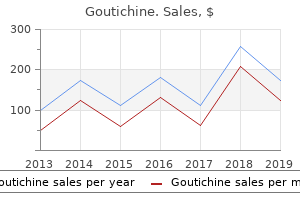
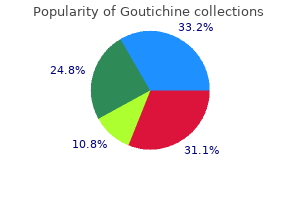
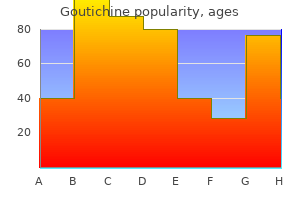
Goutichine
Mark Franklin, M.D. - Department of Anesthesiology
- Northwestern University Medical School
- Chicago, IL
Best goutichine 0.5 mgThe transverse sections are submitted in total for routine processing by way of neutral-buffered formalin (or equivalent alternative fixative) and sectioning as whole-mount sections (preferred) or after subdivision into two elements virus zapadnog nila generic 0.5 mg goutichine, 4 elements antibiotics for uti treatment goutichine 0.5 mg online, or extra antibiotic resistance nursing implications purchase 0.5mg goutichine overnight delivery, depending on the size of every slice antibiotics for sinus infection while pregnant goutichine 0.5mg lowest price. A document should be maintained in order that the prostate can be reconstructed at histologic evaluation. The percentages of Gleason major patterns four and 5, and the sum of main patterns four and 5 are estimated in 10% increments. Mucinous (colloid) carcinomas could have a variegated look and are sometimes softer than the adjacent prostate. Similar gross findings could additionally be attributable to tuberculosis, granulomatous prostatitis, and acute and chronic prostatitis. Microscopic Pathology Microscopically, most prostatic adenocarcinomas are composed of small acini organized in one or more patterns. Diagnosis depends on a combination of architectural and cytologic findings, and could also be aided by ancillary research similar to immunohistochemistry. Large firm yellow tumor mass is grossly visible on one side, but microscopic foci have been present throughout the peripheral zone bilaterally. The yellow colour is as a outcome of of abundant cytoplasmic lipid in tumor cells, which was confirmed histochemically. The acini in suspicious foci are usually small or medium, with irregular or elongate contours that stand in contrast with the graceful contours of normal prostatic acini. Variable acinar dimension is of worth, notably when there are small, irregular, abortive acini with primitive lumens. The arrangement of the acini is diagnostically helpful; malignant acini usually have an irregular haphazard arrangement, typically splitting or distorting muscle fibers in the stroma, with variable spacing between acini. The stroma incessantly contains young collagen that appears lightly eosinophilic, and desmoplasia may be prominent, though that is an uncommon and unreliable function when assessed in isolation. An understanding of the Gleason grading system is of value for interpretation of small foci due to its reliance on architectural patterns (see later). Enlarged nuclei are usually current in most malignant cells, and enlarged nucleoli are current in many. Every cell has a nucleolus, so one searches for "prominent" nucleoli, which are at least 1. Compressed stromal fibroblasts may mimic basal cells but are often only seen focally at the periphery of acini. An intact basal cell layer is current surrounding benign acini, whereas carcinoma totally lacks a basal cell layer. Sometimes, small foci of adenocarcinoma cluster round bigger acini that have intact basal cell layers, compounding the difficulty. Triple immunostain (not shown) revealed racemase staining, in addition to absence of p63 and keratin 34E12 staining. Irregular free cluster of small to intermediate acini, together with a couple of with foamy cytoplasm (bottom) that stand in contrast with the adjoining benign acini (B and C). This was recognized as "foamy gland prostatic intraepithelial neoplasia" at one other medical heart with out obtaining immunostains. This immunoprofile effectively excludes prostatic intraepithelial neoplasia from consideration and, in combination with the architectural abnormalities, is diagnostic of adenocarcinoma (Gleason 3 + three � 6) with focal foamy gland sample. Proteinaceous secretions are often present in affiliation with crystalloids and corpora amylacea. The focus of adenocarcinoma (left) shows marked nuclear and nucleolar enlargement compared with adjoining benign epithelium (right). Collagenous micronodules are formed by subepithelial accumulations of fragmented collagen fibers, presumably associated to the digestion by collagenase produced by prostatic adenocarcinoma cells. The time period mucinous fibroplasia has been erroneously utilized by some to collagenous micronodules, but these micronodules are sometimes not associated with mucin, so this term ought to be deserted. Complete circumferential development, intraneural invasion, and ganglionic invasion are almost all the time restricted to most cancers. However, benign acini can hardly ever mimic cancer with perineural indentation, monitoring, wrapping, or even intraneural unfold, so caution is warranted in relying on this feature to the exclusion of all others. Only a couple of research have tried to distinguish between lymphatic and vascular channels due to the difficulties in differentiation by gentle microscopic examination. Mean blood vessel rely is larger in tumors with metastases than in those without metastases, and most, however not all, studies show a correlation with pathologic stage. In equivocal instances, diagnosis may be aided by staining with basal cell�specific antibodies to high-molecular-weight keratin 34E12. Adenocarcinoma arising in the transition zone characteristically incorporates clear cells and is nicely or reasonably differentiated. In distinction, Gleason grade 3 and 4 carcinomas usually include cells with clear cytoplasm, beforehand referred to as the hypernephroid pattern. In addition, remedy corresponding to androgen deprivation induces plentiful clear cell change in benign and carcinomatous acini, and the analysis of adenocarcinoma in such circumstances could additionally be difficult (see discussion later in this chapter). The clear cell sample of carcinoma could also be confused with histiocytes, vacuolated stromal smooth muscle cells, and metaplastic cells. This is commonly caused by the small size of the major target, distorted acini with architectural options of malignancy that lack convincing cytologic options, and acinar atrophy or distinguished irritation during which the adjacent benign acini present distortion and reactive atypia with nuclear and nucleolar enlargement. In such instances, it may be appropriate to describe the case as "small acinar proliferation suspicious for however not diagnostic of malignancy" and to counsel rebiopsy. A extensive variety of lesions might mimic adenocarcinoma, particularly in small specimens (Table 9. When this issue arises, it is suggested that every one remaining tissue be submitted for histologic evaluation to decrease the priority for incomplete sampling. Genotypic evaluation to confirm patient id in cases of "vanishing" most cancers seems prudent to reassure patients. In one report, biopsies have been overdiagnosed as cancer in two of four circumstances with no residual most cancers after prostatectomy. Another report found that 11% of patients skilled recurrence and one had systemic progression, but that retrospective report consisted mainly of partially and incompletely sampled prostate. However, grading methods are much less successful in subdividing most reasonably differentiated adenocarcinomas which have intermediate clinical and biologic potential. Since 1999, Gleason grading is the recognized international normal for prostate cancer grading and, in our expertise, is now routinely utilized by most pathologists around the globe. In biopsies, these issues are compounded by small sample measurement, tumor heterogeneity, and undergrading of biopsy samples. Gleason Grading System the Gleason grading system resulted from the Veterans Administration Cooperative Urological Research Group examine of greater than 4000 patients between 1960 and 1975. Tumor heterogeneity is accounted for by assigning a major sample for the dominant grade and a secondary sample for the nondominant grade; the histologic score is derived by including these two patterns together. The success of the Gleason grading system is because of 4 elements: (1) histologic patterns are identified by the degree of acinar differentiation with out relying on morphogenetic or histogenetic models; (2) a simplified and standardized drawing is out there; (3) the Veterans Administration research supplied abundant prospective info that allowed objective computer-generated improvement of this self-defining grading system; and (4) unlike any other grading system in the physique, the Gleason system provided for tumor heterogeneity by figuring out primary and secondary patterns.
