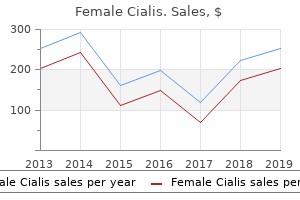
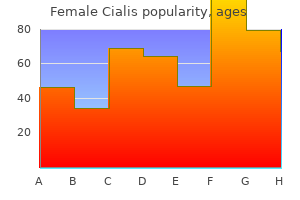
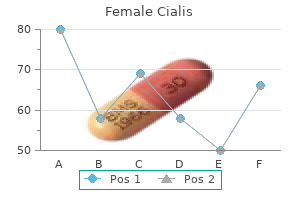
Female Cialis
James W. Albers, M.D., Ph.D. - Department of Neurology
- University of Michigan
- Ann Arbor, MI
Discount female cialis 10 mg onlineThe diaphragm is sampled most commonly within the intensive care ward menopause 41 discount female cialis 10 mg with amex, where a complication corresponding to pneumothorax is probably much less worrisome than in an outpatient setting menstruation 18th century female cialis 20 mg for sale. Combined with phrenic nerve stimulation an efficient evaluation of the nerve integrity to the diaphragm could be made pregnancy after tubal ligation cheap 20 mg female cialis. The blink reflex is considered one of these exams like the sympathetic pores and skin response menstrual underpants buy discount female cialis 20mg online, which theoretically should have an enormous contribution to the assessment not only of the fifth and seventh cranial nerves, but in addition the a quantity of pathways, which serve it within the brainstem. Of the opposite tests available motor unit number estimation (51�53) is completely possible to do in youngsters and is well tolerated. Exercise checks are also easily tolerated by youngsters and might be mentioned in the section on myotonia. The structure of this chapter will observe anatomy; so start with the anterior horn cell, passing from the nerve to the neuromuscular junction, earlier than finally contemplating situations affecting the muscle. Within this anatomical description the aetiologies will comply with routine assessment namely separating into congenital and purchased situations. Within the latter, discussion will cover the different aetiologies that may be relevant from infective, autoimmune, metabolic, vascular, iatrogenic, trauma, drugs and toxins, and at last unknown causes. There are many more neuromuscular issues, which affect kids than might be discussed on this chapter. More generally nowadays one is encountering anterior horn cell illness with none identified aetiology. Previously their weak spot was explained entirely on the basis of the upper motor neuron lesion. It is important at this point to emphasize the significance of examination of the tongue within the investigation of these kids. Instead in youngsters the differential analysis lies between segmental involvement of the spinal wire either in the cervical or lumbar area only, or a more generalized abnormality. If solely the legs have been concerned a lumbar segmental involvement can be confidently diagnosed. The children have fully flaccid arms with preserved sensory responses, however often little or no motor response. We have seen the infarction broaden additional down the spinal cord to involve the thoracic region and in these circumstances the nerve supply to the intercostals is affected (67). The scenario is far more severe and the children are unable to breathe with out air flow. This is a very completely different prognostic situation to these with an isolated cervical involvement. The downside in United Kingdom is that the cases are likely to be sporadic somewhat than epidemic, since the only widespread purpose for epidemics, the polio virus, has been eliminated. In this context is maybe one of the necessary latest developments in paediatric neurology, with the discovery that a proportion of youngsters suffering Brown Vialetto van Laere illness have been proven to have a dysfunction of their riboflavin metabolism (82�87). More remarkably treatment with giant doses of riboflavin can reverse the inexorable and relentless development of this illness beforehand considered a fatal condition. Some of the children passed very rapidly through this phase of motor neuronopathy to develop a sensorimotor neuropathy. The most nicely acknowledged cause of this phenomenon is in muscular Disorders of peripheral nerve Hereditary problems of nerves are an ever expanding and important part of paediatric electromyography. It is almost inconceivable for these not working constantly in this area to have any chance of keeping up with the variety of chromosome abnormalities which have been identified. With the rising variety of genes being identified has also come a realization of the expanding phenotype of hereditary neuropathies. The paediatric electromyographer confronted with such a baby could have their main duty to distinguish between an axonal or demyelinating neuropathy. The paediatric electromyographer has to choose what is possible and what contributes most to subsequent genetic localization of the defect. Undoubtedly conduction studies both within the upper and lower limb are important as some might differ in the extent of their involvement within the higher and decrease limbs. Also comparing the speed throughout the size of the nerve is helpful expecting to see a rise within the velocity in probably the most cranial segments, which is seen in hereditary neuropathies, however not in acquired neuropathies. Similar velocities in comparable limb segments of the 2 sides are another characteristic strongly in favour of a hereditary neuropathy. Guillain-Barr� syndrome is properly recognized to occur in kids although less frequently than in adults. The characteristic neurophysiological findings are sometimes varied with some kids only having abnormalities of the F waves while others reveal the entire vary of abnormalities described similar to important prolongation of the distal motor latency, outstanding slowing of the principle nerve with marked dispersion on proximal stimulation. The nerve conduction research present focal slowing doubtless due to the infarction of the nerve. An increasing part of our work has been to monitor the consequences of neurotoxic medicine, specifically thalidomide, which has made a re-appearance as an effective remedy significantly in disorders of the pores and skin in addition to gastrointestinal issues (95�100). While one is really helpful to examine many nerves, the examination of the sensory nerves within the legs is enough to alert the clinicians to the neuropathic change. If the nerves within the leg turn out to be affected, the following study can incorporate the arms as nicely. Metabolic conditions such as leucodystrophies at the second are a rare indication for peripheral nerve research, having normally been identified by metabolic means. In the previous before such screening grew to become commonplace, the demonstration of a big demyelinating neuropathy in a toddler showing developmental regression was an necessary pointer to these diagnoses. The only exception to this rule is nerve injury on account of trauma, significantly of the higher limb. Worryingly the state of affairs was that the progression of the disorder from one showing solely sensory abnormalities to complete loss of motor responses was very speedy certainly often occurring in less than six months. These can occur for a wide range of reasons, but mostly as the end result of surgical intervention (107). The nerve is especially susceptible in operations around the pelvis, particularly if involving the lithotomy position (108�110). Also much less easy to explain are those who have occurred in the context of operations have been no intervention either for vascular access or positioning has been made within the pelvic area. Follow-up knowledge is tough to acquire on these youngsters due to the character of our referral pattern, however from the few that have been seen again they seem to recuperate much better than adults. Thoracic outlet syndrome should all the time be sought in situations with numbness within the medial facet of the arm and hand, but is very uncommon. The presence of cervical ribs, a recognized risk factor for thoracic outlet syndrome, may make the infant more prone to obstetric brachial plexus damage (111). For a lengthy time that it was the rule to examine round three months of age, but this was pushed by the surgical strategies, which might encourage surgery if passable biceps operate had not been achieved by that date (112�114). Around 10 years ago there were maybe just one or two, whereas on the last rely there are round 14 (124).
Effective 20mg female cialisUsing preapplied adhesive defibrillator pads avoids the necessity to womens health 8 week workout buy generic female cialis 20 mg on line disrupt the sterile area in the occasion that electrical defibrillation or cardioversion is required during the procedure menstruation explained 10 mg female cialis otc. Patients with critical aortic stenosis menstrual cramps 7dpo generic 10 mg female cialis otc, extreme hypertrophic cardiomyopathy menopause the musical reviews purchase female cialis 10 mg on line, left major or extreme threevessel coronary artery disease, or decompensated coronary heart failure are at higher than common danger of complications.
