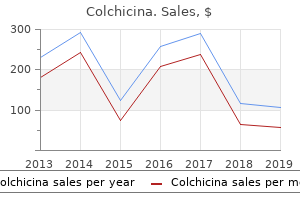
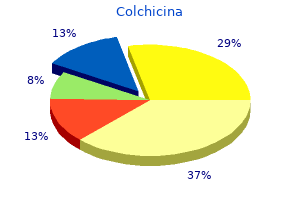
Colchicina
Bruce D. Spiess, MD, FAHA - Professor of Anesthesiology and Emergency Medicine
- Director of VCURES
- VCUñMedical College of Virginia
- Richmond, Virginia
Cheap colchicina 0.5 mg on lineOthers best antibiotic for gbs uti purchase colchicina 0.5mg with amex, evaluating ileum to cecum bacteria yeast buy generic colchicina 0.5mg on-line, discover no distinction in strain generated after a 12 months (Hedlund et al treatment for dogs eating chocolate discount 0.5 mg colchicina with mastercard, 1984) antibiotic resistance legislation purchase 0.5 mg colchicina overnight delivery. The Mainz pouch, which uses both ileum and cecum, has a median stress at capacity of 39 cm H2O with a maximum stress of sixty three cm H2O (Thuroff Motor Activity It has been instructed that splitting the bowel on its antimesenteric border discoordinates motor activity and thereby causes a lesser intraluminal stress. Clearly, the ideal scenario is to present the patient with a spheric vessel that has few or ineffective contractions of its walls. This has also been demonstrated clinically: Initially after reconfiguration of the bowel (detubularization), coordinated activity fronts have been shown to decrease. During extended periods, however, lots of the peristaltic waves (activity fronts) reappear and may be readily demonstrated. The literature is contradictory with respect to the impact of detubularization on segments of ileum and colon used to assemble storage vessels for continent diversions. Pressure within the lumen of bowel that has both ends closed could additionally be increased by adding quantity or reducing the dimensions of the bowel through contractions of its wall. Because the bowel wall is freely permeable to water, the higher osmotic content of urine obligates motion of water into the bowel lumen. In evaluating whether motor exercise is the first determinant of intravesical strain, one should be cognizant of fluid volume changes. Pressure waves recorded 1 12 months postoperatively in a affected person with a continent diversion constructed from detubularized ileum and right colon. Notice that the coordinated stress waves are of magnitude and frequency much like these present in a traditional colonicorilealsegment. Thus, reconfiguring bowel usually will increase the volume, but its long-term effect on motor activity and wall rigidity is unclear presently. It has been my observation that some patients with orthotopic bladders after numerous years of spontaneous voiding require intermittent catheterization. In these sufferers the bowel section has turn out to be flaccid, and the flexibility of the patient to generate intraluminal stress by a Valsalva maneuver is restricted. Moreover, the process previous the urinary intestinal diversion additionally has a set of complications that have to be added to these described previously. It is evident that with current modalities of urinary intestinal diversion, long-term problems considerably contribute to mortality and morbidity. Those for whom a urinary intestinal diversion has been constructed for benign illness and those who are cured of cancer are most likely to experience long-term morbid complications. The knowledge of the frequency of these issues and the proper performance of preoperative preparation, surgical technique, and postoperative care, as outlined on this chapter, should provide one of the best probability for the least mortality and morbidity in patients present process urinary intestinal diversion. Prospective study of metabolic abnormalities in sufferers with continent Kock pouch urinary diversion. Bone mineral and related biochemical variables in patients with Kock ileal reservoir or Bricker conduit for urinary diversion. Complications after use of gastric segments for lower urinary tract reconstruction. Stapled versus hand-sewn anastomoses in emergency intestinal surgical procedure: results of a potential randomized examine. The stapled gastrointestinal tract anastomosis: incidence of postoperative complications compared with the sutured anastomoses. Whole-gut irrigation versus enema in elective colorectal surgical procedure: a prospective, randomized examine. Urinary carcinogen (nitrosamine) manufacturing in a rat animal model for ureterosigmoidostomy. Detubularized intestinal segments in urinary tract reconstruction: why do they work Percutaneous transrenal electroincision of ureterointestinal anastomotic strictures: long-term results and comparison of fluoroscopic and endoscopic steering. Modified autosuture method for ileal conduit building in urinary diversion. Effect of postcystectomy infectious complications on value, size of stay, and mortality. Ureteral anastomosis in the orthotopic ileal neobladder: comparability of two strategies. Analysis of radical cystectomy and urinary diversion complications with the Clavien classification system in an Italian actual life cohort. Pathogenesis of adenocarcinoma complicating ureterosigmoidostomy: experimental observations. Dysplasia of ureteric epithelium: a supply of adenocarcinoma in ureterosigmoidostomy Salvage cystectomy after radical irradiation for bladder most cancers: prognostic factors and complications. Gastrocystoplasty: another answer to the issue of urological reconstruction in the severely compromised patient. Ureteroenteric anastomotic strictures after radical cystectomy-does operative method matter Advantages and dangers of ileovesicostomy for the management of neuropathic bladder. A survey of clinical trials of antibiotic prophylaxis in colon surgery: proof towards additional use of no-treatment controls. Electrolyte disorders following oral sodium phosphate administration for bowel cleansing in aged sufferers. Volume capacity and stress characteristics of the continent ileal reservoir used for urinary diversion. Morbidity and mortality of octogenarians following open radical cystectomy using a standardized reporting system. Experience with coapted gastric tube outlet and composite gastrointestinal reservoir for continent cutaneous urinary diversion. Long-term followup of augmentation enterocystoplasty and continent diversion in patients with benign disease. The pathophysiology of the jejunal conduit syndrome and its exacerbation by parenteral hyperalimentation. Ammonia transport within the gut chronically uncovered to urine: is it decreased over time Radical cystectomy for bladder cancer: morbidity of laparoscopic versus open surgery. Clinical and metabolic observations on osteomalacia following ureterosigmoidostomy. The osteomalacia syndrome after colocystoplasty: a remedy with sodium bicarbonate alone. Percutaneous intrapelvic pressure registration in sufferers with ureterointestinal urinary diversion. Abnormal patterns of colorectal mucin secretion after urinary diversion of different sorts: histochemical and lectin binding research. Effect of Stanford pouch and ileal conduit urinary diversions on bone density and metabolism. Pathogenesis of nocturnal urinary incontinence after ileocaecal bladder alternative: continuous measurement of urethral closure strain throughout sleep. Conduit and renal pelvic stress after ileal and colonic urinary diversion in dogs. Evaluation of 80 instances of ileal conduits in kids: indications, complications and outcomes.
