improve, epithelial cells turn out to be vacuolated, and the interlobular stromal edema increases, leading to elevated breast fullness. With menstruation and a decrease in hormone levels, apoptosis of epithelial cells and a discount in stromal edema occur. The epithelial cells lining the lumen present apocrine secretion with snouting, or cytoplasmic extrusions, into the lumen. A layer of myoepithelial cells, some of that are slightly vacuolated, is seen simply across the outdoors of the acinus. Assessment of estrogen and progesterone receptors is finished on tissues removed by biopsy or surgery to consider the biologic traits of breast carcinomas. Carcinomas that are hormone delicate could respond to remedy with agents similar to letrozole or tamoxifen. Under the affect of estrogen, terminal ducts and ductal epithelium proliferate, and progesterone promotes development of increased acini within the lobular units. The breast, a modified sweat gland, secretes by budding off of portions of cell cytoplasm (apocrine secretion) to kind breast milk with excessive lipid content material. After supply, estrogen and progesterone ranges decrease, rising the lactogenic impact of prolactin. This pores and skin might fissure, predisposing to an infection with entry of microorganisms into underlying breast tissue. Acute mastitis usually entails only one breast and is most frequently brought on by bacterial organisms such as Staphylococcus aureus, though streptococci can produce this condition, with neutrophilic infiltrates seen here microscopically.
Generic 0.5 mg cabgolin with visaThe responses to protein antigens require T cell help symptoms your period is coming buy discount cabgolin 0.5mg, so these antigens are referred to as T-dependent symptoms 4-5 weeks pregnant cabgolin 0.5mg generic. The time period helper T lymphocyte came from the belief that T cells stimulate medications may be administered in which of the following ways order cabgolin 0.5 mg line, or assist treatment 2 stroke generic cabgolin 0.5mg without a prescription, B lymphocytes to produce antibodies. In Tdependent responses some activated B cells start to produce antibodies aside from IgM; this course of known as heavy chain isotype (class) switching. As the response develops, activated B cells produce antibodies that bind to antigens with increasing affinity, and these B cells progressively dominate the response; this process is known as affinity maturation. In addition to isotype switching and affinity maturation, helper T cells stimulate the manufacturing of long-lived plasma cells and the era of memory B cells. Multivalent antigens with repeating determinants, such as polysaccharides, can activate B cells with out T cell assist. The activation of B cells is initiated by particular recognition of antigens by the surface Ig receptors of the cells. Antigen and other stimuli, including helper T cells, stimulate the proliferation and differentiation of the particular B cell clone. Progeny of the clone could differentiate into plasma cells that produce IgM or other Ig isotypes. T-dependent Protein antigen Helper T cell Isotype-switched, high-affinity antibodies; reminiscence B cells, long-lived plasma cells IgG Follicular B cells IgM IgE Mainly IgM, low-affinity antibodies; short-lived plasma cells IgA T-independent IgM Polysaccharide antigen B-1 cells, marginal zone B cells IgM Other alerts. T-dependent antibody responses to protein antigens mainly contain follicular B cells. T-independent responses to multivalent antigens are mediated primarily by marginal zone B cells in the spleen and B-1 cells in mucosal websites. In a main immune response, naive B cells are stimulated by antigen, turn into activated, and differentiate into antibody-secreting cells that produce antibodies particular for the eliciting antigen. A secondary immune response is elicited when the identical antigen stimulates memory B cells, leading to manufacturing of larger quantities of particular antibody than are produced in the primary response. Note that the traits of secondary antibody responses summarized within the desk are typical of T-dependent antibody responses to protein antigens. Primary responses outcome from the activation of beforehand unstimulated naive B cells, whereas secondary responses are due to the stimulation of expanded clones of reminiscence B cells. Therefore, the secondary response develops extra rapidly than does the primary response, and bigger quantities of antibodies are produced within the secondary response. Distinct subsets of B cells respond preferentially to several sorts of antigens. Follicular B cells in peripheral lymphoid organs primarily make antibody responses to protein antigens, and these B cell responses require collaboration with helper T cells. Marginal zone B cells in the spleen and different lymphoid tissues and B-1 cells in mucosal tissues and the peritoneum recognize multivalent antigens, such as blood-borne polysaccharides, and mount primarily T-independent antibody responses. Some marginal zone B cells participate in T-dependent responses, and some follicular B cells might make T-independent responses. With this background, we proceed to a discussion of B cell activation, starting with the interaction of antigen with B cells. We will then describe the role of helper T cells in B cell responses to protein antigens and the mechanisms of isotype switching and affinity maturation. The antigens then provoke the process of B cell activation, often working in concert with other signals which are generated during innate immune responses triggered by microbes or by adjuvants in vaccines. Antigens that elicit antibody responses could differ in measurement and composition (they could additionally be small, soluble, massive, or particulate) and may be free or sure to antibodies. Soluble antigens, usually smaller than 70 kD, might then reach the B cell zone by way of conduits that reach between the subcapsular sinus and the underlying follicles. Natural antibodies might contribute to the formation of immune complexes and the presentation of some antigens throughout main immune responses. Polysaccharide antigens may be captured by macrophages within the marginal zone of splenic lymphoid follicles and displayed or transferred to B cells in this area. Small antigens are delivered to B cells in follicles through afferent lymphatics and via conduits, and bigger antigens by subcapsular sinus macrophages or by dendritic cells in the medulla. Antigen Recognition and Antigen-Induced B Cell Activation 255 antigens recognized by B and T lymphocytes (see Chapter 6). Although the presentation of antigen to B cells by subcapsular sinus macrophages, macrophages in the splenic marginal zone, and by medullary dendritic cells has been described in experimental fashions, how these cells stop the proteins antigens they seize from being engulfed and degraded remains unclear. First, binding of antigen to the receptor delivers biochemical indicators to the B cells that initiate the method of activation. As discussed later, signaling is more robust with multivalent T-independent antigens than with T-dependent protein antigens. This antigen-presenting operate of B cells will be thought-about later within the context of T-dependent B cell activation. Complement activation typically occurs in response to microbes that activate this system in the absence of antibodies by the choice and lectin pathways, and in the presence of antibodies by the classical pathway (see Chapters four and 13). In all of those situations, complement fragments are generated that bind to the microbes. Some nonmicrobial polysaccharides additionally activate complement by the alternative or lectin pathway, and this is one cause that such antigens are able to induce antibody responses without T cell help. These sample recognition receptors provide alerts that improve or cooperate with these from the B cell receptor complex during B cell activation. In addition, the activation of myeloid cells by way of pattern recognition receptors can promote B cell activation not directly in two methods. Most T-independent antigens, corresponding to polysaccharides, contain a number of identical epitopes on every molecule. Germinal center B cells could be identified by their expression of a transcriptional repressor generally known as Bcl-6 (B cell lymphoma gene 6), whose position is described later when we consider the transcriptional regulation of B cell destiny. B cells at midnight zone and light zone have been called centroblasts and centrocytes, respectively, in the past, but these phrases are less regularly used as a outcome of the cells that cycle between the dark zone and the sunshine zone are comparable in dimension. These molecules are concerned in displaying antigens for the selection of germinal heart B cells, as described later. Selected cells within the light zone return to the darkish zone, and thus B cells bear repeated rounds of mutation and choice. Selected high-affinity B cells in the end differentiate into plasma cells and reminiscence B cells and exit the germinal heart. The rim of naive B cells in the follicle, surrounding the germinal heart, known as the mantle zone. A, the germinal center is throughout the follicle and features a basal darkish zone and an adjoining mild zone. Activated B cells migrate into the follicle and proliferate, forming the dark zone of the germinal middle. These B cells bear somatic hypermutation of Ig V genes and migrate into the sunshine zone, where they encounter follicular dendritic cells displaying antigen and Tfh cells.
