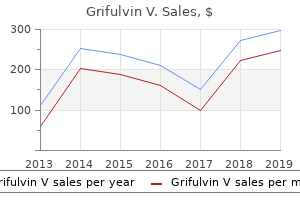
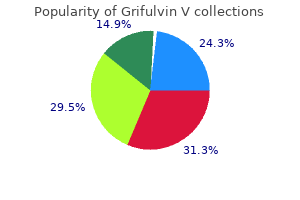
Grifulvin V
Isabel Filges, M.D. - Medical Genetics
- University Hospital Basel
- Switzerland
Order grifulvin v 250 mg without prescriptionA conservative and minimally invasive strategy to necrotizing pancreatitis improves consequence antifungal wipes generic grifulvin v 250 mg mastercard. Organ failure and an infection of pancreatic necrosis as determinants of mortality in sufferers with acute pancreatitis antifungal homeopathic generic grifulvin v 250 mg online. Persistent organ failure in the course of the first week as a marker of deadly consequence in acute pancreatitis fungus gnats organic control generic 250mg grifulvin v visa. Association between early systemic inflammatory response fungus cave neopets proven grifulvin v 250mg, severity of multiorgan dysfunction and demise in acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September eleven via thirteen, 1992. Update on acute pancreatitis: ultrasound, computed tomography, and magnetic resonance imaging options. Prediction of mortality in acute pancreatitis: a scientific evaluate of the revealed evidence. Dynamic nature of early organ dysfunction determines consequence in acute pancreatitis. Faster price of initial fluid resuscitation in extreme acute pancreatitis diminishes in-hospital mortality. Early fluid resuscitation reduces morbidity among patients with acute pancreatitis. Rapid hemodilution is associated with elevated sepsis and mortality among sufferers with extreme acute pancreatitis. Randomized clinical trial of specific lactobacillus and fibre complement to early enteral diet in sufferers with acute pancreatitis. Synbiotic management of irritation and infection in extreme acute pancreatitis: a prospective, randomized, double blind examine. Probiotic prophylaxis in predicted severe acute pancreatitis: a randomised, double-blind, placebo-controlled trial. Antibiotic therapy for prophylaxis against an infection of pancreatic necrosis in acute pancreatitis. Systematic evaluation and meta-analysis of antibiotic prophylaxis in extreme acute pancreatitis. Controlled medical trial of selective decontamination for the therapy of extreme acute pancreatitis. Effect of selective decontamination on antimicrobial resistance in intensive care models: a scientific evaluate and meta-analysis. Gastrointestinal motility and gastric tube feeding in mechanically ventilated patients. Nutritional strategy in malnourished surgical sufferers: a potential randomized research. Management of nutrition in European intensive care units: results of a questionnaire. Working group on metabolism and diet of the European Society of Intensive Care Medicine. Intestinal hypoperfusion contributes to intestine barrier failure in severe acute pancreatitis. Bacterial translocation and infected pancreatic necrosis in acute necrotizing pancreatitis derives from small bowel quite than from colon. Early endoscopic retrograde cholangiopancreatography in predicted extreme acute biliary pancreatitis: a potential multicenter study. Lack of consensus on the role of endoscopic retrograde cholangiography in acute biliary pancreatitis in printed meta-analyses and pointers: a systematic review. Systematic review of percutaneous catheter drainage as primary remedy for necrotizing pancreatitis. Efficacy of conservative treatment, without necrosectomy, for infected pancreatic necrosis: a scientific review and meta-analysis. Feasibility of minimally invasive approaches in sufferers with contaminated necrotizing pancreatitis. Management of contaminated pancreatic necrosis utilizing retroperitoneal necrosectomy with flexible endoscope: 10 years of expertise. Three-port retroperitoneoscopic necrosectomy in management of acute necrotic pancreatitis. Treatment of severe acute pancreatitis by way of retroperitoneal laparoscopic drainage. Endoscopic ultrasound-guided versus standard transmural drainage for pancreatic pseudocysts: a prospective randomized trial. Non-fluoroscopic endoscopic ultrasound-guided transmural drainage of symptomatic non-bulging walled-off pancreatic necrosis. Preliminary report on a model new, totally covered, steel stent designed for the therapy of pancreatic fluid collections. Factors impacting treatment outcomes within the endoscopic administration of walled-off pancreatic necrosis. Dual-modality drainage of contaminated and symptomatic walled-off pancreatic necrosis: long-term clinical outcomes. Outcomes after implementing a tailor-made endoscopic step-up strategy to walled-off necrosis in acute pancreatitis. Interventions for necrotizing pancreatitis: abstract of a multidisciplinary consensus convention. Diagnostic strategy and timing of intervention in contaminated necrotizing pancreatitis: an international professional survey and case vignette study. Clinical perspectives