Buy 0.5 mg colchicina otcComparative effectiveness evaluate: prostate cancer antigen three testing for the prognosis and management of prostate most cancers virus 41 states order colchicina 0.5mg without prescription. Predicting high-grade cancer at tencore prostate biopsy utilizing 4 kallikrein markers measured in blood in the ProtecT study antimicrobial humidifiers trusted colchicina 0.5 mg. Effects of systematic 12-core biopsy on the efficiency of % free prostate specific antigen for prostate cancer detection bacteria animation buy colchicina 0.5 mg cheap. A multiplex mannequin of combining genebased antibiotic used for staph purchase 0.5 mg colchicina free shipping, protein-based, and metabolite-based with constructive and negative markers in urine for the early diagnosis of prostate most cancers. Predictive value of 4 kallikrein markers for pathologically insignificant in contrast with aggressive prostate cancer in radical prostatectomy specimens: outcomes from the European Randomized Study of Screening for Prostate Cancer section Rotterdam. Substratification of stage T1c prostate most cancers based on the likelihood of biochemical recurrence. The impact of finasteride on prostate-specific antigen in males with benign prostatic hyperplasia. Prostatic quantity and ratio of free-tototal prostate particular antigen in patients with prostatic cancer or benign prostatic hyperplasia. Predicting the result of prostate biopsy: comparison of a novel logistic regression-based mannequin, the prostate cancer risk calculator, and prostate-specific antigen level alone. Monoclonal antibodies to a brand new antigenic marker in epithelial prostatic cells and serum of prostatic cancer sufferers. Prostate-specific membrane antigen and different prostatic tumor markers on the horizon. Prediction of docetaxel response in human breast cancer by gene expression profiling. Human glandular kallikrein 2 expression in prostate adenocarcinoma and lymph node metastases. Gene expression signature in superior colorectal cancer patients choose drugs and response for the use of leucovorin, fluorouracil, and irinotecan. Genomic classifier identifies men with antagonistic pathology after radical prostatectomy who profit from adjuvant radiation remedy. Optimal predictors of prostate most cancers on repeat prostate biopsy: a prospective research of 1,051 males. Comparison of serum prostate specific membrane antigen, prostate specific antigen, and free prostate particular antigen ranges in radical prostatectomy sufferers. Prostatic specific antigen and prostatic acid phosphatase in the monitoring and staging of patients with prostatic cancer. Age-related modifications in tissue ranges of prostatic acid phosphatase and prostate specific antigen. Tissue metabolite profiling identifies differentiating and prognostic biomarkers for prostate carcinoma. Metabolomic profiling of lung and prostate tumor tissues by capillary electrophoresis time-of-flight mass spectrometry. A 17-gene assay to predict prostate cancer aggressiveness within the context of Gleason grade heterogeneity, tumor multifocality, and biopsy undersampling. Seven prostate most cancers susceptibility loci recognized by a multi-stage genome-wide association research. Expression of pro form of prostatespecific antigen by mammalian cells and its conversion to mature, lively kind by human kallikrein 2. Quantitation of prostatespecific antigen in serum by a sensitive enzyme immunoassay. Elimination of serum free and total prostatespecific antigen after radical retropubic prostatectomy. Double-label time-resolved immunofluorometric assay of prostate-specific antigen and of its advanced with alpha 1-antichymotrypsin. A kallikrein-like serine protease in prostatic fluid cleaves the predominant seminal vesicle protein. Prostate-specific antigen in serum happens predominantly in advanced with alpha 1-antichymotrypsin. Synthetic protease inhibitors and post-ejaculatory degradation of human semen proteins. Activation of the zymogen form of prostate-specific antigen by human glandular kallikrein 2. Production and activation of recombinant hK2 with propeptide mutations leading to excessive expression ranges. Decreased concentrations of prostate-specific antigen and human glandular kallikrein 2 in malignant versus nonmalignant prostatic tissue. Pro-prostate-specific antigen measurements in serum and tissue are associated with treatment necessity among males enrolled in expectant management for prostate most cancers. Human seminal vesicle-specific antigen is a substrate for prostate-specific antigen (or P-30). Long distance bicycle driving causes prostatespecific antigen to increase in males aged 50 years and over. Influence of finasteride on free and total serum prostate particular antigen levels in men with benign prostatic hyperplasia. Complexed prostate specific antigen improves specificity for prostate most cancers detection: outcomes of a potential multicenter scientific trial. Intact and internally cleaved free prostate-specific antigen in sufferers with prostate cancer with totally different pathologic stages and grades. Prostate-specific membrane antigen expression as a predictor of prostate cancer development. Radical prostatectomy as therapy for prostate-specific antigen-detected stage T1c prostate cancer. Effect of ejaculation on serum prostate specific antigen degree in screening and non-screening inhabitants. Longitudinal adjustments of benign prostate-specific antigen and [-2]proprostate-specific antigen in seven years in a community-based pattern of males. Vascular targeted remedy with anti-prostate-specific membrane antigen monoclonal antibody J591 in advanced stable tumors. Use of % free prostate-specific antigen as a predictor of the pathological options of clinically localized prostate most cancers. Clinical behavior of prostatic specific antigen and prostatic acid phosphatase: a comparative examine. Serum human glandular kallikrein-2 protease ranges predict the presence of prostate most cancers among males with elevated prostate-specific antigen. Single nucleotide polymorphism of the human kallikrein-2 gene highly correlates with serum human kallikrein-2 levels and in combination enhances prostate most cancers detection.

