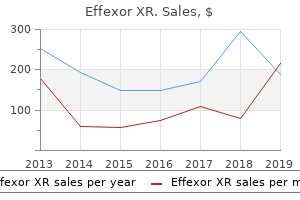
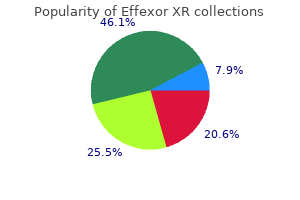
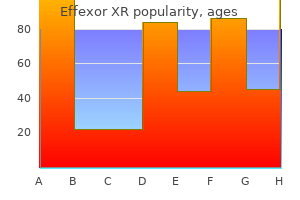
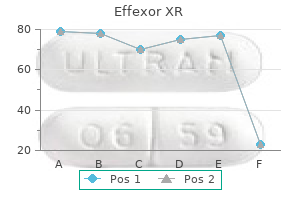
Effexor XR
G. Paul Dabrowski, M.D. - Assistant Professor of Surgery
- University of Pennsylvania
- Philadelphia, PA
Buy 75 mg effexor xr overnight deliveryKonwaler and associates (2) originally referred to as it "subcutaneous pseudosarcomatous fibromatosis anxiety symptoms for months buy effexor xr 75mg on line. Its prevalence within the orbital area was elucidated by Font and Zimmerman in 1966 (3) and subsequent reviews have expanded on its ophthalmic manifestations (4�20) anxiety symptoms jumpy buy 37.5 mg effexor xr. It may be more widespread than indicated in that report as a result of some circumstances are most likely misdiagnosed histopathologically as other spindle cell lesions anxiety free stress release formula discount 150 mg effexor xr mastercard. Survey of 1264 sufferers with orbital tumors and simulating lesions: the 2002 Montgomery Lecture anxiety heart rate best effexor xr 37.5 mg, half 1. Nodular fasciitis presenting as quickly enlarging episcleral mass in a 3-year-old. Immunohistologic and electron microscopical examine of nodular fasciitis of the orbit. Clinical Features Nodular fasciitis normally occurs in youngsters and has a somewhat speedy onset and development. Diagnostic Approaches the analysis of nodular fasciitis could be suspected on the premise of clinical findings, but is often made histopathologically after biopsy or surgical excision. With imaging studies, it exhibits features typical of different stable lots and has no distinctive findings. Pathology the histopathologic diagnosis of nodular fasciitis may be challenging, as a outcome of it could possibly simulate rhabdomyosarcoma or other soft tissue sarcomas (1�3). However, pathologists experienced with delicate tissue tumors often can make the analysis primarily based on characteristic light microscopic features. Mitotically active stellate or spindle-shaped fibroblasts are often organized in parallel bundles and lengthen in all directions, resembling cells in a tissue culture. Numerous newly formed parallel capillaries often ramify via the lesion, forming slitlike areas harking back to those seen in Kaposi sarcoma. With immunohistochemistry, nodular fasciitis reveals positive reactions against clean muscle actin and vimentin. With electron microscopy, one sees parallel bundles of actinlike filaments with fusiform densities (17). Management Because nodular fasciitis normally is well circumscribed and positioned in the anterior adnexal buildings, we suggest full surgical removal when attainable. Chapter 32 Orbital Fibrous Connective Tissue Tumors 619 Orbital Fibroma General Considerations Among the benign fibrous proliferations, fibroma is a difficult lesion to categorize (1). Clinical Features Fibroma within the orbital area normally seems as a palpable firm mass in the anterior orbit that produces proptosis or globe displacement. It can prolong anteriorly into the conjunctiva and seem as an irregular, yellow-white mass. Diagnostic Approaches There is little specific data on the diagnosis of orbital fibroma. Clinically and with imaging studies, it in all probability seems as a stable, anterior, yellow-white mass with irregular borders. Pathology Fibroma is composed of a paucicellular inhabitants of fibroblasts which are typically broadly separated by abundant collagen. The long, swish fascicles typical of fibroma and different pure fibroblastic tumors seem different on mild microscopy from the twisting storiform sample of the cells of fibrous histiocytoma. The absence of foci of irritation is useful in differentiating fibroma from sclerosing idiopathic orbital irritation, in which inflammatory cells can usually be detected regardless of large areas of fibrosis. Orbital fibromas are in all probability not radiosensitive, though it seems cheap to try radiotherapy in recurrent or unresectable circumstances that show progression and complications. Nodular fasciitis in a young boy presenting as a subcutaneous mass beneath lateral side of right upper eyelid, resembling a dermoid cyst. Magnetic resonance imaging on T2-weighted picture displaying the mass with solid inner appearance. Appearance of reddish agency mass uncovered at time of surgical procedure by a superotemporal eyelid crease strategy. However, everlasting section had been interpreted as nodular fasciitis by expert soft tissue pathologists. Orbital nodular fasciitis presenting as a subcutaneous mass behind decrease eyelid in a 2-year-old girl. Histopathology of nodular fasciitis demonstrating sheets of proliferating fibroblasts and chronic inflammatory cells. The terminology relating to these entities is complicated because they overlap clinically and histopathologically. The fibromatoses seem to symbolize intermediate lesions between the localized fibromas and the extra malignant fibrosarcomas. They can happen at any age and may be part of generalized fibromatosis or they are often solitary (myofibroma). The generalized type (fibromatosis and myofibromatosis) is commonly current at or shortly after delivery as multiple nodules within the dermis, muscle, viscera, and bone. Affected youngsters have a guarded prognosis and as many as 75% die with indicators of respiratory misery or diarrhea soon after delivery (1). There are rising numbers of such lesions being acknowledged in the orbital and eyelid area of infants, either in soft tissue or in orbital bones or periosteum (4�14). Myofibroma appears to have an excellent prognosis with an inclination to be self-limited and to remain secure or even regress after incisional biopsy. Results of immunohistochemistry are variable and controversial, but most cells stain positive for easy muscle actin. Ultrastructural studies suggest that the predominant cells are fibroblasts and myofibroblasts (1). Management the best management of suspected orbital myofibromatosis is surgical excision or generous incisional biopsy. After histopathologic affirmation, the affected person must be monitored periodically, but recurrence is unusual. Little is understood about the response to corticosteroids, chemotherapy, or irradiation, however these strategies can usually be withheld till absolutely essential. As mentioned, the solitary orbital kind generally has a very favorable prognosis, primarily based on published stories (6,9,14). Clinical Features the clinical features of orbital fibromatosis vary with whether or not the lesion is generalized or localized (8). The most typical presentation is a solitary orbital or subcutaneous mass (myofibroma) that produces proptosis and other signs and indicators of a solitary orbital tumor. Pathology Microscopically, myofibroblastic tumors are composed of spindle shaped to plump fibroblasts arranged in interlacing fascicles and embedded in a collagenous background matrix (desmoid appearance). They are fairly similar to different spindle cell Chapter 32 Orbital Fibrous Connective Tissue Tumors 623 Selected References 1. Coronal computed tomography in T2-weighted image with gadolinium enhancement, exhibiting the mildly enhancing superonasal mass. The tumor filled the entire orbit and ethmoid and prolonged into the cranial cavity of different sections.
Syndromes - Percutaneous (antegrade) technique involves a small surgical cut on the side of the body between the ribs and the hip.
- Low amounts of water in the body, most often while in the hospital.
- Baking powder
- How often do you experience muscle spasms?