Discount goutichine 0.5 mg free shippingLoss of intercellular cohesion in carcinoma in situ may result within the so-called denuding cystitis or in residual neoplastic cells loosely hooked up to the floor ("clinging" pattern) antibiotic resistant upper respiratory infection 0.5 mg goutichine fast delivery. There can also be a pattern of reactive epithelial atypia and granulomatous response deep within the bladder wall infection z cast order 0.5mg goutichine with mastercard. These embrace exfoliation antibiotics harmful goutichine 0.5 mg on-line, epithelial denudation antibiotics for uti without penicillin buy cheap goutichine 0.5 mg line, multinucleation, cytoplasmic vacuolization, and the looks of weird, nonmalignant nuclei within the superficial layer of the urothelium. Mitomycin C may also provoke eosinophilic cystitis, a helpful clue for the surgical pathologist when evaluating small bladder biopsies on this setting. Patients receiving ketamine could present reactive urothelial modifications that can mimic urothelial carcinoma in situ. The earliest change, usually seen after 3 to 6 weeks, consists of acute cystitis with desquamation of urothelial cells and hyperemia with edema of the lamina propria. The urothelium shows various degrees of atypia, together with cytoplasmic and nuclear vacuolization, karyorrhexis, stromal hyalinization, thrombosis of blood vessels, and mesenchymal cell atypia similar to that seen in giant cell cystitis. Surface ulceration with fibrin deposition, or a reactive, tumor-like epithelial proliferation associated with fibrosis of the lamina propria or muscularis propria, arteriolar mural thickening and hyalinization, and atypical and typically multinucleated stromal cells are options seen in late circumstances of radiation cystitis, usually changing into evident months or years after radiation therapy. An necessary long-term effect of radiotherapy is the event of de novo radiationinduced bladder cancer, which normally is a urothelial carcinoma however often is a squamous cell neoplasm. Rare examples of sarcomatoid carcinoma (or carcinosarcoma) and sarcoma of the urinary bladder have been reported. Dysplastic urothelium shows variability in nuclear dimension and shape, increase in nuclear-to-cytoplasmic ratio, and lack of mobile polarity. The degree of cytologic atypia is insufficient for an unequivocal prognosis of carcinoma in situ. The development from dysplasia to carcinoma in situ is characterized by the growing nuclear-to-cytoplasmic ratio, nuclear hyperchromasia, and nuclear and nucleolar enlargement. Most cellular abnormalities in dysplasia are restricted to the basal and intermediate cell layers. Individual dysplastic cells show enlarged nuclei and nucleoli with irregular contours and coarsening of the chromatin. The transition from normal to abnormal urothelium is delicate, and nondysplastic urothelial cells are sometimes dispersed among the many dysplastic cells. Nuclear and architectural options are the first criteria for distinguishing dysplasia from reactive atypia and urothelial carcinoma in situ. Alterations of p53 and allelic losses, notably in chromosome 9, might happen in dysplasia. Primary Dysplasia Primary dysplasia occurs in the absence of different urothelial tumors. Its prevalence within the common inhabitants is unknown due to lack of large-scale screening studies. In an post-mortem collection of 313 sufferers with out gross lesions, urothelial dysplasia was current in 6. It is estimated that de novo (primary) dysplasia progresses to bladder neoplasia in 14% to 19% of instances. Urothelial Carcinoma In Situ (High-Grade Intraurothelial Neoplasia) Urothelial carcinoma in situ is a flat, noninvasive lesion by which the urothelium is entirely composed of cytologically malignant cells. Clinical shows embody gross and microscopic hematuria, irritative symptoms (dysuria, ache, frequency), nocturia, and sterile pyuria. Carcinoma in situ normally is multifocal, with a predilection for the trigone, lateral wall, and dome of the bladder. Cystoscopically, it might seem as erythematous velvety or granular patches, though it might also be visually undetectable. Secondary Dysplasia Secondary dysplasia is seen in patients with a historical past of bladder neoplasia. The incidence of dysplasia in patients with established bladder neoplasia varies from 22% to 86% and approaches one hundred pc in patients with invasive carcinoma. The numbers in parentheses symbolize the number of patients underneath observation at 5, 10, and 15 years. Progression was outlined as improvement of invasive carcinoma, distant metastasis, or dying from bladder most cancers. Nevertheless, the cells of carcinoma in situ are generally small with a excessive nuclear-to-cytoplasmic ratio. Mitotic figures, which are often atypical, are seen in the uppermost layers of the urothelium. Increased Ki67 labeling is noted in carcinoma in situ, however this might be seen additionally in reactive atypia of the urothelium, thus limiting its usefulness in follow. Mapping research of cystectomy specimens present intensive carcinoma in situ, with involvement of the prostatic urethra and the ureter in as many as 67% and 57% of circumstances, respectively. Patients with coexisting invasive urothelial carcinoma have a greater threat for cancer development and cancer-specific dying than sufferers with main carcinoma in situ. Large Cell Carcinoma In Situ Large cell carcinoma in situ constitutes the most typical morphologic type of this entity. In rare cases massive cell carcinoma in situ might have minor nuclear pleomorphism but still exhibit architectural disarray. The morphologic diagnosis of carcinoma in situ requires severe cytologic atypia (anaplasia). Marked disorganization of cells is attribute, with loss of cellular polarity and decreased mobile cohesiveness. In such instances the pleomorphism is often minimal, the cytoplasm is scant, and the nuclei are enlarged and hyperchromatic, with coarse inconsistently distributed chromatin. Loss of cellular polarity and cell cohesion are seen in urothelial carcinoma in situ (A to C). In mucosal biopsies totally lacking floor epithelium, carcinoma in situ could additionally be present solely in von Brunn nests. A cautious search for carcinoma in situ in deeper sections or in different submitted biopsy fragments is necessary, and a advice for analysis of urine cytology for carcinoma cells is warranted. Carcinoma in situ exhibiting pagetoid progress is characterized by large single cells or small clusters of cells within otherwise regular urothelium of ureter, urethra, prostatic ducts, or in areas of squamous metaplasia. Individual cells showing pagetoid spread have enlarged nuclei with coarse chromatin; frequently the cytoplasm is clear. It occurs in a scientific and histologic setting of typical carcinoma in situ with coexisting invasive urothelial carcinoma, and such sufferers basically have the same progression and survival rates as sufferers without pagetoid adjustments. In cases with in depth urothelial denudation, pagetoid carcinoma in situ could also be focally current in adjoining otherwise normal-looking urothelium, thus alerting the surgical pathologist to seek for further carcinoma in situ elsewhere in the bladder. Because major extramammary Paget disease of the external genitalia and of the anal canal may extend to the bladder, and conversely, some instances of pagetoid carcinoma in situ of the bladder might extend to the urethra, ureter, and exterior genitalia, differentiating between these two entities represents an necessary diagnostic and therapeutic challenge. Some authors check with this as adenocarcinoma in situ; such lesions could show papillary, cribriform, or flat morphology.
