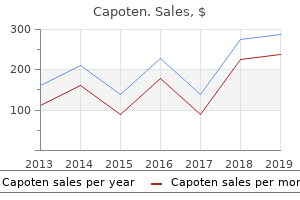
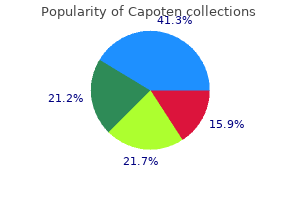
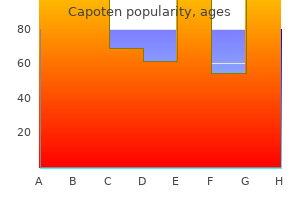
Capoten
Lisa Countryman-Jones, BS, MT(ASCP) CLS, CPT(NCA), ACCE - Faculty Member, Clinical Practice Coordinator
- Medical Laboratory Technology Program
- Portland Community College
- Portland, Oregon
Buy cheap capoten 25mg onlineRomeo et al 3 later biopsied shoulders in every stage and reported their histological findings medicine rash order capoten 25 mg with visa. Capsular tissue is regular on biopsy medications listed alphabetically best capoten 25 mg, whereas the synovium is hypervascular and hypertrophic medicine used to treat chlamydia generic 25 mg capoten with mastercard. Treatment of idiopathic adhesive capsulitis ranges from skillful neglect to surgical intervention symptoms adhd cheap capoten 25 mg otc. Grey4 revealed profitable ends in 24/25 sufferers with use of straightforward analgesics at a minimal of two years. However, Hand et al5 more just lately revealed on 269 shoulders with adhesive capsulitis. They reported only 59% of patients having normal/near regular outcomes using the Oxford Shoulder Score and 41% with ongoing signs, principally mild in nature. These 2 research most likely vary considerably due to the variable end result measures used. The majority of the research showed improved medical end result measures and passive shoulder motion at early follow-up. Similar to the oral steroid literature, these benefits over the comparability remedies had been transient and equalized at newest follow-up. Despite the restricted literature exhibiting its profit, physical therapy is the most popular treatment modality for adhesive capsulitis. A Cochrane database review found no strong proof to support the use of remedy alone as treatment. Conversely, the extent I examine revealed by Kivimaki et al19 reported solely slightly better forward flexion at 3 months when compared to the house train group. It allows for full inspection of the joint, affirmation of the analysis, and staging of the disease. The advantages of arthroscopic capsular launch have been reported in lots of printed studies. Most are in settlement that release of the rotator interval, middle glenohumeral ligament, and anterior band of the inferior glenohumeral ligament is important. Resection of the posterior capsule arguably advantages patients with inside rotation deficits. However, Snow et al 23 challenge this profit by reporting no difference in vary of movement when a posterior release is incorporated. A 360-degree capsular release with or without a partial resection of the intra-articular portion of the subscapularis has gained recognition. Jerosch, 24 Le Lievre and Takagi, 22 and LaFosse et al 25 report passable outcomes using barely totally different circumferential capsular releases. The objective for this chapter is to present the principal findings in the diagnostic analysis of a affected person with primary adhesive capsulitis as well as the step-by-step process the authors employ when performing a pancapsular release for refractory circumstances. Indications Loss of passive and active vary of movement refractory to no much less than 4 to 6 months of gentle progressive stretching (physical therapy or home remedy program) Controversial Indications Single stage rotator cuff repair in a stiff shoulder Superior migration of humeral head with rotator cuff tear Capsular launch coupled with debridement for glenohumeral osteoarthritis Arthroscopic Pancapsular Release 183 Pertinent Physical Findings Loss of exterior rotation with arm on the side Pain at end ranges of shoulder movement and evening pain (early findings) No particular areas of tenderness Referred pain to origin of deltoid Loss of each passive and lively vary of motion External rotation and abduction most notably affected Mild: exterior rotation > forty five levels Moderate: external rotation < forty five degrees Severe: exterior rotation < 10 degrees Extension and adduction hardly ever affected Pertinent Imaging Radiographs: regular Magnetic resonance imaging: not essential for prognosis. This is reported extra frequently by radiologist however with little medical correlation. Equipment 30- and 70-degree arthroscopes Arthroscopic shaver with oscillating characteristic Arthroscopic tissue biters/scissors Radiofrequency unit Positioning and Portals Positioning: Beach chair and lateral decubitus positions are acceptable for the arthroscopic capsular launch. The authors prefer the lateral decubitus position with the arm positioned in suspension at 50 to 60 degrees of abduction with 10 to 12 lbs of balanced suspension. Portals: posterior and anterior (established utilizing outside-in method) Step-by-Step Description of the Procedure Peripheral nerve block administered by anesthesia using ultrasound. Single injection vs steady infusion via a catheter Examination underneath anesthesia: evaluate the passive vary of movement of both the affected and unaffected shoulders. Document forward elevation, exterior rotation, and internal rotation in 0 degrees of abduction and ninety levels of abduction and cross-body motion. Place the affected person in a lateral decubitus place with suspension/tension as outlined beforehand. Sterile preparation of the skin with sterile draping Establish posterior portal Anterior portal established utilizing both the inside-out or outside-in technique Diagnostic intra-articular shoulder examination. Evaluate for findings of synovitis, thickened capsule, and loss of intra-articular quantity. Complete the discharge of the rotator interval tissue, together with the superior glenohumeral ligament. Identification of the coracoid course of is vital to avoiding debriding too far medially. Care should be taken to keep within the capsule adjacent to the labrum to shield other constructions. This will free the anterior capsule, subscapularis bursa, center glenohumeral ligament, and anterior band of the inferior glenohumeral ligament. Underlying subscapularis tendon and muscle tissue is visible following enough release. This contains the whole launch of the superior glenohumeral ligament and superior capsule. Using switching sticks, place arthroscopic camera through anterior portal and shaver/radiofrequency system by way of the posterior portal. This will free the posterior capsule and posterior band of the glenohumeral ligament. Subacromial decompression is usually not essential, and plenty of sufferers with idiopathic frozen shoulder have a normal subacromial bursoscopy. Postoperative Protocol Formal physical remedy program begins on postoperative day 0 or 1. Continuous passive motion devices are used between bodily remedy periods set for a snug vary of movement. The most important element of the postoperative program is the avoidance of pain while going by way of the vary of motion workout routines. Potential Complications Recurrent stiffness Anterior dislocation Axillary nerve palsy Top Technical Pearls for the Procedure 1. Arthroscopic pancapsular release must be performed only after failure of a minimum of four to 6 months of mild progressive stretching. When releasing the capsule from the glenoid, stay within 1 to 2 cm of the labrum to keep away from harm to important constructions (subscapularis, axillary nerve). Utilizing the inside-out approach to establish the anterior portal is usually useful in an distinctive stiff shoulder when visualization of the subscapularis border is difficult because of the contractures and scarring. At the conclusion of an intensive launch, muscle must be visible at all of the margins of the release. The Shoulder: Rupture of the Supraspinatus Tendon and Other Lesions in or About the Subacromial Bursa. Anti-inflammatory medicine in periarthritis of the shoulder: a doubleblind, between patient study of naproxen versus indomethacin. Short course prednisolone for adhesive capsulitis (frozen shoulder or stiff painful shoulder): a randomized, double blind, placebo controlled trial. Adhesive capsulitis of the shoulder: a scientific review of the effectiveness of intra-articular corticosteroid injections.