- Hoarseness or change in voice
- Medication side effects
Buy generic effexor xr 37.5 mg on-lineIf the diagnosis is established histopathologically anxiety symptoms webmd discount 150mg effexor xr with visa, then corticosteroid-resistant circumstances could be treated with cytotoxic brokers or radiotherapy anxiety symptoms reddit generic 37.5 mg effexor xr with visa. Orbital exenteration not often turns into needed because of extreme fibrosis or ache There has been recent curiosity in the utilization of infliximab anxiety symptoms in cats 75mg effexor xr, an anti-tumor monoclonal antibody directed against tumor necrosis factor- (20 anxiety shortness of breath discount 37.5 mg effexor xr with mastercard,21). It was used primarily in recalcitrant instances of myositis after failure of ordinary treatments. More patients and longer follow-up are necessary to decide the efficacy of this method of therapy. Myositis can intently resemble thyroid-associated orbitopathy or metastatic carcinoma. Chapter 26 Inflammatory Lesions That Simulate Neoplasms 457 Selected References 1. Idiopathic orbital inflammation: distribution, scientific features, and treatment end result. Idiopathic inflammatory pseudotumor of the orbit and Tolosa-Hunt syndrome-are they the identical illness Combined central retinal artery and vein occlusion from orbital inflammatory pseudotumour. Treatment of recalcitrant idiopathic orbital inflammation (chronic orbital myositis) with infliximab. Proptosis, eyelid edema, and conjunctival hyperemia in a 48-year-old man with acute ocular ache and visual loss. Bilateral proptosis, worse on proper aspect, in a 57-year-old man with chronic, low-grade, bilateral ocular pain. Note the bilateral orbital lots involving the lacrimal glands, lateral rectus muscular tissues, and adjoining delicate tissues. Histopathologic examination of biopsy specimen confirmed the prognosis of sclerosing idiopathic inflammation. Elderly man with proper proptosis and edema of higher and lower eyelids, however no redness. Note marked enhancement of lateral rectus muscle and medial displacement of the optic nerve. Middle-aged lady with blepharoptosis and redness of the proper upper and decrease eyelids. Axial computed tomography showing diffuse, ill-defined inflammation of the delicate tissue of the left orbit. Proptosis and lateral displacement of the right eye in a 12year-old girl with eyelid edema and delicate ache. Appearance of identical baby shortly after initiating a course of oral corticosteroids, showing dramatic improvement in the inflammation. Chapter 26 Inflammatory Lesions That Simulate Neoplasms 461 Nonspecific Acute Orbital Myositis this is a variant of idiopathic nongranulomatous orbital inflammation that solely affects the extraocular muscular tissues, usually one specific muscle. Acute redness secondary to a mass in superior epibulbar tissues in an 8-year-old boy. Note that a suture has been positioned beneath the superior rectus and the uncovered mass appears to contain the muscle itself. Proptosis of the proper eye and blepharoptosis of right higher eyelid in a 34-year-old man. There was a dramatic scientific response with the inferior rectus muscle returning to normal measurement. It most frequently happens as a periostitis that may affect the bones in younger adults, causing a chronic cold abscess or a fistula (2). It also can occur as an isolated orbital or lacrimal gland granuloma derived from the bloodstream, or it may possibly prolong into the orbit from the adjacent nasal cavity or sinuses. In such circumstances, it turns into important within the differential diagnosis of orbital tumors. Polymerase chain response can be utilized to show amplification of the Mycobacterium tuberculosis genome (4). Management Treatment contains appropriate antituberculous therapy to which orbital involvement responds favorably (1�3). Detection of Mycobacterium tuberculosis by polymerase chain response in a case of orbital tuberculosis. Biopsy confirmed granulomatous inflammation and acid-fast organisms suitable with tuberculosis or atypical mycobacteria. Facial view of an aged African-American lady showing upward displacement of left eye and no considerable inflammatory indicators. Biopsy demonstrated acid-fast organisms and the affected person responded to tuberculosis medications. In rare instances, sure species of mucormycosis have been reported to develop in immunocompetent individuals (7). There is a quite fast onset of orbital irritation with proptosis and oculomotor palsies. A characteristic black eschar develops in the concerned areas, notably the periorbital pores and skin, owing to necrosis from vascular occlusion by the organisms. Diagnostic Approaches the prognosis may be made by scientific suspicion in these medical settings and an orbital biopsy of the most accessible tissue. Pathology Histopathologically, the organism is a big (30�50 micron) nonseptate, branching hypha that stains with hematoxylin and eosin, but is much more evident with periodic acid-Schiff and specific fungal stains similar to Gomori methenamine silver stain. The organisms generally tend to invade the orbital blood vessels resulting in necrosis. Management the administration of orbital mucormycosis is considerably controversial and consists of extensive surgical debridement and acceptable antifungal brokers like amphotericin B systemically and regionally (intraconal injection) (5). Initiation of treatment is pressing as a result of the disease is incessantly deadly owing to invasion by way of the orbital tissue and into the intracranial cavity. It is caused by any of a quantity of species of the genus Aspergillus, which are opportunistic organisms that usually reside within the oropharynx and sinuses, notably in the ethmoid and sphenoid sinuses. Unlike mucormycosis, which seems in debilitated patients, orbital aspergillosis usually develops in otherwise healthy individuals (1). Hence, eyelid-sparing orbital exenteration is sometimes advocated for posterior orbital lesions, regardless of the functional standing of the eye (7,20). For anterior orbital lesions, wide debridement without exenteration may be justified (20). The medical manifestations could also be very similar to these of mucormycosis with the exception that aspergillosis normally has a extra insidious onset and sluggish course. The an infection may turn out to be organized right into a quite defined mass called an "aspergilloma. Diagnostic Approaches Computed tomography typically exhibits a diffuse mass in the sinuses with secondary unilateral or bilateral orbital extension. The analysis can be suspected on the premise of the medical findings however nice needle aspiration or incisional biopsy may be employed to set up a definitive diagnosis. The organism is a septate hypha kind branching at a characteristic 45-degree angle. Management the administration of orbital aspergillosis is wide surgical excision of the involved sinuses and orbital tissues, mixed with amphotericin B or itraconazole in applicable doses (17).
Buy effexor xr 75mg on-lineFor example anxiety lost night generic effexor xr 37.5mg on line, 7888 cholecystectomies had been carried out in Utah in 2005; 96% of those operations were laparoscopic cholecystectomies anxiety symptoms of going crazy order effexor xr 37.5mg mastercard, and 4% had been open procedures anxiety tumblr order effexor xr 150 mg with visa. A review of the National Hospital Discharge Database from 1997 to 2006 confirmed that 12% of Results the chance of open cholecystectomy has declined over the years anxiety chest pain buy cheap effexor xr 37.5mg. The mortality fee is significantly lower in sufferers operated on electively for biliary ache, with a median of less than zero. In a report of the complete Danish expertise with cholecystectomy from 1977 to 1981, sufferers beneath 50 years of age had a danger of demise of 0. Of 11,808 sufferers who underwent cholecystectomy at the New York Hospital-Cornell Medical Center between 1932 and 1978, the chance of dying from elective cholecystectomy for persistent cholecystitis was zero. Likewise, the morbidity fee, imply length of hospital stay, and common hospital expenses were considerably greater within the older sufferers than within the youthful group. Most mortality following cholecystectomy is said to cardiac disease, significantly myocardial infarction. In a big survey of 28,621 sufferers who underwent cholecystectomy in the Nineteen Sixties, complications occurred in four. Complications associated particularly to cholecystectomy include bile leaks, bile duct damage, and acute pancreatitis. Of these issues, bile duct harm is essentially the most severe and often requires endoscopic remedy and, in some cases, difficult and technically tough surgical repair. Alternatively, bile duct harm can lead to benign biliary stricture formation and bile duct obstruction with secondary biliary cirrhosis and liver failure. Historically, laparoscopic cholecystectomy was an outgrowth of diagnostic laparoscopy and the early efforts of gynecologists at operative laparoscopy. The growth of laparoscopic cholecystectomy was predicated on technical advances in miniaturized video cameras and different specialised tools. Sequential compression stockings are used to cut back the risk of decrease extremity thromboembolism. To view the abdominal contents and provide room for instruments, a space is developed by inducing a pneumoperitoneum Laparoscopic Cholecystectomy After the first stories in the late Nineteen Eighties, laparoscopic cholecystectomy quickly gained acceptance as the strategy of choice