Diseases - Hypotrichosis mental retardation Lopes type
- Mitochondrial diseases, clinically undefinite
- Kifafa seizure disorder
- Multifocal heterotopia
- Myalgia eosinophilia associated with tryptophan
- TAR syndrome
- Gastrointestinal autonomic nerve tumor
- Japanese encephalitis
- Rocky Mountain spotted fever
- Cholera
Order goutichine 0.5 mg with mastercardThe definition of papilloma remains the same in all new grading techniques and is defined as a papillary tumor with a fragile fibrovascular stroma lined by cytologically and architecturally normal urothelium without elevated cellularity or mitotic figures antibiotic induced c diff generic 0.5mg goutichine fast delivery. Attempting to differentiate biologic conduct based solely on refined histopathologic standards is fraught with difficulties and perils antibiotics for acne work order 0.5 mg goutichine overnight delivery, especially considering the significant interobserver variability that has been documented in quite a few studies with all classification schemes bacteria jewelry generic goutichine 0.5mg. The grading of papillary urothelial tumors is usually based mostly on the worst grade present infection years after knee replacement buy goutichine 0.5 mg. Subsequent studies have also advised that mixed scoring systems may be useful in the grading of bladder tumors. This added flexibility could give a extra correct representation of the tumor histology than trying to pressure a lesion into a single diagnostic class. Histologically, the neoplastic cells invade the bladder wall as nests, cords, trabeculae, small clusters, or single cells which might be often separated by a desmoplastic stroma. The tumor generally grows in a more diffuse, sheetlike sample, however even in these cases, focal nests and clusters are generally current. The cells present average to abundant amphophilic or eosinophilic cytoplasm and large hyperchromatic nuclei. The nuclei are usually pleomorphic and have irregular contours with angular profiles. Some cells include single or a quantity of small nucleoli, and others have massive eosinophilic nucleoli. Foci of marked pleomorphism may be seen, with weird and multinuclear tumor cells present. Invasive tumors are most commonly excessive grade, often displaying marked anaplasia with focal large cell formation. The smoothness of the stroma-epithelial interface could additionally be assessed on hematoxylin and eosin stains. Sometimes tentacular or finger-like extensions can be seen arising from the bottom of the papillary tumor. Invasive tumor cells often have more ample cytoplasm and a better diploma of nuclear pleomorphism. In some cases, significantly in microinvasive disease, the invasive tumor cells may purchase plentiful eosinophilic cytoplasm. Assessment of variations in stromal development pattern offers an essential diagnostic clue. The suffix "m" ought to be added to the appropriate T class to point out a quantity of tumors. The suffix "is" may be added to any T to indicate the presence of associated carcinoma in situ. Rarely the tumor induces an exuberant proliferation of fibroblasts, which can show alarming mobile atypia much like giant cell cystitis. Diagnostic Pitfalls Used with permission of the American College of Surgeons, Chicago, Illinois. The "y" prefix signifies these cases by which classification is performed during or after initial multimodality remedy. In some circumstances, retraction artifact round superficially invasive individual tumor cells could mimic angiolymphatic invasion. Often this finding is focal and should itself be one of the early indicators of invasion into the lamina propria. Invasive urothelial carcinoma could have a cellular stroma with spindled fibroblasts and variable collagenization, or a hypocellular Transurethral resection specimens are excised in a piecemeal style. Submitted tissue fragments are of variable form and measurement, and are troublesome, if not impossible, to orient properly (Table 6. Furthermore, due to their complicated structure, papillary tumors are inevitably tangentially sectioned in multiple planes, resulting in the presence of isolated nests of noninvasive tumor cells within connective tissue. Smooth, spherical, and common contours favor tangential sectioning, whereas irregular, jagged nests with haphazard association favor stromal invasion. Papillary tumors could show variable and often brisk inflammation at the tumor-stromal interface. Thermal damage or cautery artifact produces severely distorted morphology, rendering accurate prognosis of invasion difficult. This is very problematic when von Brunn nests are distinguished or when they have been distorted by inflammatory or cautery artifact. Substaging of pT1 Tumors the recurrence and progression rates for pT1 tumors are highly variable. Invading tumor cells could have extra eosinophilic cytoplasm than overlying noninvading tumor cells. Muscularis mucosae consist of skinny and wavy fascicles of easy muscle frequently related to massive, thin-walled blood vessels. The stroma related to invasive cancer could also be (A) inflammatory, (B) myxoid, or (C) fibrous. The similar investigators subsequently applied the identical criteria to a bunch of 83 consecutive sufferers recognized with pT1 bladder cancer. No prognostic differences had been found between Ta and T1 low-grade papillary urothelial carcinomas. T1 >1-mm high-grade papillary urothelial carcinomas were related to considerably higher dangers for recurrence, progression, cancer-specific mortality, and all-cause mortality compared with T1 1-mm and Ta tumors. Invasive tumor also might present variable and often brisk inflammation at the tumor-stromal interface (B and C). In these circumstances, smoothelin, a lately recognized biomarker that facilitates distinguishing muscularis mucosae from muscularis propria, could also be helpful. Muscularis propria sometimes shows intense and strong smoothelin staining, in contrast with muscularis mucosae, which has weak or negative smoothelin staining. Among sufferers with lymph node�positive bladder cancer, 10-year recurrence-free survival fee was 50% for pT2a carcinoma and 48% for pT2b carcinoma. The depth of stromal invasion in transurethral resection or biopsy specimens is measured from the basement membrane of the bladder mucosa to the deepest invasive most cancers cells utilizing ocular micrometer (top panel, A and B). Numbers in parentheses characterize the variety of sufferers beneath remark at 3, 5, and 7 years. Progression was outlined as the development of muscle-invasive or extra advanced stage carcinoma, distant metastasis, or death from bladder cancer. Substaging of T1 bladder carcinoma primarily based on the depth of invasion as measured by micrometer: a model new proposal. The subdivision of pT3 tumors into T3a (tumors with microscopic extravesical tumor extension) and pT3b (tumors with gross extravesical extension) is also of questionable utility. Lymph node and surgical margin standing had been the one components that considerably impacted affected person prognosis in this study. Cheng and his colleagues analyzed ninety patients with bladder cancer diagnosed with invasive bladder most cancers at transurethral resection. The authors discovered that the depth of invasion was related to last pathologic stage (Spearman correlation r � zero.
Goutichine 0.5mg for saleIt was not till after Papanicolaou and Marshall revealed the primary article in 1945 that urine cytology was used to detect urothelial carcinoma bacteria xanthomonas cheap 0.5mg goutichine with visa. Recent efforts described on this chapter provide great promise in resolving these issues virus yang menguntungkan buy goutichine 0.5mg with amex. This article discusses the spectrum of cytologic abnormalities in voided urine samples and washings to permit comparison with biopsy findings described in Chapters 5 and 6 best antibiotics for sinus infection mayo clinic generic goutichine 0.5 mg with visa, and presents classifications published after the last version of this textual content antibiotic kennel cough goutichine 0.5mg sale. The clinically vital and common problem of hematuria can additionally be addressed from the perspective of the cytopathologist. Utility of Urine Cytology Indications Cytologic examination of the urine sediment is of value in the analysis of a extensive variety of benign and malignant illnesses of the bladder, urethra, ureter, and kidney. Follow-up of sufferers with atypical cytology analysis or urothelial tumor, regardless of grade 3. Monitoring of sufferers with urothelial tumor present process or after remedy, together with lively surveillance8,eleven,12 4. For instance, higher urinary tract washings were superior to voided samples in detection of higher tract high-grade carcinoma (90% versus 50% yield, respectively). Obscuring parts embrace neutrophils, lubricants, other international particles, crystals, micro organism, squames, and spermatozoa. Conversely, according to one group, if there are any atypical cells, regardless of the general cellularity, this represents a satisfactory specimen. Adequacy elevated linearly for each increment of urine quantity submitted to the laboratory as much as 30 mL, after which the correlation was nonlinear, and low-volume specimens were much less prone to harbor suspicious or malignant cells. The cytospin technique was superior to direct smear, Thin Prep, and SurePath in a comparative study of voided urine specimens; the speed of unsatisfactory preparations was quite low (0. Increased cellularity is observed in specimens from sufferers with most cancers, calculi, or an infection compared with these with solely hematuria or irritative voiding symptoms. Operator-dependent components check with experience of the examiner and the potential for human bias and error. Logistic components that influence adequacy embrace size of time from assortment to processing, container leakage with potential drying artifacts, and heaps of others. Reporting and Classification Several reporting and classification systems for urine cytology have been revealed, each of which has relative strengths and weaknesses. Unlike cervical cytology, there has not been widespread acceptance and use of any single reporting system for urine cytology studies. Recently two worldwide consensus conferences printed their classifications: the Paris System 2013 and the International Consultation on Urologic Disease�European Association of Urology 2015 (Table 7. Both were based mostly on skilled consensus by small, self-selected tutorial groups with minimal enter from different cytopathologists, urologists, oncologists, or others. The supernatant is eliminated to inside roughly 1-2 mL of the cell pellet, and the pellet is then resuspended and rinsed with 10 mL of hypotonic solution (0. The cells are resedimented at 600 g for 10 minutes, and the supernatant is eliminated to within zero. The pellet is then gently vortexed and resuspended in 10 mL three:1 methanol/glacial acetic acid fixative. The urinary cells are then sedimented at 600 g for 5 minutes, aspirated, and transferred to a 2-mL microfuge tube. The ultimate cell