Order 25mg capoten otcThere are three common situations relating to treatment yellow fever discount capoten 25 mg amex nerve dysfunction after distal radius fracture shinee symptoms capoten 25mg with visa. This indicates an acute carpal tunnel syndrome at finest and impending compartment syndrome at worst medications prolonged qt discount 25 mg capoten. If signs are significant then decompression is warranted however not on an emergent basis treatment 3rd degree burns purchase 25 mg capoten with amex. This is an unstable fracture as indicated by the damage mechanism, the comminution, and the gentle tissue component, leading to nerve compression. Surgery should embody discount and secure plate fixation of the fracture in addition to median nerve decompression. A distal radial volar periarticular plate with enough length to bridge the comminution should be used and discount should consider restoring radial length, alignment, and any intra-articular step. It is really helpful that concurrent carpal tunnel decompression ought to be carried out via a separate incision. This avoids ulnar zig-zagging of the Henry incision to meet the carpal tunnel incision which locations the palmar cutaneous department of the median nerve at risk. Answers these are radiographs of the thumb of a skeletally mature patient displaying a dorsal dislocation of the thumb metacarpophalangeal joint. Most dislocations of the thumb metacarpophalangeal joints are dorsal, although palmar dislocations have also been reported. The mechanism of injury involves hyperextension with related complete rupture of the volar plate. Any traction utilized to reduce the dislocation tightens this noose, making discount troublesome. In his authentic description of the surgical approach for an irreducible dorsal dislocation Farabeuf used a dorsal incision. Also, it may be simpler to tackle any associated metacarpal head fractures using a dorsal method. Kaplan described a volar approach for the treatment of irreducible dorsal dislocations. Eaton and Dray described a technique of releasing the A1 pulley, which then releases tension on the flexor tendons allowing the proximal phalanx and attached volar plate to scale back into their anatomical positions. This is a plain radiograph of a thumb exhibiting an avulsion fracture of the proximal phalanx suggestive of avulsion of the ulnar collateral ligament. Valgus stress to the thumb can end result in ligamentous or bony disruption of the ulnar collateral ligament. This can even lead to rupture of the dorsal capsule, adductor mechanism, and extensor pollicis brevis tendon which can improve the diploma of instability discovered on examination. When the right collateral ligament is ruptured, instability might be present when the thumb is examined in flexion. Chronic ulnar collateral ligament injury usually results from the failure of a patient to seek recommendation following an acute damage. Management depends on the underlying condition of the metacarpophalangeal joint. The graft is woven via the metacarpal neck and the proximal phalanx and secured with suture anchors. In long-standing cases patients can develop arthritic changes and would profit from fusion of the metacarpophalangeal joint. This is a clinical photograph displaying a nail bed injury affecting a significant part of the proximal nail fold. I wish to get a radiograph of this finger to assess the underlying harm to the distal phalanx to be able to plan additional management. I want to acquire a full historical past of the mechanism of damage and examine for any related medical situations that will impact on the general management of this patient, such as diabetes mellitus or heavy smoking. I would like to assess the integrity of the flexor and extensor tendons by checking the mobility of the finger tip. Furthermore plain radiographs are wanted to guarantee any underlying fracture is identified. After a full medical examination I would assess for any underlying bone lack of the distal phalanx. I would watch out in ablating the nail, shortening the bone, and preserving the flexor and extensor insertions. Nail bed accidents can be categorized broadly into those involving exposure of the bone and those with out bone exposure. Surgical management is influenced by the kind of soft tissue loss, which could be classified as volar oblique, dorsal indirect, or transverse. If the bone is uncovered then the affected person will need a flap, which depends upon the sort of gentle tissue loss. Large wounds with uncovered bone and dorsal indirect injuries could be managed with cross-finger flaps. In the long run the affected person can current with stiffness within the finger, especially if the finger needs immobilization as in treatment with a cross-finger flap. Failure to remove all of the germinal matrix can result in nail spikes or nail cysts. Scarring of the eponychium and nail fold to the nail mattress is recognized as pterygium; this results in practical and aesthetic deformities such as an absence of nail development and splitting of the nail. Hooking of the nail occurs with tight closure of a fingertip amputation or lack of bony support beneath the nail mattress, which outcomes in curving of the matrix in a volar course. Many patients with finger tip accidents complain of temperature sensitivity, primarily in cold weather, and this should be explained to the patient upfront. Answers that is an anteroposterior view of the wrist showing an established non-union of the scaphoid. The blood supply to the scaphoid has been thought of to be an important explanation for nonunion. The blood supply comes from branches of the radial artery that enter the bone via dorsal foramina. As these are mainly located distally, the proximal pole has a poor blood supply, increasing the risk of non-union. The diploma of displacement of the fracture or instability of the fracture may be related. Proximal pole fractures have high non-union charges and all of these factors may play a job. The size of time from fracture to diagnosis and institution of the right therapy might influence the union rate. The objective of remedy is to obtain union, relieve signs, and cut back the long-term threat of osteoarthritis in the joint. If the non-union is established then inside fixation with bone grafting is suitable. If a affected person presents late with a non-union and already has osteoarthritic change within the wrist joint, what salvage procedures might you contemplate Simple procedures embody radial styloidectomy, excision of a half of the scaphoid-usually the proximal pole-and denervation of the wrist joint. More formal reconstructive procedures embrace scaphoid excision and four-corner fusion, arthroplasty, proximal row carpectomy, and total wrist fusion.