for the administration of the affected person with biliary pain and problems of gallstones. Pneumoperitoneum is achieved by both a closed method by which a Veress needle is inserted into the peritoneum by way of a small incision, adopted by placement of an operating trocar, or by a direct, open technique during which the operating trocar is placed instantly into the stomach underneath direct visualization through a small incision. After the pneumoperitoneum has been established, a trocar is positioned at the umbilicus and a laparoscope is introduced. Three extra trocars are positioned within the upper stomach underneath direct vision for inserting operating devices and retractors. The present strategy of laparoscopic cholecystectomy is greatest described as "the important view of safety" method,sixty two as summarized in. In this method, the whole hepatocystic triangle is dissected, exposing the cystic duct and artery, infundibulum of the gallbladder, and junction of the gallbladder and cystic duct, before a cholangiogram is performed or the cystic duct and artery are divided. The assistant retracts the gallbladder fundus cephalad, anterior to the liver, and the infundibulum laterally. The surgeon, working by way of the epigastric port, identifies and dissects the cystic duct and artery circumferentially. Special care must be taken to identify the junction of the cystic duct and gallbladder, to be positive that the bile duct has not been isolated inadvertently. If the cholangiogram exhibits regular anatomy and no evidence of choledocholithiasis, the cholangiocatheter is removed and the cystic duct and artery are divided between small steel clips. The gallbladder is then dissected out of the liver bed and delivered via the umbilical incision, normally with a specimen retrieval bag. Care is taken to keep away from perforation of the gallbladder during its dissection from the liver as a result of the spillage of gallstones and bile has been shown to increase the danger of postoperative fever and intra-abdominal abscess formation. In the 2010s, laparoscopic cholecystectomy has been carried out by some surgeons using a single-incision laparoscopic surgical procedure strategy in which the operating surgeon introduces the laparoscope and surgical instruments into the abdomen via a single operating port positioned on the umbilicus. This technique has the benefit of improved cosmetics over the standard 4-port laparoscopic strategy. The single-incision laparoscopic surgical procedure process has not gained wide acceptance due to longer operating times, larger value, a higher rate of wound issues and hernias, and, probably, a higher fee of bile duct harm. Large population studies from Australia and Sweden have demonstrated the importance of routine intraoperative cholangiography in lowering the frequency of major bile duct injuries. Despite these observations in favor of routine cholangiography, the low frequency of unsuspected bile duct stones and low fee of bile duct injury function the idea for many surgeons adopting a selective method to utilizing cholangiography. Cholangiography is completed when the historical past is suggestive of potential bile duct stones Results Several large collection have described experiences with laparoscopic cholecystectomy (Table 66. Major morbidity occurred in roughly 5% of patients, and bile duct injuries occurred in 0. Operating time ranged from 1 to 2 hours, with most patients undergoing same-day surgery and outpatient surgical procedure in elective circumstances. Patient enthusiasm for the laparoscopic method and the fast acceptance of the process by surgeons have made direct, managed comparison of the 2 procedures troublesome. Population research have shown a considerable decline in cholecystectomy-related mortality rates following the introduction of the laparoscopic method (Table sixty six. First, regional research have demonstrated a lower in the rate of bile duct injury as overall experience with laparoscopic cholecystectomy has increased. As general experience has elevated, the rate of bile duct harm for laparoscopic cholecystectomy has approximated that seen with open cholecystectomy. Second, the variety of patients with bile duct damage treated at tertiary referral medical centers has declined since the early days of laparoscopic Rationale for Cholangiography Cholangiography throughout laparoscopic cholecystectomy has 2 major purposes. In the era earlier than laparoscopic cholecystectomy, the value of routine cholangiography during cholecystectomy was debated, with some surgeons arguing in favor of its selective use. Routine cholangiography has been criticized due to its comparatively low yield, failure to determine all retained stones, occasional false-positive outcomes, price, and risk. Nevertheless, 8% to 16% of all patients with cholelithiasis harbor bile duct stones. Routine use of operative cholangiography detects unsuspected bile duct stones in about 5% of patients who endure cholecystectomy and detects anatomic ductal abnormalities in 12%. B, Cephalad retraction of the fundus towards the proper shoulder exposes the infundibulum of the gallbladder. C, Retraction of the infundibulum toward the proper lower stomach quadrant opens the hepatocystic triangle, which is the world bordered by the cystic duct, gallbladder edge, and liver edge. D, Division of the peritoneum overlying the anterior and posterior elements of the hepatocystic triangle exposes "the crucial view of security. The dramatic decline in danger as experience is gained has been attributed to a "studying curve. In an outlined well being maintenance group population in Pennsylvania, the speed of cholecystectomy elevated from 1. Similarly, statewide knowledge from Maryland confirmed that the speed of cholecystectomy rose from 1.
Discount 150 mg effexor xr mastercardThe differential diagnosis consists of basal cell carcinoma anxiety symptoms or heart problems order 150mg effexor xr fast delivery, squamous cell carcinoma anxiety cat buy effexor xr 37.5 mg visa, keratoacanthoma anxiety level quiz order 75mg effexor xr with visa, and different sweat gland and hair follicle neoplasms anxiety 025 cheap effexor xr 37.5mg with amex. Pathology Histopathologically, syringocystadenoma papilliferum is a papillomatous lesion with keratinizing epithelial-lined ducts that open on the skin surface. The cells lining the ducts exhibit decapitation secretion, characteristic of apocrine cells, and attribute papillary projections that extend into the ductlike spaces. Another attribute function is infiltration of continual inflammatory cells, principally plasma cells, in the connective tissue pores of the papillae. Electron microscopic findings assist the apocrine gland origin of this lesion (3). Management the management of suspected syringocystadenoma papilliferum is complete surgical resection. Syringoadenoma papilliferum-lesions with and with out naevus sebaceus and basal cell carcinoma. Syringocystadenoma papilliferum presenting on the higher eyelid of a 31-year-old man. In a sequence of 188 chondroid syringomas, 7 arose in the eyebrow and 1 within the eyelid (1). Like related tumors of the salivary and lacrimal glands, they sometimes endure malignant transformation into pleomorphic adenocarcinoma (malignant mixed tumor) (5). Mandeville and associates (12) reviewed 9 cases with eyelid involvement and provided a evaluation of the literature. Cutaneous benign mixed tumor (chondroid syringoma) of the eyelid: scientific presentation and administration. Clinical Features Clinically, eyelid pleomorphic adenoma seems as a slowly enlarging nontender solitary or multilobulated subcutaneous mass that varies in size from four to 17 mm at the time of clinical diagnosis. In a collaborative report of nine sufferers with ocular adnexal lesions, four have been at the eyelid margin, three have been within the sub-eyebrow space of the higher eyelid, and two within the central eyelids (12). None of the lesions was associated with significant modifications of the overlying epidermis, though one lesion confirmed overlying pigmentation. This tumor has no particular scientific options and could also be inconceivable to differentiate clinically from other subcutaneous eyelid lesions. Pathology Histopathologically, the eyelid tumor has options similar to pleomorphic adenoma of the lacrimal gland. The glandular epithelial cells kind islands or cords in a mucoid stroma, which regularly shows chondroid metaplasia. The epithelial cells type a double layer, with the inner layer being secretory and the outer layer myoepithelial in nature (2). Management the management of pleomorphic adenoma of the eyelid is full surgical removing. Although eyelid lesions hardly ever bear malignant change, benign mixed tumors within the extremities or again can metastasize domestically and hematogenously (7). Histopathology of pleomorphic adenoma of eyelid, displaying glandular, mesenchymal and chondroid components. The three most often reported malignant eyelid tumors of sweat gland origin are mucinous sweat gland adenocarcinoma, eccrine sweat gland adenocarcinoma, and apocrine adenocarcinoma of the glands of Moll (1�3). Each type has overlapping medical features, and the analysis is often not suspected clinically. Furthermore, they could be tough to affirm histopathologically, as a outcome of they may be much like other main malignancies and to metastatic adenocarcinoma to the eyelid. Mucinous sweat gland adenocarcinoma arises from the epidermal cells of eccrine sweat glands and is characterised by a high content of mucin (1�20). Eccrine sweat