pellet is left in approximately 100-500 L of residual methanol/glacial acetic acid fixative, relying on the scale of the cell pellet. A whole of 10 L of cell sediment is positioned on the slide, and the specimen is allowed to dry. Gauze is positioned over the membrane and slight strain utilized with the palm of the hand to transfer the cell filtrate. The membrane is discarded and the filter holder was deposited in a 10% bleach answer in a single day until subsequent use. Urine samples are immersed in a buffered preservative answer, transferred to a bowl, and a cylinder with a filtration membrane is then placed in the bowl to be positive that the cells are homogeneously distributed. Using adverse pressure, the erythrocytes and mucus penetrate the filtration membrane, leaving only the filtration membranes for the diagnostic process. This maneuver is repeated until an acceptable number of cells (2000-50,000) is collected. Thereafter the cylinder is faraway from the bowl; cells left on the filtration membrane are connected to the slide after which fixed in 95% alcohol. The SurePath take a look at is carried out with a proprietary liquid-based monolayer cell preparation system density gradient-based cell enrichment. Urine samples are immersed in ethanolic preservative resolution and a device is placed into the vial to ensure that cells are homogenously distributed. A polysaccharide-based density gradient reagent is used to filter particles, centrifuged, resuspended, and centrifuged once more. Agency for Healthcare Research and Quality, three key rules are required for successful conduct of systematic reviews: (1) the evaluation should be relevant and timely, specializing in the most important issues and the optimum time to initiate a evaluate; (2) the review have to be goal and scientifically rigorous, free from conflicts of interest; and (3) the evaluate should embrace public participation and transparency to ensure confidence and credibility, and supply for accountability. Nonetheless, any efforts to create standardized terminology are laudable and generate renewed interest in refinement of diagnostic standards, continuing the work of the Papanicolaou Society at creation of uniformity in cytopathology practice. The words "adverse for high-grade urothelial carcinoma" on a report might simply be mistyped or misinterpreted by the transcriptionist, cytopathologist, or urologist if the word adverse is overlooked while the word carcinoma registers, doubtlessly resulting in severe penalties for the affected person. Reasonable alternate options embrace "negative for high-grade malignancy," "negative for high-grade neoplasia," and "no particular proof of malignancy. Low-grade urothelial neoplasm should be used sparingly and at the facet of the adverse class to clarify the absence of high-grade carcinoma within the Paris System. In the Bostwick Laboratories classification, the presence of fibrovascular cores is considered suspicious. Only distinction is the cellular amount: suspicious, very few cells; high-grade carcinoma, 5-10 cells or extra. The Paris System for reporting urinary cytology: the search to develop a standardized terminology. Compared with previous classification systems, the Paris System 2013 resulted in an excellent increase within the rate of "atypical" instances while bettering sensitivity however lowering specificity. Sensitivity was higher (63% versus 49%) on the expense of lower specificity (73% versus 91%). In one other research, 70% of circumstances of "atypical" cases have been reclassified by Paris System 2013 as "adverse"; nonetheless, 18% of those were discovered to have high-grade cancer. Reclassification of such cases as "negative" decreased the rate of "atypical" from 25% to 21%, though the excessive price of subsequent "high-grade cancer" amongst nonsurveillance patients advised that the reclassification could additionally be "inappropriate. The authors concluded that this low degree of diagnostic precision may negatively influence the applicability of Paris System 2013 for widespread clinical application. Superficial squamous cells from the feminine genital tract often outnumber urothelial cells. Benign glandular cells (from cystitis glandularis), squamous cells originating in squamous metaplasia of urothelium or external genital tract pores and skin, and, not often, benign seminal vesical cells additionally fall into this category. Clusters or fragments of urothelial cells that might be seen in each instrumented and noninstrumented urine specimens ought to be categorized as "negative" until the cytomorphology of the cells forming the group fulfills the criteria for "atypical.
Goutichine: 0.5 mg
Discount 0.5mg goutichine fast deliveryEvidence for oligoclonality and tumor unfold by intraluminal seeding in multifocal urothelial carcinomas of the upper and lower urinary tract antibiotic 875mg 125mg discount goutichine 0.5mg line. Cytogenetic analysis of multifocal bladder cancer supports a monoclonal origin and intraepithelial spread of tumor cells treatment for dogs chocolate generic goutichine 0.5 mg without prescription. Oligoclonality of early lesions of the urothelium as decided by microdissectionsupported genetic evaluation antimicrobial 8536 msds cheap goutichine 0.5 mg with mastercard. Genetic instability in superficial bladder most cancers and adjacent mucosa: an interphase cytogenetic study medication for uti pain over the counter buy goutichine 0.5mg. Clonality of multifocal urothelial carcinomas: 10 years of molecular genetic research. Genetic alterations within the molecular subtypes of bladder cancer: illustration in the cancer genome atlas dataset. Independent element analysis uncovers the landscape of the bladder tumor transcriptome and reveals insights into luminal and basal subtypes. Identification of distinct basal and luminal subtypes of muscle-invasive bladder cancer with completely different sensitivities to frontline chemotherapy. Targeting the programmed cell death-1 pathway in genitourinary tumors: present progress and future perspectives. Cancer heterogeneity and its biologic implications within the grading of urothelial carcinoma. World Health Organization and International Society of Urological Pathology classification and two-number grading system of bladder tumors: reply. Papillary urothelial neoplasm of low malignant potential: evolving terminology and ideas. Classification and grading of the non-invasive urothelial neoplasms: latest advances and controversies. Prognostic Performance and Reproducibility of the 1973 and 2004/2016 World Health Organization grading classification techniques in non-muscle-invasive bladder cancer: A European Association of Urology non-muscle invasive bladder most cancers guidelines panel systematic evaluate. A retrspective evaluation of 232 patients with larger than or equal to 5-year follow-up. The relationship among multiple recurrences, development and prognosis of patients with levels Ta and T1 transitional cell most cancers of the bladder followed for no much less than 20 years. The correlation of T1 bladder tumour history with prognosis and follow-up requirements. Long-term followup of preliminary Ta grade 1 transitional cell carcinoma of the bladder. Prognostic components in non-infiltrating carcinoma of the bladder: a preliminary report. The natural historical past of papillary transitional cell carcinoma of the bladder and its remedy in any unselected inhabitants on the idea of histologic grading. Superficial bladder tumors (stage pTa, grades 1 and 2): the significance of recurrence sample following initial resection. The treated histories of patients with Ta grade 1 transitional-cell carcinoma of the bladder. Identification of a high risk subgroup of grade 1 transitional cell carcinoma utilizing picture analysis based mostly deoxyribonucleic acid ploidy analysis of tumor tissue. A simplified grading method of transitional cell carcinoma of the urinary bladder: reproducibility, medical significance and comparison with other prognostic parameters. Grading of human urothelial carcinoma primarily based on nuclear atypia and mitotic frequency. Prognosis of transitional cell bladder cancer: a multivariate prognostic score for improved prediction. The World Health Organization/International Society of Urological Pathology consensus classification of urothelial (transitional cell) neoplasms of the urinary bladder. Clinico-pathologic variations between bladder neoplasm with low malignant potential and low-grade carcinoma. Morphological classification and definition of benign, preneoplastic and noninvasive neoplastic lesions of the urinary bladder. World Health Organization classification of the noninvasive urothelial neoplasms: Inherent problems and medical reflections. Long-term outcome of bladder papillary urothelial neoplasms of low malignant potential. Biologic differences between noninvasive papillary urothelial neoplasms of low malignant potential and low-grade (grade 1) papillary carcinomas of the bladder. Interobserver discrepancy utilizing the 1998 World Health Organization/ International Society of Urologic Pathology classification of urothelial neoplasms: practical selections for affected person care. Reproducibility of the 1998 World Health Organization/International Society of Urologic Pathology classification of papillary urothelial neoplasms of the urinary bladder. Reproducibility and prognostic variability of grade and lamina propria invasion in levels Ta, T1 urothelial carcinoma of the bladder. The reliability and reproducibility of the different classifications of bladder cancer. In: Haupmann S, Dietel M, SorbrinhoSimoes M (eds), Surgical Pathology Update 2001. World Health Organization Classification of Tumours: Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs. Low-grade papillary urothelial carcinoma of the urinary bladder: a clinicopathologic evaluation of a post-World Health Organization/International Society of Urological Pathology classification cohort from a single academic middle. Clinicopathologic traits of 23 instances of invasive low-grade papillary urothelial carcinoma. Invasive low-grade papillary urothelial carcinoma: a clinicopathologic evaluation of forty one cases. High-grade papillary urothelial carcinoma of the urinary tract: a clinicopathologic evaluation of a postWorld Health Organization/International Society of Urological Pathology classification cohort from a single educational heart. Histologic grading of urothelial papillary neoplasms: impression of combined grading (twonumbered grading system) on reproducibility. Tumor grade heterogeneity in urothelial bladder carcinoma-proposal of a system using mixed numbers. Substaging of T1 bladder carcinoma based on the depth of invasion as measured by micrometer. Detection of residual tumor cells in bladder biopsy specimens: pitfalls within the interpretation of cytokeratin stains. Characteristics and outcomes of patients with medical T1 grade three urothelial carcinoma treated with radical cystectomy: outcomes from a global cohort. Clinical end result in a recent collection of restaged patients with medical T1 bladder cancer.