in pancreatology: compliance with acute pancreatitis pointers in Germany. Appropriate timing of cholecystectomy in patients who present with reasonable to extreme gallstone-associated acute pancreatitis with peripancreatic fluid collections. The role of routine fine-needle aspiration within the diagnosis of contaminated necrotizing pancreatitis. Debridement and closed packing for sterile or contaminated necrotizing pancreatitis: insights into indications and outcomes in 167 sufferers. Role of ultrasonographically guided fine-needle aspiration cytology within the analysis of infected pancreatic necrosis. Declining morbidity and mortality charges in the surgical management of pancreatic necrosis. Surgical decompression for abdominal compartment syndrome in severe acute pancreatitis. Intra-abdominal hypertension and the stomach compartment syndrome: up to date consensus definitions and clinical apply tips from the World Society of the Abdominal Compartment Syndrome. Percutaneous necrosectomy and sinus tract endoscopy in the administration of infected pancreatic necrosis: an preliminary experience. A method for laparoscopic-assisted percutaneous drainage of infected pancreatic necrosis and pancreatic abscess. Matthews ninety two C hronic pancreatitis is a progressive inflammatory dysfunction that leads to irreversible destruction of the exocrine and endocrine tissue of the pancreas. Fibrotic substitute of the traditional pancreas could also be associated with persistent abdominal ache, the development of exocrine insufficiency, and in the end, diabetes mellitus.
Safe grifulvin v 250 mgIncidence Gastric carcinoids have lengthy been thought-about rare lesions facial fungus definition grifulvin v 250mg discount, but with an increasing use of upper endoscopy and the growing use of proton pump inhibitors antifungal wash for dogs grifulvin v 250mg visa, their incidence is growing antifungal with alcohol purchase grifulvin v 250mg on-line. Over a interval of fifty years antifungal prescription 250 mg grifulvin v otc, the proportion of gastric carcinoids among all carcinoid tumors has increased from 2. The prognosis is made at gastroscopy by biopsies, which ought to be taken of the largest polyps in addition to from the antrum (two biopsies) and fundus (four biopsies). The function of biopsies is to verify that the polyps characterize carcinoid quite than extra benign (inflammatory polyps or hyperplastic polyps) or extra malignant pathologies (adenocarcinoma). In addition, the normal mucosa is sampled in order that the analysis of associated atrophic gastritis may be confirmed. Endoscopic ultrasound and cross-sectional imaging ought to be thought-about for tumors bigger than 1 cm. The principles of therapy embrace resection with extensively negative margins, formal lymphadenectomy, and assessment of metastatic illness. Those with metastatic disease may be thought-about for either surgical or percutaneous remedy of hepatic metastases in conjunction with resection of the primary, whereas these with extensively metastatic disease ought to have gastric surgical procedure only as a method of symptom management. Nearly 400 sufferers undergoing treatment for type I gastric carcinoid have been cumulatively reported by a number of teams. The overall disease-specific survival in most collection was one hundred pc, with a follow-up on the order of 5 years. Furthermore, a mixture of conservative and aggressive strategies was used, making it troublesome to kind out natural historical past from therapy impact. The perfect remedy strategy would of course be capable of determine those at highest threat for locoregional disease and treat them accordingly. Antrectomy and native resection is advised with lymphadenectomy added just for patients with positive nodes. Although they express settlement with the brink of 1 cm for surgical remedy, more than half of the sufferers who underwent resection of their series had tumors lower than 1 cm. They particularly disagree that the variety of lesions ought to guide a decision with regard to surgical therapy. As extra information accumulate, we shall be able to determine which sufferers would most benefit from surgical intervention, what the correct place of antrectomy is for these sufferers, and the way massive the good factor about surgical remedy will be for patients with a relatively indolent disease process. They can current in a protean fashion, with the symptoms mostly being obscure abdominal pain, bloating, diarrhea, weight loss, and intermittent bowel obstruction. This can happen both as a direct consequence of the tumor itself, with both luminal compromise or as a lead level for intussusception. This can lead to extensive fibrosis and kinking of the small bowel, with resultant obstruction. These tumors are multifocal in 25% of affected sufferers, particularly within the