[newline]Induction of sustained tachyarrhythmias in these patients can cause extreme deterioration. Longer procedures and ablations are actually routinely carried out utilizing intravenous aware sedation. Bispectral evaluation of mind electrical exercise is sometimes used for monitoring the depth and safety of sedation. In certain conditions, especially when mapping and ablation of an computerized or triggered-activity tachycardia are expected, sedation can suppress the arrhythmic activity and delay or preclude the mapping-ablation process. In such cases, avoiding sedation is advisable till inducibility of the tachycardia is ensured. In chosen circumstances, antiarrhythmic medicine may be continued if an arrhythmic occasion occurred whereas the patient was taking a selected agent. Therefore, affected person education is an essential part of the 62 63 Oxygen and Carbon Dioxide Monitoring Monitoring of oxygen saturation is used routinely. Exhaled carbon dioxide displays also may be useful in stopping hypercapnia in patients receiving supplemental oxygen, as a result of oxygen saturation could be misleadingly excessive. Similarly, sufferers with mechanical valvular prosthesis require uninterrupted anticoagulation. A perception of increased bleeding dangers of invasive procedures in patients taking therapeutic warfarin doses led many operators to undertake a "bridging" strategy of conversion to enoxaparin to permit ablation and subsequent hemostasis to be carried out throughout a pause in anticoagulation. Another potential benefit of this strategy is the ability to reverse warfarin effects quickly in the setting of a bleeding complication. Bipolar or quadripolar electrode catheters are used to document and pace from particular websites of curiosity within the atria or ventricles. Basket catheters able to conforming to the chamber measurement and shape have additionally been used for mapping atrial and ventricular arrhythmias. Steerable catheters enable deflection of the tip of the catheter in a single or two instructions in a single aircraft; some of these catheters have asymmetrical bidirectional deflectable curves. These catheters include insulated wires; at the distal tip of the catheter, each wire is connected to an electrode, which is exposed to the intracardiac floor. At the proximal end of the catheter, each wire is hooked up to a plug, which could be related to an external recording device. Electrode catheters are generally manufactured from woven Dacron or newer synthetic supplies, similar to polyurethane. The Dacron catheters have the benefit of stiffness, which helps keep catheter form with sufficient softness at body temperature to permit formation of loops. Recordings derived from electrodes could be unipolar (one pole) or bipolar (two poles). The higher the interelectrode spacing is on a standard bipolar electrode, the extra the recorded electrogram resembles a unipolar recording. More just lately, newer navigation systems have been tested to information catheter positioning in an effort to limit radiation exposure (see Chap. Transcaval Approach the modified Seldinger method is used to obtain a quantity of venous accesses. Multiple venous punctures and single vascular sheaths could also be used for the completely different catheters. The larger tip electrodes on ablation catheters scale back the decision of a map obtained using recordings from the distal pair of electrodes. It is then withdrawn across the tricuspid orifice whereas sustaining a slight clockwise torque for good contact with the septum till a His potential is recorded. When the catheter is additional withdrawn, the atrial electrogram seems and grows larger. The His potential usually seems as quickly as the atrial and ventricular electrograms are roughly equal in size and is manifest as a biphasic or triphasic deflection interposed between the native atrial and ventricular electrograms. Subsequently, the catheter is withdrawn until it lies at the inferoseptal aspect of the tricuspid annulus. The true interatrial septum is restricted to the ground of the fossa ovalis, the flap valve, and the anteroinferior rim of the fossa. A seek for a patent foramen ovale, which is present in 15% to 20% of regular subjects, is initially performed. The guidewire is then withdrawn, thus leaving the sheath and its dilator locked in place. Alternatively, the inner stylet could additionally be eliminated and the needle related to a pressure transducer line (pressure monitoring through the Brockenbrough needle shall be required during the transseptal puncture); steady flushing via the Brockenbrough needle is used while advancing the needle into the dilator. A third approach, when the utilization of distinction injection is deliberate, is to connect the Brockenbrough needle to a standard three-way stopcock through a freely rotating adapter. A 10-mL syringe full of radiopaque contrast is attached to the opposite end of the stopcock while a strain transducer line is attached to the third stopcock valve for steady pressure monitoring. The complete apparatus ought to be vigorously flushed to make certain that no air bubbles are present inside the circuit. The Brockenbrough needle is advanced into the dilator till the needle tip is inside 1 to 2 cm of the dilator tip. The needle tip should be stored throughout the dilator always, besides during actual septal puncture. A third abrupt leftward motion ("leap") below the aortic root indicates passage over the limbus into the fossa ovalis. The sheath and dilator meeting should never be advanced without the guidewire at any level through the process. Several fluoroscopic markers are used to affirm the place of the dilator tip at the fossa ovalis. As noted, an abrupt leftward motion (jump) of the dilator tip under the aortic knob is noticed because the tip passes under the muscular atrial septum onto the fossa ovalis (see Video 4). Another methodology that can be utilized to ensure that the tip is in opposition to the fossa ovalis is injection of 3 to 5 mL of radiopaque contrast through the Brockenbrough needle to visualize the interatrial septum. The needle tip then can be seen tenting the fossa ovalis membrane with small actions of the whole transseptal apparatus. Typically, septal staining stays seen after contrast injection, which allows for real-time septal visualization whereas monitoring the strain throughout transseptal puncture. Absence of a pressure wave recording can point out needle passage into the pericardial area or sliding up and not puncturing via the atrial septum. A second method is injection of contrast by way of the needle to assess the place of the needle tip. In addition, aortic puncture must be suspected if the guidewire appears to comply with the course of the aorta. In these conditions, distinction must be injected to assess the place of the Brockenbrough needle earlier than advancing the transseptal dilator. The sheath ought to be aspirated until blood appears without additional bubbles; this usually requires aspiration of roughly 5 mL. The sheath is then flushed with heparinized saline at a flow fee of three mL/min during the entire procedure.
Diseases - Usher syndrome
- Dementia, familial British
- Sezary syndrome
- Pulmonar arterioveinous aneurysm
- Tricuspid dysplasia
- Methylmalonic acidemia with homocystinuria
- Factor VIII deficiency
- MPS III-C
Buy female cialis 20 mg onlineReentry Basic Principles of Reentry During every regular cardiac cycle menstrual games discount 10 mg female cialis with mastercard, at the completion of regular cardiac excitation women's health issues author guidelines discount 10 mg female cialis amex, the electrical impulse originating from the sinus node becomes extinct womens health worcester generic 10 mg female cialis visa, and the subsequent excitation cycles originate from new pacemaker impulses women's health clinic gwinnett county order female cialis 20 mg amex. Reentry happens when a propagating impulse fails to die out after regular activation of the guts and persists to reexcite the guts after expiration of the refractory period. In pathological settings, excitation waves can be blocked in circumscribed areas, rotate round these zones of block, and reenter the positioning of original excitation in repetitive cycles. Reentrant tachycardia, additionally referred to as reentrant excitation, reciprocating tachycardia, circus movement, or reciprocal or echo beats, is a continuous repetitive propagation of the activation wave in a round path, returning to its web site of origin to reactivate that website. Although this distinction has a historic background and is useful for didactic functions, each the anatomical and practical varieties can coexist in a given pathological setting and share many common fundamental biophysical mechanisms. The unique three standards for reentry proposed by Mines still maintain true: (1) unidirectional block is necessary for initiation; (2) the wave of excitation should journey in a single path across the pathway, returning to its point of origin after which restarting along the identical path; and (3) the tachycardia should terminate when one limb of the pathway is minimize or briefly blocked. When the reentrant circuit forms, the road of block then is sustained by centripetal activation from the circulating wavefront that, by repeatedly bombarding the central space of block, maintains the state of refractoriness of this region. Additionally, it has now been proven that a functional extension of an anatomical line of block can happen such that it plays a job in creating the mandatory or crucial substrate for reentry. The excitation wavefront propagating within the substrate must encounter unidirectional block; in any other case, the excitation wavefronts touring down each limbs of the reentrant circuit will collide and extinguish each other. Therefore, a situation needed for reentry is the upkeep of excitable tissue forward of the propagating wavefront. In other words, the tissue initially activated by the excitation wavefront should have sufficient time to recover its excitability by the point the reentrant wavefront returns. Thus, conduction of the circulating wavefront have to be sufficiently delayed in an alternate pathway to allow for expiration of the refractory interval within the tissue proximal to the positioning of unidirectional block, and there must all the time be a spot of excitable tissue (fully or partially excitable) ahead of the circulating wavefront. This is facilitated by a sufficiently lengthy reentrant pathway (which is very important when conduction is normal alongside the reentrant path), sufficiently gradual conduction in all or a part of the choice pathway (because sufficiently lengthy pathways are normally not current in the heart), sufficient shortening of the refractory interval, or a combination of those components. The cardiac tissue that constitutes the substrate for reentrant excitation could be positioned virtually anyplace in the coronary heart. However, changes in coronary heart rate or autonomic tone, ischemia, electrolyte or pH abnormalities, or the incidence of a untimely depolarization may be enough to provoke reentrant tachycardia. The set off frequently is required as a outcome of it elicits or brings to a important state a number of of the situations necessary to achieve reentrant excitation. Thus, a premature impulse initiating reentry can arrive at one site within the potential reentrant circuit sufficiently early that it encounters unidirectional block, as a end result of that tissue has had insufficient time to recover excitability after excitation by the prior impulse. Furthermore, within the other limb of the potential reentrant circuit, the untimely arrival of the excitation wavefront causes gradual conduction or leads to further slowing of conduction of the excitation wavefront by way of an space of already slow conduction. The ensuing improve in conduction time round this limb of the potential reentrant circuit permits the region of unidirectional block within the tissue within the different limb activated initially by the untimely beat to recover excitability. It should be famous that the mechanism inflicting the untimely impulse may be different from the reentrant mechanism inflicting the tachycardia. Because the size and location of the reentrant pathway are relatively mounted, the characteristics of the reentrant circuit are decided by the characteristics of the anatomical elements of that circuit. A reentrant tachycardia is initiated when an excitation wavefront splits into two limbs after going across the anatomical impediment and travels down one pathway and not the other, thus creating a circus movement. Tachycardia rates are determined by the wavelength and by the size of the reentrant pathway (the path length). The initiation and maintenance of anatomical reentry depend upon conduction velocity and refractory interval. Thus, as long as the extension