Buy 0.5mg cabgolin with amexPosterior to the anal aperture symptoms 2 weeks after conception cheap 0.5mg cabgolin mastercard, the muscle tissue come collectively as a ligament or raphe known as the anococcygeal ligament (anococcygeal body) and attaches to the coccyx symptoms 6 months pregnant buy discount cabgolin 0.5mg line. Anteriorly medicine 93 7338 discount cabgolin 0.5 mg with amex, the muscle tissue are separated by a U-shaped defect or gap termed the urogenital hiatus medications safe during pregnancy cheap 0.5 mg cabgolin. The margins of this hiatus merge with the partitions of the related viscera and with muscular tissues in the deep perineal pouch beneath. The hiatus permits the urethra (in both males and women), and the vagina (in women), to move by way of the pelvic diaphragm. The levator ani muscles are divided into a minimal of three collections of muscle bers, based on site of origin and relationship to viscera within the midline: the pubococcygeus, the puborectalis, and the iliococcygeus muscles. The pubococcygeus originates from the body of the pubis and programs posteriorly to connect along the midline as far back as the coccyx. This part of the muscle is further subdivided on the premise of association with structures within the midline into the puboprostaticus (levator prostatae), the pubovaginalis, and the puboanalis muscular tissues. A second main collection of muscle bers, the puborectalis portion of the levator ani muscles, originates, in affiliation with the pubococcygeus muscle, from the pubis and passes inferiorly on each side to kind a sling across the terminal a half of the gastrointestinal tract. This muscular sling maintains an angle or exure, known as the perineal exure, on the anorectal junction. This angle features as a part of the mechanism that retains the tip of the gastrointestinal system closed. This a part of the muscle originates from the fascia that covers the obturator internus muscle. It joins the same muscle on the other facet in the midline to form a ligament or raphe that extends from the anal aperture to the coccyx. The levator ani muscle tissue assist assist the pelvic viscera and keep closure of the rectum and vagina. Clinical app Defecation At the beginning of defecation, closure of the larynx stabilizes the diaphragm and intra-abdominal pressure is increased by contraction of abdominal wall muscle tissue. As defecation proceeds, the puborectalis muscle surrounding the anorectal junction relaxes, which straightens the anorectal angle. Both the internal and the external anal sphincters also chill out to enable feces to transfer via the anal canal. Normally, the puborectal sling maintains an angle of about 90ďż˝ between the rectum and the anal canal and acts as a "pinch valve" to forestall defecation. When the puborectalis muscle relaxes, the anorectal angle will increase to about 130ďż˝ to 140ďż˝. The fatty tissue of the ischio-anal fossa allows for modifications in the place and size of the anal canal and 217 Pelvis and Perineum anus throughout defecation. During evacuation, the anorectal junction moves down and again and the pelvic oor usually descends barely. During defecation, the round muscular tissues of the rectal wall bear a wave of contraction to push feces toward the anus. As feces emerge from the anus, the longitudinal muscle tissue of the rectum and levator ani bring the anal canal back up, the feces are expelled, and the anus and rectum return to their normal positions. The perineal membrane and deep perineal pouch the perineal membrane is a thick fascial, triangular construction attached to the bony framework of the pubic arch. The perineal membrane is expounded above to a skinny area called the deep perineal pouch (deep perineal space). The parts of perineal membrane and constructions within the deep perineal pouch, enclosed by the urogenital hiatus above, therefore contribute to the pelvic oor and assist parts of the urogenital system within the pelvic cavity, even though the perineal membrane and deep perineal pouch are normally thought-about parts of the perineum. The perineal membrane and adjoining pubic arch present attachment for the roots of the exterior genitalia and the muscles related to them. The urethra penetrates vertically via a round hiatus in the perineal membrane as it passes from the pelvic cavity, above, to the perineum, below. In girls, the vagina also passes by way of a hiatus within the perineal membrane just posterior to the urethral hiatus. Within the deep perineal pouch, a sheet of skeletal muscle functions as a sphincter, mainly for the urethra, and as a stabilizer of the posterior fringe of the perineal membrane (Table 5. Anteriorly, a gaggle of muscle bers encompass the urethra and collectively kind the exterior urethral sphincter. Two additional groups of muscle bers are related to the urethra and vagina in ladies. One group forms the sphincter urethrovaginalis, which surrounds the urethra and vagina as a unit. The second group varieties the compressor urethrae, on all sides, which originate from the ischiopubic rami and meet anterior to the urethra. Together with the external urethral sphincter, the sphincter urethrovaginalis and compressor urethrae facilitate closing of the urethra. In each women and men, a deep transverse perineal muscle on all sides parallels the free margin of the perineal membrane and joins with its associate on the midline. These muscles are thought to stabilize the position of the perineal physique, which is a midline construction along the posterior fringe of the perineal membrane. Perineal physique the perineal body is an ill-de ned however important connective tissue construction into which muscle tissue of the pelvic oor and the perineum attach. It is positioned within the midline alongside the posterior border of the perineal Table 5. The posterior finish of the urogenital hiatus within the levator ani muscles can be related to it. The deep transverse perineal muscle tissue intersect at the perineal body; in women, the sphincter urethrovaginalis additionally attaches to the perineal body. Other muscular tissues that connect to the perineal body embrace the external anal sphincter, the super cial transverse perineal muscular tissues, and the bulbospongiosus muscles of the perineum. Op ening for vagina Opening for urethra External urethral s phincter Dee p trans vers e perineal mus cles Clinical app Episiotomy During childbirth the perineal body may