gland adenocarcinoma (also called "infiltrating signet ring carcinoma") is an uncommon variant of adenocarcinoma of sweat gland origin that resembles mammary carcinoma histopathologically (5,21�23). Apocrine adenocarcinoma can happen in areas of the pores and skin where apocrine glands are most dense, such because the perianal area, axilla, and the external auditory canal (ceruminous glands). Pathology Mucinous sweat gland adenocarcinoma is characterized by lobules and cords of epithelial cells that float in pools of mucin, separated by thin fibrovascular septa (1�19). Less generally, the mucin could additionally be largely confined to the epithelial cells and not in the extracellular spaces. The epithelial cells can sometimes type ductules or acini, imparting an "adenocystic appearance. In some cells, a big vacuole displaces the nucleus, producing a attribute signet ring look. These cells are said to be indistinguishable from these of the histiocytoid mammary carcinoma metastatic to the eyelid. Apocrine adenocarcinoma is characterised by a glandular association of enormous cells with ample eosinophilic cytoplasm and proof of decapitation secretion. They are equivalent to the apocrine adenocarcinoma that occurs in the axilla (26�31). Clinical Features Each kind of malignant sweat gland neoplasm begins as a small nodule that grows slowly and, if not controlled domestically, has a capability to recur regionally and metastasize to region lymph nodes. Mucinous sweat gland adenocarcinoma develops in the head and neck region in 75% and in the periorbital area in 40% of instances. Although most info is derived from case reports, Wright and Font (5) reported 21 instances and outlined the salient scientific and histopathologic options of mucinous sweat gland adenocarcinoma. It is extra common within the decrease eyelid and appears as a pink to blue, elevated nodule that could be strong or cystic. Eccrine sweat gland adenocarcinoma seems as a nodular, indurated subcutaneous mass that has an ill-defined, diffuse, infiltrating margin, and a blue to pink color (21�25). Porocarcinoma is a variant of sweat gland carcinoma that arise from the eccrine secretory apparatus (17). In the eyelid space, apocrine adenocarcinoma develops from the apocrine glands of Moll near the bottom of the cilia. Management the best management of a malignant sweat gland neoplasm is extensive surgical excision with frozen section or Mohs surgical procedure to monitor the margins, similar to the administration of basal cell carcinoma and different primary malignant eyelid tumors (1�5). However, incompletely excised lesions have a tendency towards local recurrence, regional lymph node metastasis and, not often, systemic metastasis. A clinicopathologic study of 21 instances with histochemical and electron microscopic observations. Primary mucinous sweat gland carcinoma of the eyelid simulating metastatic carcinoma. Eccrine duct carcinoma of the eyelid mimicking meibomian carcinoma: clinicopathological study of a case. Signet ring carcinoma of the eccrine sweat gland within the eyelid, treated by radiotherapy alone. Histiocytoid variant of eccrine sweat gland carcinoma of the eyelid and orbit: report of 5 instances. Carcinoma of the apocrine glands on the base of eyelashes; a case report and discussion of histological diagnostic criteria.
Cheap 150mg effexor xr visaThe prognosis of biliary rhabdosarcomas is sweet anxiety 5 htp buy effexor xr 75mg without a prescription, with reported 5-year survival charges of up to anxiety jaw pain purchase 37.5 mg effexor xr visa 78% anxiety 5 steps buy 75 mg effexor xr otc. Guidelines for the management of biliary tract and ampullary carcinomas: surgical remedy anxiety symptoms 35 order effexor xr 150mg visa. Genomic and genetic characterization of cholangiocarcinoma identifies therapeutic targets for tyrosine kinase inhibitors. Prognostic elements after surgical resection for intrahepatic, hilar, and distal cholangiocarcinoma. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma: a hospital-based casecontrol examine. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma in the United States: a population-based case-control research. Intrahepatic peripheral cholangiocarcinoma: mode of unfold and choice of surgical therapy. Cholangiocarcinoma with intraductal tubular progress pattern versus intraductal papillary growth sample. Intrahepatic cholangiocarcinoma arising in cirrhotic liver frequently expressed p63-positive basal/stem-cell phenotype. Exome sequencing identifies distinct mutational patterns in liver fluke-related and non-infection-related bile duct cancers. Fibroblast progress factor receptor 2 tyrosine kinase fusions outline a unique molecular subtype of cholangiocarcinoma. Fibroblast progress issue receptor 2 translocations in intrahepatic cholangiocarcinoma. New routes to targeted therapy of intrahepatic cholangiocarcinomas revealed by next-generation sequencing. Typical and atypical imaging findings of intrahepatic cholangiocarcinoma using gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid-enhanced magnetic resonance imaging. Diagnostic accuracy of fluorine-18-fluorodeoxyglucose positron emission tomography within the analysis of the first tumor in patients with cholangiocarcinoma: a meta-analysis. Radiological staging in sufferers with hilar cholangiocarcinoma: a scientific evaluate and meta-analysis. Positron emission tomography with [(18)F]fluoro-2-deoxy-D-glucose for diagnosis and staging of bile duct cancer. Advanced cytologic strategies for the detection of malignant pancreatobiliary strictures. Adjuvant remedy in the treatment of biliary tract cancer: a scientific evaluation and meta-analysis. Late growth of bile duct cancer in sufferers who had biliary-enteric drainage for benign disease: a follow-up study of more than 1,000 sufferers. Cetuximab, gemcitabine, and oxaliplatin in sufferers with unresectable advanced or metastatic biliary tract most cancers: a section 2 study. Outcome in patients with bifurcation tumors who bear unilateral versus bilateral hepatic duct drainage. Prediction of drainage effectiveness during endoscopic stenting of malignant hilar strictures: the role of liver volume evaluation. Rate of bilirubin regression after stenting in malignant biliary obstruction for the initiation of chemotherapy: how soon should we repeat endoscopic retrograde cholangiopancreatography Brachytherapy and percutaneous stenting within the remedy of cholangiocarcinoma: a prospective randomised research. Prospective examine of the effectiveness of percutaneous transhepatic photodynamic remedy for advanced bile duct cancer and the function of intraductal ultrasonography in response assessment. Trend evaluation and survival of primary gallbladder most cancers within the United States: a 1973-2009 population-based study. Biliary tract cancers: epidemiology, molecular pathogenesis and genetic risk associations. Is gallbladder cancer decreasing in view of accelerating laparoscopic cholecystectomy Number and measurement of stones in sufferers with asymptomatic and symptomatic gallstones and gallbladder carcinoma: a prospective study of 592 circumstances. Risk components for biliary tract and ampullary carcinomas and prophylactic surgery for these elements. Trans-peritoneal fine needle aspiration biopsy of hilar cholangiocarcinoma is associated with illness dissemination. Diagnostic yield of bile duct brushings for cholangiocarcinoma in major sclerosing cholangitis: a scientific evaluation and meta-analysis. Staging, resectability, and end result in 225 patients with hilar cholangiocarcinoma. Neither neoadjuvant nor adjuvant remedy will increase survival after biliary tract cancer resection with wide unfavorable margins. Surgical approach for long-term survival of sufferers with intrahepatic cholangiocarcinoma: a multi-institutional analysis of 434 sufferers. Liver transplantation for "very early" intrahepatic cholangiocarcinoma: worldwide retrospective examine supporting a potential assessment. Transarterial chemoembolization within the therapy of sufferers with unresectable cholangiocarcinoma: outcomes and prognostic factors governing therapy success. Yttrium-90 radioembolization for unresectable standard-chemorefractory intrahepatic cholangiocarcinoma: survival, efficacy, and security study. Improvement in perioperative and long-term outcome after surgical treatment of hilar cholangiocarcinoma: results of an Italian multicenter evaluation of 440 sufferers. Pancreaticobiliary maljunction and carcinogenesis to biliary and pancreatic malignancy. Prevalence and risk elements for gallbladder neoplasia in patients with major sclerosing cholangitis: evidence for a metaplasia-dysplasia-carcinoma sequence. High danger of gallbladder carcinoma in aged sufferers with segmental adenomyomatosis of the gallbladder. Preneoplastic lesions and gallbladder most cancers: an estimate of the period required for progression. Clinical significance of p53 protein in gall bladder carcinoma and its precursor lesions. Whole-exome and focused gene sequencing of gallbladder carcinoma identifies recurrent mutations in the ErbB pathway. Tumor traits and survival evaluation of incidental versus suspected gallbladder carcinoma. Differential prognosis of gallbladder lots utilizing color Doppler ultrasonography. Fourteen 12 months surgical experience of gallbladder cancer: validity of curative resection affecting survival. A 21-year analysis of stage I gallbladder carcinoma: is cholecystectomy alone enough Surgical treatment of patients with T2 gallbladder carcinoma invading the subserosal layer.