of the refractory zone behind the excitation wave, the so-called wavelength of excitation, is smaller than the complete length of the anatomically defined reentrant pathway, a zone of excitable tissue, the so-called excitable hole, exists between the tail of the previous wave and the top of the following wave. In the setting the place the wavelength of excitation exceeds the trail size, the excitation wavefront becomes extinct when it encounters the not yet recovered inexcitable tissue. A special case is present in the intermediate situation, when the head of the next wavefront meets the partially refractory tail of the previous wavefront. Such heterogeneity involves dispersion of excitability or refractoriness and conduction velocity, in addition to anisotropic conduction properties of the myocardium. The circumference of the leading circle around a useful impediment could be as small as 6 to eight mm and represents a pathway in which the efficacy of stimulation of the circulating wavefront is simply enough to excite the tissue ahead, which continues to be in its relative refractory section. Therefore, conduction by way of the practical reentrant circuit is slowed as a result of impulses are propagating in partially refractory tissue. Functional circuits can be related to ordered reentry (the reentrant circuit remains in the same place) or random reentry (the reentrant circuit adjustments size and location). Leading Circle Concept To clarify the properties of a single practical reentrant circuit, Allessie and colleagues formulated the main circle concept. The interplay between the wavefront and the refractory tail determines the properties of functional reentry. The tissue within this core is maintained in a state of refractoriness by constant centripetal bombardment from the circulating wavefront. The premature impulse that initiates reentry blocks in fibers with lengthy refractory periods and conducts in fibers with shorter refractory durations and eventually returns to the preliminary area of block after excitability has recovered there. This central space offers a useful obstacle that prevents excitation from propagating throughout the fulcrum of the circuit. The leading circle was outlined as "the smallest potential pathway by which the impulse can proceed to circulate" and "during which the stimulating efficacy of the wavefront is simply sufficient to excite the tissue ahead which continues to be in its relative refractory part. The velocity worth and the size of the circuit depend upon the excitability of the partially refractory tissue and on the stimulating efficacy of the wavefront, which is set by the amplitude and the upstroke velocity of the action potential and by the passive electrical properties of the tissue. Anisotropy is a normal feature of coronary heart muscle and is said to the variations in longitudinal and transverse conduction velocities, that are attributable to the lower resistivity of myocardium in the longitudinal (parallel to the lengthy axis of the myocardial fiber bundles) versus the transverse course. Anisotropy in myocardium composed of tissue with structural options different from those of adjacent tissue ends in heterogeneity in conduction velocities and repolarization properties (see later discussion), which can lead to blocked impulses and slowed conduction, thereby setting the stage for reentry (referred to as anisotropic reentry). Circuits with this shape can have a smaller dimension than circular circuits, such as the leading circle. Reentrant circuits caused by anisotropy also can happen with out well-defined anatomical pathways and may be classified as useful. Anisotropic reentrant circuits normally remain in a set position and trigger ordered reentry. The excitable hole is caused by the sudden slowing of conduction velocity and a decrease in the wavelength of excitation because the reentrant impulse turns the nook from the quick longitudinal direction to the gradual transverse direction and from the slow transverse course to the fast longitudinal course. Anisotropic reentry is often initiated by a premature stimulus that blocks in the direction of propagation parallel to the long axis of the cells and then propagates slowly within the transverse direction of fiber orientation due to excessive axial resistance (see later). The wavefront then breaks via the arc of block to reexcite the tissue proximal to the block. The single arc of block is thus divided into two, and reentrant activation continues as two circulating wavefronts that travel clockwise and counterclockwise across the two arcs in a pretzel-like configuration. In such a scenario, an motion potential propagates towards, however not by way of, the inexcitable zone.

Discount female cialis 20mg on lineDiaphragmatic paralysis secondary to damage to the best phrenic nerve should be minimized if ablative lesions are confined to the crista itself or positioned just anterior to it menstruation heavy bleeding cheap 20mg female cialis overnight delivery. Additionally menstrual vaginal discharge purchase 20mg female cialis fast delivery, suspicion of phrenic nerve injury ought to be considered within the case of hiccup breast cancer pins cheap 10mg female cialis fast delivery, cough women's health clinic vero beach discount female cialis 10mg without a prescription, or decrease in diaphragmatic tour during energy supply. Such junctional rhythm usually disappears with the return of sinus rhythm inside several days. Nattel S: Inappropriate sinus tachycardia and beta-receptor autoantibodies: a mechanistic breakthrough Calo L, Rebecchi M, Sette A, et al: Efficacy of ivabradine administration in patients affected by inappropriate sinus tachycardia, Heart Rhythm 7:1318�1323, 2010. Mantovan R, Thiene G, Calzolari V, Basso C: Sinus node ablation for inappropriate sinus tachycardia, J Cardiovasc Electrophysiol 16:804�806, 2005. However, the contour of the Koch triangle could also be small and even horizontal in some patients. The transition from one cell area to the opposite is gradual, with intermediate cells exhibiting intermediate motion potentials with great changes related to the autonomic tone. The connections between atrial and transitional cells are so gradual that no clear anatomical demarcations may be detected. Importantly, the restoration of excitability after conduction of an impulse is faster for the sluggish pathway than for the quick pathway for reasons that are unclear. The tachycardia circuit could seldom contain the left posterior nodal extension (see later). The fast pathway is less properly outlined from an anatomical and structural standpoint. However, the nature of the proximal hyperlink between these pathways is unclear, and the existence of an upper widespread pathway continues to be a matter of controversy (Tables 17-2 and 17-3). The earliest atrial activation site throughout retrograde conduction over the fast pathway is within the anterior apex of the triangle of Koch at the identical web site recording the proximal His potential (although some research confirmed the earliest site of atrial activation occurring within the anterior interatrial septum above the tendon of Todaro, outdoors the triangle of Koch), whereas that over the gradual pathway is in the base of the triangle of Koch. The proximal atrial insertions of the quick and slow pathways are anatomically distinct throughout retrograde conduction, and a number of other necessary functional variations exist between the two pathways (Table 17-4). Whether these pathways symbolize discrete anatomically distinct circuits or are functionally present due to nonuniform anisotropy is unclear. It may be possible for each the leftward and rightward extensions, both collectively or separately, to participate in nodal reentry. Factors that contribute to the therapeutic decision embody the frequency and period of tachycardia, tolerance of symptoms, the effectiveness and tolerance of antiarrhythmic medication, the necessity for lifelong drug remedy, and the presence of concomitant structural heart disease. Because of its excessive efficacy (greater than 95%) and low incidence of problems, catheter ablation has become the popular therapy over long-term pharmacological remedy and may be provided as an initial therapeutic choice. This is characterised as regular fast tachycardia of abrupt onset and termination. Rapid ventricular charges can be related to complaints of dyspnea, weakness, angina, or even frank syncope and may at times be disabling. Patients often learn to use certain maneuvers corresponding to carotid sinus therapeutic massage or the Valsalva maneuver to terminate the arrhythmia, though many require pharmacological remedy. The physical examination correlate of this phenomenon is continuous pulsing cannon A waves in the jugular venous waveform (described because the "frog" sign). The earliest retrograde atrial activation is normally in the inferoposterior part of the triangle of Koch. Slow pathways with longer conduction instances have a extra inferior location within the triangle of Koch. A jump in the A2-H2 (or H1-H2) interval of 50 milliseconds or extra in response to a 10-millisecond shortening of either the A1-A2 interval. At the break in the curves, atrioventricular nodal reentrant tachycardia is initiated. The last paced impulse, nevertheless, conducts anterogradely over both the quick (red arrow) and slow (blue arrow) pathways, resulting in two His bundle and ventricular responses. However, the wavefront conducting down the fast pathway reaches the distal junction of the two pathways earlier than the impulse conducting down the slow pathway, and, subsequently, it conducts retrogradely up the slow pathway to collide with the impulse conducting anterogradely down that pathway. The 1:2 response should be differentiated from pseudo�simultaneous fast and slow pathway conduction, which is a a lot more frequent phenomenon throughout speedy atrial pacing. Thus, the last paced atrial impulse is adopted by two His potentials and two ventricular complexes. The last occasion ends in anterograde postdepolarization refractoriness, which would consequently make the fast pathway refractory to the wavefront invading it within the retrograde direction. The commonest mechanism entails retrograde block of the ventricular stimulus within the gradual pathway and retrograde conduction up the quick pathway, followed by anterograde conduction down the slow pathway. Subsequently, the wave of atrial activation propagates radially cephalad and laterally to activate both atria. In truth, the narrowest P wave throughout any arrhythmia is seen when the atrial activation begins at the apex of the triangle of Koch. Moreover, Wenckebach-type block can happen within the decrease common pathway and can lead to a altering relationship between the His potential and the atrial electrogram. In the remaining patients, the His potential can range from being rudimentary to massive in amplitude. Note the adjustments within the H-H and V-V intervals previous similar adjustments in the A-A interval. This can occur even with out affecting the timing of the subsequent atrial activation, if conduction delay occurs only within the lower common pathway but not within the slow pathway. In truth, the anterograde His potential (H) is visualized shortly after the pacing artifact (arrow), occurring on the anticipated timing (the tachycardia cycle size is indicated by the red lines). For this reason, care ought to be taken not to measure unstable intervals immediately after ventricular pacing. Under such circumstances, constant fusion during entrainment is nearly impossible (unless a second connection exists between the atria and ventricles; i. The main benefit of this method is its independence of tachycardia continuation after cessation of pacing. This target can be defined by considered one of two approaches: a purely anatomical approach and an electroanatomical method. Rarely, profitable gradual pathway ablation may require an application of vitality on the left aspect of the posterior septum, alongside the mitral annulus. These potentials have been utilized by some to define the site of the sluggish pathway inside the triangle of Koch, and so they can be utilized successfully as a guide to target ablation. Whether they characterize nodal tissue activation, anisotropic conduction by way of muscle bundles in various websites in the triangle of Koch, or a mix of both is unclear. The electrogram morphology of the gradual potentials has been variously described as sharp and fast (representing the atrial connection to the sluggish pathway; see. Despite these observations, the chance of recording putative gradual potentials at the website of efficient gradual ablation is more than 90%. Note the sharp (blue arrow, left decrease panel) and broad (red arrow, proper decrease panel) potentials recorded between the atrial and ventricular electrograms on the ablation websites.