Generic 0.5 mg goutichine overnight deliveryPerigraft air 3 months after placement of the graft should increase concern of a graft infection infection gone septic purchase goutichine 0.5mg visa. Graft infections manifesting as perigraft fluid could be appropriately treated by percutaneous drainage of the fluid and long-term antibiotics antibiotic resistance global statistics generic goutichine 0.5 mg free shipping. The nice majority of sufferers have full decision of perigraft air by approximately 8 to 12 weeks following implantation herpes simplex virus goutichine 0.5 mg on-line. Which of the following statements regarding Staphylococcus epidermidis graft infections is true Routine Gram stain and tradition of the graft are often enough for establishing the diagnosis virus hoax goutichine 0.5 mg online. Extended (>24 hours) perioperative protection with antibiotics is more effective at stopping graft infections compared with a single preoperative dose. The options for reconstruction of an infected aortofemoral bypass graft embody all of the following besides: a. Grafts involving the femoral artery have a better price of an infection than grafts anastomosed to the iliac arteries. The surgeon is the principal and most likely supply of the organism infecting the prosthesis. The mortality of an operation to deal with prosthetic aortic graft infection approaches 75% to 80%. Infection complicating arterial grafts: private expertise with 12 cases and evaluation of the literature. Prosthetic vascular graft infection: a threat issue evaluation utilizing a case�control study J Infect. The incidence and factors related to graft an infection after aortic aneurysm restore. Aseptic periprosthetic fluid assortment: a late complication of Dacron arterial bypass. Identification of Staphylococcus epidermidis vascular graft infections: a comparison of tradition techniques. Differential results of a gramnegative and a gram-positive an infection on autogenous and prosthetic grafts. Wound an infection after infrainguinal bypass operations: multivariate evaluation of putative risk factors. The relevance of arterial wall microbiology to the therapy of prosthetic graft infections: graft an infection vs. Bacteremic infectability of vascular grafts: the influence of pseudointimal integrity and duration of graft perform. Systemic and native antibiotic prophylaxis in the prevention of prosthetic vascular graft infection: an experimental research Eur J Vasc Endovasc Surg. Systemic and local antibiotic prophylaxis in the prevention of Staphylococcus epidermidis graft infection. Prevention of an infection in peripheral arterial reconstruction: a scientific review and meta-analysis. Graft-related complications after belly aortic aneurysm repair: reassurance from a 36-year population-based expertise. Aorto-enteric Fistula After Endovascular Abdominal Aortic Aneurysm Repair: Case Report and Review. Aortoenteric and paraprosthetic-enteric fistulas: problems of analysis and administration. Composition and antimicrobic resistance of skin flora in hospitalized and healthy adults. The effective period of preventive antibiotic action in experimental incisions and dermal lesions. The timing of prophylactic administration of antibiotics and the danger of surgical-wound infection. Practice guidelines for adult antibiotic prophylaxis throughout vascular and interventional radiology procedures. Written by the Standards of Practice Committee for the Society of Interventional Radiology and Endorsed by the Cardiovascular Interventional Radiological Society of Europe and Canadian Interventional Radiology Association [corrected]. Efficacy and period of antistaphylococcal activity evaluating three antibiotics bonded to Dacron vascular grafts with a collagen launch system. Prophylaxis of graft an infection with rifampicinbonded Gelseal graft: 2-year follow-up of a potential medical trial. Preoperative pores and skin antiseptics for stopping surgical wound infections after clean surgery Cochrane Database Syst. Experience with a brand new unfavorable strain incision management system in prevention of groin wound infection in vascular surgical procedure patients. Negative pressure wound remedy for atrisk surgical closures in sufferers with a number of comorbidities: a potential randomized controlled research Ann Surg. Negative pressure wound therapy for pores and skin grafts and surgical wounds healing by main intention. Natural history of periprosthetic air on computerized axial tomographic examination of the stomach following belly aortic aneurysm repair. Detection of stomach aortic graft infection: comparison of magnetic resonance imaging and indium-labeled white blood cell scanning. Indium 111-labeled leukocyte scanning for detection of prosthetic vascular graft an infection. Utility of the indium 111-labeled human immunoglobulin G scan for the detection of focal vascular graft an infection. Long-term suppressive antimicrobial therapy for intravascular device-related infections. In vitro efficacy of antibiotic beads in treating belly vascular graft infections. Regional antibiotic delivery for the treatment of experimental prosthetic graft infections. Use of antibiotic-loaded polymethylmethacrylate beads for the treatment of extracavitary prosthetic vascular graft infections. Antibiotic-loaded polymethylmethacrylate beads for the therapy of extracavitary vascular surgical web site infections. Priority of revascularization in sufferers with graft enteric fistulas, contaminated arteries, or contaminated arterial prostheses. Aortic and peripheral prosthetic graft an infection: differential administration and causes of mortality Am J Surg. Axillobifemoral bypass and aortic exclusion for vascular septic lesions: a multicenter retrospective research of ninety eight cases.
Yun-Zhi (cloud mushroom) (Coriolus Mushroom). Goutichine. - Boosting immune function, herpes, chronic fatigue syndrome, hepatitis, lung disorders, body building, ringworm, skin infections (impetigo), urinary and digestive tract infections, poor appetite, and other uses.
- What other names is Coriolus Mushroom known by?
- Dosing considerations for Coriolus Mushroom.
- What is Coriolus Mushroom?
- How does Coriolus Mushroom work?
- Are there safety concerns?
- Cancer when used with chemotherapy regimens (when PSK products isolated from coriolus mushroom are used).