be stretched and torn. Traditionally it was felt that if a perineal tear is likely, the obstetrician could proceed with an episiotomy. This is a procedure by which an incision is made within the perineal body to enable the head of the fetus to cross via the vagina. There are two forms of episiotomies: a median episiotomy cuts via the perineal body, whereas a mediolateral episiotomy is an incision 45ďż˝ from the midline. The maternal bene ts of this procedure have been thought to be much less trauma to the perineum and decreased pelvic oor dysfunction. A Sphincter urethrovaginalis Compres s or urethrae Dee p perine al p ouc h Perineal memb rane Op ening for urethra External urethral s phincter Dee p tra ns vers e perineal mus cles B Perineal memb ra ne De ep pe rine al pouch. The viscera are arranged within the midline, from front to back; the neurovascular provide is thru branches that cross medially from vessels and nerves associated with the pelvic partitions. Gastrointestinal system Pelvic components of the gastrointestinal system consist mainly of the rectum and the anal canal, though the terminal part of the sigmoid colon is also in the pelvic cavity. The rectum, probably the most posterior factor of the pelvic viscera, is straight away anterior to , and follows the concave contour of the sacrum.
Discount cabgolin 0.5 mg mastercardThis central necrosis results in symptoms 9 days after embryo transfer purchase 0.5mg cabgolin fast delivery the gross characteristic of extrusion of cheesy material from the ducts with strain (similar to a comedone) treatment endometriosis generic cabgolin 0.5mg otc. This sample is uncommon medications for ibs purchase cabgolin 0.5 mg with mastercard, however the overall prognosis for patients with comedocarcinoma is usually good symptoms night sweats buy cabgolin 0.5mg low price. The massive Paget cells of Paget disease of the breast have plentiful clear cytoplasm and seem within the epidermis either singly or in clusters. The nuclei of the Paget cells are atypical and, although not seen right here, usually have prominent nucleoli. As it does so, the marked improve within the dense fibrous tissue stroma produces the attribute onerous, scirrhous appearance of the everyday infiltrating ductal carcinoma. Perineural invasion is a frequent characteristic of invasive carcinoma and may account for the boring but fixed character of neoplastic ache. This lesion felt agency on physical examination with palpation and was not freely movable. The reduce surface of this excised lesion felt gritty due to desmoplasia and microcalcifications. The margins of the specimen had been inked with green dye after removal to help in figuring out whether most cancers prolonged to the margins after histologic sections had been made. The mammogram in the proper panel exhibits tiny peripheral calcifications inside a lesion in keeping with a neoplasm within the higher portion above and simply to the left of the marking the purpose at which the patient felt some ache on palpation. There are areas of yellowish necrosis within the parts of neoplasm infiltrating into the encompassing breast and adipose tissue. The attribute "Indian file" strands of infiltrating lobular carcinoma cells are seen here throughout the fibrous stroma. There is a couple of 20% chance that the alternative breast may even be involved, and plenty of of those neoplasms arise multicentrically in the identical breast. Shown here at low energy, sheets and nests of cells are surrounded by a lymphoid stroma with little desmoplasia. These well-differentiated neoplastic cells kind a single cuboidal layer in small, spherical to teardropshaped ductules broadly spaced in a fibrous stroma. The prognosis tends to be higher than for an intraductal carcinoma, despite the multifocal nature and bilaterality which are extra widespread with this variant, due to the well-differentiated nature of the cells and the youthful common age at onset (40s). Most happen as a subareolar mass with nipple discharge in elderly males and have spread to contiguous constructions, giving them a excessive stage at analysis. The identical diagnostic strategies, similar to mammography, can be used for screening and prognosis. At low energy on the right may be seen a duct in a fibrous stroma, with absence of lobules, typical of male breast. Breast cancers most frequently metastasize to the axillary lymph nodes, and these nodes can be sampled or removed on the time of surgery. Rarely, a metastasis is detected first because the primary site is occult and never detectable by physical examination or radiographic imaging techniques. The blue dye round this fibroadenoma was used to mark the lesion throughout needle localization in radiology so that the surgeon may discover this small mass within the breast tissue. Fibroadenomas are widespread causes of breast lumps and the commonest benign breast tumor in women. During reproductive years they might progressively improve in dimension, then they regress after menopause. During menstrual cycles they could cause some pain with transient enlargement in response to increasing estrogen levels. These lesions are most probably to be found as a breast lump on examination in younger women. Some fibroadenomas are true neoplasms, whereas others symbolize polyclonal proliferations. Phyllodes tumors are low-grade neoplasms that not often metastasize but can recur domestically after excision. Projections of stroma between the ducts create the leaflike sample for which these tumors are named (from the Greek word phyllodes, which means "leaflike"). The biologic habits of a phyllodes tumor is troublesome to predict, and it might recur locally, but not often are there high-grade lesions that may metastasize. These neoplasms tend to occur at an older age than do fibroadenomas, most commonly in the sixth decade. In pubertal boys, it could be idiopathic and resolve spontaneously or may persist and require surgical elimination, as in this case. With gynecomastia, this stromal and ductular tissue is elevated, and there could be ductal epithelial hyperplasia, or distinguished periductular edema as here. However, the adjacent breast stroma has quite a few infiltrating discohesive cells representing invasive lobular carcinoma. This gene encodes for an epithelial progress factor receptor on the cell membrane that stimulates mobile proliferation. An underlying breast carcinoma is often palpable in half of ladies at the time of