Female Cialis: 20 mg, 10 mg
Discount female cialis 10mg with mastercardAt this time the primary floor localized rhythm with ictal transformation is seen 3 menstrual cycles in 1 month discount female cialis 10 mg fast delivery. Basal electrodes women's health specialists zanesville ohio cheap female cialis 10 mg with visa, such because the sphenoidal or modified Maudsley system are used to present lower protection menstruation explained purchase female cialis 10mg online. Early switch of hippocampal seizures can lead to pregnancy and diarrhea generic female cialis 10mg without a prescription incorrect scalp lateralization, and sometimes from subdural recordings. Poorer operative outcomes are seen within the presence of multifocal or generalized discharges, fast swap of seizure sides or the presence of average to severe studying difficulties. Other authors have normally recorded complications in about 1% of procedures (21�23). Historically, it fashioned some 80% of instances, although worldwide the dysfunction now seems much less widespread. The electroclinical options have been extensively reviewed (24) and solely those issues of explicit relevance to presurgical evaluation are discussed right here (see Box 31. Unfortunately the bottom line of electrodes in the 10-20 system is larger, running from the inion and nasion. Basal electrodes, such as the inferior frontal in the Maudsley system, or the superficial or deep sphenoidal have been extensively used to document from this space. However, they characteristically have a wide field spreading from the prefrontal to the occipital contacts (26). The occurrence of a mid- or posterior temporal most is more commonly related to a lateral focus. Because of the wide electrical subject, reference recordings could also be extra helpful than bipolar derivations. During the aura, intracranial recording exhibits the onset of low voltage fast exercise in the hippocampus. The seizure could cease at this level or the affected person then loses awareness and has a motionless stare. Around the time of loss of consciousness the hippocampal quick activity increases in amplitude and slows to the theta range, taking over a rhythmic sharpened appearance. Spikes and slowing are seen, although usually remaining maximal in the temporal lobe. If the ictal discharges unfold over the hemisphere the contralateral arm could come up with the pinnacle turned in the course of it and clonic jerks appear because the seizure turns into secondarily generalized. A hanging function of medial temporal epilepsy is that the seizures may switch sides. Small operative collection recommend that, if these criteria are rigorously adopted, early outcomes seem to not be not dissimilar from unilateral hippocampal sclerosis. Some have reported an elevated incidence of reminiscence deficits after leftsided operations, again as seen with unilateral pathology. Removal of non-scarred structures, especially from the dominant hemisphere, may have higher risks for reminiscence. Most centres carry out an en bloc anterior temporal resection as advocated by Falconer, or a modified resection after the work of Spencer, which leaves extra lateral temporal neocortex (30). Lateral temporal epilepsy, insular, and opercular seizures the presence of unformed auditory auras or early ictal dysphasia, suggests involvement of the superior temporal gyrus. Psychic auras with illusions or hallucinations suggest involvement of posterior affiliation areas, while extreme salivation, epigastric, and different autonomic auras are seen with insular seizures. The frontal operculum overlaying the sylvian fissure could produce motor seizures of the face and tongue, and speech arrest whereas posteriorly the second sensory area may give rise to intensive hemisensory disturbances and possibly pain. Pathology outdoors of the temporal lobe, so known as twin pathology, occurs in around 10% of circumstances (32). More strips may be directed in the course of different sites relying on imaging and electroclinical findings. During this time a series of objects and words are presented and memorized over about 5 min. It is necessary to emphasize that the reminiscence function and integrity of the hippocampus contralateral to the side of injection is examined. The solely operation that will be carried out is elimination of the scarred facet so that earlier than depth recording an amytal test is performed to show that the side opposite the lesion is ready to assist memory. Neuropsychology and amytal testing are wanted to present that the temporal lobes help memory. A technetium labelled pharmaceutical is injected usually within around 30 s of seizure onset, which is taken up in the brain in proportion to blood flow. It stays fixed for a period of hours and imaging is done with a rotating gamma digicam producing tomographic 364 (A) (B). Complex partial seizures with a visual aura and left hippocampal sclerosis and no other lesion. The deepest contacts (Channel 8, contact 1) of the strip labelled mid temporal lies near the left hippocampus. Second arrow, build-up of rhythmic spikes in the deepest contacts of the mid temporal electrode, near to hippocampus. Ictal exercise is now in the lateral, superficial contacts of the mid- and posterior temporal strips, once more with little involvement of the occipital electrodes. Note some sharp waves over the deepest mid temporal strip, but no distinguished hippocampal spread. Appropriate adjustments are seen in some 70�80% of instances of temporal lobe epilepsy (39). It produces data useful to presurgical analysis in around 30% of sufferers (40,41). It requires considerable organization to arrange and late injections can be misleading because of seizure spread. There is lack of the traditional layered structure, thickening of the cortex and loss of the grey white junction. Unlike tumours or scars, that presumably produce seizures by an impact on surrounding neurons, cortical dysplasia is inherently epileptogenic (46). Arrow shows brief burst of quick activity and a decrement within the deepest contact of proper anterior hippocampal/amygdala electrode followed by activity in the subsequent hippocampal depth (blue channels). Note the main seizure type, advanced partial seizures arises from the non-scarred hippocampus. This might explain the high seizure frequency and tendency to bouts of serial seizures and standing epilepticus seen in frontal epilepsy. The lesions are often fairly circumscribed, which makes them open to resection and they typically occur in folks with regular growth and well preserved cognition. They also appear to have a predilection for the depths of cerebral sulci and for areas around the central and sylvian fissures, overlapping with eloquent cortex (see Box 31. Frontal seizures are said to have a rapid unfold and a tendency to become shortly generalized; circumstances as a end result of focal cortical dysplasia, nonetheless, usually have a protracted aura and extra prolonged onsets. The epileptogenic space is usually larger than the lesion and resection should be guided by intra or extraoperative corticography.
