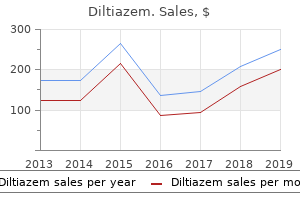
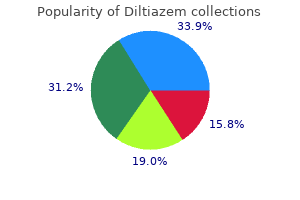
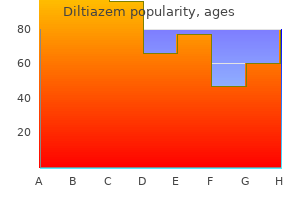
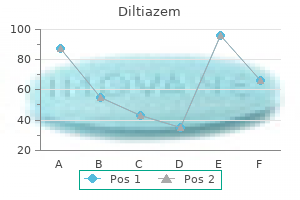
Diltiazem
Charles H. Cook, M.D. - Assistant Professor of Surgery and Critical Care
- The Ohio State University Hospitals
- Columbus, OH
Discount 60mg diltiazem visaBoth processes are passive steps which might be driven by the Na+ gradient into the cell (set up by the Na+ pump) 4 medications list order 180mg diltiazem mastercard. Hence medications reactions discount 180 mg diltiazem visa, glucose entry typically is referred to as secondary active transport although the entry step is passive medications by class discount diltiazem 60 mg on line. Once inside the cell symptoms emphysema buy diltiazem 60mg with mastercard, glucose is transported passively throughout the basolateral membrane by a facilitated diffusion course of (passive glucose transporter) into the interstitial area and taken up into the peritubular capillaries. Under regular circumstances, all filtered glucose is reabsorbed, aside from hint portions, from the tubular lumen of the proximal tubule, using the Na+glucose cotransport process at the luminal border. However, each Na+ and glucose must bind to particular, but saturable, sites on the Na+-glucose cotransport carrier protein, making glucose reabsorption saturable. In the presence of un-reabsorbed glucose, the "trapped" glucose will act as an osmotic solute, resulting in an osmotic diuresis. The related diuresis could be notably problematic in patients with diabetes mellitus. Galactose can compete with glucose for binding and transport by the Na+-glucose service so that with elevated plasma ranges of galactose, corresponding to in being pregnant, galactose can contribute to look of glucose in the urine. The proximal tubule can additionally be the positioning of reabsorption of sure organic acids, with essentially the most dominant usually being lactate anion. Two Na+dependent cotransport process at the luminal membrane appear to underlie organic acid reabsorption: one specific for monocarboxylates similar to lactate, pyruvate, acetoacetate, and -hydroxybutyrate and the opposite for di- and tricarboxylates such as malate, succinate, and citrate. Once contained in the cell, the carboxylates exit the cell via quite lots of exchange processes. Other natural acids, such as urate, an end product of purine catabolism, are each secreted and reabsorbed within the proximal tubule; each processes are Na+-independent, with the reabsorptive mechanisms dominating. Finally, the proximal tubule is the location of secretion of quite a few natural anions (paraaminohippurate, oxalate) and cations (choline, guanidine) by separate, saturable transport processes that always involve anion trade processes which are Na+-independent. Larger peptides and proteins corresponding to myoglobin and albumin bind to the luminal membrane and enter the cell by receptor-mediated endocytic processes and are delivered to lysosomes for degradation. Some filtered inorganic anions, similar to sulphate and phosphate, also are reabsorbed in the proximal tubule by way of a Na+ cotransport process; hence, their transport could be defined by a Tm and renal plasma threshold. His urine is "tea" coloured because of breakdown of skeletal muscle by the cocaine, so-called rhabdomyolysis. In diabetes mellitus, during which plasma glucose levels are markedly elevated, the excessive glucose load being filtered (with an elevated concentration) can exceed the capability of the luminal Na+-glucose cotransporter to reabsorb glucose (ie, the carrier is saturated). In diabetic ketoacidosis, plasma levels of glucose are elevated, resulting in an extra filtered load of glucose. The elevated fee of filtration of glucose can exceed the capacity of the Na+-glucose cotransporter in the proximal tubule to reabsorb all the glucose. Larger peptides and proteins corresponding to myoglobin and albumin bind to the luminal membrane and enter the cell by receptormediated endocytic processes and are delivered to lysosomes for degradation. Myoglobin, if crystallized in the renal tubules, can result in a poisonous effect, generally even renal failure. The reabsorption of glucose is coupled to Na+ by way of a luminal membrane Na+-glucose cotransporter. Many amino acids are reabsorbed within the proximal tubule by Na+amino acid cotransport processes, whereas others are reabsorbed by Na+-independent transport processes. Oligopeptides are reabsorbed within the proximal tubule by first being metabolized to their constitutive amino acids by luminal membrane peptidases after which being transported by Na+-amino acid cotransporters and Na+-independent amino acid transporters into the cell. Large peptides and proteins are reabsorbed in the proximal tubule by receptor-mediated endocytosis. His pulmonary edema and peripheral edema enhance when furosemide (Lasix), a loop diuretic, is administered. He returns to his main care doctor three weeks after the hospitalization and complains of weak point, dizziness, and nausea. Loop diuretics: Act on the sodium-potassium-chloride cotransporter in the loop of Henle and decrease the reabsorption of sodium and water. Hypokalemia with loop diuretics: An increased circulate rate by way of the late distal tubule and cortical collecting duct causes dilution of luminal potassium concentration and favors potassium secretion. Patients with congestive heart failure, cirrhosis, and pulmonary edema typically are began on these medicines. Their web site of motion is totally on the sodium-potassium-chloride cotransporter (Na-K-Cl cotransporter) in the loop of Henle, therefore the time period loop diuretics. This expected facet effect results as a result of the elevated move fee via the distal tubule and cortical amassing duct causes a dilution decrease within the luminal potassium concentration and favors potassium secretion. Hypokalemia presents clinically with muscle weak point, nausea, fatigue, dizziness, and intestinal ileus and, if potassium is low enough, could result in coma and fatal cardiac arrhythmias. Know about reabsorption and secretion within the loop of Henle, distal tubule, and amassing duct. Potassium-sparing diuretic: A diuretic that acts by inhibiting sodium reabsorption and potassium secretion within the late distal tubule and cortical collecting duct, thereby inhibiting the loss of potassium. Aldosterone: A mineralocorticoid hormone that stimulates the reabsorption of sodium from and the secretion of potassium into the late distal tubule and cortical amassing duct. The loop of Henle performs a particularly central function in giving the kidneys the ability to both concentrate and dilute urine, providing the inspiration for both osmotic steadiness and quantity steadiness. The loop of Henle consists of the thin descending limb, the skinny ascending limb, and the thick ascending limb, which ends on the macula densa (adjacent to its personal glomerulus). Active reabsorption of Na+, together with Cl-, by the thick ascending limb renders the medullary interstitial fluid hypertonic, causing reabsorption of water from the descending limb. However, relatively extra NaCl than water is transported into the interstitium, and so the medullary interstitium turns into hypertonic. With the countercurrent circulate of fluid down the descending limb and up the ascending limb, a vertical amplification of the interstitial hypertonicity develops, rising from approximately 290 mOsmol/kg on the corticomedullary junction to as excessive as 1200 to 1400 mOsmol/kg near the tip of the papilla (see the references at the end of this case for extra detail). Conversely, fluid leaving the thick ascending limb is hypotonic (approximately one hundred mOsmol/kg). An essential transport course of for Na+ and Cl- reabsorption within the thick ascending limb is the entry step at the luminal membrane: Modulating or inhibiting this cotransporter directly regulates internet transport of NaCl across the cell, thereby regulating the magnitude of the medullary interstitial hypertonicity. The K+ and Cl- diffusion processes set up a lumen-positive membrane potential, as proven in the determine. Because the paracellular pathway via the tight junctions is more selective for cations, the lumen-positive potential arising from the mobile transport processes will lead to passive reabsorption of Na+ between the cells as a part of the process of NaCl reabsorption on this section. As fluid leaves the loop of Henle, it enters the distal convoluted tubule within the cortex. Here Na+, along with Cl-, is reabsorbed actively, with the entry of Na+ across the luminal membrane being coupled to Cl- by a thiazidesensitive NaCl cotransporter. The water permeability of the section is comparatively low in order that little water is reabsorbed by this section. Fluid passes from the distal convoluted tubule into the late distal tubule (connecting tubule/initial accumulating tubule) and on into the cortical collecting duct and medullary amassing duct segments. The similar cells also comprise a K+ channel on the luminal border, and this supplies for K+ secretion across the luminal border into the tubular fluid. K+ enters the cell across the basolateral membrane via the Na+ pump, which maintains high intracellular K+ concentrations, after which exits the cell both via the luminal membrane K+ channel, giving rise to K+ secretion, or by way of a basolateral membrane K+ channel, recycling back into the interstitium. Aldosterone secretion is stimulated by volume depletion (through the renin-angiotensin-aldosterone system), as is noticed in hemorrhage and after the administration of high-ceiling loop diuretics.