Paprika (Capsicum). Effexor XR. - Are there safety concerns?
- Dosing considerations for Capsicum.
- What is Capsicum?
- Back pain.
- Reducing painful tender points in people with fibromyalgia when applied to the skin.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96908
Effexor xr 37.5 mg otcLocalized corneal epitheliectomy being carried out with a small scalpel utilizing a mild anxiety symptoms skipped heart beats buy 37.5 mg effexor xr free shipping, managed scrolling technique anxiety jealousy discount effexor xr 37.5 mg free shipping. The corneal epithelium is gently everted and laid on the floor of the primary tumor at and behind the limbus anxiety 4 year old boy buy cheap effexor xr 75 mg on line. A superficial scleral groove has been made around the tumor base anxiety 6 months after quitting smoking order effexor xr 150mg on-line, which is being removed by dissecting a skinny layer of superficial sclera immediately beneath the tumor and just posterior to the limbus. The tumor has been removed and placed flatly on a bit of sterile cardboard on the operating table. The same principle applies to different conjunctival and iris lesions that are removed surgically. After the tumor has been removed and placed in fixative, double freeze thaw cryotherapy is utilized from beneath the conjunctiva in an outward path. Large drawing of extensive main acquired melanosis, probably giving rise to melanoma. Diffuse conjunctival main acquired melanosis in one other case giving rise to melanoma that may be eliminated by the methods proven in steps under. Alcohol being applied with a cotton-tipped applicator to treat peripheral corneal invasion by major acquired melanosis. Note several further small nodules of pigmentation in different areas of the conjunctiva. All nodular pigmented areas have been eliminated by a circular conjunctival excision carried all the method down to bare sclera. A small staging map biopsy is being taken from the bulbar conjunctiva near the fornix. Such a biopsy is generally taken in all 4 quadrants even though the conjunctiva seems to be clinically regular in that area. Clinically, the lesion resembles a pingueculum however proved histopathologically to be in situ squamous cell carcinoma. Melanoma of bulbar conjunctiva with peripheral corneal invasion in a 45-year-old woman. Melanoma arising from major acquired melanosis and secondarily invading the cornea. Appearance of same space 6 months after removal and cryotherapy, showing excellent outcome with no tumor recurrence. Chapter 25 Surgical Management of Conjunctival Tumors 443 Treatment of Conjunctival Malignancies With Topical Chemotherapy and Interferon Topical chemotherapy can sometimes be used as ancillary remedy for conjunctival malignancies, notably squamous cell carcinoma, primary acquired melanosis, and superficial melanoma. Appearance of recurrent conjunctival squamous cell carcinoma with corneal invasion before treatment with topical mitomycin C. After 2 weeks of topical mitomycin C therapy, the tumor showed a dramatic response. Diffuse squamous cell carcinoma involving limbal conjunctiva and cornea for six clock hours. Appearance after four weeks of topical mitomycin C treatment displaying complete resolution of the tumor. Appearance of squamous cell carcinoma involving superior bulbar conjunctiva for eight clock hours of cornea in an elderly man from a nursing home. After surgical resection, the wound has healed well but histopathology confirmed extensive scleral invasion and potential optimistic superior margin. Recurrent amelanotic conjunctival melanoma occupying entire superior fornix in a 60-year-old woman. At time of surgery, tumor was eliminated completely with postlamellar dissection of eyelid. Design of plaque to deal with whole floor of conjunctiva; the patient had a number of prior recurrences in all quadrants. Radiation dose plot showing distribution of radiation to anterior section of the attention. Eyelid has been sutured closed during the 7 days that plaque will remain on the eye. In addition, there are a variety of bacterial, fungal, and idiopathic granulomatous problems that can occur within the orbit. The various nomenclature for this intriguing entity has been complicated and inconsistent and includes Graves disease, Graves orbitopathy, Graves ophthalmopathy, thyroid eye illness, thyroid orbitopathy, thyroid ophthalmopathy, dysthyroid orbitopathy, dysthyroid ophthalmopathy, thyroid-related orbitopathy, thyroid-associated orbitopathy, and thyroid-associated ophthalmopathy. We have chosen to use the term "thyroid-related ophthalmopathy" as a result of the condition is said to thyroid dysfunction and impacts different ocular constructions (eyelids, conjunctiva) along with the orbit. In extra advanced circumstances, the patient can develop diplopia, exposure keratopathy, and optic disc edema owing to compression of the optic nerve within the orbit (1�17). Ultrasonography has been largely changed by these superior imaging methods (1). Pathology On surgical inspection or gross examination, the extraocular muscle tissue are enlarged, agency, and rubbery. Histopathology reveals infiltration of the affected enlarged muscular tissues by lymphocytes, plasma cells, and scattered mast cells (1,4). Chapter 26 Inflammatory Lesions That Simulate Neoplasms 451 Selected References 1. Thyroid-related ophthalmopathy with attribute proptosis and eyelid retraction affecting primarily the proper eye in a 35-year-old woman. Thyroid-related ophthalmopathy with bilateral symmetric proptosis and eyelid retraction in a 43-year-old girl. Axial computed tomography exhibiting typical enlargement of extraocular muscle tissue with sparing of the tendons. Coronal computed tomography through the midportion of the orbit, exhibiting enlargement of a quantity of rectus muscle tissue. Middle-aged lady with typical eyelid edema, eyelid retraction, and left esotropia. Woman with retraction of right higher eyelid and extra extreme involvement of the left eye with downward displacement of the globe. Bilateral eyelid retraction producing typical "thyroid stare" in a 27-year-old man. It most commonly occurs because of infectious extension from the ethmoid or frontal sinuses (1�8). However, it may possibly also develop by contiguous spread from websites of trauma or an infection, together with dacryocystitis and conjunctivitis. Mucocele and mucopyocele, which can additionally lengthen into the orbit from the sinuses, are mentioned in Chapter 27. Infectious orbital inflammation has been categorized into 5 classes (1): Group 1: Preseptal cellulitis Group 2: Orbital cellulitis Group three: Subperiosteal abscess Group 4: Orbital abscess Group 5: Cavernous sinus thrombosis Based on conventional terminology, we use the umbrella time period "orbital cellulitis" to embrace all of those classes. Management Treatment generally involves microscopic research and cultures of the discharge and appropriate antibiotic remedy (2). The prognosis is generally good unless extreme cavernous sinus thrombosis develops. Clinical Features the clinical findings in orbital cellulitis range with the inciting trigger and the class and severity of the disease.