Generic female cialis 10mg fast deliveryIn addition menstruation with large fleshy clots cheap 20 mg female cialis with visa, the 3-D image could be clipped with a customizable cutting airplane menstruation visceral fat purchase female cialis 20 mg with mastercard, to allow inside (endoscopic) views 8 menopause myths buy female cialis 20mg on-line. Moreover menstrual like cramping in late pregnancy quality female cialis 10mg, tags can be positioned on the floor of the registered 3-D image to mark ablation websites and other websites of interest. The real-time update of the catheter tip location and the marking of ablation lesions on the detailed 3-D image can doubtlessly enhance the quality of lesion units, reduce issues, and shorten procedure and fluoroscopy times. This scenario is confounded by the inevitable imperfection of the created virtual geometry of the cardiac chamber. These elements can impede the clinical utility of picture integration in roughly 25% of patients. The twenty first century has additionally seen the speedy improvement of integrated, anatomy-based mapping and ablation. This progress has been driven by a realization of each the critical coupling and dependence of arrhythmias on their underlying anatomy and the limitations of surrogate geometries of up to date mapping systems for reflecting that anatomy. However, the success of this strategy is primarily dependent on the accuracy of the picture integration course of. Even if the 3-D cardiac chamber image supplies an accurate model of a matched section of the chamber quantity on the time of the procedure, it must be accurately registered to the procedural chamber orientation to present reliable navigation. Current registration algorithms depend on correct catheter geometry; this requires an accurate update of 3-D coordinates of the catheter tip, as recorded and displayed on the computer picture. The precise location of the initial fiducial factors picked by the operator using fluoroscopy in the 3-D space could additionally be misleading. Movement of the catheter tip is complicated and is affected by wall movement and respiration. Additionally, catheter tip stress could cause tenting of the chamber wall, thereby distorting the chamber geometry. Catheter contact can range with the type of ablation catheter and introducer sheath, in addition to the diploma of regional wall movement; for example, the mitral annulus and appendage are extra dynamic than the posterior atrial wall. The registration technique has also varied, including three- or fourpoint registration or floor registration. Alternatively, a single level and the floor have been used as nicely (visual alignment). The C-arc x-ray system is rotated around the patient over 240 degrees to create a circumferential run of many publicity images of the region of interest distributed over the 360-degree (or similar) trajectory. The esophagus may be opacified using a barium paste prior to the image acquisition. The latest model of the software allows registration of the segmented 3-D volume on a reside fluoroscopy screen. In addition, this technique is technically easier and doubtlessly safer than extra downstream injections. Given such complexities, this method could additionally be harder to implement in clinical follow. The x-ray acquisition pace is 30 frames per second, which results in a complete of 120 frames within the rotational run. The patient is instructed to cease respiration instantly previous to initiation of the rotational run to stop respiratory motion of the construction of curiosity and insufficient reconstruction. With registration of the 3-D volume, all movements of the C-arm are translated into the suitable rotation or shift, thus maintaining the connection between the fluoroscopic coronary heart shadow and reconstructed picture unchanged. However, shifting the x-ray desk is commonly required after 3-D rotational angiography, especially given the truth that intracardiac catheters ought to be placed only after the rotational run to prevent artifacts. Therefore, registration is often needed as a result of, in its present iteration, overlay movement is linked only to C-arm rotation and to not x-ray desk repositioning. Ablation points can be marked on the overlaid 3-D rotational angiography mannequin to track the completeness of lesions. In addition, the technique is delicate to affected person actions in the course of the study period. One shortfall of 3-D rotational angiography is the absence of streaming electrogram data. These embody incorporation of respiratory and cardiac movement compensation and the ability to show electrogram data on the 3-D shell (activation timing, scar and voltage maps, and dominant frequency). Interval modifications in volume status, respiratory phase, and cardiac rhythm can end result in temporal changes within the measurement and placement of the anatomical constructions between the time of image acquisition and the registration process. More generally, cardiac mapping is performed with catheters launched percutaneously into the heart chambers that sequentially document the endocardial electrograms with the aim of correlating native electrogram to cardiac anatomy. The alternative of a particular mapping system for a selected 6 interventional case is formed by the significance of a particular attribute in the mapping course of. With these arrhythmias, the noncontact mapping array works well, although the maps can be filter frequency dependent. Substrate mapping, corresponding to scar or voltage mapping, is a helpful various to noncontact mapping. In some instances, the selection of mapping system is decided by the skill and expertise of the operator. The noncontact system requires more steps within the creation of user-friendly working geometry. Each of those techniques is at present in the improvement stage, and their numerous capabilities can change considerably over the subsequent several years. At most, such techniques must be used as an adjunctive device to facilitate mapping and ablation. The operator should perceive the benefits and shortcomings of each system and will acknowledge that these methods may be misleading and complicated and provide inaccurate information because of both incorrect data acquisition or inherent limitations of the technology. Esato M, Hindricks G, Sommer P, et al: Color-coded three-dimensional entrainment mapping for analysis and remedy of atrial macroreentrant tachycardia, Heart Rhythm 6:349� 358, 2009. Pappone C, Vicedomini G, Manguso F, et al: Robotic magnetic navigation for atrial fibrillation ablation, J Am Coll Cardiol forty seven:1390�1400, 2006. Haghjoo M, Hindricks G, Bode K, et al: Initial scientific experience with the model new irrigated tip magnetic catheter for ablation of scar-related sustained ventricular tachycardia: a small case collection, J Cardiovasc Electrophysiol 20:935�939, 2009. Vollmann D, Luthje L, Seegers J, et al: Remote magnetic catheter navigation for cavotricuspid isthmus ablation in sufferers with common-type atrial flutter, Circ Arrhythm Electrophysiol 2:603�610, 2009. Zhang X, Ramachandra I, Liu Z, et al: Noninvasive three-dimensional electrocardiographic imaging of ventricular activation sequence, Am J Physiol Heart Circ Physiol 289:H2724� H2732, 2005. Sra J, Ratnakumar S: Cardiac image registration of the left atrium and pulmonary veins, Heart Rhythm 5:609�617, 2008. Sanders P, Hocini M, Jais P, et al: Characterization of focal atrial tachycardia using highdensity mapping, J Am Coll Cardiol 46:2088�2099, 2005. Schilling R, Friedman P, Stanton M: Mathematical reconstruction of endocardial potentials with non-contact multielectrode array, In Field medical training guide, St. Sivagangabalan G, Pouliopoulos J, Huang K, et al: Comparison of electroanatomic contact and noncontact mapping of ventricular scar in a postinfarct ovine model with intramural needle electrode recording and histological validation, Circ Arrhythm Electrophysiol 1:363� 369, 2008. Soejima K: How to troubleshoot the electroanatomic map, Heart Rhythm 7:999�1003, 2010.
Opuntia Ficus-Indica (Prickly Pear Cactus). Female Cialis. - Diabetes. Some forms of prickly pear cactus seem to lower blood sugar levels in people who have type 2 diabetes.
- Dosing considerations for Prickly Pear Cactus.
- What is Prickly Pear Cactus?
- What other names is Prickly Pear Cactus known by?
- Hangover. Taking prickly pear cactus before drinking alcohol might reduce some symptoms of hangover the next day.
- Are there any interactions with medications?