Cheap diltiazem 180 mg without a prescriptionThereafter treatment molluscum contagiosum cheap 180mg diltiazem with mastercard, a prophylactic broad-spectrum antibiotic (not a fortified antibiotic) may be given at a therapeutic dose till the corneal epithelium is healed medicine keppra purchase diltiazem 60 mg on-line. Table 5-5 Notes for Table 5-5: Preparation of topical antibiotics Cefazolin 50 mg/mL 1 symptoms bipolar buy 60mg diltiazem with amex. Systemic antibiotics-especially the fluoroquinolones symptoms magnesium deficiency order 60mg diltiazem with visa, which have excellent ocular penetration- and intensive topical antibiotics are indicated in cases with suspected scleral and/or intraocular extension of infection. The profitable use of topical fluoroquinolones in the 1990s led to a reduction in the variety of cultures carried out for circumstances of presumed infectious keratitis. American Academy of Ophthalmology follow tips proceed to recommend initial cultures for infiltrates that stretch to the center of the cornea, into deep stroma, or throughout a large area (>2 mm), in addition to for these patients whose history or medical features suggest fungal, amebic, mycobacterial, or drug-resistant organisms because the causative agents. The yield for corneal cultures and smears is significantly larger before the initiation of antibiotic treatment, but cases unresponsive to such therapy ought to still be cultured, with some suggesting discontinuation of antibiotics for 12�24 hours to encourage yield. If cultures are carried out, initial broad-spectrum remedy ought to proceed till an organism is recovered. Once the offending microbe is identified, or the clinical response suggests the change, acceptable monotherapy may be thought-about (see Table 5-5) to keep coverage and reduce toxicity. However, laboratory sensitivities are based on antibiotic tissue ranges achievable by systemic administration, and the degrees achieved by topical administration are much greater. Often, a bacterial keratitis will reply in vivo even when in vitro information suggest resistance. Several medical parameters are helpful to monitor clinical response to antibiotic remedy: blunting of the perimeter of the stromal infiltrate decreased density of the stromal infiltrate reduction of stromal edema and endothelial inflammatory plaque reduction in anterior chamber inflammation reepithelialization cessation of corneal thinning the position of corticosteroid remedy for bacterial keratitis stays controversial. Tissue destruction results from a mixture of the direct effects of the bacteria and an exuberant host inflammatory response consisting of polymorphonuclear leukocytes and proteolytic enzymes, which predominate even after corneal sterilization. Corticosteroids are effective at modifying this response, but additionally they inhibit the host response to an infection. The literature strongly suggests that corticosteroid therapy administered previous to applicable antibiotic remedy worsens prognosis. No impact on last visible consequence or complication fee was seen, however a pattern toward improved outcomes was famous in those sufferers with the worst preliminary imaginative and prescient who acquired corticosteroids. In reality, selected sufferers may profit from the addition of corticosteroids to antibiotic therapy. Future research of the appropriate timing and dosage could additional refine the indications for corticosteroid use. The affected person must have the ability to return for frequent follow-up examinations and demonstrate adherence to applicable antibiotic therapy. No different related virulent or difficult-to-eradicate organism is found or suspected. Corticosteroid drops could additionally be began in average dosages (prednisolone acetate or phosphate 1% every 6 hours), and the patient must be monitored at 24 and 48 hours after initiation of therapy. If the patient shows no antagonistic effects, the frequency of administration could additionally be adjusted based on scientific response. The involved area must be recognized preoperatively, and an try should be made to circumscribe all areas of an infection. Peripheral iridectomies are indicated, as a end result of patients may develop seclusion of the pupil from inflammatory pupillary membranes. The affected person must be treated with acceptable antibiotics, cycloplegics, and intense topical corticosteroids postoperatively. The relative danger of ulcerative keratitis amongst customers of daily-wear and extended-wear gentle contact lenses. Srinivasan M, Mascarenhas J, Rajaraman R; Steroids for Corneal Ulcers Trial Group. The commonest pathogens are Mycobacterium fortuitum and Mycobacterium chelonei, which can be found in soil and water. These organisms must be suspected in delayed-onset postrefractive infections, classically with recalcitrant, nonsuppurative infiltrates. The prognosis may be confirmed with acidfast stain or culture on Lowenstein-Jensen media. Treatments include oral and topical clarithromycin, moxifloxacin, and gatifloxacin. Amikacin, beforehand the only remedy choice, has been largely changed by these newer treatment choices. Infections following laser in situ keratomileusis: an integration of the published literature. Comparative efficacy of topical gatifloxacin with ciprofloxacin, amikacin, and clarithromycin in the treatment of experimental Mycobacterium chelonae keratitis. Fungal Keratitis Fungal keratitis is less frequent than bacterial keratitis, typically representing lower than 5%�10% of corneal infections in reported medical series in the United States. Trauma to the cornea with plant or vegetable materials is the leading risk factor for fungal keratitis. Contact lens put on is rising as another risk factor for the event of fungal keratitis. In early 2006, an outbreak of contact lens�associated Fusarium keratitis was observed, first in Singapore and the Pacific Rim and then in the United States. Bausch and Lomb withdrew the solution from the world market on May 15, 2006, with a subsequent steep decline in Fusarium instances across the United States. Patients with fungal keratitis are most likely to have fewer inflammatory signs and signs through the initial interval than these with bacterial keratitis and should have little or no conjunctival injection upon initial presentation. On the other hand, ache in fungal keratitis may be out of proportion to the relatively uninflamed cornea. Superficial lesions may appear graywhite; elevate the floor of the cornea; and have a dry, rough, or gritty texture detectable on the time of diagnostic corneal scraping. Occasionally, multifocal or satellite infiltrates may be present, though these are much less frequent than beforehand reported. In addition, a deep stromal infiltrate might happen within the presence of an intact epithelium. An endothelial plaque and/or hypopyon can also happen if the fungal infiltrate(s) is sufficiently deep or giant or has penetrated the anterior chamber. As the keratitis progresses, intense suppuration might develop, and the lesions might resemble these of bacterial keratitis. At this point, rapidly progressive hypopyon and anterior chamber inflammatory membranes could develop. Extension of fungal an infection into the anterior chamber is often seen in circumstances with rapidly progressive anterior chamber irritation. Occasionally, fungus might invade the iris or posterior chamber, and angle-closure glaucoma may develop from inflammatory pupillary block.