Cheap capoten 25 mg on lineWhen measured on a scanogram symptoms 5dpo order capoten 25 mg with amex, the injured extremity is 1 cm shorter than the unhurt one medications for ocd order 25mg capoten with visa, with the entire discrepancy in the femur treatment pneumonia discount 25 mg capoten visa. Patella dislocation Tibial eminence avulsion fracture Tibial tubercle avulsion fracture Medial collateral ligament harm Anterior cruciate ligament rupture Patella tendonitis Patella fracture Posterolateral corner harm Quadriceps tendon rupture For each of the next eventualities select probably the most acceptable choice from the list treatment effect buy capoten 25mg line. An 11-year-old boy falls off his bicycle and presents with a big haemarthrosis however no palpable point bony tenderness. When playing football a 14-year-old boy kicks the ground as a substitute of the ball, sustaining a knee injury. A 15-year-old woman sustains an harm to her knee while altering course in a netball match. Valgus Procurvatum Recurvatum Valgus and recurvatum Valgus and procurvatum Varus and recurvatum Varus and procurvatum For each of the next eventualities choose the most applicable possibility from the record. Which is the classic deformity of a non-operatively treated proximal metaphyseal tibial fracture Which deformity that may be anticipated with isolated fracture of the tibia at midshaft level Lateral two-part triplane Medial three-part triplane Lateral three-part triplane Medial two-part triplane Pronation�eversion exterior rotation Supination�plantar flexion Supination�inversion Supination�adduction For each of the following situations select essentially the most applicable possibility from the record. Minimal swelling and deformity but ache and tenderness over anterolateral tibia are discovered with injury mechanism Answers: 1-A; 2-G; 3-A the majority of clavicle fractures in children could be handled non-operatively. The 16-year-old in Question 2, with problem swallowing and respiration, has sustained a sternoclavicular joint injury- either a dislocation or extra doubtless at physeal separation. These can usually be handled conservatively, however in the case of impingement on midline constructions they require discount and stabilization. Conservative interventions for treating middle third clavicle fractures in adolescents and adults. Outcome of distal clavicular fracture separations and dislocations in immature skeleton. Answers: 1-C; 2-F; 3-G Common accidents to the new child on account of traumatic delivery include humeral and clavicle fractures, as well as humeral�physeal separations-best seen on ultrasound. Humeral fractures in children are nicely tolerated, but relative indications for fixation include growing age and polytrauma. Answers: 1-C; 2-A; 3-A, B, and D Medial epicondyle fractures are frequent injuries in kids and adolescents between the ages of 9 and 14. They account for up to 20% of all elbow fractures in the paediatric inhabitants and 60% of cases associated with elbow dislocation. Clinically, there may be swelling and local tenderness immediately over the medial epicondyle. In considerably displaced fractures (>5 mm), the fragment remains proximal to the true joint floor. The key medical discovering is often a block to elbow movement, specifically extension. Documented absolute indications for surgical intervention embrace open fractures and fracture fragments incarcerated within the joint. Relative surgical indications embrace ulnar nerve dysfunction and valgus instability of the elbow, as nicely as high-demand higher extremity perform. Operative versus nonoperative administration of pediatric medial epicondyle fractures: a systematic review. Answers: 1-C and E; 2-A; 3-B Fractures of the lateral condyle commonly occur in children between the ages of 5 to 10. In Milch kind I the fracture extends by way of the ossification centre of the capitellum and enters the joint lateral to the trochlear groove. The most generally used system (not recognized by name) identifies three fracture patterns. Answers: 1-C; 2-B; 3-D Radial neck fractures in youngsters may be categorized utilizing the Judet system. Answers: 1-C; 2-D; 3-H the Salter�Harris classification describes physical fractures in kids. Risk factors related to lack of position after closed reduction of distal radial fractures in youngsters. Answers: 1-A; 2-B and C; 3-C and F; 4-D, F, and G; 5-E the management of paediatric femoral fractures varies with age and also the load of the kid. Social circumstances ought to be taken into account-more just lately a shift in the path of fixation to enable for earlier discharge has been favoured. Answers: 1-D; 2-E; 3-G Distal femoral fractures in kids must be recognized and treated promptly. Leg length discrepancy of (or predicted to be) <2 cm should be accepted and could be efficiently treated with a shoe raise only. Predicted discrepancy of 2�5 cm ought to be addressed by epiphysiodesis of the contralateral leg with appropriate timing utilizing an Eastwood�Cole chart. Discrepancy of >5 cm is normally beyond catch-up development and an ipsilateral lengthening process ought to be considered. Significant angular deformity can be addressed with hemiepiphysiodesis and osteotomy in isolation or together. The impact of percutaneous pin fixation in therapy of distal femoral physeal fractures. A loud pop in a non-contact scenario is almost pathognomonic for anterior cruciate ligament rupture in all ages. An important clue to the most likely site of extensor mechanism disruption is age. Although not all the time the case, the lesion usually becomes extra proximal as age increases: <16 years, tibial tubercle avulsion; 16�35, patella tendon rupture; 35�60, patella fracture; >60 years, quadriceps tendon rupture. Answers: 1-B; 2-A; 3-B the Cozen fracture is the proximal tibial metaphyseal fracture that dangers a typical valgus deformity of uncertain aetiology. The aetiology of valgus angulation after metaphyseal fractures of the tibia in kids. Answers: 1-A; 2-I; 3-D A Tillaux fracture represents an exterior rotation force pulling on the unevenly fused distal tibial physis. Some authors imagine the Tillaux and triplane fractures are brought on by related mechanisms but with higher energy seen within the triplane. A Tillaux fracture is a extra refined damage, which might easily be missed due to restricted medical and radiographic signs. Specific pathways for investigation and administration ought to be in place in all establishments caring for children with fractures.