- How does Prickly Pear Cactus work?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96848
Generic 10 mg female cialis amexIn a current 30-year study of 185 sufferers sixty five years of age and older menstruation black blood cheap female cialis 10 mg on line, the prognosis of community-acquired bacterial meningitis was tougher because of the absence of characteristic meningeal signs355; in contrast with adult sufferers younger than sixty five years of age menopause weight gain solutions buy generic female cialis 10 mg, older sufferers confirmed larger neurologic severity breast cancer karyotype buy 20mg female cialis otc, with a high number presenting with coma on admission pregnancy hormone levels buy female cialis 10 mg otc, seizures, and hemiparesis. In patients with head trauma, the symptoms and signs of meningitis could also be present because of the underlying harm and not meningitis. The prognosis of bacterial meningitis in neutropenic sufferers requires a high index of suspicion, because symptoms and signs may initially be subtle because of the impaired ability of the affected person to mount a subarachnoid space inflammatory response. A particular etiologic analysis in sufferers with bacterial meningitis could also be advised by certain signs or indicators. Early in the middle of illness, the rash is often erythematous and macular, but it shortly evolves into a petechial phase with further coalescence into a purpuric form. The rash usually matures quickly, with new petechial lesions showing in the course of the bodily examination. In one evaluation of the medical manifestations of 255 sufferers with acute meningococcal meningitis,356 a petechial rash was observed in three fourths of the sufferers; the rash was more commonly seen in kids and adults youthful than 30 years (81%) than in patients 30 years and older (62%). However, others have noticed a rash to be present in only as a lot as 26% of instances and (if present) is extra prone to be scanty or extra atypical than that seen in sufferers with meningococcal septicemia. In a potential examine of 30 adults with Listeria meningitis, the most typical scientific manifestations were headache (88%), nausea (83%), fever higher than 38� C (100. Focal abnormalities such as hemiplegia, aphasia, and psychological standing changes were seen less generally. Meningovascular syphilis is clinically distinguished from syphilitic meningitis temporally and on the basis of focal neurologic findings on account of focal syphilitic arteritis, which nearly all the time occurs in association with meningeal inflammation. Focal deficits, which reflect episodes of ischemia in areas of the mind by concerned blood vessels (usually within the distribution of the center cerebral artery), can also occur; if untreated, these deficits may progress to a stroke syndrome with attendant irreversible neurologic deficits. Because of early involvement of the olfactory area, early symptoms of irregular odor or taste may be reported. Confusion, irritability, and restlessness progress to delirium, stupor, and, lastly, coma. Death in untreated patients typically happens within 2 to 3 days from the onset of symptoms. However, longer durations of sickness have also been reported (range, 5 to 18 months). Symptoms of meningitis begin 6 to 30 days (typically 1 to 2 weeks) after the ingestion of raw mollusks or different sources of the parasite. In a current outbreak in 12 people with a typical foodborne exposure in Jamaica, the imply incubation period was eleven days (range, 6 to 31 days). Visual disturbances or photophobia had been seen in 92% of patients, and nuchal rigidity or neck pain and fatigue were current in 80% of instances. In a review of 18 instances in Hawaii from 2001 to 2005, 94% of sufferers had headache and 65% had sensory signs consisting of paresthesias, hyperesthesias, and/or numbness; those signs lasted a median of 17 and fifty five days, respectively. Photophobia, nausea, and vomiting are intermediate in frequency between headache and neck stiffness. About two thirds of sufferers have accompanying systemic symptoms, including malaise, fatigue, myalgias, fever, arthralgias, and involuntary weight reduction. Patients sometimes expertise recurrent assaults of meningeal symptoms lasting several weeks and alternating with comparable durations of milder symptoms. Facial nerve palsy is the most typical (80% to 90%) of the cranial nerve palsies total and occurs with fast onset (often in 1 to 2 days), frequently accompanied by slight ipsilateral facial numbness or tingling or ipsilateral ear or jaw ache. The facial palsy is bilateral in 30% to 70% of instances, though the 2 sides are affected asynchronously in most cases. Although isolation of a nonpolio enterovirus from the throat or rectum of a patient with aseptic meningitis is suggestive of an etiologic analysis, the imply shedding durations from those websites after infection are 1 week and several weeks, respectively. Follow-up acute and convalescent serologic testing for the precise isolated strain could affirm the etiologic diagnosis. Complement fixation and hemagglutination inhibition on serum specimens are essentially the most reliable serologic tests for the diagnosis of mumps. Testing of paired acute and convalescent sera ought to demonstrate a diagnostic fourfold rise in mumps antibody titer. Mumps virus could be isolated from saliva from just about all patients with mumps parotitis and may also be recovered in urine for up to 2 weeks after the onset of illness. In just about all circumstances, the opening stress is elevated, with values over 600 mm H2O suggesting the presence of cerebral edema, intracranial suppurative foci, or communicating hydrocephalus. The clinical utility of the Gram stain additionally is dependent upon the bacterial pathogen384: bacteria have been observed in 90% of instances of meningitis brought on by S. False-positive results have occasionally resulted in unnecessary remedy and prolonged hospitalization. A mixture of scientific manifestations, with or without test outcomes, has been assessed to develop fashions in an try and precisely predict the probability of bacterial meningitis compared with other potential causes (most often viruses). Despite the positive outcomes of this meta-analysis and different studies, clinical judgment ought to proceed to be used in choices about the need for administration of empirical remedy in sufferers with suspected bacterial meningitis. Prediction models may be most helpful in doubtful instances, once they can be utilized to suggest a reconsideration of the analysis. Several proteins have been examined for their usefulness within the analysis of acute bacterial meningitis. In one study, heparin-binding protein had a sensitivity of 100 percent and specificity of 99. Further large-scale studies are wanted to determine the sensitivity and specificity of this system. The greatest at present out there laboratory test for the prognosis of Lyme illness is demonstration of particular serum antibody to B. False-positive reactions have been reported in sufferers with rheumatoid arthritis, Rocky Mountain spotted fever, infectious mononucleosis, tuberculous meningitis, leptospirosis, yaws, syphilis, and relapsing fever,one hundred sixty though excessive titers of cross-reacting IgG antibodies have been detected solely in patients with syphilis or relapsing fever. False-negative outcomes may be obtained from an unreliable assay, early infection, or early antibiotic use, which may blunt the traditional humoral immune response. It is presently beneficial that when the pretest chance of Lyme illness is 0. In addition, intrathecal synthesis of antibodies can persist for several months to a number of years after successful diagnosis. After their dying, trophozoites could be demonstrated by mild or electron microscopy of brain tissue. Many authorities would continue empirical antimicrobial therapy (see Table 89-12) pending organism identification. Once the infecting meningeal pathogen is isolated and susceptibility testing results recognized, antimicrobial remedy may be modified for optimum treatment (Table 89-13). The inflammatory response induced by either reside pneumococci or pneumococcal cell wall was lowered by agents.
20 mg female cialis amexEntrainment with concealed fusion means that the pacing web site is within a protected isthmus inside or outdoors women's health center heritage valley 10mg female cialis with mastercard, however connected to pregnancy early symptoms order 20mg female cialis with visa, the reentrant circuit womens health 60 years generic 20 mg female cialis otc. In this example women's health clinic melbourne cbd discount 20mg female cialis with visa, transient entrainment is achieved when the orthodromically directed stimulated wavefront resets the tachycardia, but the antidromically directed stimulated wavefront collides with the tachycardia wavefront in or near the reentry circuit and fails to exit the slow conduction zone. Compared with the intrinsic tachycardia, this antidromic capture might end in earlier intracardiac recordings from websites located adjoining to the pacing area. At websites distant from the circuit, stimulated wavefronts propagate to the circuit, then by way of the circuit, and finally again to the pacing website. In areas of scar, electrode catheters usually document multiple potentials separated in time, some of which are far-field potentials that end result from depolarization of adjoining myocardium. The near-field potential is obscured by seize during pacing, whereas far-field potentials may be undisturbed throughout pacing. On the other hand, pacing websites outdoors the reentrant circuit have an electrogram-exit interval considerably (more than 20 milliseconds) shorter than the stimulus-exit interval. However, the electrogram-exit interval may not be precisely equal to the stimulus-exit interval at sites inside the reentrant circuit. One potential issue is decremental conduction properties of the zone of gradual conduction that produce lengthening of the stimulus-exit interval throughout pacing; nevertheless, this appears to happen not often. Additionally, failure of the recording electrodes to detect low-amplitude depolarizations at the pacing website can account for a mismatch of the stimulus-exit and electrogram-exit intervals. Potential ablation websites are sought by pacing at websites thought to be associated to the reentrant circuit, based mostly on different mapping modalities, similar to activation mapping and pace mapping. However, proof of entrainment is greatest obtained by pacing from websites distant from the circuit, which most readily reveal fusion. Pacing ought to be continued for an extended sufficient duration to allow for entrainment; short pacing trains are usually not helpful. Features of entrainment when pacing from totally different sites are listed in Table 5-1 (see also. Furthermore, makes an attempt at entrainment can result in termination, acceleration, or transformation of the index tachycardia into a unique one, thus making additional mapping challenging. Bipolar pacing at comparatively excessive stimulus strengths used during entrainment can result in capture of an area larger than the local space. This requirement is normally satisfied by pacing from electrodes 1 and three and recording from electrodes 2 and 4 of the mapping catheter. There are differences, albeit slight, of the area from which the second and fourth electrodes document as compared with the first and third. The bipolar pacing technique has the potential for anodal contribution to local seize. The total space captured by the pacing stimulus can exceed the local area, particularly when excessive currents (more than 10 mA) are required for stimulation. Far-field electrical signals generated by depolarization of adjacent tissue may cause false-positive entrainment criteria at some sites. Achievement of entrainment of tachycardia establishes a reentrant mechanism of that tachycardia and excludes triggered activity and irregular automaticity as potential mechanisms. Entrainment can also be used to estimate how far the reentrant circuit is from the pacing site qualitatively. Focal ablation of all websites outlined as throughout the reentrant circuit may not end in a remedy of reentrant tachycardia.