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96638
Buy cheap goutichine 0.5mg onlinePatients with rates decrease than 50 mL/min experience atrophy of the seminiferous epithelium antibiotic resistance nhs purchase goutichine 0.5mg with amex. Earlier research suggested that hypogonadism is a frequent discovering in men with celiac illness and ends in scientific signs in 5% to 10% of untreated sufferers bacteria you can eat 0.5 mg goutichine for sale. Spermiograms present lowered motility and numerous morphologic anomalies in spermatozoa antimicrobial agent definition best goutichine 0.5mg. The cause of pituitary derangement is unknown virus protection free discount goutichine 0.5mg on line, but one possible trigger is deficiency of fat-soluble nutritional vitamins, similar to A and E. Vitamin A is essential for Sertoli cell function, as well as for early spermatogenetic phases. Vitamin E helps correct differentiation and function of epididymal epithelium, spermatic maturation, and secretion of proteins by the prostate. Chronic Anemia In patients with continual anemia who require multiple transfusions, excess iron accumulates in tissues and varieties reactive oxygen species inflicting irreparable injury (secondary hemochromatosis). The most frequent persistent anemias are -thalassemia, sickle cell anemia, and Fanconi anemia. The cause is mutation in the -globin gene, leading to ineffective erythropoiesis, hemolysis, and anemia. The -thalassemia trait is current in 2% to 3% of the general population, and incidence is larger in Mediterranean and African people. The gene liable for the illness is located on chromosome 11, and greater than 90% of synthesized hemoglobin is sort A. Patients might present with delayed puberty, hypogonadism that varies from slight to severe, eunuchoid habitus, decreased libido, erectile dysfunction, priapism, and poor semen high quality. The testicular interstitium and atrophic tubules show Perl stain�positive iron deposits. Fanconi anemia is a uncommon inherited disorder characterized by chromosomal instability, bone marrow failure, developmental defects, and predisposition to cancer. Patients with Hb Bart syndrome, the most extreme form, are affected during gestation and are born with generalized edema, pleural and pericardial effusions, and severe hypochromic anemia. Hydrocephaly, hepatosplenomegaly, extramedullary erythropoiesis, urologic defects (ambiguous genitalia, undescended testis, and hypospadias), and cardiac defects are frequent. Nonetheless, few studies have addressed the effect of weight problems on gonadal growth in childhood, recognizing that there could additionally be an impact on hypothalamopituitary-gonadal perform. This impairment could be secondary to altered neurotransmitter status at the hypothalamic stage. The underlying problems likely embrace erectile dysfunction, decreased sexual activity, and alterations of the hypothalamic�pituitary-testicular axis. Patients also have Leydig cell atrophy, cuboidal metaplasia of the rete testis, and epididymal atrophy. The syndrome is more frequent in Iranian Jews (1 in 6500 to 9000) and Finnish individuals (1 in 25,000), whereas low frequency is noticed in Norway with an incidence of 1 in eighty,000. The testes appeared atrophic, and seminiferous tubules present decreased diameter, absence of elastic fibers, and just some dysgenetic Sertoli cells in numbers that fluctuate extensively from one tubule to another. In patients without adrenal insufficiency, the hypogonadism is often hypogonadotropic. Hemochromatosis and Infertility Hereditary hemochromatosis is probably the most frequent genetic disease in the Northern Hemisphere. It outcomes from excessive iron absorption and accumulation in a quantity of tissues and organs, and leads to cirrhosis, diabetes, hypogonadism, and arthralgia. In males the disease seems at a younger age than in women and usually is extra severe. Iron stability depends on intestinal absorption, regulated by the hepatic peptide hormone hepcidin via its receptor, the mobile exporter ferroportin, and adequate iron recycling. Excessive iron absorption is because of hepcidin deficiency or insensitivity of ferroportin to hepcidin. Iron deposits accumulate in the liver, pancreas, hypophysis, heart, adrenals, and gastric mucosa. Once intracellular ferritin saturation occurs, extra free iron participates in generating intracellular redox reactions, producing poisonous reactive oxygen species, and causing cell injury or cell death. It is autosomal dominant and impacts the basolateral iron carrier ferroportin 1, resulting in iron deposition in macrophages. Types 1, 2, and three have recessive autosomal inheritance and present an identical distribution sample of iron deposits. Hypogonadism may be the first sign of illness when it begins in adult life as in type 2 hemochromatosis and will be the initial symptom. The cause of these testicular disorders may be preferential deposition of iron in gonadotropic cells. Given that early diagnosis is feasible in all kinds of hemochromatosis, clinicians in countries with a high prevalence of the disease must be vigilant, thereby allowing affected sufferers to start treatment at an early age and thus avoid later problems. The principal characteristics of this syndrome are progressive exterior ophthalmoplegia, pigmentary retinopathy, cardiac conduction defects, and cerebellar ataxia. Disorders of the reproductive system, together with cryptorchidism, delayed puberty, testicular hypoplasia, and low gonadotropin ranges, are present in 20% to 30% of cases. The incidence is estimated to be 1 in 20,000, with no differences amongst ethnic teams. The phenotype is diversified, however no correlation exists between genotype and phenotype. Today, a minimum of nine phenotypes are identified in male sufferers and two in female patients. Cerebral demyelization is initially manifest by attention-deficit/ hyperactivity dysfunction, ophthalmic or ear abnormalities, and psychological issues. Seminiferous tubules have tremendously reduced diameters, with thickened walls and an epithelium with low number of Sertoli cells and few spermatogonia. The caput of the epididymis is lowered to a loose connective tissue during which the silhouettes of the efferent ducts are hardly noticed. Adrenal gland exhibiting severe atrophy of the cortex and globoid cells at the periphery. Physical examination exhibits scant pubic hair (50%), gynecomastia (35%), and small testes (12%). Testosterone level is much like controls, although free testosterone stage is decrease. At the onset, spermatogenesis and sperm count may be normal, though teratozoospermia and asthenozoospermia are frequent. Later, spermatogenesis undergoes speedy deterioration, with variable diploma of germ cell arrest and azoospermia. Patients in the early phases might profit from hematopoietic cell transplantation, whereas these with advanced illness are candidates for experimental therapies. Seminiferous tubules include primarily Sertoli cells with solely isolated spermatogonia. Patients usually have cutaneous angiokeratomas, posterior capsular cataracts, and tortuous retinal veins.
Order goutichine 0.5mg overnight deliveryIt is commonly troublesome to antimicrobial washcloths generic goutichine 0.5mg with amex, decide whether a patient wants a remote bypass in such a setting; due to this fact the safest approach is to carry out quick revascularization within the majority of cases antibiotic nerve damage generic 0.5mg goutichine fast delivery. Some research have additionally checked out in situ alternative of the infected graft somewhat than extraanatomic bypass infection red line up arm purchase 0.5 mg goutichine amex, with good outcomes infection prevention discount goutichine 0.5mg otc. One research showed a 90% survival for the operation with no cases of limb loss and 83% of surviving patients experiencing no points after a mean of 5. One of seven died of fungal septicemia, and one of seven required laparotomy for persistent sepsis. Three of seven patients have been alive at long-term follow-up at a imply of three years with out proof of recurrent an infection or bleed. These information suggest that endovascular remedy may be an alternate in highrisk sufferers. These findings prompted the authors to conclude that, among patients with evidence of severe infection, endovascular repair should be thought-about only as a bridge to extra definitive excision. This is most likely as a end result of residual an infection within the bed of the graft in the perigraft and para-aortic tissues. The perigraft debridement should therefore be generous sufficient to ensure eradication of all infected tissue. The aorta must then be oversewn in two layers, if possible, using polypropylene sutures. Treatment of Specific Graft Site Infections Aortic Grafts When one is faced with an aortic graft infection, some elementary points must be addressed. First, one has to determine whether or not the aortic graft was carried out for aneurysmal or occlusive disease. If the graft was positioned for aneurysmal disease, it goes to be an end-to-end anastomosis; if the graft was placed for occlusive disease, the configuration of the anastomosis could also be end to end or end to side. The distal implantation web site has to be addressed as nicely; if the graft extends right down to the femoral vessels, revascularization shall be a bit more involved than if the distal anastomosis is to the iliac arteries. The inflow anastomosis is created at the proximal axillary artery the distal anastomoses can. This operation may be adopted immediately by graft excision or, alternatively graft excision can be performed 1 to 2 days later. This, staged strategy is associated with significantly less morbidity than the traditional simultaneous procedure (see section Revascularization). This method supplies uninterrupted perfusion of the lower limbs and reduces the morbidity related to ischemic changes occurring when reconstitution of circulate is delayed until after the aortic graft has been eliminated. For aortic graft excision, celiotomy is carried out, and the aortic graft is isolated through the retroperitoneum. Although systemic heparin is indicated for the axillofemoral bypass, the advantage of the staged operation is that no anticoagulation is necessary during the aortic graft excision. If the procedures are done consecutively the, heparin should be reversed before the aortic graft is approached. Careful dissection in the stomach is performed, and the graft is separated from adherent bowel and viscera. Once the complete graft has been exposed, proximal management is obtained on the supraceliac aorta. The iliac arteries distal to the anastomoses are similarly isolated and control is obtained. The entire graft is then excised, and the aorta is debrided back to regular, healthy-appearing