Order capoten 25mg on lineLesion at the level of the cerebral peduncle (crus cerebri) (3): con-tralateral spastic hem iparesis medications dispensed in original container buy 25 mg capoten otc. Lesion at the level of the pons (4): contralateral hem iparesis or bilateral paresis medicine qid capoten 25mg free shipping, relying on the dimensions of the lesion medications purchase 25mg capoten free shipping. Because the bers of the pyram idal tract occupy a larger cross-sectional space in the pons than in the inside capsule symptoms 8 days after ovulation best 25 mg capoten, not all the bers are dam aged in m any instances. For example, the bers for the facial nerve and hypoglossal nerve are usually una ected because of their dorsal location. Dam age to the ab - ducens nucleus m ay cause ipsilateral dam age to the trigem inal nucleus (not shown). Lesion at the degree of the pyramid (5): Flaccid contralateral paresis happens as a outcome of the bers of the extrapyram idal m otor pathways. Lesion at the stage of the spinal wire (6, 7): A lesion at the level of the cervical twine (6) results in ipsilateral spastic hem iplegia as a outcome of the bers of the pyram idal and extrapyram idal system are intently interwo ven at this degree and have already crossed to the opposite aspect. A lesion on the degree of the thoracic cord (7) leads to spastic paralysis of the ipsilateral leg. Lesion on the degree of the peripheral nerve (8): this lesion dam ages the axon of the alpha m otor neuron, resulting in accid paralysis. This fact was unknown when pyramidal tract lesions were rst described, nevertheless, and it was assumed that a pyramidal tract lesion led to spastic paralysis. Because this truth has few sensible implications, spasticit y remains to be described in some textbooks because the basic signal of a pyramidal tract lesion. In most circumstances it would be wager ter simply to regard spastic paralysis as a type of central paralysis. The spinal twine ends approxim ately at the L 1 degree, and the neural tissue within the vertebral canal beneath that stage consist s solely of ventral and dorsal roots (see additionally p. The ventral m otor root and dorsal sensory root unite in the intervertebral foram en to kind the spinal nerve. The root s enter and em erge from the spinal dural sac through t wo separate openings (b). This is the anatom ical basis for the reality that sensory de cits (pain, lack of sensation) and m otor de cits (m uscular weakness ranging to paralysis) m ay develop individually in patient s with nerve root compression (see E). L2 C8 C7 L3 S5 S4 S3 S2 L4 C8 C7 S1 L5 L4 L5 B Projection of radicular innervation to the pores and skin: dermatomes After the dorsal and ventral root s unite to type the spinal nerve (see A), their nerve bers are distributed to their respective territories. Functiona l Systems Sensory dorsal root Spinal nerve in the intervertebral foram en Peripheral nerve Maxim um space provided by a cutaneous nerve Dorsal ram us Cutaneous nerve Dorsal root ganglion Sympathetic trunk Autonom ous space of a cutaneous nerve Overlapping territories of t wo cutaneous nerves Plexus Intercostal nerve C Location of a radicular lesion A radicular lesion is situated on the ventral m otor root or dorsal sensory root bet ween its website of em ergence from the spinal wire and the union of both root s to form a peripheral nerve. The derm atom es on the lim bs are shifted because of m igratory processes during em bryonic developm ent, but the derm atom es on the trunk retain their segm ental pat tern of innervation (see B and D). Lateral cutaneous branches Anterior cutaneous branches D Radicular innervation of the trunk the segm ental arrangem ent of the m usculature is preserved in the trunk, and so the trunk retains a segm ental (radicular) innervation pattern. It could be seen that a erent bers from the sympathetic trunk reach the peripheral nerves distal to the root s. This explains why radicular lesions are often not related to autonom ic de cits in the a ected derm atom es. Cauda equina Nucleus pulposus Anulus fibrosus L5 vertebral physique L4 root L5 root E Pressure on spinal nerve roots from a herniated lumbar disk of L4/5 A herniated intervertebral disk m ay exert pressure on the spinal nerve root or cauda equina. The disk consist s of a central gelatinous core (nucleus pulposus) and a peripheral ring of brocartilage (anulus brosus). When the anulus brosus is dam aged, m aterial from the gelatinous core m ay be extruded by way of the ring defect and impinge upon the foundation at it s entry into the intervertebral foram en. This is a frequent reason for radicular sym ptom s, which have t wo grades of severit y: � Irritation of the nerve root in the area of the intervertebral foramen. This leads to pain in the low back (lum bago), probably accompanied by ache radiating into the lower lim b in the derm atone of the a ected root (sciatica). This dam ages the L5 root passing behind the herniated disk however not the descending L4 root, which has already entered the intervertebral foram en at that level. Only a far lateral disk herniation will dam age the root that exits on the sam e level as the a ected disk. The m aterial herniates through the posterior longitudinal ligam ent and impinges on the cauda equina. The locations of the de cit s related to speci c root lesions are described in the subsequent unit. Just as the a ected derm atome indicates the site of the sensory root lesion, the a ected muscle indicates the level of the broken spinal wire segment or its root. The m uscles which are predominantly provided by a specific spinal wire phase are referred to as its indicator muscle tissue (analogous to the derm atomes for the dorsal roots). Because indicator muscle tissue are equipped predominantly but, as a rule, not solely by a single segment, a lesion in a single segm ent or spinal nerve root normally causes weak point (paresis) of the a ected m uscle rather than full paralysis (plegia). The indicator muscles within the higher and lower limbs are listed within the tables below. Whereas sensory (dorsal) root lesions may occur in isolation, motor (ventral) root lesions usually occur in affiliation with dorsal root lesions, and due to this fact the derm atomes are additionally listed within the tables. Note: Because the nerves of the trunk are derived instantly from the spinal nerve roots with none intervening plexuses, the pat tern of segm ental innervation in the trunk is equivalent to the pat tern of peripheral innervation. Cord section Indicator muscle C Clinical manifestations of nerve root irritation � Pain within the a ected derm atom e � Sensory losses in the a ected derm atom e C4 C5 C6 C7 C8 L3 L4 L5 S1 Diaphragm Deltoid Biceps brachii Triceps brachii Hypothenar m uscles, exor digitorum profundus on ulnar aspect Quadriceps fem oris Quadriceps fem oris, vastus m edialis Extensor hallucis longus, tibialis anterior Triceps surae, peronei, gluteus maximus � Increased ache throughout coughing, sneezing, or straining � Pain bers m ore severely a ected than other sensory bers � Motor de cits within the indicator muscles of the section � Re exes associated with the a ected segment are absent or diminished. By de nition, t wo form s of brachial plexus paralysis are distinguished: upper brachial plexus paralysis, which is brought on by a lesion of the C 5 and C 6 ventral ram i (see C), and lower brachial plexus paralysis, which is brought on by a lesion of the C eight and T 1 ventral ram i (see D). C 7 kind s a "watershed" guess ween the t wo form s of paralysis and is t ypically una ected by both form. Because the ventral ram i carry both m otor and sensory bers, a brachial plexus lesion all the time causes a com bination of m otor and sensory de cit s. The resulting paralysis (see C) is always of the accid t ype due to it s peripheral nature (lesion of the second m otor neuron). The arm hangs limply on the side (loss of the upper arm exors), and the palm faces backward (loss of the supinator with dom inance of the pronators). There m ay even be partial paralysis of the extensor m uscles of the elbow joint and hand. Typical circumstances current with sensory disturbances on the lateral surface of the higher arm and forearm, but these signs m ay be absent. It a ect s the hand m uscles, the digital exors, and the exor m uscles in the wrist (claw hand with atrophy of hand m uscles, a). Because the sympathetic bers for the pinnacle go away the spinal cord at T 1 (b), the sympathetic innervation of the head is also lost. This is m anifested by a unilateral Horner syndrome, characterised by m iosis (contracted pupil due to paralysis of the dilator pupillae) and narrowing of the palpebral ssure (not ptosis) because of a lack of sympathetic innervation to the superior and inferior tarsal m uscles. The narrowed palpebral ssure m im ics enophthalm os (sinking of the eyeball into the orbit). The lum bosacral plexus is divided right into a lum bar plexus (T 12�L4) and sacral plexus (L5�S 4). The inferior bers of L4 as nicely as all bers of L5 m erge to kind the lum bosacral trunk, which is the connection to the sacral plexus.