[newline]Cure requires ablation of an isthmus bordered by limitations on both facet, which is crucial to the reentrant circuit. Differences in the morphology between pacing and spontaneous tachycardia in a single lead could be crucial. Unsuccessful ablation can result, partially, from subjective differences in the opinion of a tempo map match to the medical tachycardia. It has been suggested that an automatic objective interpretation can have some advantage to qualitative interpretation. It is important to observe that such subtle variations in multiple leads may be reflected in a single quantitative quantity. This works well when pacing is carried out throughout tachycardia, at which era wavefront propagation is constrained in a single path via a corridor bounded by limitations that may be anatomically or functionally determined. However, tempo mapping on the similar websites during sinus rhythm can yield different outcomes as a end result of the limitations could not exist then, the preferential path of propagation will not be the same as during tachycardia, or each. Delivery of a vesicular extrastimulus (or a practice of ventricular pacing) to advance ventricular activation and repolarization can enable cautious distinction of the P wave onset and morphology. Pace mapping is ideally performed with unipolar stimuli (10 mA, 2 milliseconds) from the distal electrode of the mapping catheter (cathode) and an electrode within the inferior vena cava (anode), or with closely spaced bipolar pacing at twice diastolic threshold to eliminate far-field stimulation results. The greater is the degree of concordance between the morphology throughout pacing and tachycardia, the closer the catheter shall be to the positioning of origin of the tachycardia. Clinical Implications Pace mapping is typically used to confirm the results of activation mapping. It can be utilized to focus preliminary mapping efforts to areas more likely to include the reentrant circuit exit or abnormal conduction, but it is probably not sufficiently particular or delicate to be the only real guide for ablation. Spatial resolution deteriorates with wide electrodes, bipolar stimulation, and pacing at pathological areas. Spatial decision worsens with bipolar stimulation by inducing electrical seize at both electrodes with variable contribution of the proximal electrode (generally anode) to depolarization. Sosa E, Scanavacca M: Epicardial mapping and ablation methods to control ventricular tachycardia, J Cardiovasc Electrophysiol 16:449�452, 2005. Esato M, Hindricks G, Sommer P, et al: Color-coded three-dimensional entrainment mapping for evaluation and therapy of atrial macroreentrant tachycardia, Heart Rhythm 6: 349�358, 2009. This stems partially from the limitations of fluoroscopy and traditional catheter-based mapping methods to localize arrhythmogenic substrates which are removed from fluoroscopic landmarks and the dearth of characteristic electrographic patterns. These newer methods are aimed toward bettering the decision, three-dimensional (3-D) spatial localization, and rapidity of acquisition of cardiac activation maps. These systems use novel approaches to decide the 3-D location of the mapping catheter precisely, and native electrograms are acquired using conventional, well-established methods. The software of these numerous strategies for mapping of particular arrhythmias is described elsewhere in this text, as are the details of the prognosis, mapping, and treatment of particular arrhythmias. The basket catheter consists of an open-lumen catheter shaft with a collapsible, basket-shaped, distal end. Currently, baskets are composed of 64 platinum-iridium ring electrodes mounted on eight equidistant, flexible, self-expanding nitinol splines (metallic arms; see. Each spline is recognized by a letter (from A to H) and every electrode by a quantity (distal 1 to proximal 8). The basket catheter is constructed of a superelastic material to enable passive deployment of the array catheter and optimize endocardial contact. The measurement of the basket catheter used is dependent upon the scale of the chamber to be mapped, and it requires antecedent analysis (usually by echocardiogram) to ensure proper measurement choice. The Astronomer is used for navigation with the ablationmapping catheter inside the basket catheter. This system consists of a switching-locating system and a laptop laptop with proprietary software program.
Discount 20 mg female cialis mastercardThe internet effect for a scalp recording is that each correspond to surface negativity breast cancer 5k order female cialis 20mg line. Action potentials in giant cortical neurons normally are initiated at or near the axon initial segment menstruation under graviditet female cialis 20 mg cheap, a specialized construction at the junction between the cell body women's health clinic eating disorders discount female cialis 10 mg, or soma 4 menstrual stages buy 20mg female cialis with mastercard, and the axon. In some circumstances, additionally they propagate up the dendrites as back-propagating action potentials. The longer durations of post-synaptic currents additionally increases the chance of summation of synaptic currents generated by massive numbers of neurons receiving comparable inputs. Microwires are significantly good for recording motion potentials as a end result of their frequency response characteristics make them most effective at detecting the quickly altering voltages discovered during transient motion potentials. Clusters of microwires could be inserted down medical depth electrodes, and have led to thrilling work on the correlations of the firing of particular person neurons within the temporal lobe with ideas, as an example, where an individual or an object triggers a response no matter whether or not the stimulus is a picture, a written word or perhaps a spoken word (9). During the late twentieth and early twenty-first centuries, know-how developed to permit the manufacture of multi-electrode arrays comprising giant numbers of penetrating microelectrodes. They have been inserted through or beneath subdural mat electrodes throughout presurgical evaluation of individuals with medically intractable epilepsy. Early reports confirmed the sooner work that neurons in general reduced their firing rates during electrographic seizures (10). Experimental evidence from rodent mind slices in vitro instructed that this was because of synaptic inhibition constraining synaptic excitation in tissue that obtained inputs from the more focal region of neuronal hyperactivity (12,13). If the cause of the epilepsy is the pathologically accelerated firing of very native areas of cortex then it will seem to follow that elimination of the tissue that begins the pathological firing should stop seizures starting. However, less invasive recording methods might detect consequences of high-frequency neuronal firing. Perhaps the obvious is high-frequency oscillations, that are defined by being sooner than frequencies of 100�300 Hz depending on recording situations and locations. In experimental contexts high-frequency oscillations may be generated by action potentials in the absence of synaptic activity (14), the place their spatial extent of co-firing clusters of neurons was a fraction of a millimetre. This can explain why microelectrodes detect excessive frequency oscillations than traditional medical depth or sub-dural contacts (15). The distinction between synaptic and action potentials in scientific signals is greater than an intellectual distraction. There already is proof that profitable outcomes for surgical resection of epileptic foci increase with the quantity of tissue producing high-frequency oscillations removed (16). Feedforward inhibition contributes to the control of epileptiform propagation pace. Neuronal firing in human epileptic cortex: the ins and outs of synchrony throughout seizures. High-frequency network activity, world increase in neuronal exercise and synchrony growth precede epileptic seizures in vitro. Role of ictal baseline shifts and ictal highfrequency oscillations in stereo-electroencephalography evaluation of mesial temporal lobe seizures. Intracranially recorded ictal direct present shifts may precede high frequency oscillations in human epilepsy. Perhaps the clearest example comes from gradual potentials recorded with intracranial electrodes throughout seizures (17�19). Together with high-frequency oscillations, slow potentials could provide more exact localization of epileptic foci. The most simple thought is that the negative potential shift is expounded to the removing of K+ ions from the extracellular fluid. Conclusions Movement of ions across neuronal surface membranes are crucial to the signalling and computational processing of cortical neurons. Inputs to neurons are offered by synapses, utilizing quite so much of neurotransmitters, mainly onto the dendrites, somata, and axon initial segments. The many inputs every neuron receives are built-in to determine whether or not or not the neuron will set off an action potential, which transmits the neurons output to its target neurons. All these membrane currents produce extracellular currents and related voltage gradients. The laminar construction of the cortex leads to the summation of the small currents produced by individual neurons, as long as giant numbers of neurons obtain similar synaptic inputs, as occurs through the rhythmic and/or synchronous actions discovered during epileptic seizures, sleep, and evoked potentials. These sort of summations lead to high current densities throughout the tissue resulting in substantial voltage gradients that might be recorded by way of the scalp. More invasive recordings can detect the firing of particular person neurons or small clusters of neurons. A quantitative description of membrane current and its utility to conduction and excitation in nerve. We present various primary concepts, together with quantity conduction, recording of electrical indicators, electrical stimulation and security, and aspects which are related within the digitization and post-processing of information. A drawback of extracellular recording is the unfold of extracellular currents that rely, in a fancy way, on the passive electrical properties. The medical neurophysiologist ought to always be conscious of these features to stop unjustified conclusions. Measuring in the extracellular area, mass activity, and quantity conduction in clinical neurophysiology Neurophysiological indicators are traditionally recorded in an area across the actual bioelectrical sources. For the central nervous system this has primarily to do with the relative inaccessibility of the related structures, i. Also, the danger of harm during the acquisition of neural indicators should be minimal. The peripheral neuromuscular system can bodily be approached by a recording electrode with relative ease, however one should realize that when an axon or a muscle fibre is penetrated by the relatively giant needle electrode, the cell membrane is broken, and the motion potential propagation is disrupted. Although the absence of entry to intracellular recordings may at first sight appear disadvantageous, extracellular recordings provide useful info at a worldwide level as it outcomes from synchronized activity of neural assemblies or axon bundles, which has been proven to be very helpful for diagnostic purposes. Of course, recording individual cell exercise provides diagnostic data, as well. Also, evaluation and explanatory models Moving and non-moving sources the basic source of electrical activity in the neurophysiology of the peripheral nervous system is the action potential, an nearly monophasic transient change in membrane voltage, with a period of 1�2 ms (see Chapters 1 and 4). In the primary case the source may be described bodily as a so-called present dipole. In the latter case the supply is a linear quadrupole, additionally indicated as a tripole (8,9). These two kinds of supply differ considerably in their capability to generate potentials at a distance in the above mentioned volume conduction. For the idealized case by which a dipole supply is embedded in an infinite and also homogenous volume conductor, which is biologically impossible, of course, fundamental physics states that the potential drops as 1/R 2 the place R is the space between the supply and measuring electrode. Such a possible component may be recorded over very long distances, even over the whole body. The best example of a dipole as a far-field generator is the center as a bioelectric supply. Extracellular recordings of propagating sources are basically triphasic because of the +/�/+ character of such sources. That also contributes to the fact that most measured activity comes from massive cell populations. The common precept of measuring electric potentials brought on by the move of ions in a fluid is to switch the ionic current and resulting potential to the movement of electrons within the metal electrode and wire related to the amplifier.