Cheap colchicina 0.5 mg without prescriptionOthers have found these maneuvers antibiotic skin infection cheap colchicina 0.5mg visa, particularly supracrural rerouting antibiotics for dogs urinary infection cheap colchicina 0.5 mg visa, to be pointless and/or unhelpful (Morey and McAninch virus 2014 season cheap colchicina 0.5mg on-line, 1997; Rosenstein and Jordan antibiotics lyme disease buy colchicina 0.5mg fast delivery, 2003; Cooperberg et al, 2007; Kizer et al, 2007). Total elimination of the symphysis pubis, first reported by Pierce in 1962 (Pierce, 1962), has been beneficial when severe accidents lead to complicating options corresponding to fistula or marked displacement or retropubic fixation of the prostate (Netto, 1985; McAninch, 1989; Asci et al, 1999). Alternatively, a combined abdominoperineal approach (with or without partial pubectomy) has proved useful in circumstances of extreme fibrosis, fistula, previous failed anastomotic urethroplasty, and related bladder neck damage and in pediatric instances (Waterhouse, 1976; Al-Rifaei et al, 1991; Koraitim, 2003, 2005; Pratap et al, 2006). It is important to limit the lithotomy time to 5 hours or less to prevent lower extremity complications (Anema et al, 2000) when any complicated urethral reconstruction is undertaken. These studies help the conclusion that these problems are often the end result of the damage itself and not of the therapy (Follis et al, 1992; Elliott and Barrett, 1997; Porter et al, 1997; Corriere, 2001). Some sufferers who turn out to be impotent after injury spontaneously get well erectile operate 1 or 2 years later (Turner-Warwick, 1989; Morey and McAninch, 1997; Koraitim, 2005). Many sufferers who turn out to be impotent as a end result of pelvic fracture have a point of arterial insufficiency (Armenakas et al, 1993; Matthews et al, 1995). Because patients with impotence may be extra weak to restenosis after posterior urethroplasty because of bulbar urethral ischemia, some consultants have advised that "at-risk" patients undergo preoperative penile arterial duplex Doppler studies to establish candidates appropriate for initial penile revascularization (Matthews et al, 1995; Rosenstein and Jordan, 2003). However, indications for penile revascularization as a treatment for post-traumatic erectile dysfunction are extremely restricted (Kawanishi et al, 2004). Overall charges of incontinence, anejaculation, and areflexic bladder are low (2% to 4%) (Corriere et al, 1994; Elliott and Barrett, 1997; Asci et al, 1999; Anger et al, 2008), and these conditions are likely to be secondary to the original harm. After posterior urethroplasty, 5% to 15% of sufferers have recurrent stenosis at the anastomosis (Mundy, 1996; Flynn et al, 2003; Koraitim 2005; Cooperberg et al, 2007). Urinary continence after urethral distraction is the rule quite than the exception, regardless of destruction of the exterior sphincter from either the injury itself or the next repair. The mechanism of continence is assumed to be largely attributable to bladder neck perform (Iselin and Webster, 1999). Urodynamic knowledge present that a significant proportion of sufferers also have identifiable distal rhabdosphincteric perform (Whitson et al, 2008). AnteriorUrethralInjuries In distinction to posterior urethral distraction, anterior injuries are most often isolated (Kiracofe et al, 1975). Most occur after straddle injury and contain the bulbar urethra, which is prone to compressive harm due to its mounted location beneath the pubis. A smaller share of injuries to the anterior urethra are the end result of direct penetrating damage to the penis. As with posterior urethral harm, a high index of suspicion have to be maintained in all patients with blunt or penetrating trauma within the urogenital region, and urethrography ought to be carried out in any case of suspected urethral harm (Husmann et al, 1993). Clinical indicators of anterior urethral injuries include blood on the meatus, perineal hematoma, gross hematuria, and urinary retention. In extreme trauma, Buck fascia could additionally be disrupted, leading to blood and urinary extravasation into the scrotum. The main morbidity of straddle damage is urethral stricture, which can turn into symptomatic years later (Park and McAninch, 2004). Some degree of impotence is famous in 82% of sufferers with pelvic fracture and urethral distraction damage (Flynn et al, 2003), although the common reported price is roughly 50% (Corriere et al, 1994; Routt et al, 1996; Elliott and Barrett, 1997; Asci et al, 1999; Koraitim, 2005). The etiology is multifactorial and variably attributed to cavernous nerve damage, arterial insufficiency, venous leak, and direct corporeal harm (Narumi et al, 1993; Munarriz et al, 1995; Shenfeld et al, 2003). Factors that correspond to the severity of the damage, such as diastasis of the pubic symphysis, lateral displacement of the urethra, and lengthy urethral gap, have been discovered to correlate with erectile dysfunction (Koraitim, 2013). Some surgical sequence have proven a small variety of sufferers with new-onset or worsened erectile dysfunction after reconstruction (Tunc et al, 2000); nonetheless, the issues of the original pelvic injury are troublesome to differentiate from the issues of attempts to restore urethral and bladder accidents. Accounts of greater danger of erectile dysfunction and incontinence with main realignment have been published before the advent of flexible endoscopes (Koraitim et al, 1996). Contusions and incomplete accidents could be treated with urethral catheter diversion alone. Initial suprapubic cystostomy is the usual of look after main straddle injuries involving the urethra (Park and McAninch, 2004); nevertheless, primary anterior urethral realignment has shown promising outcomes with respect to stricture price and erectile dysfunction in patients with straddle accidents of lesser magnitude (Ying-Hao et al, 2000; Yu et al, 2007). Intraoperative view of normal membranous urethra after fibrotic tissue was excised throughout perineal bulbomembranous urethroplasty. Debridement of the corpus spongiosum after trauma must be restricted as a outcome of corporeal blood provide is normally strong, enabling spontaneous therapeutic of most contused areas (Kiracofe et al, 1975; Husmann et al, 1993). Initial suprapubic urinary diversion is recommended after high-velocity gunshot wounds to the urethra, adopted by delayed reconstruction. Delayed Reconstruction Before any deliberate process, a retrograde urethrogram and voiding cystourethrogram must be obtained to define the positioning and size of the obliterated urethra clearly. Urethral ultrasound examination might assist delineate the size and severity of stricture. Dense fibrous tissue from trauma often demonstrates a fixed, nondistensible look sonographically with vital shadowing (Morey and McAninch, 2000). Anastomotic urethroplasty is the procedure of selection within the totally obliterated bulbar urethra after a straddle harm. The proximal and distal urethra may be mobilized for a tension-free, end-to-end anastomosis. This is a highly successful procedure in more than 95% of circumstances (Santucci et al, 2002; Jordan et al, 2010). Endoscopic incision via the scar tissue of an obliterated urethra is a hopeless procedure doomed to failure. Partial urethral narrowing can initially be handled by endoscopic incision or dilation with larger success. Repeated endoscopic manipulation is neither clinically efficient nor cost-effective for the remedy of urethral strictures (Greenwell et al, 2004). Patients who undergo repeated endoscopic procedures are also more more likely to require complicated reconstructive procedures corresponding to grafts (Park and McAninch, 2004; Hudak et al, 2012). Open restore must be delayed for a quantity of weeks after instrumentation to permit the urethra to stabilize, and a 2-month period of suprapubic urinary diversion may be prudent preoperatively to optimize situations for restore of complex or recurrent strictures which were catheter dependent (Terlecki et al, 2011). Finally, UroLume stents are contraindicated in the setting of traumatic urethral strictures (Wilson et al, 2002). Use of ultrasonography for the diagnosis of testicular injuries in blunt scrotal trauma. Unintended negative penalties of major endoscopic realignment for men with pelvic fracture urethral injuries. Does timing of presentation of penile fracture affect end result of surgical intervention The value of magnetic resonance imaging within the analysis of suspected penile fracture with atypical scientific findings. Gunshot wound injury of the testis: the use of tunica vaginalis and polytetrafluoroethylene grafts for reconstruction. Accuracy of ultrasonography in analysis of testicular rupture after blunt scrotal trauma. Anatomy and energy of the tunica albuginea: its relevance to penile prosthesis extrusion. Penile fracture: preoperative analysis and surgical method for optimum patient consequence. Penile zipper entrapment: a simple and less threatening strategy utilizing mineral oil. The efficacy of magnetic resonance imaging for the analysis of testicular rupture: a potential preliminary research.