Generic diltiazem 180 mgThe inheritance sample is usually autosomal recessive abro oil treatment buy diltiazem 180 mg, however autosomal dominant forms have been reported hair treatment cheap diltiazem 60 mg. Note the marked attenuation of the photoreceptor cell nuclei within the outer nuclear layer and loss of the outer segments over the confluent drusen medications vascular dementia diltiazem 60 mg sale. A symptoms 5 days before your missed period diltiazem 60mg cheap, Color photograph reveals ill-defined, yellowish, reticular sample (between arrowheads) in the superior macula. The pathologic discovering of pigment-containing cells with lipofuscin and drusen-like materials within the subretinal house correlates clinically with the vitelliform look. Adult-onset foveomacular pigment epithelial dystrophy: clinicopathologic correlation of three cases. D, Subretinal drusenoid deposits (yellow arrowheads) are the histologic correlate of reticular pseudodrusen. Submicrometer epoxy part, toluidine blue stain, osmium paraphenylenediamine postfixation. Only the commonest diffuse photoreceptor dystrophy, retinitis pigmentosa, is mentioned right here. The disease is characterized primarily by the lack of rod photoreceptor cells via apoptosis. Cones are seldom immediately affected by the identified mutations; nonetheless, they degenerate secondary to the loss of rods. The term retinitis pigmentosa is a misnomer, as a end result of clear proof of irritation is missing. The arterioles, although narrowed clinically, show no histologic abnormality initially. The optic nerve may present diffuse or sectoral atrophy, with gliosis as a late change. Histopathologic-genotypic correlations in retinitis pigmentosa and allied diseases. Note the multicellular, thick ganglion cell layer figuring out the macular area (H&E stain). Immunohistochemical research have demonstrated that tumor cells stain optimistic for neuron-specific enolase, rod outer phase photoreceptor�specific S-antigen, and rhodopsin. Tumor cells also secrete an extracellular substance generally recognized as interphotoreceptor retinoid-binding protein, which can be a product of regular photoreceptors. The regular gene suppresses the development of retinoblastoma (and probably other tumors, such as osteosarcoma). Retinoblastoma develops when each homologous loci of the suppressor gene become nonfunctional, either by a deletion error or by mutation. Although 1 normal gene is sufficient to suppress the event of retinoblastoma, when 1 regular gene and 1 abnormal gene are current, the prevalence of a mutation in the normal gene may result in loss of tumor suppression and permit retinoblastoma to develop. This type of unilateral retinoblastoma is characterized by distinct histologic features (ie, undifferentiated cells with outstanding and multiple nucleoli, necrosis, apoptosis, little calcification, absence of FlexnerWintersteiner rosettes, and nuclear molding), just a few of the genomic copy quantity changes which might be characteristic of retinoblastoma, and really early age (ie, median age of four. Histologic options Histologically, retinoblastoma consists of cells with round or oval nuclei which are approximately twice the size of a lymphocyte. Mitotic exercise is normally excessive, although frequent apoptotic cells could make this troublesome to assess. Cuffs of viable cells course alongside blood vessels; regions of ischemic necrosis start 90�120 �m from nutrient vessels. Cells shed from retinoblastoma tumors remain viable within the vitreous and subretinal space, and will ultimately become seeds throughout the eye. The formation of extremely organized FlexnerWintersteiner rosettes is a characteristic characteristic of retinoblastoma that happens only in rare instances in different neuroblastic tumors (eg, primitive neuroectodermal tumors). A, Elevated, red-orange, surround a central lumen lined by a refractile structure. B, Late fluorescein this refractile lining corresponds to the exterior limiting angiogram (860 seconds) shows membrane of the retina that represents websites of hyperfluorescent polypoidal lesions (arrows) attachments between photoreceptors and M�ller cells. Note the rosette is characterised by a single row of columnar the persistent red-orange lesions within the cells with eosinophilic cytoplasm and peripherally peripapillary area. Evidence of photoreceptor differentiation has additionally been documented for an additional flowerlike construction generally identified as a fleurette. The fleurette expresses a greater degree of retinal differentiation than the Flexner-Wintersteiner rosette. Progression the most common route for a retinoblastoma tumor to spread from the attention is by means of the optic nerve. High-risk histologic features related to metastasis and survival embody optic nerve invasion (laminar, retrolaminar, or reduce margin), large choroidal invasion, extraocular extension, and in depth tumor necrosis. Spread to regional lymph nodes could also be seen when a tumor involving the anterior segment grows into the conjunctival substantia propria, especially when the trabecular meshwork is concerned. Extensively necrotic retinoblastoma is associated with high-risk prognostic components. Proceedings of the consensus conferences from the International Retinoblastoma Staging Working Group on the pathology tips for the examination of enucleated eyes and evaluation of prognostic risk elements in retinoblastoma. Retinocytoma differs from retinoblastoma in the following ways: Retinocytoma cells have more cytoplasm and extra evenly dispersed nuclear chromatin than retinoblastoma cells. Although calcification may be recognized in retinocytoma, necrosis is usually absent. Medulloepithelioma Medulloepithelioma is a congenital neuroepithelial tumor arising from primitive medullary epithelium (ie, the internal layer of the optic cup). This tumor usually happens in the ciliary body however has also been documented in the retina and optic nerve. Cell nuclei are stratified in three to 5 layers, and the whole construction is lined on one side by a skinny basement membrane. One surface secretes a mucinous substance, rich in hyaluronic acid, that resembles primitive vitreous. Stratified sheets of cells are capable of forming mucinous cysts which might be clinically attribute. Medulloepitheliomas that contain strong lots of neuroblastic cells indistinguishable from retinoblastoma are tougher to classify. Medulloepitheliomas that have substantial numbers of undifferentiated cells with observed (H&E stain). A, Yellowish, egg yolk�like lesion with focal pigment clumping and mottling within the central macula. Note the reticular pseudodrusen, that are inconspicuous in the scientific photograph, in the superior and inferior macula (asterisks). D, Histologic findings embody pigmentcontaining cells in the subretinal area (arrowheads) and outer neurosensory retina (arrow) (H&E stain). E, Electron microscopy shows pigment-containing cells filled with lipofuscin (arrowheads). Heteroplastic tissue, similar to cartilage or clean muscle, may be found in medulloepitheliomas. Tumors composed of cells from 2 completely different embryonic germ layers are referred to as teratoid medulloepitheliomas.