Order capoten 25 mg lineShe asked her husband to come indoors treatment thesaurus purchase capoten 25 mg on-line, but he fainted as soon as he tried to stand medicine 029 purchase capoten 25mg free shipping. The spouse known as for an ambulance medications high blood pressure purchase capoten 25 mg fast delivery, and the person was taken to a hospital and diagnosed with a situation referred to as heatstroke symptoms zoloft dosage too high buy discount capoten 25mg on line. Based on that, what would you expect to happen to skin blood vessels when a person first begins feeling warm Conversely, as in our instance right here, if physique temperature increases, warmth production decreases and warmth loss will increase. When our affected person began gardening on a hot, humid day, his body temperature began to increase. At first, the blood vessels in his skin dilated, making him appear flushed and helping him dissipate warmth throughout his skin. To understand this, we must consider that a number of homeostatic variables were disrupted by his activities. As the sweating continued, it resulted in decreased fluid ranges and a negative balance of key ion concentrations in his body; this contributed to a lower in psychological operate, and he grew to become confused. As his body fluid levels continued to lower, his blood strain additionally decreased, further endangering mind perform. By doing so, the extra important organs of the body-such because the brain-could receive adequate blood. It additionally made it tougher for sweat glands in the pores and skin to acquire the fluid required to produce sweat. The man steadily decreased perspiring and finally stopped sweating altogether. Often, when one physiological variable similar to body temperature is disrupted, the compensatory responses initiated to correct that disruption cause, in turn, imbalances in other variables. These secondary imbalances must even be compensated for, and the importance of each imbalance should be "weighed" against the others. In this example, the person was treated with intravenous fluids made up of a salt answer to restore his fluid levels and concentrations, and he was immersed in a cool bathtub and given cool compresses to assist reduce his body temperature. Efferent pathways carry info away from the integrating heart of a reflex arc. In a reflex arc initiated by touching a hand to a hot range, the effector belongs to which class of tissue The kind of tissue involved in many types of transport processes, and which regularly lines the internal surfaces of tubular constructions, is called. Physiological adjustments that occur in anticipation of a future change to a homeostatic variable are known as processes. A is a chemical issue released by cells that acts on neighboring cells without having to first enter the blood. When lack of a substance from the body exceeds its achieve, an individual is claimed to be in balance for that substance. The Inuit of Alaska and Canada have a outstanding ability to work within the cold with out gloves and never endure decreased skin blood circulate. Explain how an imbalance in any given physiological variable could produce a change in one or more different variables. Indeed, in such a situation, pores and skin blood vessels would dilate to bring heat blood to the skin surface, where the warmth could depart the body across the pores and skin. A fascinating view inside actual human our bodies that additionally incorporates animations to assist you to understand homeostasis, the central concept of physiology. To fully recognize the mechanisms by which homeostasis is achieved, we must first understand the essential chemistry of the human body, including the key options of atoms and molecules that contribute to their capacity to work together with each other. Such interactions form the idea for processes as numerous as maintaining a wholesome pH of the body fluids, figuring out which molecules will bind to or in any other case influence the perform of different molecules, forming useful proteins that mediate quite a few physiological processes, and sustaining energy homeostasis. In this chapter, we also describe the distinguishing characteristics of a variety of the main organic molecules in the human body. The particular functions of those molecules in physiology will be introduced right here and mentioned more absolutely in subsequent chapters where acceptable. This chapter will give you the data required to finest respect the significance of one of the basic principles of physiology introduced in Chapter 1, particularly that physiological processes are dictated by the laws of chemistry and physics. Each sort of atom-carbon, hydrogen, oxygen, and so on- is called a chemical element. A one- or two-letter symbol is used as an abbreviated identification for each component. Although greater than a hundred components occur naturally or have been synthesized within the laboratory, solely 24 (Table 2. Components of Atoms the chemical properties of atoms may be described in phrases of three subatomic particles-protons, neutrons, and electrons. The bigger the atom, the more electrons it incorporates, and subsequently the extra orbitals that exist across the nucleus. Orbitals are found in regions known as electron shells; further shells exist at higher and higher distances from the nucleus as atoms get bigger. An atom such as carbon has more shells than does hydrogen with its lone electron, however fewer than an atom similar to iron, which has a larger number of electrons. The second shell can maintain up to eight electrons; the first two electrons fill a spherical orbital, and subsequent electrons fill three additional, propeller-shaped ("p") orbitals. Additional shells can accommodate additional orbitals; this can happen once the internal shells are filled. First electron shell is full of two electrons s orbital of second electron shell is crammed with two electrons Major Elements: ninety nine. Up to two electrons might occupy an orbital, shown here as areas by which an electron is prone to be found. The orbitals exist within electron shells at progressively larger distances from the nucleus as atoms get bigger. Chemical Composition of the Body and Its Relation to Physiology 21 An atom is most steady when the entire orbitals in its outermost shell are crammed with two electrons each. For most of the atoms which might be most important for physiology, the outer shell requires eight electrons in its orbitals so as to be crammed to capacity. Protons have one unit of optimistic cost, electrons have one unit of adverse charge, and neutrons are electrically neutral. Because the protons are positioned in the atomic nucleus, the nucleus has a internet positive charge equal to the number of protons it incorporates. One of the elemental principles of physics is that reverse electrical charges appeal to each other and like expenses repel each other. It is the attraction between the positively charged protons and the negatively charged electrons that serves as a major drive that varieties an atom. The whole atom has no web electrical cost, however, as a outcome of the variety of negatively charged electrons orbiting the nucleus equals the number of positively charged protons in the nucleus.