Buy colchicina 0.5mg onlineImpact of medical remedy on transurethral resection of the prostate: twenty years of change antibiotic resistance nice discount 0.5mg colchicina mastercard. Transurethral incision versus resection of the prostate for small to medium benign prostatic hyperplasia antibiotics osteomyelitis generic 0.5mg colchicina with mastercard. Effect of transurethral resection of the prostate on erectile function: a prospective comparative examine antibiotics for tooth infection cheap colchicina 0.5 mg otc. Insight into mechanism of neodymium: yttrium-aluminum-garnet laser prostatectomy using the high-power contact-free beam method antibiotic rash discount 0.5 mg colchicina with mastercard. Laser vaporization of bovine prostate: a quantitative comparison of potassium-titanyl-phosphate and lithium triborate lasers. Transurethral electrovaporization of the prostate: a novel technique for treating men with benign prostatic hyperplasia. Comparison of transurethral vaporization utilizing PlasmaKinetic power and transurethral resection of prostate: 1-year follow-up. Maintenance of erectile perform after photoselective vaporization of the prostate for obstructive benign prostatic hyperplasia. The long-term outcomes of transurethral vaporization of the prostate using plasmakinetic vitality. Removal of UroLume endoprosthesis: expertise of the North American Study Group for detrusorsphincter dyssynergia utility. Long-term outcomes of a randomized trial comparing holmium laser enucleation of the prostate and transurethral resection of the prostate: outcomes at 7 years. The development of benign prostatic hyperplasia among volunteers within the Normative Aging Study. Ethanol injection therapy of the prostate for benign prostatic hyperplasia: preliminary report on utility of a new technique. Application of external microwave thermotherapy in urology: previous, current, and future. A modified prostatic UroLume Wallstent for wholesome patients with symptomatic benign prostatic hyperplasia: a European Multicenter Study. Cumulative prevalence of prostatism matches the autopsy prevalence of benign prostatic hyperplasia. Photoselective vaporization of prostate: five-year outcomes of whole clinic affected person population. Transurethral microwave thermotherapy for benign prostatic hyperplasia: medical outcome after 4 years. Suprapubic catheter following transurethral resection of the prostate: a method to decrease the number of urethral strictures and improve the end result of operations. Cell death induced in a murine mastocytoma by 42-47 levels C heating in vitro: evidence that the form of death changes from apoptosis to necrosis above a important warmth load. Dilutional hyponatremic shock: one other concept of the transurethral prostatic resection reaction. The importance of the strain in the prostatic fossa and absorption of irrigating fluid during transurethral resection of the prostate. National developments in surgical therapy for benign prostatic hyperplasia in the United States (2000-2008). Photoselective vaporization prostatectomy: experience with a novel 180 W 532 nm lithium triborate laser and fiber supply system in residing canines. Results from a world multicentre double-blind randomized controlled trial on the perioperative efficacy and safety of bipolar vs. Bipolar versus monopolar transurethral resection of the prostate: a systematic review and metaanalysis of randomized controlled trials. A randomized doubleblind placebo-controlled phase 2 dose-ranging research of onabotulinumtoxinA in males with benign prostatic hyperplasia. Relief by botulinum toxin of voiding dysfunction due to benign prostatic hyperplasia: outcomes of a randomized, placebo-controlled study. The 12-year consequence evaluation of an endourethral wallstent for treating benign prostatic hyperplasia. The 12-year symptomatic consequence of transurethral resection of the prostate for patients with lower urinary tract signs suggestive of benign prostatic obstruction compared to the urodynamic findings before surgical procedure. Predictability of irritative voiding signs following photoselective laser vaporization of the prostate. Alfuzosin 10 mg once every day in the management of acute urinary retention: results of a double-blind placebo-controlled research. A multicenter, randomized, double-blind, placebo controlled examine of onabotulinumtoxinA 200 u to treat decrease urinary tract signs in males with benign prostatic hyperplasia. Transurethral resection of the prostate and transurethral incision of the prostate. The prostatron transurethral microwave system within the therapy of bladder outflow obstruction because of benign prostatic hyperplasia. Defining optimum laser-fiber sweeping angle for efficient tissue vaporization using one hundred eighty W 532 nm lithium triborate laser. Urolume stent placement for the treatment of postbrachytherapy bladder outlet obstruction. Experience with greater than 1,000 holmium laser prostate enucleations for benign prostatic hyperplasia. Transurethral holmium laser enucleation of the prostate versus transurethral electrocautery resection of the prostate: a randomized prospective trial in 200 patients. Does perioperative outcome of transurethral holmium laser enucleation of the prostate depend upon prostate size Holmium laser enucleation of the prostate versus open prostatectomy for prostates larger than a hundred grams: 5-year follow-up outcomes of a randomised clinical trial. Potassium-titanyl-phosphate laser vaporization of the prostate: a comparative practical and pathologic examine in canines. Therapeutic results of add-on botulinum toxin A on patients with giant benign prostatic hyperplasia and unsatisfactory response to combined medical therapy. Randomized research of transurethral resection of the prostate and mixed transurethral resection and vaporization of the prostate as a therapeutic alternative in men with benign prostatic hyperplasia. Day-case holmium laser enucleation of the prostate for gland volumes of <60 mL: early experience. Temperature-correlated histopathologic changes following microwave thermoablation of obstructive tissue in patients with benign prostatic hyperplasia. The efficacy of transurethral resection of the prostate in males with reasonable signs of prostatism. Minimally invasive treatments for benign prostatic enlargement: systematic evaluate of randomised managed trials. The clinical effectiveness of transurethral incision of the prostate: a scientific evaluate of randomised managed trials. Contemporary apply patterns of endoscopic surgical management for benign prostatic hyperplasia amongst urologists within the United States. PlasmaKinetic SuperPulse transurethral resection versus typical transurethral resection of prostate. Thermo-expandable intraprostatic stents in bladder outlet obstruction: an 8-year research. Vaporization of prostates of > or =80 mL using a potassium-titanyl-phosphate laser: midterm-results and comparability with prostates of <80 mL.