Proven diltiazem 60mgHowever symptoms after conception buy generic diltiazem 180mg online, their use for more than 5�7 consecutive days might predispose to compensatory persistent vascular dilation treatment 6th feb cheap diltiazem 60mg with visa. Topical mast-cell stabilizing agents corresponding to cromolyn sodium and lodoxamide tromethamine may be helpful for treating seasonal allergic conjunctivitis medications causing pancreatitis diltiazem 180mg on line. Treatment effects usually require continued use over 7 or extra days; hence medications for schizophrenia diltiazem 60 mg without a prescription, these agents are generally ineffective in the acute part of hay fever conjunctivitis. Topical cyclosporine and oral antihistamines may provide symptom relief in some sufferers. Hyposensitization injections (immunotherapy) could be beneficial if the offending allergen has been identified. Topical corticosteroids are very efficient in managing ocular allergy, however they want to be used with caution, besides in very severe cases, due to their adverse results. It occurs predominantly in sufferers of African or Asian descent and is more prevalent in hotter climates. The limbus has a thickened, gelatinous appearance, with scattered opalescent mounds and vascular injection. Punctate epithelial erosions in the superior and central cornea are incessantly observed. Pannus happens most commonly in the superior cornea, however often 360� corneal vascularization could develop. Climatotherapy, such as the use of home air-conditioning or relocation to a cooler setting, could be helpful. Patients with delicate to reasonable illness might reply to topical mast-cell stabilizers. In sufferers with seasonal exacerbations, these drops must be began no much less than 2 weeks before signs often start. Because of the chance that sufferers will develop corticosteroid-related issues from long-term administration, however, these medication must be reserved for exacerbations that end in moderate to extreme discomfort and/or decreased vision. To discourage indiscriminate use for aid of gentle symptoms, the affected person and family have to be completely knowledgeable of the potential dangers of long-term topical corticosteroid therapy. Cooperative sufferers could be supplied a substitute for topical delivery that avoids the issue of continuing self-medication: supratarsal injection of corticosteroid. The supratarsal subconjunctival area is positioned superior to the higher border of the superior tarsus and is most easily reached by everting the upper eyelid. After the upper eyelid is everted and the supratarsal conjunctiva has been anesthetized, supratarsal injection of zero. Monitoring of intraocular stress is obligatory, as corticosteroid-induced strain spikes are attainable. Reported adverse results of cyclosporine embrace punctate epithelial keratopathy and ocular surface irritation. Recent patents and emerging therapeutics within the treatment of allergic conjunctivitis. A randomized, placebo-controlled scientific trial of tacrolimus ophthalmic suspension 0. Atopic people show indicators of kind I quick hypersensitivity responses as well as depressed systemic cell-mediated immunity. Complications associated to this predisposition to infection might contribute to , or compound, the first immunopathogenic manifestations. Eosinophils in conjunctival cytology specimens are much less quite a few and are less usually degranulated. Characteristic posterior subcapsular and/or multifaceted or shield-shaped anterior subcapsular lens opacities might often develop. Corneal findings embody punctate erosions, persistent epithelial defects, an increased incidence of ectatic corneal illnesses such as keratoconus and pellucid marginal degeneration, and an increased incidence of staphylococcal and herpes simplex infections. In addition, patients ought to be carefully monitored for issues of infectious diseases that will warrant specific remedy, such as secondary staphylococcal infections. In these extreme instances, the indications for systemic remedy embody continual ocular floor inflammation unresponsive to topical remedy, discomfort, progressive cicatrization, and peripheral ulcerative keratopathy. Topical tacrolimus ointment for therapy of intractable atopic keratoconjunctivitis: a case report and evaluate of the literature. Latent and activated types of matrix metalloproteinase-9 have also been identified. The explanation for ligneous conjunctivitis has recently been linked to severe deficiency in sort I plasminogen, with hypofibrinolysis as the first defect. Use of purified plasminogen, white-red lesions of agency consistency in each contemporary frozen plasma, heparin, corticosteroids, eyelids of the left eye. Many instances of ligneous conjunctivitis eventually resolve spontaneously after several months to a couple of years. Treatment of ligneous conjunctivitis with topical plasmin and topical plasminogen. Heparin in the long-term administration of ligneous conjunctivitis: a case report and evaluate of literature. Ligneous conjunctivitis: a clinicopathological, immunohistochemical, and genetic research including the remedy of two sisters with multiorgan involvement. As granzyme enters a target cell by way of the perforin channels, it leads to keratinocyte apoptosis. If Fas is the demise receptor protein on the goal cell membrane, extension of the apoptosis can result. The time period erythema multiforme refers to an acute inflammatory vesiculobullous response of the skin and mucous membranes. It is characterized by keratinocyte apoptosis and epidermal necrolysis with minimal inflammatory infiltrate within the dermal stroma. Fever, arthralgia, malaise, and higher or decrease respiratory symptoms are usually sudden in onset. Skin eruption follows within a quantity of days, with a basic "goal" lesion consisting of a purple middle surrounded by a pale ring after which a pink ring, although maculopapular or bullous lesions are also widespread. The mucous membranes of the eyes, mouth, and genitalia may be affected by bullous lesions with membrane or pseudomembrane formation. New lesions may seem over 4�6 weeks, with approximately 2-week cycles for every crop of lesions. Long-term ocular issues outcome from ocular floor cicatrization, resulting in conjunctival shrinkage, keratinization of the eyelid margins, trichiasis, and tear deficiency. Eyelid margin keratinization and scarring is an important risk factor for poor long-term outcomes in these sufferers. Immediate discontinuation of the offending agent has been related to lowered mortality and improved outcome. Systemic therapy is principally supportive and is geared toward managing dehydration and superinfection. The mainstay of acute ocular remedy contains lubrication with preservative-free synthetic tears and ointments and vigilant surveillance for the early manifestations of ocular infections.
Buy 180 mg diltiazem overnight deliveryIf this "wedge of stress" exceeds the tensile power of ocular constructions symptoms 7 cheap diltiazem 60 mg online, the vessels in the peripheral iris and face of the ciliary body may rupture treatment wetlands diltiazem 60mg low price, leading to doctor of medicine buy 180mg diltiazem amex hyphema medications mobic buy diltiazem 180mg on line. The drive could cause scleral ruptures, typically at the limbus and posterior to the muscle insertions, the place the sclera is thinner and unsupported by the orbital bones. Severe trauma results in subluxation of the lens, retinal dialysis, optic nerve avulsion, and/or vitreous hemorrhage. Medical management the general treatment plan for traumatic hyphema must be directed at minimizing the potential of secondary hemorrhage. Specifics of medical management stay controversial; however, most patients are treated with the following: protecting protect over the injured eye, restriction of physical exercise, elevation of the top of the mattress, and day by day observation. To reduce the danger of rebleeding, nonaspirin analgesics must be used for ache reduction; nevertheless, even nonsteroidal anti-inflammatory medications can increase the chance of rebleeding. Most ophthalmologists administer long-acting topical cycloplegic agents initially for consolation, to facilitate posterior phase analysis, and to get rid of iris motion. Topical corticosteroids are helpful in controlling anterior chamber irritation and preventing synechiae formation, and so they may play a job in stopping rebleeding. Oral corticosteroids could additionally be used to facilitate the decision of extreme inflammation and/or to stop rebleeding. Topical antihypertensives (-blockers and -agonists) are the mainstay of remedy, although often intravenous or oral hyperosmotic brokers could additionally be required. Surgery is usually beneficial on the earliest definitive detection of blood staining. Patients with preexisting optic nerve harm or sickle hemoglobinopathies could require earlier intervention. Table 13-4 the best surgical technique is anterior chamber irrigation with balanced salt resolution via a paracentesis. The objective is to remove circulating red blood cells that will obstruct the trabecular meshwork; elimination of the whole clot is neither necessary nor wise. The use of a cutting instrument or intraocular diathermy may be needed in extreme circumstances. Iris damage, lens damage, endothelial cell trauma, and extra bleeding are the major complications of surgical intervention. Sickle cell complications When an African American affected person develops a traumatic hyphema, a sickle cell workup should be performed to evaluate the patient for the potential for sickle cell hemoglobinopathy. Sickle cell sufferers and carriers of the sickle cell trait are predisposed to sickling of pink blood cells in the anterior chamber. Carbonic anhydrase inhibitors and osmotic brokers should be used with caution due to their tendency to reduce the pH and lead to hemoconcentration, both of which can exacerbate sickling of red blood cells. After a topical anesthetic has been utilized, the conjunctival laceration ought to be explored under slit-lamp examination using sterile forceps or cotton-tipped applicators. If any query remains as to whether or not the globe has been penetrated, consideration