Effexor XR: 150 mg, 75 mg, 37.5 mg
Cheap 75 mg effexor xr with amexIf a analysis of pancreatic pseudocyst can be ruled out anxiety symptoms 3 weeks order 75 mg effexor xr amex, analysis should subsequently concentrate on identifying these tumors that require surgical resection due to precise or potential malignancy anxiety symptoms 5 year old discount 150 mg effexor xr mastercard. As against anxiety 6 weeks postpartum purchase effexor xr 37.5mg fast delivery ductal adenocarcinoma anxiety uncertainty management theory purchase 150 mg effexor xr with amex, cystic neoplasms with malignant potential are slow rising, and favorable prognoses have been reported even in the setting of malignant degeneration. Serous cystadenomas, in contrast, are virtually universally benign; they characterize approximately one third of all pancreatic cystic neoplasms. The initial challenge is to segregate benign from doubtlessly malignant cystic tumors (see later). The tougher task is to separate premalignant from invasive tumors, each to avoid overtreatment in older-adult, high-risk sufferers and to focus surveillance imaging in an economical manner to facilitate a secure -operative strategy. These imaging methods allow tumor localization and, generally, discrimination between pseudocysts and cystic neoplasms. They are solitary, mucin-containing, multiloculated or unilocular lesions with a thick fibrotic wall. They are solitary, mucin containing, multilocular, or unilocular lesions with a thick fibrotic wall. In older sequence, most patients complained primarily of stomach pain or a palpable mass. Distal pancreatectomy with or with out splenectomy is the process of choice, given that almost all tumors are located in the physique or tail of the gland. A laparoscopic approach is suitable and results in less blood loss and shorter length of stay, with no difference in operative time, morbidity, or mortality. In cases of small or benign-appearing lesions, enucleation can be carried out without danger of local recurrence and with no mortality. The significant threat of a brief lived fistula is suitable to enable parenchymal preservation and avoid pancreatic insufficiency in low-risk tumors. Historically, most sufferers offered with obscure stomach ache or discomfort, but a big quantity can present with a palpable mass when the tumor has attained a large dimension (10 to 25 cm). Currently, the bulk are found as incidental asymptomatic tumors detected throughout evaluation for other unrelated conditions. A, At surgical procedure, most of the pancreatic parenchyma has been changed by a cystic neoplasm. C, Histopathology displaying cysts containing serous fluid and lined by bland cuboidal cells wealthy in glycogen (H&E). Rare case reviews of serous cystadenocarcinomas exist however represent lower than 3% of known instances. Options for resection depend upon tumor location and include distal pancreatectomy with or with out splenectomy, Whipple process, middle pancreatectomy, or enucleation. Observation carries the risk of continued development, which may result in issues similar to hemorrhage, mass impact causing obstructive jaundice and pancreatic duct obstruction with exocrine insufficiency, or gastric outlet obstruction. Another sequence of patients adopted for a imply of forty two months found that tumor dimension correlated with subsequent growth price. A variety of terms have been applied in reference to these tumors and include mucinous ductal ectasia, intraductal mucin-producing tumor, intraductal cystadenoma, pancreatic duct villous adenoma, and intraductal papillary neoplasm. At the best of the picture is the duodenum, which is focally invaded by the mucinous tumor on the prime right (H&E low power). Approximately 75% of sufferers are symptomatic, with abdominal ache and weight reduction being the most typical complaints. A history of recurrent pancreatitis is given by 20% of patients, and acute pancreatitis is found in roughly 25% at presentation. Other findings during pancreatography embrace major duct dilation, filling defects attributable to viscid mucus or tumor nodules. Factors related to worse outcome in sufferers with invasive histology embrace lymph node metastases, lymphovascular invasion, perineural invasion, and constructive margins. One study found 21% of patients had recurrence at a median follow-up of forty six months. During a mean follow-up of seventy three months, 20% of 153 margin-negative patients had recurrence lesions; three of those 31 had invasive cancer. Patients with recurrent disease localized to the pancreas can profit from completion pancreatectomy. At least 15% of tumors are discovered as incidental findings, usually throughout routine physical exams or throughout analysis after trauma. The tumors could be quite large at presentation, with 34% of sufferers having masses larger than 10 cm in diameter. Grossly, small tumors are comparatively solid, whereas larger variants present significant cystic degeneration. Microscopically, a mix of solid, pseudopapillary, and hemorrhagic pseudocystic areas are observed. A giant meta-analysis of revealed series found a 20% frequency of stable pseudopapillary carcinoma. Complete resection is the remedy of selection, and resection of synchronous or interval metastases can be really helpful when possible. Acinar cell carcinomas are extraordinarily uncommon, representing 1% to 2% of pancreatic tumors. Clinical presentation could additionally be indistinguishable from pancreatic ductal adenocarcinoma. Overall, acinar cell carcinomas are considered an aggressive malignancy, and 50% of instances current with liver metastasis; nonetheless, prognosis seems to be higher than for ductal adenocarcinoma. In basic, this is a disease of younger women of their 30s, with very few circumstances (5%) reported in adults older than 50 years. An R0 resection was obtained after a standard femoral vein graft was used to replace a long segment of portal vein and superior mesenteric vein involvement. Treatment often consists of a combination of chemotherapy and radiation therapy, and treatment rates near 30% are reported in the literature. Pancreatic ductal adenocarcinoma: state-of-the-art 2017 and new therapeutic strategies. High cancer threat in Peutz-Jeghers syndrome: a systematic review and surveillance suggestions. Association of diabetes mellitus and pancreatic adenocarcinoma: a metaanalysis of 88 studies. Pancreatitis, pancreatic, and thyroid most cancers with glucagon-like peptide-1-based therapies. World Health Organization classification of tumours: Pathology and genetics of tumours of the digestive system. Prognostic factors in resected pancreatic adenocarcinoma: analysis of precise 5-year survivors.

Discount effexor xr 37.5 mg lineThe ductular modifications to canalicular bile include (1) the absorption of solutes corresponding to glucose anxiety symptoms vs heart attack symptoms order effexor xr 150mg on-line, amino acids anxiety problems best 75mg effexor xr, and bile acids; (2) the movement of water via specific channels (aquaporins) and paracellularly; and (3) the secretion of solutes such as bicarbonate and chloride anxiety symptoms body purchase effexor xr 150 mg with visa. The contribution of this ductular secretion varies amongst species anxiety counseling generic 150mg effexor xr otc, with estimates suggesting that it might account for up to 30% of bile move in humans but less than 10% of bile move in animals similar to rats. To maintain this course of, hepatocytes should transport bile acids efficiently from the portal blood into bile. Bile acid flux via the liver and the number of taking part hepatocytes range. In the fasting state, uptake of bile acids is highest in the periportal hepatocytes (closest to the portal venules), whereas during feeding, extra distal hepatocytes within the liver acinus are recruited to take part. Conversely, production and secretion of newly synthesized bile acids is highest in pericentral hepatocytes (closest to the central vein). In this trend, the periportal hepatocytes transport a larger fraction of the bile acid pool and are thought to be major drivers of bile aciddependent bile move. Bile Acid�Independent Bile Flow Hepatocyte canalicular bile circulate can additionally be generated by active secretion of primary solutes in addition to bile acids. Uptake by the liver is typically expressed as fractional extraction, or first-pass extraction, and represents the percentage of bile acids removed throughout a single passage by way of the hepatic acinus. The fractional extraction of bile acids from sinusoidal blood ranges from 50% to 90% and remains constant regardless of systemic bile acid concentrations. The sinusoidal membrane additionally incorporates a sodium-hydrogen exchanger and a sodium-bicarbonate cotransporter (symporter). Because of their significance for bile secretion, the bile acid transporters are highlighted; nevertheless, the hepatocyte sinusoidal and canalicular membranes also categorical specialized transport proteins for a wide spectrum of endogenous and exogenous compounds. This variant, which is prevalent in Asian populations (minor allele frequency starting from three. Studies using in situ perfused intestinal segments to measure bile acid absorption demonstrated that ileal bile acid transport is a highcapacity system and sufficient to account for the biliary output of bile acids. Ileal active transport is the most important route of conjugated bile acid uptake, significantly for the more hydrophilic and taurine-conjugated species. In the proximal small gut, a fraction of the glycine-conjugated bile acids are protonated and can endure nonionic passive diffusion when the intraluminal pH becomes transiently acidic during digestion. In addition, metabolism by the gut microbiota in the small gut and colon generates unconjugated hydrophobic bile acids, that are weak acids and are passively absorbed if they proceed to be in answer. Renal Bile Acid Transport A fraction (10% to 50%, relying on the bile acid species) of the bile acids returning in the portal circulation escapes hepatic first-pass extraction and spills into the systemic circulation. The binding of bile acids to plasma proteins reduces glomerular filtration and minimizes urinary excretion of bile acids. In healthy humans, the kidney filters roughly a hundred mol of bile acids every day. Remarkably, just one to 2 mol are excreted within the urine because of extremely efficient tubular reabsorption. Even in sufferers with cholestatic liver disease, in whom plasma bile acid concentrations are considerably elevated, the 24-hour urinary excretion of nonsulfated bile acids is far lower than the amount that undergoes glomerular filtration. Subsequent research have shown that bile acids within the glomerular filtrate are actively reabsorbed from the renal tubules, and this course of contributes to the rise in serum bile acid concentrations in patients with cholestatic liver illness. As in the ileum, the renal proximal tubule epithelium expresses a Na+ gradient�driven transporter that features as a salvage mechanism to preserve