Order colchicina 0.5 mg overnight deliveryIn contrast 775 bacteria that triple every hour 0.5 mg colchicina with mastercard, only thirteen of 106 sufferers (12%) with an intussuscepted ileal nipple developed problems with their stoma bacteria pseudomonas aeruginosa colchicina 0.5mg low cost. The continence mechanism is created by placing the tube into the adjoining taenial trough antibiotic resistance ethics order 0.5 mg colchicina with amex. A mucosal window is opened on the base of the U antibiotics classes buy colchicina 0.5mg with mastercard, and the tube sutured to the mucosa with interrupted sutures. Another novel Mitrofanoff continence mechanism was described by Montie (1997), who conceived of a procedure in which a 2- to 3-cm phase of terminal ileum is isolated on its blood provide. The width of the phase was chosen to correspond to the circumference of the tube to be created. Once isolated, the segment is opened near one of its mesenteric junctions to create a longitudinal reconfiguration. When longer tubes are essential, two adjoining segments may be isolated, reconfigured, and joined collectively. Although the method was originally described in dogs, Montie (1997) has used it in humans without complication. Montie (1997) reported on a excessive price of stomal stenosis in dogs, but this may have been secondary to infrequent catheterizations. Other teams have used tapered ileum to create a tunneled access into the best colon. Using tapered ileum for this objective has the benefit of a blood provide impartial of the reservoir and no length restrictions while having the disadvantage of additional limiting intestinal absorptive surface. Wiesner and colleagues (2007) lately in contrast their longterm ends in 458 sufferers who underwent Mainz I pouch development. The anastomosis was made utilizing a submucosal tunnel in 809 renal-ureteric items, and using a serosa-lined extramural tunnel in seventy four models. At 17 months postoperatively they found a significantly higher incidence of anastomotic obstruction in the submucosal tunnel group compared with the extramural group (7. It is important to notice that they found a much higher rate of obstruction in patients with previously dilated higher tracts (14%) or with a history of neurogenic bladder (17%). In another comparison of sufferers with a Mainz I pouch, Wiesner and colleagues (2006) reported on 800 patients with almost eight years of follow-up. Newtechniques for building of efferent conduits based mostly on the Mitrofanoff precept. Ischemic degeneration of the continence mechanism occurred virtually three times more often in the appendiceal group. Right Colon Pouches with Intussuscepted Terminal Ileum Additional pouches utilizing nipple valve technology for the continence mechanism embrace those proper colon pouches by which intussusception of the terminal ileum and ileal cecal valve is employed. These are variations on the continent cecal reservoir initially described by Mansson (1987) that make use of an intact cecal phase. These surgical procedures differ from each other by only some features, mainly related to the technique employed for stabilizing the nipple valve. Unless the appendix is being used as a continence mechanism, appendectomy must be performed in all cases as a result of an in situ appendix would function a nidus for an infection and abscess formation. The reader is referred to the prior edition of this textual content for an in-depth description of these operations. This operation, which involved the partial spatulation of the cecal section and attachment of an ileal patch, represented main contributions to the unique ileocecal reservoir as described by Gilchrist and associates (1950), by which the intact bowel reservoir was employed and no try was made to strengthen the ileocecal valve. Originally, strengthening the ileocecal valve consisted of creating a double row of imbricating sutures to the complete ileal section (Rowland et al, 1985, 1987). It soon grew to become obvious that this was necessary solely in the area of the ileocecal valve. The remaining "neourethra" might be tapered and introduced through an abdominal or perineal stoma. At Indiana University as nicely as other establishments it grew to become clear that the idea of marsupializing solely a portion of the ascending colon phase left sufficient peristaltic integrity in the cecal region to generate pressures sufficiently excessive to overcome the continence mechanism in some patients. A number of groups contributed to the idea of using the entire proper colon or more, marsupializing the complete structure and refashioning it in a Heineke-Mikulicz configuration (Lockhart, 1987; Bejany and Politano, 1988; Benson et al, 1988; Rowland, private communication, 1989). These variations have been entitled the Florida pouch (Lockhart, 1987) and the University of Miami pouch (Bejany and Politano, 1988). However, they characterize comparatively minor variations on the theme of the Indiana pouch. The Indiana pouch in its present type entails isolating a segment of terminal ileum roughly 10 cm in size together with the entire right colon to the junction of the right and center colic artery blood provides. After bowel continuity is reestablished, appendectomy is performed and the appendiceal fat pad obscuring the inferior margin of the ileocecal junction is removed by cautery. The complete right colon is opened along its antimesenteric border, and ureteral-taenial implants are customary. With nonabsorbable sutures, interrupted Lembert sutures are taken over a distance of 3 to four cm in two rows for the double imbrication of the ileocecal valve as described at Indiana University. The second row of sutures should try to deliver the other mesenteric edges of ileum collectively, often over a 12- to 14-Fr catheter. These two rows of sutures should be placed roughly eight mm from one another, and the preliminary suture in each row may be taken in a purse-string fashion across the cecal margin as properly. Alternatively, the University of Miami group suggests placing purse-string sutures in the identical ileal area (Bejany and Politano, 1988). Finally, the Tampa group suggests placement of apposing Lembert sutures on both sides of the terminal ileum. The remaining ileum may be tapered over the catheter and excess ileum removed with a stapling technique. It is important to carry out the imbrication while the cecal reservoir is still open (Rowland, 1996) in order that the gradual closure of the ileocecal valve could be carefully observed. The pouch is then closed in a Heineke-Mikulicz configuration with a operating absorbable suture. Ureteral stents and a suprapubic tube are taken by way of a stab wound within the pouch and led via the proper decrease stomach quadrant. The pouch is rotated in order to convey the ileal neourethra as close as potential to the chosen stoma web site. A fingerbreadth-wide skin button is transected along with an analogous button from the anterior and posterior fascia. The ileal neourethra is advanced between bundles of the rectus muscle through the stoma and excess ileum is transected. The ileal edges are sewn to skin with interrupted sutures so as to create a flush stoma. In addition to the differences within the strategy of ileocecal valve imbrication, both the University of Miami and the Florida pouches differ within the amount of colon used. The complete ascending colon and the proper third or half of the transverse colon is isolated together with 10 to 12 cm of ileum.