should be given to performing a peritomy within the working room to higher discover and examine the injured space. Conjunctival Foreign Body Foreign our bodies on the conjunctival surface are best acknowledged with slit-lamp examination. It is imperative to evert the upper eyelid to look at the superior tarsal plate and eyelid margin in all sufferers with a historical past that means a overseas body. Following eversion of the upper eyelid, copious irrigation should be used to cleanse the fornix. This process ought to then be repeated using a Desmarres retractor for the higher and lower eyelids. Glass particles, cactus spines, and insect hairs are sometimes difficult to see, but a cautious search of the cul-de-sac with high magnification aids in identification and removal. With slit-lamp magnification, the examiner uses a moistened cotton-tipped applicator to take away superficial foreign materials. When a patient stories foreign-body sensation, topical fluorescein should be instilled to verify for the fantastic, linear, vertical corneal abrasions that are attribute of retained foreign our bodies on the eyelid margin or superior tarsal plate. Foreign matter embedded in tissue is eliminated with a sterile, disposable hypodermic needle. Corneal Foreign Body Identifying the probable composition of a foreign physique based mostly on a detailed historical past is essential as a outcome of the increased risk of an infection associated with vegetable matter. Corneal overseas bodies are identified most effectively throughout slit-lamp examination. Before removing the corneal overseas physique, the clinician should assess the depth of corneal penetration. If anterior chamber extension is present or suspected, the international body ought to be removed in a sterile operating-room surroundings. Overly aggressive attempts to remove deeply embedded foreign our bodies on the slit lamp may end in leakage of aqueous humor and collapse of the anterior chamber. If several glass foreign our bodies are current, the entire uncovered fragments ought to be removed. Fragments which might be deeply embedded in the cornea are often inert and may be left in place. Careful gonioscopic analysis of the anterior chamber is important to be sure that the iris and the angle are freed from any retained glass particles. Corneal iron foreign our bodies and rust rings can often be removed on the slit lamp under topical anesthesia with a disposable (25- or 26-gauge) hypodermic needle, resulting in minimal tissue disruption. A battery-powered dental burr with a sterile tip may be used; nonetheless, caution have to be taken to keep away from excessive tissue disruption and thus decrease scar formation. A metallic international physique that enters the corneal stroma beyond the Bowman layer at all times ends in some extent of scar formation. When these scars happen in the visual axis, they may lead to glare and decreased imaginative and prescient from irregular astigmatism. Judicious decision making is obligatory; if multiple, very small overseas our bodies are seen within the deep stroma (as might happen after an explosion) with no resultant irritation or sign of an infection, the affected person may be monitored closely, as a end result of aggressive surgical manipulation of the cornea seeking the final particle may be pointless. In these cases, a radiologic search, together with use of computed tomography, for an intraocular international body should be carried out. Therapy following the removing of a corneal foreign body consists of topical antibiotics, cycloplegia, and occasionally the appliance of a firm strain patch or bandage contact lens to help the healing process. If a stress patch or bandage contact lens is used, the risk of an infection is increased and therefore the patient ought to be carefully monitored. It is very important to make a distinction between a "clear" corneal abrasion, which generally has sharply outlined edges and little to no related inflammation (when seen acutely), and a true corneal ulcer, which is characterized by an inflammation-mediated breakdown of the stromal matrix and attainable thinning. Also, it may be very important evert the upper eyelid and look at the superior cul-de-sac to rule out a retained foreign physique as a explanation for the abrasion. Occasionally, a patient could not recall a particular historical past of trauma but still present with signs and symptoms suggestive of a corneal abrasion. Herpes simplex virus keratitis should be excluded as a possible diagnosis in such instances. Abrasions could additionally be managed with antibiotic ointment in combination with topical cycloplegia alone. Topical nonsteroidal anti-inflammatory brokers have anesthetic properties and could additionally be used for the primary 24�48 hours for pain aid in selected sufferers.
Agaricus (Agaricus Mushroom). Diltiazem. - Dosing considerations for Agaricus Mushroom.
- How does Agaricus Mushroom work?
- What other names is Agaricus Mushroom known by?
- Type 2 diabetes. Some research shows that taking agaricus mushroom extract along with other diabetes medications might decrease insulin resistance which is common in people with type 2 diabetes.
- What is Agaricus Mushroom?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97109
Discount 60mg diltiazem fast deliveryThese cases should be referred to as "anterior and intermediate uveitis" and never as "panuveitis medicine remix diltiazem 180mg fast delivery. Anterior Uveitis the anterior chamber is the primary web site where irritation is noticed in anterior uveitis-the results of inflammation of the iris and ciliary physique medications i can take while pregnant buy discount diltiazem 60 mg line. If the inflammation is confined to the anterior chamber it could also be known as iritis; whereas if there are cells in the retrolental (anterior vitreous) house treatment west nile virus buy diltiazem 60 mg without a prescription, it could even be known as iridocyclitis medications jfk was on diltiazem 60 mg on line. When more than one ocular construction is concerned, the conference is that the first website of irritation is recognized as first. Table 5-4 Intermediate Uveitis In intermediate uveitis, the main website the place irritation is apparent is the vitreous cavity. Inflammation in this center portion (posterior ciliary physique, pars plana) of the attention manifests primarily as floaters affecting imaginative and prescient; the attention regularly appears quiet externally. Posterior Uveitis Posterior uveitis is defined as intraocular inflammation primarily involving the retina and/or choroid. Inflammatory cells may be noticed diffusely throughout the vitreous cavity, overlying foci of energetic inflammation, or on the posterior vitreous face. Ocular examination reveals focal, multifocal, or diffuse areas of retinitis or choroiditis, with varying levels of vitreous mobile exercise; totally different entities might have a similar clinical appearance. Certain posterior uveitic syndromes current both as a focal or multifocal retinitis, whereas others localize predominantly to the choroid in a similar distribution, involving the retina secondarily, with or without vitreous cells and/or involvement of the retinal vasculature (Table 5-5; see Table 5-4). Chapters 6 and 7 focus on noninfectious and infectious posterior uveitis, respectively, in greater detail. Table 5-5 Table 5-5 Panuveitis In panuveitis, irritation is diffuse with no predominant website. Inflammation is observed within the anterior chamber, vitreous, and retina and/or choroid. Many systemic infectious and noninfectious ailments related to uveitis may produce diffuse intraocular irritation with concomitant anterior uveitis and posterior uveitis. Chapters 6 and seven talk about noninfectious and infectious panuveitis, respectively, in greater depth, and Chapter eight covers endophthalmitis. Retinal Vasculitis Retinal vasculitis is defined by the presence of retinal vascular adjustments in association with ocular irritation. The time period is utilized in distinction to vasculopathy, during which there are vessel modifications but no visible proof of inflammation. Blood vessel changes embody perivascular sheathing and vascular leakage or occlusion proven on fluorescein angiography studies. Categorization by Clinical Course Uveitis may be subcategorized as acute, chronic, or recurrent: acute uveitis is used to describe episodes of sudden onset and restricted period that often resolve inside 3 months or less, whereas persistent uveitis is persistent, with relapse occurring in lower than 3 months after discontinuing remedy. Recurrent uveitis is characterised by repeated episodes separated by periods of inactivity without remedy that last three months or longer. Whether the irritation is extreme or low grade can influence categorization and prognosis. The inflammatory course of could happen in 1 or each eyes, or it may alternate between them. The distribution of ocular involvement-focal, multifocal, or diffuse-is also helpful to notice when classifying uveitis. Nongranulomatous irritation usually has a lymphocytic and plasma cell infiltrate, whereas granulomatous reactions additionally embrace epithelioid and giant cells. Symptoms of Uveitis Symptoms produced by uveitis depend on which part of the uveal tract is infected, the rapidity of onset (sudden or insidious), the length of the illness (limited or persistent), and the course of the disease (acute, continual, or recurrent). Acute-onset anterior uveitis causes pain, photophobia, redness, and blurred imaginative and prescient. Pain often results from the acute onset of inflammation within the area of the iris, or from secondary glaucoma. The pain related to ciliary spasm in anterior uveitis could also be a referred pain that radiates over the bigger area served by cranial nerve V (the trigeminal nerve). Epiphora, redness, and photophobia are normally current when irritation entails the iris, cornea, or iris�ciliary physique. Floaters end result from the shadows solid by vitreous cells and "snowballs" on the retina. Presenting signs in sufferers with posterior uveitis embrace painless decreased visual acuity, floaters, photopsia, metamorphopsia, scotomata, nyctalopia, or a combination of