Generic female cialis 20 mgThe peak ratio is measured in at least 10 websites in each muscle to acquire consultant values womens health research cheap female cialis 10mg with amex. As the interference sample varies in numerous elements of the muscle women's health lose 10 pounds cheap 10mg female cialis free shipping, these 10 websites ought to be rigorously distributed in the muscle utilizing at least three insertions in every muscle (111 menstruation tiredness cheap 10mg female cialis amex,114) pregnancy facts purchase 20mg female cialis with visa. Reference material exists for the brachial biceps, abductor pollicis brevis, anterior tibial and medial vastus muscles (115). Reference material for the brachial biceps, extensor digitorum communis, quadriceps, and anterior tibial (120), orbicularis oculi and oris (205), and frontalis and mentalis muscles (139). Cloud technique (C) the force level had an affect on the sensitivity of the cloud method. The peak ratio is a quick method that can be carried out in 5�10 min for every muscle. Cloud evaluation in muscular tissues from patients with myopathy showed elevated variety of small segments, although the data factors had been usually inside the normal cloud of variety of small segments towards activity. In muscles from sufferers with Ratio of turns to amplitude the peak ratio is the maximum worth of the ratio of turns/s to mean amplitude obtained through the use of the imply amplitude per flip as an indicator of pressure (123). Mean amplitude can be substituted for drive, because it will increase linearly with pressure (114,one hundred fifteen,131). This level could additionally be reached at completely different pressure levels at different websites in the muscle, depending on the density of the motor items (133). Peak-ratio evaluation within the brachial biceps muscle of 25 patients with different sorts of myopathy showed an elevated peak ratio in 92%, and 84% had an elevated number of small time intervals lower than 1. The analysis of peak values of turns/s, imply amplitude and ratio was shown to be extra delicate than the cloud technique (95% versus 80%) (138). In 19 patients with myopathy, evaluation of the ratio of turns to mean amplitude in the anterior tibial muscle showed myopathic features in 68% (98). In the frontalis muscle of sufferers with myopathy, the ratio of turns to mean amplitude had a sensitivity of 62% and a specificity of 97% compared with controls and sufferers with neurogenic circumstances (140). This pattern suggests either random block of muscle fibres giving a myopathic picture, or functional block of the whole or a serious a half of the motor unit or changed recruitment sample giving a neurogenic picture (73,74) or an related myopathy (44). Disuse atrophy the disused quadriceps muscle examined at a pressure of 30% of mvc in sufferers having the leg immobilized for four weeks by a plaster solid confirmed decreased turns/s and mean amplitude consistent with practical loss of active motor models (146). Eight days later, when many of the pressure had been regained, turns/s and mean amplitude had been again regular. Such reversible motor dysfunction may be because of lack of sensory feedback affecting recruitment. The speedy reactivation of motor units is an example of the plasticity of the nervous system within the regulation of voluntary effort (146). Turns-amplitude analysis in neurogenic lesions In muscle tissue from sufferers with neurogenic disorders, peripheral sprouting is mirrored as increased length and excessive amplitude of particular person motor unit potentials. The large motor unit potentials are related to a decreased number of turns/s, elevated mean amplitude per flip, decreased ratio of turns to mean amplitude, and decreased number of small time intervals (68). This is reflected in a proportional improve in amplitude divided by turns/ s with rising fibre density (141). In neurogenic muscle, the loss of complete motor items ends in an additional decrease within the variety of turns/s. Cloud analysis of the brachial biceps in eight sufferers with motor neuron disorders confirmed that the upper centile amplitude was increased compared with controls in all sufferers. All sufferers had information factors above the cloud of higher centile amplitude towards activity, while the variety of small segments was decreased or normal. Peak ratio evaluation in 21 sufferers with neurogenic problems confirmed decreased peak ratio in 86% and decreased number of small time intervals less than 1. In one other study of the anterior tibial muscle of 21 sufferers with neurogenic problems, 81% had a neurogenic peak ratio evaluation (143). An enhance in ratio of turns to amplitude 6 weeks or extra after botulinum toxin therapy counsel a reversible, random loss of muscle fibres (149�151). This discovering accords with the decreased imply duration of individual motor unit potentials that occurs after therapy (152). The floor electrode has, nonetheless, an inherent drawback particularly with respect to diagnosis of patients with myopathy. A new methodology makes use of the application of excessive frequency, low depth alternating current to a limb and measures the ensuing surface voltages over a muscle given as impedance modifications, i. With respect to differentiation between myopathic and neurogenic muscle changes it seems that more research are needed (167). Fibrillation potentials may be seen both in important sickness neuropathy and in important illness myopathy. In order to differentiate between neuropathy and myopathy in these instances, a method using direct muscle stimulation was suggested (196,197). Thus, in myopathic muscle tissue the ratio between compound muscle action potential amplitude obtained by nerve stimulation and the motion potential obtained by direct muscle stimulation is excessive, as much as 1, while the ratio in neurogenic muscle tissue is small and will even be zero. Muscle fibre conduction velocity the conduction velocity of propagation alongside the muscle fibre has been determined throughout voluntary effort (15,183) and by stimulation (184). Only motor items recruited at weak effort are included and on average solely 4% of maximum (range 0�20%) could be analysed, i. Action potential parameters in regular human muscle and their dependence on bodily variables. Action potential parameters in normal human muscle and their physiological determinants. Muscle motion potentials in myopathies with special regard to progressive muscular dystrophy. Computer assisted on line measurement of motor unit potential parameters in human electromyography. Moreover, motor units recruited both at low effort and at greater effort are included within the analysis. The pitfalls are: Development of fatigue if too high an effort is performed for too long, and the rests between contractions are too brief. For instance, a contraction of up to 50% of maximum requires a 30-s pause to be able to keep away from fatigue. Both fatigue and sampling outside the muscle could mimic adjustments seen in a neurogenic lesion. What is preferable is dependent upon the disorder and the chosen technique of the examination. Intra-rater reliability of motor unit number estimation and quantitative motor unit evaluation in topics with amyotrophic lateral sclerosis. Comparison of typical and decomposition-enhanced spike triggered averaging techniques. The diagnostic yield of quantified electromyography and quantified muscle biopsy in neuromuscular issues. Simulation research on the motor unit potentials with satellite parts in amyotrophic lateral sclerosis and spinal muscle atrophy.
References - Tobias-Machado M, Correa WF, Reis LO, et al: Single-site video endoscopic inguinal lymphadenectomy: initial report, J Endourol 25(4):607n610, 2011.
- Westfall TC, Westfall DP: Adrenergic agonists and antagonists. In Brunton LL, Lazo JS, Parker KL, editors: Goodman and Gilmanis the pharmacological basis of therapeutics, New York and Chicago, 2006, McGraw-Hill, pp 237n296. Wheeler JS Jr, Robinson CJ, Culkin DJ, et al: Naloxone efficacy in bladder rehabilitation of spinal cord injury patients, J Urol 137:1201n1206, 1987.
- Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. Clin Infect Dis. 2005;41:1373-1406.
- Kohli P, et al. Statins and safety: can we finally be reassured? Lancet 2011;378(9808): 1980-1981.
- Landman, J., Venkatesh, R., Lee, D. I. et al. Combined percutaneous and retrograde approach to staghorn calculi with application of the ureteral access sheath to facilitate percutaneous nephrolithotomy. J Urol 2003;169:64-67.
|