Colchicina: 0.5 mg
Cheap colchicina 0.5mg onlineThe cause for this finding is that bilateral prostate most cancers may symbolize (1) a dominant tumor nodule with contralateral small antibiotics for uti flucloxacillin order colchicina 0.5 mg free shipping, low-grade virus nucleus discount 0.5 mg colchicina with mastercard, clinically insignificant tumor; (2) significant discrete right and left tumor nodules; or (3) a single antibiotic resistance quiz buy generic colchicina 0.5mg online, large antimicrobial agents examples colchicina 0.5mg without prescription, confluent tumor mass involving either side. This writer merely denotes "stage T2" with out subclassification into "T2a" or "T2b" or "T2c" (Kheirandish and Chinegwundoh, 2011; van der Kwast et al, 2011). Pathologic stage T3 represents a tumor that has prolonged out of the prostate gland, which is additional subclassified into T3a and T3b, relying on whether or not the extraprostatic tumor is without or with seminal vesicle invasion, respectively. The location and grade of the tumor additionally modulate the impact of tumor quantity (Christensen et al, 1990; McNeal et al, 1990; Greene et al, 1991). For instance, transition zone tumors prolong out of the prostate at bigger volumes than do peripheral zone tumors because of their decrease grade and greater distance from the sting of the gland. Location In medical stage T2 carcinomas and in 85% of nonpalpable tumors identified on needle biopsy (stage T1c), the main tumor mass is situated within the posterior portion of the prostate in the peripheral zone (McNeal, 1969; Byar and Mostofi, 1972; Epstein Grade the Gleason system is predicated on the glandular sample of the tumor as recognized at relatively low magnification (Mellinger et al, 1967; Gleason and Mellinger, 1974). Architectural patterns are recognized and assigned a grade from 1 to 5, with 1 being the most differentiated and 5 being undifferentiated (see Box 110-1). Although within the original Gleason system, the commonest and second commonest grades have been combined, in 2005 the Gleason system was up to date and modified with one change being that on biopsy the most typical and highest-grade patterns on a given core have been added to outcome in the Gleason rating (Epstein et al, 2005). If a tumor has just one histologic sample, then for uniformity, each patterns are assigned the identical grade. In theory, nevertheless, the Gleason scores vary from 2 (1 + 1 = 2), which represents tumors uniformly composed of Gleason pattern 1 tumor, to 10 (5 + 5 = 10), which represents completely undifferentiated tumors. It is affordable to assign a full Gleason score even to small foci of cancer on needle biopsy as a outcome of it has been demonstrated that the grade assigned to these minimal cancers is just as correct in comparability with instances with more intensive most cancers on biopsy (Steinberg et al, 1997). Oversimplification of the Gleason grade classification, such as combining Gleason scores 8 to 10 or classifying sufferers into low-, intermediate-, and high-risk classes primarily based on Gleason scores less than 7, 7, and higher than 7, loses important prognostic information. A more modern grouping of Gleason scores based mostly on differing prognoses is as follows: Gleason scores 6; 3 + 4 = 7; 4 + three = 7; 8; 9 to 10, which reflect Grade Groups I to V (Pierorazio et al, 2013b). At the top of every biopsy report that shows carcinoma, we add the next: the overall Gleason score for this case is predicated on the core with the highest Gleason score. Gleason scores may be grouped and vary from Grade Group I (most favorable) to Grade Group V (least favorable). Consequently, an issue with the current system is that Gleason score 6 is usually the bottom grade assigned on biopsy materials. For instance, just about no organ-confined Gleason score 6 tumor is related to progression after radical prostatectomy, whereas this occasionally occurred using the unique Gleason system (Hernandez et al, 2008). Multiple cores of Gleason rating 6 nonetheless correlate with favorable findings at radical prostatectomy (Ellis et al, 2013). Using the modified Gleason system, in a study from Johns Hopkins of 6462 males, almost 95% and 97% of sufferers with Gleason rating 6 cancer at biopsy and radical prostatectomy (no tertiary sample 4 at radical prostatectomy), respectively, have been predicted to be cured of illness at 5 years following radical prostatectomy (Pierorazio et al, 2013a). Using the modified Gleason system, this research showed that Gleason rating three + four = 7 tumor has a very favorable prognosis with an estimated 5-year biochemical-free survival of 83% and 88% for biopsy and radical prostatectomy, respectively. Gleason scores 9 to 10 tumor had the Gleason grade on biopsy material has additionally been proven to correlate fairly well with that of the subsequent prostatectomy specimen (Fine and Epstein, 2008). In basic, a Gleason rating less than or equal to 6 on biopsy corresponds to a Gleason score less than or equal to 6 within the radical prostatectomy in about 65% of instances. An unavoidable cause of discrepant grading between the biopsy and subsequent prostatectomy specimen is that attributable to sampling error by the needle biopsy. Although, in general, larger tumors are excessive grade and small tumors are low grade, exceptions occur (Epstein et al, 1994a). There is an inclination to hypothesize that tumors start as low-grade tumors and, on reaching a sure dimension, dedifferentiate into higher-grade lesions, accounting for the connection between measurement and grade. Alternatively, high-grade tumors could additionally be high grade at their inception but are detected at an advanced measurement because of their rapid progress. Similarly, low-grade tumors may evolve so slowly that they have a tendency to be detected at decrease volumes. As long as cores are submitted in separate containers or the cores are in the same container yet specified by the urologist as to their location. If cores are mixed in a container without designation, some pathologists still attempt to assign separate scores for every core and others simply provide an total Gleason score as if all the cores have been one lengthy core. Differential Diagnosis the underdiagnosis of restricted adenocarcinoma of the prostate on needle biopsy is likely certainly one of the most frequent issues in prostate pathology (Epstein, 2004). There are also quite a few benign mimickers of adenocarcinoma of the prostate (Srigley, 2004). Benign glands include basal cells and are labeled with these antibodies, whereas prostate most cancers exhibits no staining. In certain circumstances, there are findings suggestive of, however not diagnostic of, carcinoma. The incidence of atypical needle biopsy specimens is about 5% (Epstein and Herawi, 2006). Pathologists ought to sign out atypical circumstances descriptively as "a focus of atypical glands" quite than using ambiguous terminology such as "atypical hyperplasia" or "atypical small acinar proliferation. The likelihood of most cancers after an atypical diagnosis is about 40% to 50% (Iczkowski et al, 1997; Chan and Epstein, 1999; Epstein and Herawi, 2006). Cases diagnosed as atypical have the best probability of being changed on skilled review, and