the appearance of an eczematous, pruritic nipple lesion. The presence of an elevated proliferative price (high S phase) and aneuploidy, as shown within the move cytometric sample of this breast carcinoma, suggests a worse prognosis. Embryologically, the anterior pituitary (adenohypophysis) is derived from an upward evagination of the oral cavity, known as Rathke pouch. The posterior pituitary (neurohypophysis) is derived from the diencephalon and consists of modified glial cells (pituicytes) and their axons extending down the pituitary stalk (seen here superiorly) from supraoptic and paraventricular hypothalamic nuclei. The adenohypophysis has a twin blood supply, with a hypophyseal portal system and small perforating arteries. The secretions of these cells are underneath control of hypothalamic-releasing components, that are all constructive acting except for dopamine, which inhibits lactotrophs. They could additionally be null-cell adenomas producing a mass effect, but with out detectable hormonal secretion, or composed of both acidophils or basophils secreting an extra of one hormone (or, much less generally, several hormones). Overall, the most typical forms of pituitary adenomas (and their medical outcomes) embody prolactinoma (amenorrhea-galactorrhea in women, decreased libido in men), followed by null-cell adenoma, corticotroph adenoma (Cushing disease), gonadotroph adenoma (paradoxical hypogonadism), and somatotroph adenoma (acromegaly in adults and gigantism in children). Macroadenomas by their dimension can erode the sella turcica to produce complications and impinge on the optic chiasm to produce visual area defects, most commonly bitemporal hemianopsia, as shown by the diagram. Occasionally there could be acute hemorrhage into the adenoma to enhance the mass effect. Growth hormone�secreting adenomas are commonest in youngsters however are uncommon in adults. Microscopically, there are cystic areas, and nests of squamoid cells are surrounded by columnar cells. Although histologically benign, these neoplasms are difficult to eradicate because of their location and their extension to adjoining constructions corresponding to brain and bone.
Syndromes - Intentionally or unintentionally overdosing on the medications used to treat diabetes
- Heartburn (acid reflux)
- Gradually increase in size of the affected area
- Breathing problems
- Discomfort when opening the mouth
- Spinal tap to remove a sample of CSF (cerebrospinal fluid) for examination
Trusted 0.5 mg cabgolinThe consequence of elevated intraventricular strain and concentric hypertrophy is elevated myocardial oxygen demand treatment jiggers cheap cabgolin 0.5mg free shipping. At the same time medications held before dialysis 0.5 mg cabgolin free shipping, diastolic filling pressure is increased symptoms uterine fibroids discount 0.5mg cabgolin fast delivery, resulting in a lower coronary perfusion stress treatment syphilis buy generic cabgolin 0.5 mg. It leads to ventricular hypertrophy that happens in various patterns, not just involving the interventricular septum. Presenting signs are often dyspnea on exertion, poor exercise tolerance, syncope, palpitations, and fatigue. Some sufferers stay asymptomatic much of their lives and unfortunately are recognized after sudden cardiac death. The resulting strain gradient increases all through systole, creating obstruction to cardiac output. Any factor lowering left ventricular size will improve this gradient and further hinder cardiac output. Examples embrace will increase in coronary heart price and contractility and decreases in preload and afterload. Therefore, anesthetic administration focuses on avoiding tachycardia and maintaining euvolemia and normal systemic vascular resistance. Hypotension on this inhabitants is best treated with -adrenergic agonists and volume. Treatment with inotropic medication similar to epinephrine is contraindicated and may worsen the dynamic obstruction and hypotension. Rapid deterioration of left ventricular operate develops, leading to dyspnea and eventual cardiovascular collapse. Once symptomatic, life expectancy diminishes dramatically, with anticipated survival of only 5 to 10 years. Mitral Stenosis the mitral valve space is often four to 6 cm2 and is made up of an anterior and posterior leaflet. Mitral stenosis is nearly all the time as a outcome of rheumatic coronary heart illness and is subsequently fairly uncommon in the United States and different extremely developed nations. Consequently, the left atrial stress turns into chronically elevated, leading to left atrial dilatation and elevated pulmonary venous pressure. Patients with mitral stenosis are at excessive threat for growing atrial fibrillation, which may be the presenting signal of the disease. Mitral stenosis sufferers are often asymptomatic for many years till the mitral valve space has decreased to 1 to 1. Any excessive cardiac output state or the onset of atrial fibrillation may cause important will increase within the left atrial and pulmonary arterial pressures, resulting in acute congestive coronary heart failure. Chronically elevated left atrial pressures lead to increases in pulmonary vascular resistance, pulmonary hypertension, restrictive lung illness, and proper heart failure. Frequently, sufferers with mitral stenosis have received diuretics preoperatively to management their pulmonary congestion and are relatively hypovolemic. Thus, enough fluid administration during anesthesia is crucial, but an excessive quantity of fluid administration can lead to additional pulmonary congestion and pulmonary edema. The regurgitated blood causes left atrial and ventricular dilatation (eccentric ventricular hypertrophy) and elevated ventricular compliance. Table 35-2 summarizes the hemodynamic goals in sufferers with valvular coronary heart disease. Did You Know the cornerstone within the management of mitral regurgitation is reduction of the systemic vascular resistance to promote forward ejection of blood and limit regurgitation. Diseases of the aorta can be localized to one segment, multiple segments, or contain the entire aorta. The superior mediastinum extends inferiorly from the superior thoracic aperture to the transverse thoracic plane. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2013:160, with permission. Aortic Dissection Aortic dissection occurs because of a tear in the intimal and medial layers of the aorta, which causes separation of the partitions and leads to creation of a false lumen. Blood travels into the false lumen of the media and might journey the length of the vessel. Intimal tears typically originate from an ulcer as a end result of chronic hypertension or connective tissue disorders, such as Marfan syndrome. As the false lumen propagates, thrombus and dissecting layers can cause disruption in perfusion of important organs as a end result of decreased blood flow to main arteries such because the carotids, subclavian, spinal, or mesenteric arteries. Type A aortic dissection, which entails the ascending aorta, is a surgical emergency with a mortality that will increase exponentially by the hour. It is commonly associated with cardiac tamponade, myocardial ischemia (due to dissection of coronary arteries), and acute aortic insufficiency. Type B dissections contain the aorta distal to the left subclavian artery and may be managed medically unless ongoing signs (back pain, stomach pain, or embolic or ischemic phenomenon) persist or end-organ failure develops. Medical therapy focuses on reducing aortic wall stress and controlling heart price and blood pressure with beta-blockers and nondihydropyridine calcium channel blocking agents (2). Patients with kind A dissection require aortic graft placement and might have aortic valve substitute and reattachment of the coronary arteries or arch vessels, relying on the placement of the dissection. Anesthetic administration for aortic dissection involves prevention of hypertension, sufficient intravenous entry, including central venous access, invasive 35 Cardiac Anesthesia 675 Table 35-3 Preload Afterload Contractility Rate Rhythm. Aortic Aneurysm the aorta is an elastic structure that adjustments shape with every cardiac contraction. Degenerative diseases, together with age, hypertension, hypercholesterolemia, and atherosclerosis, cause premature loss of its elasticity and are the major reason for aortic aneurysms. Connective tissue diseases similar to Marfan syndrome cause cystic medial necrosis, principally involving the aortic root. Men are more affected than women and the age of presentation is 50 to 70 years (3). In sufferers with Marfan syndrome or a bicuspid aortic valve, surgical repair is indicated when the aortic diameter reaches four. Aortic repair with or without coronary implantation and aortic valve alternative could also be required in patients with root aneurysms. Involvement of the good vessels could require deep hypothermic circulatory arrest for reconstruction of the aortic arch. Cerebral protective procedures, corresponding to retrograde or antegrade cerebral perfusion, can also be used to present hypothermic protective effects on mind tissue, flush toxins, and decrease the cerebral metabolic rate. Cerebral protective effects are controversial and outcomes have been confounding (4). Left heart bypass, from the left atrium to the femoral artery, can present retrograde aortic perfusion to aortic branches distal to the repair to perfuse the spine and stomach. The anesthetic management for affected person with aortic aneurysms is much like that for sufferers with aortic dissection. Cardiopulmonary Bypass the cardiopulmonary bypass machine is made up of four primary parts: venous and arterial cannulae to take blood from and again to the center, a venous reservoir to gather and transiently retailer the blood drained from the guts, an oxygenator membrane for exchanging carbon dioxide and oxygen, and a pump to propel blood back to the body. The cannula and oxygenator are primed with approximately 800 to 1,500 mL of answer that approximates normal plasma osmolarity. Venous drainage via this cannula occurs passively by gravity siphon and is dependent on proper cannula position and a drop in peak from the heart to the venous reservoir.
Buy cabgolin 0.5mg without prescriptionSide effects can include respiratory depression medications 123 safe 0.5 mg cabgolin, headache symptoms 32 weeks pregnant order cabgolin 0.5 mg on-line, pruritus top medicine order cabgolin 0.5 mg online, peripheral edema treatment management system discount 0.5mg cabgolin overnight delivery, granuloma formation, and hormone disruption. The effectiveness of lumbar interlaminar epidural injections in managing continual low back and decrease extremity ache. Effectiveness of cervical epidural injections in the administration of continual neck and higher extremity ache. Regional anesthesia in the affected person receiving antithrombotic or thrombolytic remedy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (third edition). The physiologic condition of withdrawal symptoms when an opioid is discontinued C. A disease marked by altered habits to seek the specified substance despite negative consequences D. For which affected person is an opioid basal infusion price indicated for intravenous patientcontrolled analgesia Anesthesia for surgical procedures performed in offices and ambulatory surgery facilities is addressed Chapter 25, and anesthesia and analgesia provided for labor and delivery is mentioned in Chapter 31. Children often require sedation or anesthesia for diagnostic and therapeutic procedures. Preoperative communication with the proceduralist is essential and must include dialogue of contingency plans for emergencies and complications. These areas have been typically designed before or without contemplating whether or not anesthesia would be wanted for patients undergoing care. Proceduralists and ancillary workers could additionally be unfamiliar with the necessities for secure anesthesia care and tips on how to help anesthesia suppliers when a problem is encountered. Away from the working room, immediate help from anesthesia colleagues in case of emergency may not be available. Prior to the anesthetic, the presence and correct functioning of all gear wanted for protected patient care must be established; that is described in Table 38-3. Anesthesia care may be regarded as a continuum, with a gradual transition from the awake state, by way of progressively deepening sedation to common anesthesia (Table 38-4) (2). As sedation deepens, progressive blunting of the airway reflexes, with the potential for airway obstruction, together with despair of spontaneous ventilation can ensue. It is, therefore, essential that the person offering sedation be properly educated to take care of a affected person who drifts to a deeper stage of sedation than the extent originally intended. Did You