bile acids. After their efflux, the conjugated or unconjugated bile acids are carried in sinusoidal blood to more pericentral hepatocytes for reuptake and secretion into bile. In addition, the modified bile acids generated by hepatocyte section 1 or part 2 metabolism are also effluxed across the sinusoidal membrane and cross into the systemic circulation, where they are often filtered by the kidney and excreted in urine. These hepatoprotective mechanisms, which also embrace downregulation of the major liver bile acid uptake transporters, are an necessary a part of the adaptive response to conditions of bile acid overload. Although inherited defects in biosynthesis are uncommon, these disorders serve to illustrate the importance of bile acid synthesis for normal hepatic and intestinal function. The results of a block in bile acid synthesis embody depletion of the bile acid pool by fecal excretion, loss of bile acid�dependent bile circulate, decreased biliary excretion of cholesterol and xenobiotics, malabsorption of fats and fat-soluble nutritional vitamins, and accumulation of cytotoxic bile acid biosynthetic intermediates. Inherited defects in 11 of the enzymes and 1 transporter involved in bile acid biosynthesis have been reported. In addition to these particular defects, problems that disrupt peroxisome biogenesis similar to Zellweger syndrome additionally have an result on bile acid synthesis as a end result of the bile acid facet chain modification steps happen within the peroxisome (see Chapter 77). A single enzyme defect is normally not adequate to block manufacturing of all bile acids, as a end result of a quantity of biosynthetic pathways exist. Clinically, sufferers with bile acid synthesis defects sometimes present with steatorrhea, development retardation, sequelae related to fat-soluble vitamin malabsorption, and mild to severe liver illness. Depending on the step within the pathway and the nature of the mutation, the implications of bile acid biosynthesis defects can vary, with the most extreme producing neonatal cholestatic liver disease or neurologic disease later in life. The illness is characterised by progressive intrahepatic cholestasis and accumulation of irregular bile acids. Clinical manifestations embrace unconjugated hyperbilirubinemia, jaundice, serum aminotransferase elevations, steatorrhea, fat-soluble vitamin deficiency, pruritus, and poor development. The development of disease is variable however finally leads to cirrhosis and hepatic failure in a high proportion of affected individuals. Impaired hepatic transport of bile acids and different natural solutes is a distinguished characteristic of both inherited and acquired forms of cholestatic liver disease. Disorders of the enterohepatic circulation are usually categorised into the following 4 classes: (1) defects in bile acid formation (synthesis and conjugation); (2) defects in membrane transport of bile acids (uptake and secretion); (3) disturbances involving bacterial transformation (deconjugation and dehydroxylation); and (4) disturbances in movement by way of or between organs (bile acid circulation). However, measurement of complete serum bile acid concentrations without profiling the individual bile acids and bile acid intermediates seems to offer little, if any, benefit over conventional liver biochemical exams in the prognosis or administration of most types of liver illness or bile acid malabsorption. In the absence of biliary phospholipid, the hydrophobic bile acids are poisonous and cause cholestatic liver harm. The unconjugated bile acids are much less soluble than their glycine or taurine conjugates and precipitate within the intestine lumen or are absorbed passively if they proceed to be in solution. As a result, in depth bacterial deconjugation reduces the intraluminal focus of bile acids available to kind micelles with dietary lipids in the small gut. A portion of the retained bile acids is modified by sulfation, and both sulfated and unsulfated bile acids are regurgitated from hepatocytes again into the systemic circulation. Despite elevated urinary excretion of bile acids, plasma concentrations of bile acids rise as much as 20-fold. In a patient with a biliary fistula, bile acids are diverted from entering the small intestine. Because bile acid biosynthesis is controlled by unfavorable suggestions, bile acid synthesis rises markedly, as a lot as 20-fold. As in biliary obstruction, decrease bile acid concentrations within the small gut end in malabsorption of fat-soluble nutritional vitamins. Absorption of dietary fat, especially dietary triglycerides that contain long-chain saturated fatty acids, is also decreased.
Effexor xr 75 mg low costThere is typically overlap clinically histopathologically amongst capillary hemangioma anxiety symptoms 6 year old order 150mg effexor xr visa, cavernous hemangioma anxiety kit buy effexor xr 37.5 mg overnight delivery, and lymphangioma anxiety in relationships generic effexor xr 75 mg with amex, making precise categorization troublesome anxiety while sleeping 150mg effexor xr overnight delivery. Clinical Features Like its eyelid counterpart, conjunctival capillary hemangioma typically seems at or shortly after start and reveals progressive progress for up to 2 years after which slowly regresses. It can happen anyplace within the conjunctiva and appears as a definite or diffuse pink conjunctival mass. It can occur as an isolated lesion or it could be seen in affiliation with a periocular cutaneous capillary hemangioma (see eyelid section). Conjunctival involvement can be seen in affiliation with diffuse neonatal hemangiomatosis, which is typically a deadly situation (5). Pathology Histopathologically, conjunctival capillary hemangioma is composed of lobules of proliferating endothelial cells separated by skinny fibrous septa. Lesions that have proven spontaneous regression are less vascular and contain more fibrous tissue. Management the administration of infantile conjunctival capillary hemangioma is mostly remark, with the assumption that the lesion will regress. In the uncommon case the place the lesion is larger and potentially amblyogenic, treatment with oral or intralesional corticosteroids may hasten resolution. Histopathology of capillary hemangioma showing numerous capillary channels and proliferation of endothelial cells. In latest years, the true existence of a tumor derived from pericytes has been challenged and some authorities imagine that previously reported circumstances of hemangiopericytoma could additionally be variants of solitary fibrous tumor (1). Until that problem is resolved, we continue to embrace conjunctival hemangiopericytoma. Clinical Features Conjunctival hemangiopericytoma seems as an elevated or pedunculated reddish-pink mass that has no distinct scientific options. It exhibits slow, progressive growth and infrequently is steady with a extra posterior orbital component. Pathology Hemangiopericytoma is a tumor composed of an irregular proliferation of pericytes that encompass blood vessels. With routine mild microscopy, a characteristic feature is the "staghorn" branching of the blood vessels in the tumor. Clinical Features Conjunctival glomus tumor can appear as a reddish-blue mass that intently resembles a lymphangioma. It is rare, but might have a predisposition to have an result on the insertions of rectus muscle tissue. Pathology the pathology of glomus tumor is discussed in the part on eyelid tumors. In the conjunctiva this tumor may be bigger than suspected clinically and will extend into the orbit (1). Chapter 20 Vascular Tumors and Related Lesions of the Conjunctiva 363 Conjunctival Hemangiopericytoma and Glomangioma 1. Clinical appearance of one lesion, situated within the conjunctival and subconjunctival tissues at insertion of medial rectus muscle. Vimentin stain was additionally optimistic and epithelial and endothelial cell markers have been nonreactive. There is a slight anterior bulging of left lower eyelid secondary to the inferior conjunctival mass. Kaposi sarcoma of the conjunctiva and eyelids associated with the acquired immunodeficiency syndrome. It appears as a number of painless, reddish vascular masses which will turn out to be confluent and resemble hemorrhagic conjunctivitis (1�21). Such treatment ought to be coordinated with infectious illness specialists, basic oncologists, or oncologists. When the analysis is uncertain, biopsy may be carried out to exclude simple conjunctival hemorrhage or other hemorrhagic neoplasms. Some authors imagine that surgical excision mixed with cryotherapy is the most costeffective management (17). Incomplete excision has been related to regression of residual tumor (20,21). The affected patient must also be evaluated for life-threatening visceral disease. Another case disclosing the irregular, red vascular tumor within the inferotemporal fornix. These can have distinct options or overlap significantly in their cellular constituents. Choroidal metastasis from medullary thyroid carcinoma in multiple endocrine neoplasia. General Considerations Neural tumors like easy neuroma and neurofibroma can occur in the conjunctiva (1�13). The greatest recognized simple neuromas are the delicate mucosal neural tumors that seem within the conjunctiva and other mucous membranes in patients with multiple endocrine neoplasia sort 2b (10�13). Because of the excessive affiliation with life-threatening medullary thyroid carcinoma, ophthalmologists ought to be acquainted with these conjunctival lesions. These benign neural tumors are typically asymptomatic and often require no treatment. Conjunctival and orbital neurofibromas could be divided into solitary, diffuse, and plexiform types (5). Clinical Features Solitary conjunctival neurofibroma appears as a yellow-gray sessile or dome-shaped mass situated within the conjunctival stroma. The plexiform variant is an ill-defined, agency, irregular mass that has been likened to a bag of worms. The conjunctival plexiform neurofibroma is usually in continuity with the same lesion of the eyelid and orbit. Pathology Histopathologically, diffuse and plexiform neurofibromas are composed of bundles of enlarged nerves with proliferation of Schwann cells and endoneural fibroblasts in a mucoid matrix. It can generally be troublesome to differentiate from different spindle cell tumors and particular stains for axons could help make the diagnosis in such instances (4�6). Management Solitary tumors seem as slowly enlarging elevated stromal plenty that might be managed by full surgical resection. The plexiform sort may be extraordinarily tough to take away intact and debulking procedures are sometimes necessary. It is a comparatively frequent gentle tissue tumor of the orbit (1) and may often happen in the conjunctiva (2�5). Management Like different slowly progressive, circumscribed, benign tumors, the best administration is full surgical excision. Clinical Features In the conjunctiva, schwannoma presents as a lightweight pink-yellow, elevated mass that typically lies in the stroma of the bulbar conjunctiva or episcleral tissues.