Cheap capoten 25mg otcA neuron treatment 1st metatarsal fracture generic capoten 25 mg visa, endocrine gland cell medicine werx discount 25 mg capoten visa, and different cell kind may all secrete the same chemical messenger symptoms 7 days after conception purchase capoten 25mg line. In some instances medicine vials discount 25mg capoten with amex, a particular messenger might typically function as a neurotransmitter, a hormone, or a paracrine or autocrine substance. All types of intercellular communication described so far on this section involve secretion of a chemical messenger into the extracellular fluid. The first type happens by way of gap junctions, which are bodily linkages connecting the cytosol between two cells (see Chapter 3). Molecules can move immediately from one cell to an adjacent cell by way of gap junctions without coming into the extracellular fluid. For example, the messenger could also be a plasma membrane protein with part of its construction extending into the extracellular space. When the cell encounters one other cell sort able to responding to the message, the 2 cells link up by way of the membrane-bound protein. This kind of signaling, typically termed juxtacrine, is of specific significance in the progress and differentiation of tissues in addition to in the functioning of cells that shield the body in opposition to pathogens (Chapter 18). It is a technique by which similar forms of cells "recognize" each other and type tissues. Let us take sweating in response to heat exposure as an example and carry out a easy experiment. On day 1, we expose a person for half-hour (min) to an elevated temperature and ask her to do a standardized train check. The sweating offers a mechanism for increasing heat loss from the body and subsequently tends to minimize the increase in body temperature in a sizzling surroundings. Then, for a week, our subject enters the warmth chamber for 1 or 2 hours (h) per day and workouts. On day 8, her body temperature and sweating price are again measured throughout the same train test carried out on day 1. The striking finding is that the topic begins to sweat sooner and much more profusely than she did on day 1. She has undergone an adaptive change induced by repeated publicity to the warmth and is now higher in a place to respond to warmth exposure. The precise anatomical and physiological changes that bring about elevated capability to stand up to change throughout acclimatization are extremely varied. Typically, they involve a rise within the quantity, dimension, or sensitivity of a number of of the cell varieties in the homeostatic control system that mediates the essential response. Biological Rhythms As noted earlier, a striking characteristic of many body capabilities is the rhythmic modifications they manifest. The most typical type is the circadian rhythm, which cycles approximately once each 24 h. They add an anticipatory element to homeostatic management systems, in impact, a feedforward system operating with out detectors. The negative feedback homeostatic responses we described earlier Body temperature (�C) 38 Lights on Lights off 37 36 6:00 A. Note the increase in physique temperature that occurs simply prior to lights on, in anticipation of the increased activity and metabolism that occur throughout waking hours. In contrast, the brain referred to as the hypothalamus, a particular collection of neubiological rhythms enable homeostatic mechanisms to be utilized rons (the suprachiasmatic nucleus) functions as the principal immediately and automatically by activating them at times when pacemaker, or time clock, for circadian rhythms. During sleep, metabolism is slower than ment effects exerted by the external surroundings. In flip, the during the energetic hours, and subsequently body temperature decreases pacemaker sends out neural indicators to different components of the brain, at the moment. One output of the pacemaker goes to the drive the rhythm but quite provide the timing cues important for pineal gland, a gland inside the mind that secretes the hormone entrainment, or setting of the particular hours of the rhythm. These neural alerts from the pacemaker trigger the sic experiment will make clear this distinction. It has been hypothesized, therefore, that melatonin isolated them from their ordinary exterior environment, including may act as an important mediator to influence different organs either information of the time of day. For the primary few days, they have been immediately or by altering the activity of the parts of the mind that exposed to a 24 h rest�activity cycle in which the room lights management these organs. Under these Balance of Chemical Substances in the Body conditions, their sleep�wake cycles were 24 h long. Then, all environmental time cues have been eradicated, and the subjects were Many homeostatic systems regulate the stability between addition allowed to management the lights themselves. On common, bedtime began about is a generalized schema of the possible pathways concerned in 30 min later each day, and so did wake-up time. The pool occupies a place of central wake cycle endured in the full absence of environmental importance in the stability sheet. In this quantity of the substance and is commonly identical to the quantity prescase, it was approximately 24. The pool receives substances and that cues are required to entrain or set a circadian rhythm to 24 h. Thus, if several folks had been present process the experiment simply be synthesized inside the physique from other supplies. A substance may be misplaced within the urine, feces, expired room, social cues would entrain all of them to the identical rhythm. The substance can also be chemirhythms-in other words, to reset the interior clock. The substance could also be shifts take time, nevertheless, and the disparity between external time taken from the pool and amassed in storage depots-such and inner time is considered one of the causes of the signs of jet lag-a as the accumulation of fats in adipose tissue. Homeostasis: A Framework for Human Physiology 13 leave the storage depots to reenter the pool. Finally, the substance may be included reversibly into another molecular structure, similar to fatty acids into plasma membranes. Incorporation is reversible as a outcome of the substance is liberated once more whenever the more complicated structure is broken down. This pathway is distinguished from storage in that the incorporation of the substance into different molecules produces new molecules with particular functions. For any substance, three states of total-body steadiness are potential: (1) Loss exceeds acquire, in order that the total quantity of the substance within the physique is decreasing, and the person is in negative stability; (2) achieve exceeds loss, in order that the whole amount of the substance in the body is rising, and the person is in positive steadiness; and (3) gain equals loss, and the individual is in secure stability. Clearly, a steady stability can be upset by a change in the amount being gained or misplaced in any single pathway within the schema. Conversely, secure balance may be restored by homeostatic control of water consumption and output. The focus of Ca21 in the extracellular fluid is important for regular mobile functioning, notably muscle cells and neurons, but in addition for the formation and maintenance of the skeleton. The control techniques for Ca21 balance target the intestines and kidneys such that the amount of Ca21 absorbed from the food regimen is balanced with the quantity excreted within the urine. During infancy and childhood, nevertheless, the web balance of Ca21 is optimistic, and Ca21 is deposited in growing bone.