tissue. Care is taken to avoid damage to the ureters, and placement of ureteral stents previous to the process is commonly helpful. If debridement is critical above the renal arteries, it must be performed with out compromise and the renal arteries then revascularized by antegrade bypasses from branches of the celiac axis. Perfusion of the pelvic circulation is maintained by retrograde circulate from the axillofemoral bypass through the exterior and internal iliac arteries. If the distal anastomoses are to the exterior iliac arteries and require excision, perfusion to no less than one inner iliac artery should be maintained via a bypass. Axillobifemoral bypass has long been thought-about an imperfect resolution to aortic graft an infection. Long-term survival is poor, with solely 56% to 78% survival at long-term follow-up reported in recent studies. Reported incidence rates have been noted to be as excessive as 30% for aortic stump blowout after excision and extraanatomic bypass, although more recent information suggest that these occasions have turn into rarer, with rates nearer to 3%. When all adverse outcomes have been combined, any one of many in situ reconstructions was favored over extraanatomic bypass. The benefit of this approach is that the reconstruction is totally autogenous, thereby avoiding the need for extraanatomic bypass. Thirty-day mortality rates are reported to be low at lower than 10%, and 5-year mortality charges are noted to be similar to extraanatomic bypass at 30% to 50%. Patency rates are high, with lower than 4% early thrombosis and 62% to 91% primary patency at 5 years. Animal studies have suggested lowered charges of reinfection with cryopreserved allografts. In one examine of 57 in situ revascularizations of the belly aorta using cryopreserved arterial homograft, 30-day mortality was found to be 9%, with the vast majority of deaths attributable to sepsis-related multiorgan system failure. Next, placement of in situ rifampin-soaked prosthetic grafts with omental protection and antibiotic suppression has been advocated for the remedy of aortic graft an infection. Studies have revealed a 30-day mortality of 7% to 21% and a 1-year survival of 64% to 100% associated with this method. Moreover, regardless of concern for a high danger of reinfection, graft reinfection occurred in only 4% of sufferers. A whole of 257 sufferers were randomized at 14 vascular centers to both rifampin-bonded grafts or common collagen-impregnated grafts. There was no important difference within the incidence of graft an infection on early follow-up (1 month). The authors concluded that, despite studies on almost 3000 patients, there was no convincing proof that rifampin bonding decreases the incidence of prosthetic extraanatomic graft an infection. Also of some concern with use of rifampin-bonded grafts is the efficacy of this method in the face of rising antibiotic resistance. Although rifampin enjoys broad activity in opposition to many organisms, including Streptococcus and Staphylococcus species, animal and medical studies have suggested attainable limitations in the use of rifampin-bonded grafts towards methicillin-resistant S. The silver is assumed to inhibit bacterial colony formation on the prosthetic graft. One current study compared silver-coated grafts with arterial homografts with and without immunosuppression.
Generic goutichine 0.5 mg lineThe childish form may be related to other disorders antibiotic resistance warning buy 0.5 mg goutichine with mastercard, similar to hemihypertrophy and Beckwith-Wiedemann syndrome antibiotics for uti cost buy goutichine 0.5mg without prescription, and may be included in the spectrum of households with cancer predisposition as a result of abnormalities in genes that encode transcription components implicated in cell proliferation antimicrobial chemotherapy 6th edition purchase goutichine 0.5 mg free shipping, differentiation infection without fever order goutichine 0.5 mg amex, senescence, apoptosis, and genomic instability. The differential analysis between adenoma and carcinoma could also be difficult even for an skilled pathologist. Gonadal impairment depends on the sort of diabetes and time of illness onset (infancy and childhood, puberty, or adulthood). Small interstitial blood vessels show diabetic microangiopathy characterized by enlargement and duplication of the basal lamina, pericyte degeneration, and endothelial cell alterations. There is a rise within the variety of fibroblasts and amount of collagen and intercellular matrix within the interstitial connective tissue. Sexual dysfunction is current in more than one-half of patients, who complain of impotence, decreased libido, disorders of intercourse, and retrograde ejaculation. Neuropathy might be chiefly responsible for erectile failure in males with diabetes. The most frequent are enlargement and calcifications of seminal vesicles and vasa deferentia. The third presentation, so as of frequency, includes a group of healthy infertile sufferers with irregular seminal parameters or nonobstructive azoospermia. Whether the lesions of sperm excretory ducts correspond to agenesis or atresia remains controversial. As a outcome, epididymides are small, ductus deferentia are solely epithelial cords, and the walls include just some rings of loose connective tissue. The spermiogram is attribute of obstructive azoospermia, with acid pH, decreased semen quantity and fructose concentration, and elevated citric acid and acid phosphatase. Most testes show tubular ectasia with minimal lesions of the adluminal compartments. These lesions are most likely secondary to obstruction, which can be superimposed on those derived from chronic nutrition deficiency. Chronic hepatic failure damages the hypothalamohypophyseal-testicular axis and consequently all related endocrine glands. Hypogonadism is frequent within the ultimate phases of severe persistent liver ailments, including alcoholism and nonalcoholic fatty liver illnesses. Sections of the ductus epididymidis present decreased lumen diameter with surrounding concentric rings of unfastened connective tissue. The association of atrophy with gynecomastia and hepatic cirrhosis is referred to as Silvestrini-Corda syndrome. Acute alcoholic intoxication suppresses serum testosterone stage in male nonalcoholic volunteers and laboratory animals. Long-term alcohol ingestion, even in the absence of cirrhosis, causes hypogonadism, with signs of Leydig cell failure, including testicular atrophy, infertility, decreased libido, impotence, and decreased measurement of the prostate and seminal vesicles. Most men with chronic alcoholism, with or without cirrhosis, have significant testicular lesions. Seminiferous tubules have lowered diameters, thickened lamina propria, and decreased or absent germ cells. The epididymis becomes atrophic, primarily in the ductuli efferentes, because of androgen deprivation. The epithelium of the rete testis turns into cuboidal or columnar in response to estrogens. The spermiogram correlates with variability of histologic findings, and usually exhibits marked discount in number and motility of spermatozoa and enhance in the percentage of morphologically abnormal spermatozoa. The protein product controls chlorine ion flux throughout the plasma membrane and plays an necessary position in hydration of epithelial secretions. Secretions subsequently turn out to be thick and sticky, producing obstructions in the excretory ducts of many glands (respiratory tract, pancreas, sweat glands), in addition to in the growing sperm excretory ducts, such as the ductus epididymis and ductus deferens. The seminiferous tubules show decreased diameter, thickening of the tubular wall, and spermatogonia and Sertoli cells exhibiting intense vacuolation of the adluminal compartment. The testicular interstitium exhibits marked Leydig cell atrophy and numerous macrophages. In 1-antitrypsin deficiency, testicular operate and fertility are conserved for years; only in superior levels of the illness do minor biochemical alterations happen. Hypogonadism is manifest by small testes, delayed puberty, and, in adults, lack of germ cell development. The seminiferous tubules show untimely sloughing of major spermatocytes and Sertoli cells with vacuolation of the apical cytoplasm. It is associated with cysts in liver and pancreas, cardiovascular pathology (aneurysms), and infertility. The associated sexual dysfunction consists of erectile dysfunction, diminution of libido and semen volume, oligozoospermia or azoospermia, and infertility. Patients with end-stage renal illness who endure dialysis, especially older patients and people receiving extended dialysis, show calcifications in a quantity of organs and tissues, including the male genital system (epididymidis, tunica albuginea, and cavernous tissue) in 87% of instances, with isolated cases of calcification of the testicular parenchyma and microlithiasis. These crystals are deposited beneath the epithelium and are sometimes sloughed into the lumen. Reactive adjustments in the rete testis, together with cystic transformation, are frequent. Ductules efferentes show pseudostratified epithelium of large columnar cells with clear cytoplasm. Patients with quiescent Crohn, ulcerative colitis, or indeterminate (unclassified) colitis are normally as fertile as the general population, although those with active Crohn illness and ulcerative colitis have problems with fertility (27% and 24% of patients, respectively). Zinc deficit may be responsible for comparable alterations in Crohn illness, apparently associated to the extent of intestinal involvement and severity of signs. The most frequent medical symptoms in kids are acroparesthesia, hypohidrosis, and cornea verticillata. Other signs such as tinnitus, recurrent vertigo, headache, diminished degree of activity, fatigue, and despair can also be observed. Seminiferous tubules show most frequent type of major hyperoxaluria is kind I, attributable to poor or absent exercise of liver-specific peroxisomal alanine/ glyoxylate aminotransferase enzyme. Renal results embrace recurrent nephrolithiasis, nephrocalcinosis, and early renal failure. Involvement of the genital tract varies from hypergonadotropic hypogonadism with azoospermia and low serum testosterone to patients with normal testicular perform and paternity. Both basal and principal cells of the epididymis present pale and vacuolated cytoplasms, because of lipid deposits. Clinical manifestations could start with what it is named "Fabry crisis" (strong, burning pain within the palms and ft related to fever and elevated erythrocyte sedimentation rate). The deposits noticed in the ductus epididymidis epithelium include a number of, parallel-arranged laminae (zebra bodies). Sertoli cells accumulate lipids, and germ cells are restricted to a quantity of spermatogonia.