Purchase effexor xr 75 mg on-lineQuantifying anomalous intestinal sterol uptake anxiety symptoms change buy 37.5 mg effexor xr, lymphatic transport anxiety heart rate discount effexor xr 37.5 mg mastercard, and biliary secretion in Abcg8(-/-) mice anxiety symptoms pain effexor xr 37.5mg amex. Hepatic Niemann-Pick C1-like 1 regulates biliary cholesterol concentration and is a goal of ezetimibe anxiety from weed purchase effexor xr 150 mg mastercard. Homozygous disruption of the murine mdr2 P-glycoprotein gene leads to a complete absence of phospholipid from bile and to liver disease. Genotype-phenotype relationships within the low-phospholipid-associated cholelithiasis syndrome: a research of 156 consecutive patients. Severe cholestasis induced by cholic acid feeding in knockout mice of sister of P-glycoprotein. Nucleation time: a key factor in the pathogenesis of ldl cholesterol gallstone illness. Central adiposity, regional fats distribution, and the chance of cholecystectomy in women. Gallbladder illness is associated with insulin resistance in a high risk Hispanic population. Gallstone illness is associated with extra severe liver harm in patients with non-alcoholic fatty liver disease. Cholelithiasis and markers of nonalcoholic fatty liver illness in patients with metabolic danger elements. Fatty liver illness: predictors of nonalcoholic steatohepatitis and gallbladder illness in morbid obesity. Abnormalities of serum cholecystokinin and gallbladder emptying in celiac illness. Gallbladder emptying and somatostatin and cholecystokinin plasma ranges in celiac illness. Impaired intestinal cholecystokinin secretion, an interesting but missed hyperlink between coeliac disease and ldl cholesterol gallstone disease. Long-term statin use and the risk of gallstone disease: a population-based case-control study. A potential study of coffee consumption and the chance of symptomatic gallstone illness in men. Coffee consumption is associated with decrease threat of symptomatic gallstone disease in girls. Ternary and quaternary aqueous methods containing bile salt, lecithin, and ldl cholesterol. Characterization of crystallization pathways throughout cholesterol precipitation from human gallbladder biles: identical pathways to corresponding mannequin biles with three predominating sequences. Phenotypic characterization of Lith genes that determine susceptibility to ldl cholesterol cholelithiasis in inbred mice: physical-chemistry of gallbladder bile. Filamentous, helical, and tubular microstructures during ldl cholesterol crystallization from bile. Phospholipid molecular species influence crystal habits and transition sequences of metastable intermediates throughout ldl cholesterol crystallization from bile salt-rich model bile. Newer pathogenetic concepts in ldl cholesterol gallstone formation: a unitary hypothesis. Role of gallbladder mucus hypersecretion in the evolution of ldl cholesterol gallstones. Mucus hypersecretion in the gallbladder epithelium of floor squirrels fed a lithogenic food plan for the induction of ldl cholesterol gallstones. Targeted disruption of the murine mucin gene 1 decreases susceptibility to cholesterol gallstone formation. Isolation of a potent cholesterol nucleation-promoting exercise from human gallbladder bile: role within the pathogenesis of gallstone illness. Inhibition of ldl cholesterol crystal formation by apolipoproteins in supersaturated mannequin bile. Apolipoprotein A-I in bile inhibits ldl cholesterol crystallization and modifies transcellular lipid switch by way of cultured human gallbladder epithelial cells. The impact of bile acid hydrophobicity on nucleation of several types of ldl cholesterol crystals from model bile vesicles. Effects of bile salt and phospholipid hydrophobicity on lithogenicity of human gallbladder bile. Gallbladder motility and cholesterol crystallization in bile from sufferers with pigment and cholesterol gallstones. Gallbladder emptying determines early gallstone clearance after shock-wave lithotripsy. Cholesterol gallstone formation in man and potential therapies of the gallbladder motility defect. Gallbladder emptying in vivo, bile composition, and nucleation of ldl cholesterol crystals in patients with ldl cholesterol gallstones. Bile concentration promotes nucleation of ldl cholesterol monohydrate crystals by rising the ldl cholesterol concentration within the vesicles. Gallbladder histopathology during murine gallstone formation: relation to motility and concentrating perform. Impaired human gallbladder lipid absorption in ldl cholesterol gallstone illness and its effect on ldl cholesterol solubility in bile. Enhanced gallbladder absorption during gallstone formation: the roles of cholesterol saturated bile and gallbladder stasis. High cholesterol absorption efficiency and fast biliary secretion of chylomicron remnant cholesterol improve cholelithogenesis in gallstone-susceptible mice. Targeted disruption of the murine cholecystokinin-1 receptor promotes intestinal ldl cholesterol absorption and susceptibility to ldl cholesterol cholelithiasis. Deoxycholic acid influences cholesterol solubilization and microcrystal nucleation time in gallbladder bile. Roles of gall bladder emptying and intestinal transit in the pathogenesis of octreotide induced gall bladder stones. Composition of gall bladder stones associated with octreotide: response to oral ursodeoxycholic acid. Phenotypic characterization of Lith genes that determine susceptibility to cholesterol cholelithiasis in inbred mice. Identification of cholelithogenic enterohepatic Helicobacter species and their position in murine ldl cholesterol gallstone formation. Helicobacter pylori and ldl cholesterol gallstone formation in C57L/J mice: a prospective research. The integrity of the cholecystokinin receptor gene in gallbladder disease and weight problems. Cholesterol crystallization in human gallbladder bile: relation to gallstone quantity, bile composition, and apolipoprotein E4 isoform.
References - Kaufman SS, Chatterjee NK, Fuschino ME, et al. Calicivirus enteritis in an intestinal transplant recipient. Am J Transplant. 2003; 3:764-768.
- Makhdoom ZA, Komar MJ, Still CD. Nutrition and enterocutaneous fi stulas. J Clin Gastroenterol. 2000;31:195-204.
- Farrell DJ, Mendes RE, Ross JE, et al. LEADER program results for 2009: an activity and spectrum analysis of linezolid using 6,414 clinical isolates from the United States (56 medical centers). Antimicrob Agents Chemother. 2011 Jun 13 [Epub ahead of print]. 143.
- Green, T.D., Joseph, J.V., Feng, C., Ertuck, E. Evaluation and management of post shock wave lithotripsy pain and third generation lithotriptors using rofecoxib. J Endourol 2009;23:395-398.
- Chaney MA, Nikolov MP, Blakeman BP, et al: Intrathecal morphine for coronary artery bypass graft procedure and early extubation revisited, J Cardiothorac Vasc Anesth 13:574, 1999.
|