Know the identical standards for working rooms ought to be utilized to sufferers being cared for in all nonoperating room websites. The C-arm moves backwards and forwards across the affected person through the procedure, requiring massive quantities of house, limiting entry to the patient, and serving as a method of dislodging intravenous strains and endotracheal tubes. For youngsters or adults with neurologic or psychological issues, sedation or anesthesia could also be required. Patients with acute thoracic, abdominal, and cerebral trauma usually require pressing imaging to facilitate diagnosis. Hazards of Ionizing Radiation the consequences of ionizing radiation on biologic tissues are categorized as deterministic (severity of tissue harm is dose dependent, corresponding to in cataract or infertility) and stochastic (probability of prevalence is dose associated, similar to in most cancers or genetic effect) (4). Protective measures to reduce affected person publicity to radiation ought to all the time be taken. Using protective shielding (lead aprons, thyroid shields, and leaded eyeglasses) 4. However, magnetizable supplies and digital gadgets characterize potential hazards to the patient and workers. For example, cardiac pacemakers could malfunction, intracerebral aneurysm clips could transfer, and transdermal medicine patches may trigger burns. Did You Know the intensity of the radiation is inversely proportional to the square of the gap from the source (the inverse sq. law). Patient displays, ventilators, and electrical infusion pumps could malfunction in proximity to the scanner, and magnet-safe technology is out there for these instances. Adverse reactions to distinction agents might occur and may be divided into renal adverse reactions and hypersensitivity reactions. Renal Adverse Reactions Contrast agents are eliminated through the kidneys, and patients with pre-existing chronic renal illness, diabetes mellitus, dehydration, advanced age, and concomitant use of nephrotoxic medication. Preventative measures in opposition to contrast-induced nephropathy include sufficient hydration, maintaining an excellent urine output, and using sodium bicarbonate infusions to improve elimination of the contrast agent. Hypersensitivity Reactions Hypersensitivity reactions to distinction media are divided into quick (<1 hour) and nonimmediate (>1 hour) reactions. The clinical manifestations of varied hypersensitivity reactions to contrast media are outlined in Table 38-5. Treatment of reasonable and extreme immediate hypersensitivity reactions is similar to that of anaphylaxis. Diagnostic and Interventional Radiology Angiography Angiography causes minimal discomfort and may be performed under native anesthesia with or without gentle sedation (6). Interventional Neuroradiology Endovascular embolization may be used to deal with cerebral aneurysms, arteriovenous malformations, and certain vascular tumors similar to meningiomas. General anesthesia and conscious sedation are each appropriate strategies for interventional neuroradiology relying on the complexity of the procedure, the need for blood stress manipulation, and the requirement for neurologic assessment during the process. Radiation Therapy External beam radiation is a typical remedy for youngsters with malignancies (Table 38-6) (7). The doses of radiation used are very high, and all personnel should leave the room through the therapy. An interfaced system of closed-circuit television, telemetric microphones, and standard monitoring is used to permit shut remark of the affected person during the process. Complete absence of motion is crucial during radiation therapy and general anesthesia or deep sedation techniques, with propofol the anesthetic of choice throughout these procedures. Light or During interventional procedures, the anesthesiologist could additionally be uncovered to as much if no more radiation than the radiological interventionalist. However, basic anesthesia is more and more required for extra prolonged and complex procedures. Cardioversion Transthoracic cardioversion is usually used electively to deal with dysrhythmias, particularly atrial fibrillation and atrial flutter. A small bolus of intravenous induction agent such as propofol or etomidate is normally adequate for the process. Nonoperating Room Pediatric Cardiac Procedures Cardiac catheterization is performed in children with congenital coronary heart illness for both hemodynamic assessment and interventional procedures. These kids are often very sick and will current with cyanosis, dyspnea, congestive coronary heart failure, and intracardiac shunts. In patients with a patent ductus arteriosus, high oxygen pressure can result in premature closure, and prostaglandin infusions are often used to preserve duct patency. Gastroenterology Procedures generally performed in the gastrointestinal endoscopy suite are outlined in Table 38-2. The majority of these procedures may be carried out with gentle sedation (commonly fentanyl and midazolam or propofol infusion) without the involvement of an anesthesiologist. Local anesthetic is sprayed into the oropharynx to facilitate passage of the endoscope. Under basic anesthesia, patients usually require tracheal intubation to shield the proximal airway, which is shared with the endoscope in the course of the process.
Purchase cabgolin 0.5mg free shippingBecause of the anatomical position of the sigmoid colon there are a variety of problems that will occur medicine to stop vomiting purchase cabgolin 0.5 mg. In ammation may spread to the bladder section 8 medications discount cabgolin 0.5 mg on line, producing a stula between the sigmoid colon and the bladder symptoms quad strain discount cabgolin 0.5 mg fast delivery. De s ce nding colon Clinical app Bowel obstruction A bowel obstruction can be both mechanical or practical: Mechanical obstruction is caused by an intraluminal symptoms cervical cancer generic 0.5 mg cabgolin with amex, mural, or extrinsic mass, which could be secondary to a international body, obstructing tumor in the wall, or extrinsic compression from an adhesion, or an embryological band. A practical obstruction is usually because of an inability of the bowel to peristalse, which again has a number of causes, and most regularly is a postsurgical state as a outcome of excessive intraoperative bowel handling. Small bowel obstruction is often attributable to adhesions following earlier surgery, and history