ileum. Importantly, clonality research have instructed that multiple tumors are metastases from the first tumor quite than distinct primaries. Prognostic indicators for carcinoid neuroendocrine tumors of the gastrointestinal tract. At presentation, solely 31% of small bowel tumors are localized, 37% are regional, and 27% are distant. The estimates for lymphatic metastases from small bowel tumors less than 1 cm in measurement range from 11% to 44%. The 5-year survival of the most favorable group of sufferers with small bowel carcinoids (T1, N0) is only 86%, suggesting that early tumors can still behave aggressively. This typically occurs when liver lesions are detected by ultrasound and then additional imaging is undertaken. With cross-sectional imaging, the bowel, liver, and peritoneal cavity can all be adequately evaluated. Octreotide scanning may be very helpful for disease staging and is positive in more than 80% of sufferers with small bowel carcinoids. Its limitations are for small lesions and those tumors lacking sorts 2 and 5 somatostatin receptors. Capsule endoscopy should be used solely with caution provided that, in patients with important small bowel tethering and luminal disease from carcinoid, it could result in obstruction. Treatment It is essential in all cases of small bowel carcinoid to think about the potential of different concomitant malignancies, reported to occur in 12% to 46% of instances. Furthermore, at exploration, an intensive search of the stomach cavity ought to all the time be undertaken. Resection of small bowel carcinoids entails segmental resection with broad mesenteric lymphadenectomy. These sufferers often have significantly foreshortened mesenteries and in depth fibrotic modifications throughout the mesentery that can make this procedure difficult and unsafe. These troublesome instances could be approached by mobilizing the right colon and small bowel mesenteries off of the retroperitoneum and isolating the mesenteric vessels as they exit close to the pancreatic neck. The vessels can then be dissected from the foundation out into the mesentery, peeling the nodes rigorously away from the vasculature. This approach requires delaying the bowel resection till after the mesenteric dissection is completed to protect a maximum size of well-perfused bowel. Colonic carcinoids are bigger tumors with a median dimension of 5 cm at diagnosis and are metastatic in 40% of sufferers at presentation. In distinction, rectal carcinoids are most frequently detected incidentally or with signs of rectal bleeding or pain. In distinction, serum chromogranin is very delicate and must be measured routinely. These tumors have a typical look, as sessile, submucosal tumors with a discolored, yellowed mucosal overlaying. The margins should be carefully examined to decide if further remedy is required. Endoscopic ultrasound also performs a role in the evaluation of rectal carcinoids to help in staging and figuring out suitability for endoscopic resection. For high-grade colonic lesions, a metastatic analysis ought to be undertaken with cross-sectional imaging of the chest and abdomen and an octreotide scan. Approximately three-fourths of appendiceal carcinoids are positioned in the tip of the appendix, and 95% of appendiceal carcinoids are lower than 2 cm in diameter. Careful pathologic analysis of the appendix is required and may embody tumor dimensions, depth of invasion, mitotic fee, and the presence or absence of lymphovascular invasion. Formal right hemicolectomy is at present really helpful for any one of many following: tumors higher than 2 cm in dimension, invasion on the appendiceal base, evidence of lymphovascular invasion, any invasion of the mesoappendix, blended histology (goblet cell carcinoids, adenocarcinoids), and intermediate- to high-grade tumors. For small, incidentally detected colonic carcinoids completely removed with polypectomy, endoscopic surveillance alone ought to be thought of. However, for tumors that are larger than 2 cm and invade the muscularis propria, formal colectomy with lymphadenectomy ought to be undertaken. In basic, it is suggested that rectal tumors that are larger than 2 cm, invade the muscularis propria (regardless of size), or have evidence of mesorectal lymphadenopathy ought to be managed by commonplace rectal resection techniques. For tumors lower than 10 mm in dimension, some counsel that endoscopic resection alone is adequate,55 nevertheless it has been proven that the incidence of lymph node positivity in subcentimeter rectal carcinoids may be as high as 7%. It has subsequently been suggested that rectal carcinoids lower than 2 cm in dimension be thought-about for formal resection if the tumor penetrates the muscularis or has antagonistic features similar to a excessive proliferative index, lymphovascular invasion, or gross ulceration.