Discount 25mg capoten visaPrediction of below-knee amputation wound healing using noninvasive laser Doppler velocimetry symptoms gastritis order 25 mg capoten otc. Percutaneous oxygen tension Percutaneous oxygen tension is the gold normal for measuring vascular inflow medications you can buy in mexico buy capoten 25mg mastercard. The ratio of Doppler strain at the degree being tested to the brachial systolic pressure the ratio of Doppler strain at the level being examined to the brachial systolic strain defines the ischaemic index of the limb treatment spinal stenosis discount capoten 25 mg visa. A post-menopausal lady with a fracture is obtainable remedy for osteoporosis depending on her threat components symptoms 8 weeks pregnant buy capoten 25mg low cost. Teriparatide can additionally be really helpful if a girl has another fracture and her bone density has fallen while taking alendronate, risendronate, or etidronate. Fracture liaison companies must be supplied in all orthopaedic clinics-they will handle all required aspects of the management of osteoporosis outlined in options B�E. It is characterized by pain, irregular regulation of blood circulate, sweating, and trophic modifications divided into three phases. Phase 1: vasomotor response, swelling and vasodilatation, less than three months from damage. Phase 2: dystrophic part, vasoconstriction, increased stiffness, 3 months to a yr from damage. Treatment focuses on tricyclic antidepressants, opioids, and selective neural blockade corresponding to guanethidine blocks, however typical therapies produce an unpredictable outcome. Imaging in early posttraumatic advanced regional ache syndrome: a comparability of diagnostic strategies. Epidural haematomas typically turn out to be biconvex or lenticular in form as they push the adherent dura away from the inner desk of the skull C. Epidural haematomas are most frequently positioned within the temporal or temporoparietal areas D. Epidural haematomas usually result from a tear of the center meningeal artery as the outcomes of a fracture E. Epidural haematomas classically current with a lucid interval between time of injury and neurological deterioration 3. Fluid resuscitation in children should begin with an isotonic fluid bolus of fifty ml/kg B. Hypotension occurs late in paediatric hypovolaemic shock and represents a state of decompensated shock C. If the child deteriorates during fluid resuscitation consideration must be given to the early use of 10 ml/kg of packed purple blood cells D. The weight of a child in kilograms may be estimated utilizing the method (2 � age in years) + 10 5. Initial plantar sensation is prognostic of long-term useful consequence and ought to be a component of a limb-salvage decision algorithm B. More consideration to the psychological in addition to the physical health of sufferers who sustain a limb-threatening damage could also be wanted to ensure an optimum recovery C. Patients with extreme, bilateral lower extremity accidents should be counselled that, no matter treatment mixtures, the function of each limb is analogous at 2 and 7 years D. Severity of soft tissue damage has the best impact on decision-making regarding limb salvage versus amputation E. Smoking places the affected person in danger for elevated time to union and problems 6. Current people who smoke are approximately 5 occasions more prone to develop an an infection than non-smokers D. He is taken to the nearest main trauma centre with a tough collar on a spinal board. Application of a pelvic binder if one has not already been utilized by paramedics B. Continue close monitoring with a low threshold for initiation of a massive transfusion protocol C. After optimization (including warfarin reversal) she stays frail with poor cardiorespiratory reserve. Uncemented (Thompson/Austin Moore) hemiarthroplasty on the next routine trauma list thirteen. The incidence of unstable spine accidents in unconscious sufferers with vital blunt trauma is. Which of the following is the pressing investigation of alternative for a spinal twine injury What is the utmost acceptable time delay for vascular reconstruction if confirmed vascular impairment exists in a decrease limb Following preliminary wound excision, which antibiotics ought to be administered for an open fracture In an open fracture, following wound, soft tissue, and bone excision, for what duration ought to antibiotics be given A battlefield tourniquet should be applied to the limb Early use of a tourniquet in combat situations has led to a discount in morbidity from haemorrhagic limb injuries. Use of tourniquets and their effects on limb perform in the modern combat environment. The major objective of remedy for patients with suspected traumatic brain injury is to forestall secondary brain injury. Pressures larger than 20 mmHg, particularly if sustained and refractory to remedy, are associated with poor outcomes. Tachycardia and poor pores and skin perfusion are often the one keys to early recognition of hypovolaemia. A lower in blood pressure and different indices of inadequate organ perfusion, similar to urinary output, should be monitored closely, but usually develop later. This research included a subset of fifty five patients with an insensate foot at presentation. The insensate foot following severe decrease extremity trauma: an indication for amputation Treatment with narcotic treatment in the course of the first three months Chronic pain is significantly extra widespread following severe lower extremity trauma than within the basic inhabitants. Prevalence of continual pain seven years following limb threatening lower extremity trauma. Current smokers are approximately five times extra more doubtless to develop an an infection than non-smokers Patients within the current smokers group had been twice as prone to develop an an infection and three. Log roll the affected person to study the spine for related injuries Log rolling a patient with a potentially unstable pelvic ring damage is contraindicated. This risks mechanical disturbance to the clot that has fashioned in the retroperitoneum. Ipsilateral tibial fracture Early stabilization of lengthy bone fractures is useful, but in sure conditions harm control surgery with exterior fixation and later conversion to intramedullary nailing could be indicated. It must also be considered if other injuries are present that could be impacted by intramedullary nailing, corresponding to head and chest accidents. Cemented hemiarthroplasty on the next routine trauma listing Non-operative administration is associated with excessive morbidity and a low probability of regaining unbiased mobility. A current trial in nonagenarians found comparable mortality in each groups, but better function in those who acquired surgical procedure.