should all the time be searched for any operations or stomach interventions. Other potential causes include hernias and in ammatory diverticular disease of the sigmoid colon. The instrument is often made of a exible plastic materials via which a lightweight supply and eye piece are attached at one end. In gastrointestinal and abdominal medication, an endoscope is used to assess the esophagus, stomach, duodenum, and proximal small bowel. The tube is swallowed by the patient underneath gentle sedation and is extremely properly tolerated. Assessment of the colon is performed by passage of the tube via the anus and into the rectum. Surfaces of the liver embody: a diaphragmatic surface in the anterior, superior, and posterior directions, and a visceral surface in the inferior path. The porta hepatis serves as the purpose of entry into the liver for the hepatic arteries and the portal vein, and the exit point for the hepatic ducts. Diaphragmatic floor the diaphragmatic surface of the liver, which is smooth and domed, lies towards the inferior floor of the diaphragm. The hepatorenal recess is a component of the peritoneal cavity on the best aspect between the liver and the best kidney and right suprarenal gland. Associated ligaments the liver is hooked up to the anterior stomach wall by the falciform ligament and, aside from a small area of the liver against the diaphragm (the bare area), the liver is almost utterly surrounded by visceral peritoneum. Additional folds of peritoneum connect the liver to the abdomen (hepatogastric ligament), the duodenum (hepatoduodenal ligament), and the diaphragm (right and left triangular ligaments and anterior and posterior coronary ligaments). Right lobe Left lobe Diaphragm Visceral surface the visceral floor of the liver is roofed with visceral peritoneum except within the fossa for the gallbladder and on the porta hepatis (gateway to the liver;. The right lobe of liver is the biggest lobe, whereas the left lobe of liver is smaller. The quadrate and caudate lobes are described as arising from the right lobe of liver, but functionally are distinct. The quadrate lobe is visible on the anterior part of the visceral surface of the liver and is bounded on the left by the ssure for ligamentum teres and on the right by the fossa for the gallbladder. The caudate lobe is seen on the posterior a half of the visceral surface of the liver. It is bounded on the left by the ssure for the ligamentum venosum and on the best by the groove for the inferior vena cava. Imaging app Visualizing the liver Quadrate lobe Gallbladder Portal vein Inferior vena cava Right lobe of liver Right crus Left lobe of liver Neck of pancreas Stomach Aorta Spleen Left crus Left kidney. Left hepatic artery Right hepatic artery Left fuel tric artery Hepatic artery correct Clinical app Ostomies It is sometimes essential to surgically externalize bowel to the anterior belly wall. Gastrostomy is carried out when the abdomen is connected to the anterior belly wall and a tube is positioned via the pores and skin into the abdomen. The jejunostomy is used as a site where a feeding tube is positioned by way of the anterior belly wall into the proximal efferent small bowel. Cys tic artery Supraduodenal artery Gas troduodenal artery Right fuel tric artery Abdominal aorta Superior mes enteric artery Splenic artery. Clinical app Segmental anatomy of the liver For many years the segmental anatomy of the liver was of little importance. However, for the reason that growth of liver resection surgical procedure, the dimensions, shape, and segmental anatomy of the liver has become clinically important, particularly with regard to liver resection for metastatic illness. The liver is divided by the principal airplane, which divides the organ into halves of approximately equal measurement. This imaginary line is de ned by a parasagittal line that passes through the gallbladder fossa to the inferior vena cava. Importantly, the principal airplane divides the left half of the liver from the best half. The lobes of the liver are unequal in dimension and bear solely little relevance to operative anatomy. The conventional eight segment anatomy of the liver pertains to the hepatic arterial, portal, and biliary drainage of those segments. It has: a rounded end (fundus of gallbladder), which may project from the inferior border of the liver; a major half within the fossa (body of gallbladder), which can be against the transverse colon and the superior part of the duodenum; and a slender half (neck of gallbladder) with mucosal folds forming the spiral fold. It extends throughout the posterior belly wall from the duodenum, on the best, to the spleen, on the left. The pancreas is (secondarily) retroperitoneal apart from a small part of its tail and consists of a head, uncinate course of, neck, body, and tail. Projecting from the decrease a half of the pinnacle is the uncinate process, which passes posterior to the superior mesenteric vessels. Posterior to the neck of the pancreas, the superior mesenteric and the splenic veins be part of to type the portal vein. The body of pancreas is elongate and extends from the neck to the tail of the pancreas. It passes to the right by way of the body of the pancreas and, after getting into the top of the pancreas, turns inferiorly. In the lower part of the top of pancreas, the pancreatic duct joins the bile duct. The joining of those two structures varieties the hepatopancreatic ampulla (ampulla of Vater), which enters the descending (second) a part of the duodenum on the main duodenal papilla. Surrounding the ampulla is the sphincter of ampulla (sphincter of Oddi), which is a collection of smooth muscle cells. The accessory pancreatic duct empties into the duodenum simply above the most important duodenal papilla at the minor duodenal papilla. If the accent duct is followed from the minor papilla into the top of the pancreas, a branch level is discovered: One department continues to the left, by way of the pinnacle of the pancreas, and should join with the pancreatic duct at the point where it turns inferiorly. A second branch descends into the lower part of the pinnacle of pancreas, anterior to the pancreatic duct, and ends in the uncinate process. The presence of these two ducts re ects the embryological origin of the pancreas from dorsal and ventral buds from the foregut. Clinical app Annular pancreas the pancreas develops from ventral and dorsal buds from the foregut.