these symptoms. Blurred vision may result from refractive error such as a myopic or hyperopic shift related to macular edema, hypotony, or a change in lens place. Table 5-6 Signs of Uveitis the chemical mediators concerned in inflammation (see Chapter 1) result in vascular dilation (ciliary flush), elevated vascular permeability (aqueous flare), and chemotaxis of inflammatory cells into the eye (aqueous and vitreous mobile reaction). Perilimbal vascular engorgement (ciliary flush) or diffuse injection of the conjunctiva, episclera, or both is typical with acute anterior uveitis. Large keratic precipitates similar to these typically indicate a granulomatous disease course of. Note the three types of iris nodules: A, Koeppe nodules (pupillary border); B, Busacca nodules (midiris); and C, Berlin nodules (iris angle). The vitreous grading scale shown right here was used within the Multicenter Uveitis Steroid Treatment Trial. Vitreous cells are usually graded by observing the retrolental house in a dilated eye utilizing the slitlamp biomicroscope and a 1- � 0. The consensus is that cells within the vitreous strands are old, and cells in the syneretic areas could additionally be new. With this method, standardized pictures are used for comparison with scientific images to finally arrive at the stage of vitreous haze. Additional uveitic adjustments may be noticed in the vitreous, specifically, snowball opacities, that are widespread in sarcoidosis or intermediate uveitis exudates over the pars plana (snowbank). Posterior Segment Signs within the posterior segment of the attention embody retinal or choroidal inflammatory infiltrates inflammatory sheathing of arteries or veins exudative, tractional*, or rhegmatogenous* retinal detachment retinal pigment epithelial hypertrophy or atrophy* atrophy or swelling of the retina, choroid, or optic nerve head* preretinal or subretinal fibrosis* retinal or choroidal neovascularization* An asterisk is used to indicate structural problems. Standardization of vitreal inflammatory activity in intermediate and posterior uveitis. A complete history and evaluation of techniques is of paramount importance in helping to elucidate the cause for uveitis. In this regard, a diagnostic survey for uveitis as proven in the appendix can be very helpful. The age, sex, sexual practices, and racial background of the affected person are important components in some uveitic syndromes. Table 5-10 Although ocular irritation may be an isolated course of involving solely the eye, it may additionally be related to a systemic situation. In some cases, the uveitis may very well precede the event of irritation at different body sites.
Syndromes - Antacids or histamine blockers to control stress ulcers
- Abdominal distention (swelling)
- Wheezing
- Fear of dying
- Have a swollen abdomen (distention) that does not go away
- You also have slurred speech, a change in vision, problems moving your arms or legs, loss of balance, confusion, or memory loss with your headache
- Medicines to decrease swelling
- Apolipoprotein B blood test
60 mg diltiazem amexLeft untreated medications mothers milk thomas hale cheap diltiazem 180 mg on-line, persistent corneal epithelial defects can progress to vascularization and corneal opacification or scarring treatment tracker purchase diltiazem 60mg on line. Alternatively medications qt prolongation cheap diltiazem 180mg with mastercard, progressive irritation can result in medicine rap song generic diltiazem 180mg necrosis and thinning of the stroma, occasionally leading to perforation. This medical downside could additionally be unrecognized and normally presents as a diffuse punctate keratopathy. In some instances, pericentral pseudodendritiform lesions and pseudogeographic defects could happen. Persistent epithelial defects usually occur in sufferers with diabetic retinopathy following epithelial debridement during vitreoretinal procedures. Diabetic neuropathy is assumed to be a possible reason for neurotrophic keratopathy and nonhealing epithelial defects. The administration of neurotrophic keratopathy with or without persistent epithelial defects starts with a cautious historical past. Initially, any potentially aggravating topical medications have to be discontinued, as beforehand described. Autologous serum drops (20%) containing growth elements and fibronectin can be very useful. In cases involving significant dry eye, momentary or everlasting punctal occlusion is effective in bettering the tear film and restoring the ocular floor. Patching; low-water-content, highly oxygen-permeable therapeutic contact lenses; or scleralbearing contact lenses with a fluid-filled reservoir might facilitate reepithelialization or enhance the keratopathy. Lateral and/or medial tarsorrhaphy may be required to forestall surface desiccation. Tarsorrhaphy decreases tear-film evaporation and tear-film osmolarity, presumably by decreasing the surface area of corneal exposure. Corneal collagen crosslinking early in the center of a melt has been reported to be helpful in a small variety of sufferers. Amniotic membrane grafting has been reported to encourage therapeutic of persistent epithelial ulcerations. Partial or complete conjunctival flaps forestall corneal melting, however they should be used as a last resort to have the ability to protect the eye. Trichiasis and Distichiasis Trichiasis is an acquired condition during which eyelashes emerging from their regular anterior origin curve inward towards the cornea. Most cases are most likely the end result of subtle cicatricial entropion of the eyelid margin. Distichiasis is a congenital (often autosomal dominant) or acquired situation in which an extra row of eyelashes emerges from the ducts of meibomian glands. These eyelashes can be fine and properly tolerated or coarser and a risk to corneal integrity. Aberrant eyelashes emerge from the tarsus as a outcome of chronic inflammatory circumstances of the eyelids and conjunctiva, corresponding to trachoma, mucous membrane pemphigoid, Stevens-Johnson syndrome, persistent blepharitis, and chemical burns. Mechanical epilation is temporary as a result of the eyelashes usually grow again inside 2�3 weeks. Electrolysis works nicely just for removing a few eyelashes; nevertheless, it may be preferable in youthful sufferers for beauty reasons. Cryotherapy continues to be a common remedy for aberrant eyelashes, however freezing can lead to eyelid margin thinning, lack of adjoining regular eyelashes, and protracted lanugo (hairs), which may continue to abrade the cornea. Treatment at �20�C must be limited to less than 30 seconds to minimize complications. The most popular surgical approach for aberrant eyelashes is tarsotomy with eyelid margin rotation. Three-year outcomes of the Surgery for Trichiasis, Antibiotics to Prevent Recurrence trial. Factitious Ocular Surface Disorders Factitious disorders embrace a spectrum of self-induced accidents with signs or bodily findings that the patient deliberately produces to find a way to assume the sick function. Factitious conjunctivitis usually reveals evidence of mechanical harm to the inferior and nasal quadrants of the cornea and conjunctiva. Patients often have medical training or work in a medical setting, and so they typically have an perspective of serene indifference. The detached conjunctival tissues usually present no proof of inflammation on pathologic examination. Mucus-fishing syndrome Mucus-fishing syndrome is characterized by a well-circumscribed sample of rose bengal or lissamine green staining on the nasal and inferior bulbar conjunctiva. All sufferers have a history of increased mucus production as a nonspecific response to ocular surface damage. Patients normally demonstrate vigorous eye rubbing and compulsive removing of mucus strands from the fornix (mucus fishing). The resultant epithelial harm heightens the ocular floor irritation, which in flip stimulates further mucus production, leading to a vicious circle. Topical anesthetic abuse Clinical utility of topical anesthetics has turn into an integral part of the trendy follow of ophthalmology. However, indiscriminate use of topical anesthetics can cause serious ocular surface toxicity and problems. Loss of microvilli, discount of desmosomes and other intercellular contacts, and swelling of mitochondria and lysosomes have been reported in ultrastructural research. The clinical features of anesthetic abuse are characterised by the failure of the presenting condition, corresponding to corneal abrasions or infectious keratitis, to reply to acceptable remedy. As the abuse continues, the eye becomes extra injected and epithelial defects seem or take on a neurotrophic appearance. As the process continues, keratic precipitates and hypopyon develop, thus mimicking an infectious course. Stromal vascularization may occur in chronic abuse, and secondary an infection might ensue. Because of the presence of corneal infiltrates and anterior phase inflammation, infectious keratitis have to be dominated out by way of corneal scraping, tradition, or biopsy. Differential analysis includes bacterial, fungal, herpetic, and amebic keratitis. Often, the prognosis is made solely when the patient is found concealing the anesthetic drops. Once the analysis is made and infectious keratitis is dominated out, corneal healing normally occurs if all exposure to anesthetics is removed. The epithelium exhibits punctate irregularities overlying a thinned area of dehydrated corneal stroma. Treatment with frequent ocular lubrication or stress patching accelerates the healing process and restores stromal hydration. The orbital and conjunctival tissues surrounding the sclera additionally play a job in maintaining scleral hydration. This operate turns into especially evident during surgical procedures by which the conjunctiva and extraocular muscles are removed from the scleral surface. Removal of the perilimbal conjunctiva and interference with the wetting effect of the tear film (as after excision of a pterygium using the bare sclera technique) could cause the underlying sclera to turn into markedly thinned and translucent, forming a scleral delle. Limbal Stem Cell Deficiency the ocular surface consists of permanently renewing populations of epithelial cells.