urologists ought to consider sending such circumstances for consultation to try and resolve the prognosis as both definitively benign or malignant before subjecting the affected person to repeat biopsy (Chan and Epstein, 2005). The ways during which most cancers may be measured on needle biopsy include number of positive cores, whole millimeters of most cancers amongst all cores, percentage of most cancers per core, and whole proportion of cancer in the whole specimen. An equal variety of studies claim superiority of one technique over the other, with no one method adopted uniformly (Epstein, 2011). It is proposed that pathologists report the variety of positive cores together with one other measurement of tumor extent. Perineural invasion on biopsy is prognostic in males undergoing external-beam radiotherapy, however is much less so with brachytherapy (Harnden et al, 2007). There are knowledge that atrophy and associated inflammation are linked with prostate carcinogenesis (DeMarzo et al, 2003). By processing 8 to 10 cassettes, more than 90% of stage T1a lesions are recognized (Newman et al, 1982; Murphy et al, 1986; Vollmer, 1986; Rohr, 1987). Differential Diagnosis One of the most common lesions to be confused with low-grade adenocarcinoma is adenosis (atypical adenomatous hyperplasia) (Gaudin and Epstein, 1994, 1995). Seminal vesicle invasion is a a lot more dire prognostic discovering, with a 65% 5-year development fee after surgery (Epstein, 2001; Pierorazio et al, 2011). Novara and Ficarra (2013) reported the mean rate of constructive margins within the robotic-assisted radical prostatectomy collection, revealed between 2008 and 2011 (each including >100 cases), to be 15%, which ranged from 6. Only approximately 50% of males with constructive margins progress after radical prostatectomy (Epstein et al, 1993). A few studies have documented the performance of frozen part alongside the size of the prostate within the region of the neurovascular bundle with a positive intraoperative margin resulting in resection of the ipsilateral neurovascular bundle (Schlomm et al, 2012; von Bodman et al, 2013). The technique features a low false-negative and false-positive rate in comparability with the everlasting sections of the same slides. However, in two studies by which a frozen-section margin was positive in the region of the neurovascular bundle and the bundle was removed, solely 23% to 25% of the bundles showed residual most cancers. Arguments posited in help of this procedure are (1) without the frozen sections most of those patients would have had the bundles resected due to preoperative high-risk characteristics; and (2) the overall sum of saved neurovascular bundles was markedly higher than the unnecessary secondary extensive excisions (Schlomm et al, 2012; von Bodman et al, 2013).
Quality 0.5 mg colchicinaHowever antibiotics pharmacology purchase colchicina 0.5mg amex, results from massive prospective studies confirmed no association between dietary fat intake and prostate cancer risk (Park et al medicine for lower uti order 0.5 mg colchicina fast delivery, 2007; Wallstrom et al antibiotic resistance mutation purchase colchicina 0.5mg without a prescription, 2007; Crowe et al antibiotic use in agriculture buy discount colchicina 0.5mg line, 2008). Observations on the affiliation of dietary fat and danger could have different explanations. Diets excessive in meat that are sources of fats are also normally low in vegetables, which comprise vitamins that will shield towards prostate cancer. Furthermore, meats and dairy products include different constituents, such as zinc and calcium, that will affect prostate cancer risk. The dietary complexity of the standard Western food regimen, the affiliation of more healthy dietary habits with healthier lifestyle selections (physical activity and smoking avoidance), and the potential interplay of particular nutrients with genetic variability among people are vital limitations to understanding how food regimen influences threat. Masko and colleagues (2013) have summarized the state of preclinical and clinical proof that particular dietary elements may exert an affect on prostate most cancers risk and development. Recent revelations concerning the position of intratumoral androgen in driving castrate-resistant prostate most cancers have increased give attention to ldl cholesterol as a danger factor (Sharifi, 2013). Coupled with epidemiologic proof that lower levels of serum ldl cholesterol and use of cholesterol-lowering agents (statins) scale back the chance of aggressive and advanced-stage illness, loss of cholesterol homeostasis could additionally be a contributor to prostate most cancers threat and development (Platz et al, 2006, 2009). Diet Descriptive epidemiologic research of migrants, geographic variations, and temporal studies recommend that dietary elements may contribute to prostate most cancers development (Bostwick et al, 2004). The incidence of latent prostate cancers is comparable around the globe, but the incidence of clinically manifest cancers differs, with Asians having the lowest rates of clinical illness (Center et al, 2012). Thus probably the most convincing evidence for the position of diet and other environmental elements in modulating prostate most cancers threat comes from migration research showing an elevated incidence of prostate most cancers in first-generation immigrants to the United States from Japan and China (Muir et al, 1991; Shimizu et al, 1991). These observations counsel that food regimen may play a task in tumor development, allowing latent cancers to turn into clinically evident. A sturdy positive correlation exists between prostate cancer incidence and the corresponding rates of a quantity of different diet-related cancers, including breast and colon (Bostwick et al, 2004). White fats in mammals serves not solely as an essential power reservoir, but additionally as an endocrine organ, with secretion of cytokines and brokers with cytokine-like activity (tumor necrosis factor-; interleukin-1, -6, -8, and -10; and reworking development factor-) in addition to their soluble receptors (Trayhurn and Wood, 2004). Treatment of weight problems via discount in fats consumption and increased exercise has been shown to scale back oxidative stress, suggesting that life-style modification could presumably be necessary in decreasing the risk of prostate cancer (Roberts et al, 2002). These observations likely replicate higher grade and more regionally advanced disease at presentation, technical challenges in surgical procedure and radiotherapy in overweight males, and extra aggressive biology pushed by adipocyte-derived biologic elements. Latent prostate most cancers is believed to have an analogous prevalence worldwide and amongst all ethnicities, whereas the incidence of scientific prostate cancer varies dramatically between and inside different international locations. For this reason, an understanding of prostate cancer etiology must encompass the steps leading to each the initiation of histologic cancer and progression to clinically evident illness. Mutations, downregulation by promoter methylation and other mechanisms, and protein modification have all been implicated in progression of prostate cancer. Alcohol Consumption Alcohol consumption