Diseases - Chromosome 1, monosomy 1q25 q32
- Ichthyosis, keratosis follicularis spinulosa Decalvans
- Epidermolysis bullosa, dermolytic
- Sparse hair ptosis mental retardation
- Acroosteolysis osteoporosis skull and mandible changes
- Gynecomastia
- MAT deficiency[disambiguation needed]
- Mental retardation short stature hypertelorism
- Homologous wasting disease
Buy 250mg grifulvin v with amexThe proximal jejunum is split about 30 cm from the ligament of Treitz and a jejunojejunostomy is made fungus gnats rockwool grifulvin v 250 mg lowest price, making a Roux limb roughly 40 to 60 cm lengthy definition of fungus mold discount 250 mg grifulvin v amex. The cystojejunostomy anastomosis is fashioned with sutures or a surgical stapler according to fungus gnats beer purchase grifulvin v 250 mg line surgeon choice antifungal generic drugs purchase grifulvin v 250 mg with mastercard. A longitudinal duodenotomy must be used to expose the medial wall of the duodenum. An aspirating needle can be used to identify the world of nearest apposition of the pseudocyst to the duodenal wall. When creating the 2- to 3-cm-long cystoduodenostomy, caution should be taken to avoid harm to the gastroduodenal artery, in addition to the frequent bile duct or the primary pancreatic duct. If those buildings impede clear entry to the pseudocyst from the medial duodenal wall, a cystojejunostomy could also be preferable. The lateral duodenotomy is then closed in a single or two layers and a closed-suction drain could also be positioned per surgeon desire. Historically, a lateral side-to-side cystoduodenostomy has a excessive price of morbidity and mortality related to anastomotic dehiscence and abscess formation, and due to this fact it ought to rarely (if ever) be carried out. Nealon and Walser studied 103 patients with pseudocyst and continual pancreatitis with a major pancreatic duct diameter of greater than 7 mm who received longitudinal pancreaticojejunostomy (Puestow procedure) alone for duct drainage or surgical cystojejunostomy mixed with duct drainage. The wall of the pseudocyst should be mature and thick enough to hold suture for anastomosis, which is often true more than 6 weeks after the initial appearance of the pseudocyst. In chronic pancreatitis, surgery for a pseudocyst could proceed as quickly as any acute inflammation has subsided. Given the usual important irritation from the antecedent pancreatitis, dissection across the pseudocyst should be minimized whenever attainable. Residual debris or necrotic material inside the pseudocyst cavity should also be gently suctioned or debrided previous to anastomosis. Cystogastrostomy, Roux-en-Y cystojejunostomy, or cystoduodenostomy are options for inner drainage depending on the anatomic location of the pseudocyst. Especially in cases of big pseudocysts, the anastomosis ought to be positioned to optimize dependent drainage of the pseudocyst. Cystogastrostomy When the anterior pseudocyst wall is seen to be directly opposed to the posterior abdomen wall from its location in the lesser sac, generally cystogastrostomy is the internal drainage process of alternative. This approach includes a longitudinal gastrotomy on the stage of the anterior wall of the stomach, sometimes within the body. The bulge of a large pseudocyst can be visualized by pressing into the posterior abdomen wall, or an aspirating needle can be utilized to localize a smaller lesion. The pseudocyst is entered by incision (or excisional biopsy) of the posterior abdomen wall no less than three cm lengthy and the pseudocyst contents are suctioned out. There have been no pseudocyst recurrences in the cohort with duct drainage alone over a mean follow-up of greater than 5 years, and 89% of patients had full decision of their preoperative ache symptoms. Toward the top of this examine, the index pseudocyst was addressed by a single intraoperative aspiration through the ductal drainage procedure. There are data that counsel surgical intervention in chronic pancreatitis may be extra environment friendly and efficient for ache aid than endoscopic interventions. Pancreatic Resection Partial pancreatic resection is usually not thought of the primary choice in the therapy of pseudocysts due to the resultant decrease in pancreatic endocrine and exocrine function and the more intensive surgical dissection required in an space of chronic irritation and fibrosis. Patients with a small pancreatic remnant less than 6 cm lengthy and the presence of splenic vein thrombosis were most likely to have distal pancreatectomy and splenectomy. Other patients treated through resection of the left pancreatic remnant had a small pancreatic duct unsuitable for anastomosis. Pseudocysts in the pancreatic head of sufferers receiving surgery for symptoms of persistent pancreatitis may be eliminated together with a duodenum-preserving pancreatic head resection or Whipple process, to guarantee postoperative ache aid. Disconnected pancreatic duct syndrome: illness classification and administration methods. External Drainage Open external drainage of a pseudocyst often creates a controlled pancreaticocutaneous fistula and is related to delayed closure of the fistula, depending on the degree of communication with the underlying pancreatic duct. When emergent surgical procedure is undertaken to control hemorrhage or