Capoten: 25 mg
Order capoten 25 mg free shippingSome surgeons favor a bigger distal gap in the pusher treatment kidney cancer discount 25mg capoten amex, which permits for deliberate passage over the knot medications rapid atrial fibrillation buy 25mg capoten with amex. Double-holed knot pushers and self-tensioning suture devices are additionally available medications and side effects buy 25mg capoten free shipping, however these have largely fallen out of favor medications with weight loss side effect buy capoten 25 mg amex. Some knot pushers are open-sided, which allows for engagement of the suture limbs throughout the joint or inside the cannula. These knot pushers are inclined to disengage from the suture limb (which can be a nuisance), and they can sometimes rating or fret the suture (which weakens it). Some surgeons favor to use a "sixth-finger" design, which permits for persistent tension on the knot whereas half-hitches are delivered, using one instrument to accomplish both tasks. Some surgeons are snug flipping posts on sequential throws without changing the knot pusher, just by preferential pull on one suture strand or the other. Some surgeons choose to bodily swap the knot pusher from one limb to the other, which provides a bit of time to the process. This approach facilitates selection of the best technique by every individual surgeon. In basic, arthroscopic knots should all the time be delivered down an arthroscopic cannula. Violation of this principle may end up in substantial frustration and sometimes technical failure as a end result of sutures can encircle nontarget tissues during knot supply. It is a very good idea to take away all sutures, other than the two strands which are being tied, which normally requires use of a loop grasper or crochet hook to ship sutures out one other portal or cannula. It is easy for sutures to turn out to be tangled with one another throughout the cannula during knot tying and, once they turn into entangled, it could be extraordinarily difficult to right. Sutures may be "parked" exterior of the cannula throughout the similar pores and skin portal, but care must be taken to keep away from injury to sutures by the exterior threads of the cannula itself. Suture safety may be facilitated by utilizing small plastic "straws" as tiny conduits that shield the sutures. The major message is to keep away from tangling sutures by maintaining solely the 2 strands of concern inside the cannula throughout knot tying. This extra step (which requires only a little bit of time) shall be rewarded by decreased frustration and larger overall surgical effectivity. Arthroscopic Knot Tying 5 Arthroscopic Suture Materials Arthroscopic sutures could be monofilament or braided, absorbable or nonabsorbable, and standard power or excessive power (so known as super-sutures). High-tensile strength sutures include Hi-Fi (ConMed Linvatec), Ultrabraid (Smith & Nephew), FiberWire (Arthrex), and Orthocord (DePuy Mitek). Once a monofilament suture is passed via the tissue, it can be tied round a limb of braided suture with a easy overhand throw. As pressure is utilized to the opposite end of the monofilament suture, the braided limb is delivered by way of the target tissue. Alternatively, commercially out there shuttling units can serve the same purpose. Antegrade suture-passing instruments have made the management of braided sutures much more convenient, whereby braided suture may be superior in a single step by way of the tissue on the tip of a needle. Some antegrade devices are additionally self-capturing, which eliminates the want to grasp the suture with an impartial gadget. Care should be taken when utilizing these gadgets as the sharp needles can minimize or nick beforehand placed sutures. Super-sutures lower the incidence of suture breakage throughout knot tying, which minimizes this previously frequent expertise with commonplace energy suture. Super-sutures are far more immune to fraying than conventional suture materials. Super-sutures can be quite slippery, and some investigators have reported an inclination for knot slippage with out suture breakage with various super-sutures. It is helpful to reap the advantages of the target suggestions offered by a knot tester if potential in order to maximize proficiency throughout the range of materials which are prone to be used in the operating room. Some super-sutures are so sturdy that they induce glove tears and finger lacerations during arthroscopic shoulder surgical procedure. More importantly, skin lacerations are a mirrored image of the amount of drive that may be applied by super-sutures throughout the glove and into the finger. Surgeons must be conscious of glove tears throughout surgical procedure to find a way to reduce the chance of bacterial contamination from the skin of the surgeon. Specific Arthroscopic Knots (Sliding and Nonsliding) Many arthroscopic knots are well-described in the literature. Most knots work nicely as lengthy as the surgeon understands and adheres to elementary ideas of knot safety and loop safety, together with proper use of back up halfhitches. Every arthroscopic surgeon have to be comfortable with a minimal of 2 "go-to" knots for the 6 Chapter 1 working room. It is efficient and efficient to become facile and technically according to a minimal of one sliding knot, one nonsliding knot, and, if potential, one sliding-locking knot. Sliding knots are advantageous because the knot is configured exterior of the arthroscopic cannula. The knot is then delivered to the target location by the post strand sliding by way of tissue and the suture anchor. It is due to this fact necessary to routinely assess suture sliding earlier than creating the knot. Sliding knots require a shortened post, which returns to appropriate working length because the knot is delivered and the publish is retrieved. Some surgeons choose to use a nonsliding knot routinely, which consists of a sequence of reversed halfhitches on alternating posts. The main driver of success is meticulous surgical approach and a focus to detail, as opposed to particular knot choice. There are instances throughout surgical procedure when a sliding-locking knot is advantageous, corresponding to when the repair has a tendency to "spring again" from the goal tissue. This tendency can create loop expansion and associated gap formation at the restore web site in the brief second between primary knot placement and half-hitch delivery. The approach for delivering and securing a sliding-locking knot involves 3 sequential steps: 1. Tripping and locking the knot by pulling on the non-post limb It is necessary to remove all loop slack by deliberate pretension of the publish limb. Surgical assistants, significantly the person holding the arthroscope, ought to watch the monitor rigorously during this stage of the process. It is essential to advise the operating surgeon if the loop loosens at any level throughout knot tying because this is a correctable downside whether it is identified earlier than the position of further half-hitches. Arthroscopic knot safety is achieved by the location of at least 3 reversed throws on alternating posts to again up the preliminary knot.
References - Sanchez-de-Badajoz, E.D.-R.F., Vara-Thorbeck, C. Endoscopic varicocelectomy. J Endourol 1990;4:371-374.
- Mirza W, McHugh K, Aslam M, et al: CT pelvis in children; should we routinely scan pelvis for Wilms tumor and hepatoblastoma? Implications for imaging protocol development, J Coll Physicians Surg Pak 25:768n770, 2015.
- O'Ryan F, Schendel S. Nasal anatomy and maxillary surgery. II. Unfavorable nasolabial esthetics following the Le Fort I osteotomy. Int J Adult Orthodon Orthognath Surg 1989;4:75.
- Chaganti RS, Houldsworth J: The cytogenetic theory of the pathogenesis of human adult male germ cell tumors. Review article, APMIS 106(1):80n83, discussion 83n84, 1998.
- Richstone, L., Montag, S., Ost, M., Reggio, E., Permpongkosol S., Kavoussi, L.R. Laparoscopic partial nephrectomy for hilar tumors: evaluation of short-term oncologic outcome. Urology 2008;71:36-40.
- Silver SA, Tavassoli FA. Primary osteogenic sarcoma of the breast: a clinicopathologic analysis of 50 cases. Am J Surg Pathol. 1998;22(8):925-933.
- Bauer RM, Mayer ME, Gratzke C, et al: Prospective evaluation of the functional sling suspension for male postprostatectomy stress urinary incontinence: results after 1 year, Eur Urol 56:928n933, 2009.
- Ahonen J, Jokela R. Recombinant factor VIIa for lifethreatening post-partum haemorrhage. Br J Anaesth 2005; 94: 592-5.
|