and threat of prostate cancer is of interest due to the affiliation of alcohol with other cancers, its effect on estrogen and T, and the excessive content of polyphenolic compounds with antioxidant exercise in purple wine (Sutcliffe et al, 2007b). Epidemiologic research, together with each case-control and cohort designs, have reported combined outcomes, with some suggesting elevated risk, some null, and a few suggesting a protecting effect of alcohol use (reviewed in McGregor et al, 2013). Type 1 5-reductase is expressed primarily in the skin and liver and to lesser extent in prostate, whereas the type 2 enzyme is expressed predominantly in prostate epithelium and other genital tissues (Andriole et al, 2004a, 2004b). Males with inherited 5-reductase deficiency have minuscule prostatic tissue, and biopsies demonstrate stroma but no epithelium (Imperato-McGinley and Zhu, 2002). In addition to the shortage of enzyme activity, a lack of T can also shield in opposition to the event of prostate cancer, as evidenced by the atrophic prostates seen in men after surgical castration (Wilson and Roehrborn, 1999). For men with regular baseline T (10 nmol/L), higher T ranges at baseline had been unrelated to prostate cancer danger. This model is supported by animal studies displaying that intraprostatic androgen ranges and prostate mass in castrated rats are extremely sensitive to serum T around near-castrate levels, however plateau above this level (Wright et al, 1999) and related findings in intact rats exhibiting that standard prostate development plateaus with increasing doses of exogenous T (Banerjee et al, 1994), as nicely as by numerous scientific observations in humans (reviewed by Morgentaler and Traish, 2009). In concept, stem cells have the ability to self-renew and produce differentiated progeny that populate practical prostatic cells in both the stromal and epithelial compartments. The epithelial cell layer of the prostate, from which cancers come up, accommodates 4 distinct cell types: basal, secretory luminal, neuroendocrine, and transit-amplifying cells which have distinct morphology and molecular phenotypes (Prajapati et al, 2013). Transit-amplifying cells specific each basal and luminal cell markers, and likely represent an intermediate cell sort between these two. Recent studies counsel that prostate stem cells comprise about 1% of the basal cell population, based on particular marker expression and growth characteristics (Collins et al, 2001). Various genetic occasions in these cells can lead to tumor formation from any of these cell types (Maitland and Collins, 2008). The biologic processes that permit stem cells to turn out to be cancers could also be different than for luminal cells: the former must stay in a protecting niche that enables for technology of amplifying cells even with out speedy cell progress; the latter could solely require changes that lead to lack of progress control. Unlike in many metabolic ailments, level and missense mutations leading to altered proteins are rare in prostate cancer, estimated to occur in solely about 1% of primary tumors (Taylor et al, 2010). This part highlights probably the most well-characterized genomic events in early-stage prostate most cancers; for a complete overview the reader is referred to numerous glorious main sources (Taylor et al, 2010; JerÔøΩnimo et al, 2011; Prensner and Chinnaiyan, 2011; Frank and Miranti, 2013; Barbieri and Tomlins, 2014). Stem Cells Stem cells are required for the maintenance of high cell turnover tissues the place cells frequently have to get replaced, and like most epithelial organs, the prostate incorporates stem cells capable of multilineage differentiation. The saturation model (curve c) describes a steep T-dependent curve at T concentrations at or under the near-castrate range, with a plateau representing little or no additional progress above this focus. Both hypo- and hypermethylation define a field cancerization effect in regular prostate tissue, as revealed by methylation microarray analysis of tumor-associated and nonÔøΩtumor-associated regular prostatic tissue (Yang et al, 2013a). Chromatin reworking and histone post-translational modifications are additionally important epigenetic mechanisms of gene deregulation in prostate most cancers. These fusions, and different gross chromosomal rearrangements, happen by a process termed chromoplexy, whereby translocations and deletions arise in an interdependent manner and disrupt a number of cancer genes in a coordinated fashion (Baca et al, 2013). The presence of gene fusions that happen solely in most cancers additionally makes them targets for novel therapies. The pathway could additionally be activated by a quantity of mechanisms and leads to alterations in proliferation, cell survival, and invasion. The percentages spotlight the estimated frequency of every gene fusion on the premise of revealed screens. The objective of chemoprevention is to decrease the incidence of a given most cancers, simultaneously decreasing both treatmentrelated unwanted aspect effects and mortality. Primary chemoprevention targets the overall inhabitants of healthy individuals at risk to prevent the development of prostate most cancers. Tertiary prevention goals to forestall the event of a second primary cancer in an affected particular person. Numerous epidemiologic observations suggest associations between dietary and life-style elements and the risk for developing prostate cancer. The biologic rationale is that premalignant modifications seem as lengthy as 20 to 30 years earlier than the appearance of most cancers (Nelson et al, 2003; Umar et al, 2012), providing a possibility to intervene before a malignancy is established through the use of way of life modifications (dietary alterations, smoking cessation, exercise) or by chemoprevention. The problem of chemoprevention is finding an effective intervention that has acceptable toxicity, in addition to identifying a inhabitants of people at sufficiently increased risk for developing prostate cancer for whom chemoprevention is suitable and cost-effective. Although the security and feasibility of expectant administration have been well demonstrated, in the United States a analysis of prostate most cancers in an individual generally leads to curative-intent remedy (Welch and Albertsen, 2009) since lively surveillance has not been widely embraced due to considerations that medical staging and grading will underestimate the threat posed by cancers (Carter et al, 2003; Harlan et al, 2003; Barocas et al, 2008).
References - Brown HM, Storey G, George WH. Beclomethasone diproprionate: a new steroid aerosol for the treatment of allergic asthma. Br Med J 1972; 1: 585-590.
- Humphrey LS: Esophageal stethoscope loss complicating transesophageal echocardiography, J Cardiothorac Anesth 3:356, 1988.
- Nakada SY, Jerde TJ, Jacobson LM, et al: Cyclooxygenase-2 expression is up-regulated in obstructed human ureter, J Urol 168:1226, 2002.
- Dejung, B. (1994). Manuelle Triggerpunktbehandlung bei chronischer Lumbosakralgie. Schweizerische Medizinische Wochenschrift, 124 (Suppl. 62), 82n 87.
- Galant C, Rousseau E, Ho Minh Duc DK, Pauwels P. Re: Plexiform angiomyxoid myofibroblastic tumor of the stomach. Am J Surg Pathol 2008;32:1910;author reply 1912.
|