Order diltiazem 60 mg otcThis setup supplies direct illumination 911 treatment for hair cheap 60 mg diltiazem amex, and purposeful shifting of alignment allows for oblique illumination symptoms uti in women cheap diltiazem 60mg without a prescription. Direct Illumination Methods Diffuse illumination With diffuse illumination symptoms whiplash buy cheap diltiazem 60 mg on line, the light beam is broadened medicine nobel prize 2016 order diltiazem 180 mg on line, lowered in depth, and directed on the eye from an oblique angle. Swinging the illuminator arm to produce highlights and shadows can improve the visibility of raised lesions of the ocular surface and iris. Focal illumination With focal illumination, the sunshine and the microscope are targeted on the same spot, and the slit aperture is adjusted from wide to narrow. Broad-beam illumination, utilizing a slit width of around three mm, is perfect to visualize eyelid lesions as nicely as the corneal opacities seen in dystrophies or scarring. The examiner can use a very narrow slit beam to assist identify refractive index differences in clear structures as light rays move by way of the cornea, anterior chamber, and lens. The examiner can also scale back the peak of a narrow beam to decide the presence and amount of cell and flare within the anterior chamber. Specular reflection Specular reflections are normal light reflexes bouncing off a surface. An instance is the intense spherical or oval spot seen reflected from the ocular floor in a typical flash photograph of an eye. However, the clarity and sharpness of those reflections from the tear movie give clues to the condition of the underlying tissue. Following are the steps for examining the corneal endothelium with specular reflection: 1. Begin by setting the slit-beam arm at an angle of 60� from the viewing arm and utilizing a brief slit or zero. Use the joystick to move the biomicroscope barely ahead to have the ability to focus the endothelial reflex. A setting of �25 to �40 is usually needed to acquire a clear view of the endothelial mosaic. Cell density and morphology are noted; guttae and keratic precipitates appear as nonreflective dark areas. Indirect Illumination Methods Proximal illumination Turning a knob on the illumination arm slightly decenters the light beam from its isocentric position, causing the sunshine beam and the microscope to be centered at different however adjacent spots. This method, proximal illumination, highlights an existing opacity in opposition to deeper tissue layers and permits the examiner to see small irregularities that have a refractive index similar to that of their surroundings. Moving the light beam forwards and backwards in small oscillations can help the examiner detect small 3-dimensional lesions such as a corneal international body. Reflective opacities stand out in opposition to the darkish field, whereas areas of lowered light transmission within the cornea are seen as shades of grey. Retroillumination Retroillumination can be used to study more than one space of the attention. Retroillumination from the iris is performed by displacing the beam tangentially whereas examining the cornea. Through observing the zone between the light and dark backgrounds, the examiner can detect subtle corneal abnormalities. Clinical Use the slit-lamp examination ought to be done in an orderly fashion, starting with direct illumination of the eyelids (margin, meibomian glands, and eyelashes), conjunctiva, and sclera. A broad beam illuminates the cornea and overlying tear movie in the optical section. The examiner estimates the height of the tear meniscus and appears for mucin cells and different particles in the tear movie. Discrete lesions are measured with a slit-beam micrometer or an eyepiece reticule. Direct, slit, and retroillumination methods are used to determine abnormalities of the iris and lens. The examiner actively controls the sunshine beam with a quantity of illumination strategies to sweep throughout the attention, using shadows and reflections to deliver out particulars. Having the patient blink can also help the examiner distinguish adjustments of the ocular floor from tiny opacities floating within the tear film. After initial low-power screening, a lot of the slit-lamp examination is carried out utilizing larger magnifications. Except for the anterior vitreous humor, deeper and peripheral intraocular buildings require special lenses. A contact lens allows examination of the intermediate and posterior portions of the eye and is often combined with angled mirrors and prisms for gonioscopy and peripheral fundus examination. Fluorescein is most commonly used for applanation tonometry and analysis of the tear film, including filaments. Fluorescein detects disruption of intercellular junctions and can stain punctate and macroulcerative epithelial defects (positive staining) corresponding to herpetic dendritic lesions or dysplastic epithelium. It also can highlight nonstaining lesions that project by way of the tear movie (negative staining), such as basement membrane dystrophy or Thygeson superficial punctate keratitis. Fluorescein that collects in an epithelial defect will diffuse into the corneal stroma and trigger a green flare in the anterior chamber. Pooling of the dye due to an indentation or thinning of the cornea must be distinguished from actual staining. In the dye disappearance check, the tear meniscus is observed for the disappearance of fluorescein. The Seidel check is used to detect seepage of aqueous humor by way of a corneal perforation. Rose Bengal and Lissamine Green Rose bengal and lissamine green (both available as a 1% resolution or in impregnated strips) are other watersoluble dyes. These dyes are routinely used for evaluating tear-deficiency states and for detecting and assessing various epithelial lesions, such as the extent of corneal intraepithelial neoplasia. To reduce irritation to the cornea through the test, a skinny filterpaper strip (5 mm wide, 30 mm long) is positioned at the junction of the center and lateral thirds of the decrease eyelid, with 5 mm of the paper folded inside the inferior cul-de-sac and the remaining 25 mm of paper projecting over the lower eyelid. The Schirmer I take a look at, which is similar to the basic secretion take a look at however is done without topical anesthetic, measures primary and reflex tearing mixed. Using decrease cutoff measurements will increase the specificity of those tests however decreases their sensitivity. However, after the filter-paper strips have been inserted into the inferior fornices, a cottontipped applicator is used to irritate the nasal mucosa. Wetting of lower than 15 mm after 2 minutes is according to a defect in reflex secretion. An different to traditional Schirmer strips is the phenol red�impregnated cotton thread test, which permits for faster assessment of tear secretion but has not been totally validated. Concentrated fluorescein on the sting of the aqueous rivulet (Seidel test) signifies an lively move of fluid from a leaking anterior chamber. As our understanding of the tear film has increased, commercial assays to measure its various components have been developed.