Buy generic cabgolin 0.5mg lineThe cortex is fibrotic symptoms 2 months pregnant buy 0.5 mg cabgolin overnight delivery, the glomeruli are sclerotic from hyaline obliteration symptoms endometriosis order cabgolin 0.5mg fast delivery, there are scattered interstitial continual inflammatory cell infiltrates symptoms gallstones 0.5 mg cabgolin visa, and the arteries are thickened medications medicare covers buy cabgolin 0.5 mg lowest price. Tubules are sometimes dilated and filled with pink casts and give an appearance of "thyroidization. Diminished renal clearance of phosphate predisposes to secondary hyperparathyroidism. This glomerulosclerosis is attributable to metabolic alterations with hyperglycemia, with a marked increase in mesangial matrix from cellular harm secondary to nonenzymatic glycosylation of proteins. Also observe the markedly thickened arteriole on the decrease proper, which is typical of hyaline arteriolosclerosis seen in diabetic kidneys. In early phases of this illness, microalbuminuria is present, however it progresses to overt proteinuria that presages renal failure. Diffuse glomerulosclerosis is related to long-standing kind 1 or 2 diabetes mellitus. Changes of glomerulosclerosis with diabetes mellitus take a decade or longer to develop and gradually worsen. Patients with diabetes mellitus, whether kind 1 or 2, are in danger for many renal illnesses, including nephrosclerosis, pyelonephritis, and papillary necrosis, in addition to glomerulosclerosis. The end-stage renal illness seen right here with small native kidneys and granular surfaces was handled in the left panel with renal transplantation. In this case the affected person developed persistent rejection, which is why the transplant kidney is slightly swollen with focal hemorrhages. In the proper panel the smaller reddish kidney has undergone infarction from renal arterial thrombosis. The distribution of necrosis and apoptosis is more segmental with ischemic accidents, as proven right here, with some tubules nonetheless having intact epithelium, whereas others show appreciable harm. Lesser levels of injury with lack of the comb border and cell swelling are frequent. The patient may be maintained on dialysis until the recovery section occurs with polyuria. Incompetence of the vesicoureteral valve can predispose to reflux with retrograde move of urine. In kids this is most often attributable to congenital shortening of the intravesical portion of the ureter. Decreased bladder contraction from autonomic neuropathy or spinal wire damage can result in reflux in adults. Shown here are numerous inflammatory cells, mainly neutrophils, filling renal tubules and increasing into the interstitium. This case of acute pyelonephritis resulted from an ascending urinary tract infection that started within the bladder. Nearly all such cases are brought on by bacterial organisms, including Enterobacteriaceae (Escherichia, Klebsiella, Proteus, Providencia, Edwardsiella, Enterobacter) and streptococci and staphylococci. Urinary stasis from congenital anomalies, obstructive uropathy, or decreased bladder emptying may predispose to ascending urinary tract an infection. This pattern of acute pyelonephritis is commonest of hematogenous dissemination of an infection to the kidney in patients with septicemia. Ascending urinary tract infection resulting in acute pyelonephritis is more frequent than the hematogenous route. A rare complication not seen right here is papillary necrosis, which is extra more doubtless to occur in sufferers with diabetes mellitus or urinary tract obstruction. This is an unusual however extreme complication of acute pyelonephritis, significantly in sufferers with diabetes mellitus or urinary tract obstruction. Papillary necrosis can also occur with analgesic nephropathy or sickle cell disease. An extensive acute pyelonephritis difficult this course of, and the an infection became difficult by a perinephric abscess that prolonged to the right flank region, seen right here as irregular areas of decreased attenuation throughout the skeletal muscle of the posterior flank and back on the best. This has adopted severe inflammation and atrophy from hydronephrosis and pyelonephritis. Nearly complete or total obstruction with extensive irritation destroys renal parenchyma. Nephrectomy could also be accomplished in circumstances of pyonephrosis as a result of the kidney turns into nonfunctional and serves solely as a source of continuing infection. If this process is unilateral, the issue originates from a disease involving a location from the ureteral orifice as a lot as the renal pelvis. In this case, an obstructing urinary tract calculus had been current for many years. Vesicoureteral reflux, most often manifesting in childhood, could produce an analogous discovering. If the obstructive course of had been bilateral, the underlying illness would originate within the bladder trigone or urethra (or the prostate across the urethra of males) or some course of. There are coarse, discrete, corticomedullary scars that overlie dilated, blunted, or deformed calyces. Lymphocytes and plasma cells characteristic of chronic pyelonephritis are seen at excessive magnification (right panel). Causes embrace chronic urinary obstruction resulting from a calculus (often a staghorn calculus), stricture, or impinging neoplasm, all conditions which are more frequent in middle-aged adults. Like a malignancy, it might prolong into the perinephric fat and adjacent retroperitoneal structures. In either case, microscopically many pale to foamy macrophages (xanthoma cells) are current, along with inflammatory round cells from breakdown of renal parenchyma with ongoing inflammation. For obscure causes, abnormalities in liver perform happen in half of affected sufferers. Urinalysis findings are often absent, though urine tradition might yield the typical bacterial organisms found in urinary tract infection. Shown listed here are scattered eosinophils, along with neutrophils and mononuclear cells in an infected interstitium, indicative of acute kidney damage. There may be fever, peripheral blood eosinophilia, a skin rash, oliguria, hematuria, and proteinuria. Half of instances result in acute renal failure with rising serum urea nitrogen and creatinine. The aspirin inhibits formation of prostaglandin (a vasodilator) to potentiate ischemic injury. An acute urate nephropathy can occur with a "lysis" syndrome resulting from massive cellular necrosis of leukemia or lymphoma cells with chemotherapy. An extra complication of hyperuricemia is nephrolithiasis with uric acid calculi. The pale pink casts might act as a foreign body and elicit a multinucleated big cell response round them. Additional renal issues with a number of myeloma include amyloidosis, light-chain glomerulopathy, hypercalcemia with nephrocalcinosis, hyperuricemia with urate nephropathy, and urinary tract infection with pyelonephritis. The process could additionally be termed benign in most older adults who proceed to have normal renal operate, as decided by normal serum creatinine and urea nitrogen ranges. There may be a mild discount in the glomerular filtration price and mild proteinuria.
References - Park, S.J., Kim, J.K., Kim, K.W., Cho, K.S. MDCT Findings of renal trauma. AJR Am J Roentgenol 2006;187:541-547.
- Moore JW, George L, Kirkpatrick SE, et al. Percutaneous closure of small patent ductus arteriosus using occluding spring coils. J Am Coll Cardiol. 1994;23:759-65.
- Yang Y, Shuaib A, Li Q, et al: Neuroprotection by delayed administration of topiramate in a rat model of middle cerebral artery embolization, Brain Res 804:169-176, 1998.
- Morey AF, Iverson AJ, Swan A, et al: Bladder rupture after blunt trauma: guidelines for diagnostic imaging, J Trauma 51:683n686, 2001.
- Nickel, J. C., & Sorensen, R. (1996). Transurethral microwave thermotherapy for nonbacterial prostatitis: A randomized, double-blind sham controlled study using new prostatitis specific assessment questionnaires. Journal of Urology, 155, 1950n1954.
- Weiner DJ, McDonough J, Perez M, et al. Heated, humidified high-flow nasal cannula therapy. Pediatrics 2008;121:1293-4.
- Hoebeke P, Van Laecke E, Van Camp C, et al: One thousand video-urodynamic studies in children with non-neurogenic bladder sphincter dysfunction, BJU Int 87:575-580, 2001.
- Navari RM, Sullivan KM, Springmeyer SC, et al. Mycobacterial infections in marrow transplant patients. Transplantation. 1983;36: 509-513.
|