Purchase goutichine 0.5mg free shippingRetroperitoneal lymphadenectomy for scientific stage A testis cancer (1965 to 1989): modifications of method and impact on ejaculation antibiotic 3 2 order goutichine 0.5mg with amex. Uninfected anastomotic false aneurysms following arterial reconstruction with prosthetic grafts bacteria quizzes cheap 0.5mg goutichine free shipping. Anastomotic aneurysms after vascular reconstruction: problems of incidence antibiotic resistant std purchase goutichine 0.5mg mastercard, etiology and therapy antibiotic ointment for cats buy 0.5 mg goutichine overnight delivery. Durability of open restore of infrarenal stomach aortic aneurysm: a 15-year follow-up study J Vasc Surg. Femoral anastomotic aneurysms: pathogenic elements, scientific shows and therapy. Impending aortoenteric hemorrhage: the impact of early recognition on improved outcome. The aortofemoral graft: detection and identification of healing issues by ultrasonography Surgery. Endovascular restore of paraanastomotic aneurysms after earlier open aortic prosthetic reconstruction. Endovascular repair of paraanastomotic aneurysms of the aorta and iliac arteries: most popular therapy for a posh drawback. Endovascular remedy of anastomotic pseudoaneurysms after aorto-iliac surgical reconstruction. Hemorrhage and thrombosis as early issues of femoropopliteal bypass grafts: causes, treatment, and prognostic implications. Treatment of acute peripheral arterial and graft thromboses with low-dose streptokinase. Blood transfusion is associated with increased morbidity and mortality after decrease extremity revascularization. Failure of autogenous reversed saphenous vein femoropopliteal grafting: Pathophysiology and prevention. The significance of vein wall thickness and diameter in relation to the patency of femoropopliteal saphenous vein bypass grafts. Intimal hyperplasia as a complication of the use of the polytetrafluoroethylene graft for femoral-popliteal bypass. Platelet mechanisms in the genesis and prevention of graft related vascular damage reactions and thromboembolism: nature of the vascular interface. Biologic fate of autogenous vein implants as arterial substitutes: Clinical, angiographic and histopathologic observations in femoro-popliteal operations for atherosclerosis. A decade of experience with dorsalis pedis artery bypass: evaluation of end result in more than a thousand cases. Randomization of autogenous vein and polytetrafluorethylene grafts in femoral-distal reconstruction. Above-knee polytetrafluoroethylene femoropopliteal bypass graft: is it an affordable different to the below-knee reversed autogenous vein graft Femoropopliteal and tibioperoneal artery reconstruction using human umbilical vein. The impact of a venous anastomosis Tyrell vein collar on the first patency of arteriovenous grafts in patients present process hemodialysis. Interposition vein cuff anastomosis alters wall shear stress distribution within the recipient artery J Vasc Surg. Heparin-bonded Dacron or polytetrafluorethylene for femoropopliteal bypass: five-year results of a potential randomized multicenter medical trial. Effectiveness of reoperation after late failure of femoropopliteal reconstruction. Postoperative surveillance of femoro-distal grafts: the application of echo-Doppler (duplex) ultrasonic scanning. Is balloon angioplasty of perianastomotic stenoses of failing peripheral arterial bypasses worthwhile Endoscopic intravascular surgery removes intraluminal flaps, dissections, and thrombus. Thrombolytic therapy for delayed occlusion of knitted Dacron bypass grafts in the axillofemoral, femoropopliteal and femorotibial positions. Local thrombolysis in the therapy of thrombosed arteries, bypass grafts, and arteriovenous fistulas. Recanalization of completely occluded femoropopliteal vein grafts with low-dose streptokinase infusion. Lysis of arterial clot by intravenous or intra-arterial administration of streptokinase. Streptokinase after late failure of reconstructive surgery for peripheral arteriosclerosis. Intraoperative fibrinolytic remedy: an adjunct to catheter thromboembolectomy J Vasc Surg. Long-term consequence of infrainguinal bypass grafting in patients with serologically proven hypercoagulability J Vasc. Platelet consumption by arterial prostheses: the results of endothelialization and pharmacologic inhibition of platelet perform. Reoperations and different reinterventions for thrombosed and failing polytetrafluoroethylene grafts. The relative importance of graft surveillance and warfarin therapy in infrainguinal prosthetic bypass failure. Surgical wound infections after vascular surgical procedure: potential multicenter observational study Scand J Surg. Wound complications of autogenous subcutaneous infrainguinal arterial bypass surgery: predisposing components and administration. Prospective study of wound issues in steady infrainguinal incisions after lower limb arterial reconstruction: incidence, risk elements, and value. Female gender and oral anticoagulants are associated with wound complications in decrease extremity vein bypass: an analysis of 1404 operations for critical limb ischemia. Influence of renal insufficiency on limb loss and mortality after preliminary decrease extremity surgical revascularization. Angioscopy guided in situ bypass versus angioscopy guided non reversed bypass for infrainguinal arterial reconstructions. Are wound therapeutic disturbances and size of hospital keep reduced with minimally invasive vein harvest Evaluation of endoscopic vein extraction on structural and useful viability of saphenous vein endothelium. Endoscopic vein harvesting for coronary bypass grafting: a blessing or a malicious program Durability of the in situ saphenous vein arterial bypass: a comparison of primary and secondary patency J Vasc Surg. Is early postoperative duplex scan surveillance of leg bypass grafts clinically essential Prospective validation of threshold criteria for intervention in infrainguinal vein grafts present process duplex surveillance. The importance of routine surveillance of distal bypass grafts with duplex scanning: a study of 379 reversed vein grafts.
References - Tomaszewski JE, Landis JR, Russack V, et al: Biopsy features are associated with primary symptoms in interstitial cystitis: results from the Interstitial Cystitis Data Base study, Urology 57(6 Suppl 1):67n81, 2001.
- Albers P, Siener R, Kliesch S, et al: Risk factors for relapse in clinical stage I nonseminomatous testicular germ cell tumors: results of the German Testicular Cancer Study Group Trial, J Clin Oncol 21:1505n1512, 2003.
- Asao T, Kuwano H, Nakamura J, Morinaga N, Hirayama I, Ide M. Gum chewing enhances early recovery from postoperative ileus after laparoscopic colectomy. J Am Coll Surg 2002;195(1):30- 32.
- Lunde K, Solheim S, Aakhus S, et al: Intracoronary injection of mononuclear bone marrow cells in acute myocardial infarction. N Engl J Med 2006;355:1199-1209.
- Gaujoux S, Gonen M, Tang L, et al. Synchronous resection of primary and liver metastases for neuroendocrine tumors. Ann Sug Oncol. 2012;19(13): 4270-4277.
- Irwin, B.H., Pradeep, P.R., Stein, P.J., Desai, M.M. Laparoendoscopic single site surgery in urology. Urol Clin North Am 2009;36:223-235.
- Lack EB. Safety of ultrasonic-assisted liposuction (UAL) using a non-water-cooled ultrasonic cannula. A report of six cases of disproportionate fat deposits treated with UAL. Dermatol Surg. 1998;24(8):871-4.
|