Diltiazem: 180 mg, 60 mg
Order 60mg diltiazem free shippingMetastatic lesions to the uveal tract medications 500 mg purchase diltiazem 60mg overnight delivery, orbit treatment 2 stroke effective 60 mg diltiazem, or paranasal sinuses can prolong into the conjunctiva medicine wheel native american order diltiazem 180mg without a prescription. Developmental Anomalies of the Globe and Sclera Cryptophthalmos Cryptophthalmos medicine website purchase 180mg diltiazem, or "hidden eye," is a rare, often bilateral situation during which the eyelids and related buildings of the brows and lashes fail to type (ablepharon). Associated ocular findings embrace corneal and conjunctival dermoid, absence of the lacrimal glands and canaliculi. Pseudocryptophthalmos occurs when the eyelids and associated structures form but fail to separate (ankyloblepharon). Cryptophthalmos happens in each an isolated and a recessive syndromic type as Fraser syndrome. Patients with this syndrome could have a combination of acrofacial and urogenital malformations with or with out cryptophthalmos. B, Incomplete cryptophthalmos of cosmesis or relief of ache from absolute glaucoma. Pseudocryptophthalmos may profit from fornix reconstruction utilizing buccal mucosal and amniotic membrane grafts, with eyelid reconstruction to defend the corneas. There is commonly an related cystic outpouching of the posteroinferior sclera, probably due to a failure of the fetal fissure to close properly, and colobomatous defects of the iris, ciliary physique, uvea, and optic nerve are sometimes current. Most instances of nonsyndromic microphthalmos are sporadic, although autosomal dominant, autosomal recessive, and X-linked forms have been reported. Systemic associations are numerous, together with mental disability and dwarfism. Associated conditions ought to be sought and managed appropriately, and genetic counseling must be thought of. Localization of a novel gene for congenital nonsyndromic easy microphthalmia to chromosome 2q11-14. Nanophthalmos Nanophthalmos is characterised by a small, functional eye with comparatively regular internal group and proportions. Patients have a excessive degree of hyperopia (7�15 diopters [D]) because of a short axial length (15�20 mm), and so they also have a excessive lens-to-eye volume ratio that can result in crowding of the anterior segment and angle-closure glaucoma. In addition, these patients have thickened sclera, steep corneal curvature, slender palpebral fissures, and crowded anterior segments associated with angle-closure glaucoma. Choroidal effusions or hemorrhage has been incessantly encountered during anterior segment surgery. Nanophthalmos may be sporadic or hereditary, and both autosomal dominant and autosomal recessive inheritance patterns have been reported. One gene locus for the autosomal dominant kind has been mapped to chromosome arm 11p. Laser iridotomy, typically combined with peripheral laser iridoplasty, could additionally be effective therapy of the angle-closure part. Cataract surgical procedure may be complicated by uveal effusion or hemorrhage and exudative retinal detachment, although advances in small-incision surgical procedure have lowered the frequency of these problems. Phacoemulsification and intraocular lens implantation in nanophthalmic eyes: report of a medium-size collection. Blue Sclera the striking clinical image of blue sclera is expounded to generalized scleral thinning, with increased visibility of the underlying uvea. This anomaly have to be distinguished from the slate-gray appearance of ocular melanosis bulbi and from acquired causes of scleral thinning corresponding to rheumatoid arthritis or staining from minocycline remedy. Osteogenesis imperfecta kind I is a dominantly inherited generalized connective tissue disorder characterized mainly by bone fragility, in addition to blue sclerae. These syndromes might share comparable manifestations of fractures from minor trauma in childhood, kyphoscoliosis, joint extensibility, and elastic skin. Postmenopausal girls should have interaction in a long-term physical therapy program to strengthen the paraspinal muscular tissues. Estrogen and progesterone substitute and adequate calcium and vitamin D intake are indicated. Developmental Anomalies of the Anterior Segment See Table 9-1 for a abstract of developmental anomalies of the anterior section. Anomalies of Size and Shape of the Cornea Microcornea Microcornea refers to a transparent cornea of normal thickness whose diameter is lower than 10 mm (or <9 mm in a newborn). If the complete eye is small and malformed, the time period microphthalmos is utilized in distinction to nanophthalmos, during which the eye is small but in any other case relatively regular. The trigger is unknown and may be related to fetal arrest of development of the cornea in the fifth month. Alternatively, it could be associated to overgrowth of the anterior tips of the optic cup, which leaves much less space for the cornea to develop. Microcornea could also be transmitted as an autosomal dominant (most commonly) or recessive trait with equal intercourse predilection. Because their corneas are relatively flat, patients with microcornea are normally hyperopic and have a higher incidence of angle-closure glaucoma. Significant systemic associations include myotonic dystrophy, fetal alcohol syndrome, achondroplasia, and Ehlers-Danlos syndrome. If microcornea occurs as an isolated finding, the affected person has an excellent visual prognosis with spectacles to deal with the hyperopia ensuing from the flat cornea. Megalocornea Megalocornea is a bilateral, nonprogressive corneal enlargement with an X-linked recessive inheritance pattern (see Table 9-1). Males are more usually affected, however heterozygous ladies could demonstrate a slight improve in corneal diameter. The etiology could also be associated to failure of the optic cup to develop and of its anterior tricks to close, leaving a larger area for the cornea to fill. Alternatively, megalocornea might characterize arrested buphthalmos and exaggerated progress of the cornea in relation to the remainder of the eye. An abnormality in collagen production is suggested by the association of megalocornea with systemic problems of collagen synthesis (eg, Marfan syndrome). Megalocornea could additionally be associated with iris translucency (diaphany), miosis, goniodysgenesis, cataract, ectopia lentis, arcus juvenilis, and glaucoma (but not congenital glaucoma). Congenital glaucoma must be ruled out by intraocular strain measurement and careful biomicroscopy. Ultrasonography could also be of worth in figuring out the short vitreous length, deep lens and iris position, and regular axial length that distinguish megalocornea from buphthalmos attributable to congenital glaucoma. Care must be taken throughout cataract surgery to implant the intraocular lens into the lens capsular bag. Standard-sized posterior chamber lenses are sometimes too short to be fixated in the ciliary sulcus, and anterior chamber lenses are similarly problematic in the enlarged anterior chamber. Cornea plana Cornea plana refers to a flat cornea, the place the radius of curvature is lower than forty three D, and readings of 30�35 D are common. These proteins are thought to play an essential function within the common spacing of corneal collagen fibrils. Other related ocular or systemic abnormalities embrace cataracts, anterior and posterior colobomas, and EhlersDanlos syndrome. Cornea plana often produces hyperopia, but any type of refractive error could additionally be present because of variations in globe size. Angle-closure glaucoma occurs due to a morphologically shallow anterior chamber, and open-angle glaucoma happens due to angle abnormalities.
References - Masso Gonzalez EL, Patrignani P, Tacconelli S, Garcia Rodriguez LA. Variability among nonsteroidal antiinflammatory drugs in risk of upper gastrointestinal bleeding. Arthrit Rheum 2010;62:1592.
- Dake MD, Kato N, Mitchell RS, et al: Endovascular stent graft placement for the treatment of acute aortic dissection, N Engl J Med 340:1546-1552, 1999.
- Calabro F, Sternberg CN: New drugs and new approaches for the treatment of metastatic urothelial cancer, World J Urol 20:158n166, 2002.
- Zettl A, deLeew R, Haralambieva E, Mueller-Hermelink H-K. Enteropathy-type T-cell lymphoma. Am J Clin Pathol 2007; 127:701.
- Gorback MS: Problems associated with the determination of pulmonary vascular resistance, J Clin Monit 6:118, 1990.
|