peritonitis from pseudocyst rupture, external drainage will be the most expedient temporizing motion. If the pseudocyst wall is unexpectedly too thin and immature for anastomosis, external drainage may be performed. In operations when a deliberate inside drainage procedure is anatomically unachievable due to adhesions, then external drainage of the pseudocyst is an affordable "bailout" choice. If an contaminated pseudocyst is encountered at the time of necrosectomy for an acute necrotic collection, exterior drainage of the pseudocyst can also be warranted. Once adequately drained, the pseudocyst cavity obliterates and fuses to the wall of the organ to which it was anastomosed. These modern sequence demonstrate the continued significance of surgical remedy for pancreatic pseudocysts. No Endoscopic or surgical internal drainage process Yes Surgery Duct extensive sufficient for anastomosis Yes Endoscopic or surgical cystogastrostomy or cystoduodenostomy or cystojejunostomy No Yes Transpapillary pancreatic duct stent placement No Successful decompression of pseudocyst Additionally, prior catheter drainage from a percutaneous or surgical intervention for pancreatitis might result in an external pancreatic fistula. Severe disruption of the pancreas from blunt or penetrating trauma can also cause an inner pancreatic fistula. Pseudocysts managed with out intervention can progress to rupture lower than 5% of the time and kind an inner pancreatic fistula. Although this event can occasionally be detected by way of sudden symptoms of ache, hemorrhage, or chemical peritonitis requiring emergent intervention, extra usually the internal fistula develops silently and is detected as signs of belly discomfort, shortness of breath, or bowel obstruction slowly progress. These patients often had a residual pseudocyst cavity suitable for cystojejunostomy, but 18% required fistula tract�jejunostomy due to prior collapse of the pseudocyst and 11% required distal pancreatectomy as a result of the fistula emanated from a disconnected left pancreatic remnant. The exterior drain (D) is injected with distinction medium, which opacifies an area of walled-off pancreatic necrosis (N), the fistula (arrow), and descending colon (C). Pancreaticocolonic fistulas secondary to extreme acute pancreatitis treated by percutaneous drainage: successful nonsurgical outcomes in a single-center case series. Although in some cases this could lead to fortuitous decompression and determination of a pseudocyst or walled-off pancreatic necrosis, the inflammatory means of fistula formation more usually causes hemorrhage or sepsis from infected pancreatic necrosis. A pancreaticoenteric fistula might develop de novo or as a complication following manipulation by necrosectomy or closed drainage. In a current study of 311 patients with acute pancreatitis and infected necrosis, 38% developed pancreaticoenteric fistulas and 61% of fistulas concerned the colon. Fluid analysis is the vital thing to the analysis of pancreatic ascites or pancreaticopleural fistula, because most of these internal pancreatic fistula are classically the sequelae of an indolent course of persistent pancreatitis and solely a minority of those sufferers will present with belly pain or tenderness on bodily examination to recommend pancreatic pathology. Note the large left pleural effusion with enhancing rim (thin red arrow in [A]), periaortic fistulous tract extending from stomach into mediastinum (bold purple arrows in [B] and [C]), and pancreatic pseudocyst deep to the dilated main pancreatic duct (green arrow in [D]).
250 mg grifulvin v free shippingIn an identical fashion fungus za mdomoni discount grifulvin v 250mg with amex, pressing operation should be thought-about for most sufferers with penetrating injuries fungus eye eq buy grifulvin v 250 mg low cost. With coaching and apply zeasorb antifungal treatment buy grifulvin v 250 mg on-line, the sensitivity and specificity for detection of fluid in these views is 83% and ninety nine fungus gnats self watering pot discount grifulvin v 250mg with mastercard. If concern for hemoperitoneum persists, the patient might require an exploratory laparotomy as a diagnostic and doubtlessly therapeutic modality. Guidelines generated by the Western Trauma Association, the Eastern Association for the Surgery of Trauma, and, extra just lately, the World Society of Emergency Surgery every provide essential course within the care of these patients. Nonoperative administration is extra common in patients with accidents from blunt trauma. A study of patients from the National Trauma Data Bank examined the position of nonoperative administration in patients with high grade (Abbreviated Injury Scale of four or higher) liver accidents. Of observe, failed nonoperative management was independently related to greater mortality. Predictors of want for conversion to operative administration included older age, female gender, larger damage severity rating, and hypotension. Need for blood transfusion or the incidence of hemodynamic instability prompts thorough reassessment and consideration of angiography or operation. In a hemodynamically unstable patient with no extra injuries, we pursue selective angioembolization primarily quite than proceeding to laparotomy. Our follow is to "bring the surgical intensive care unit to the patient" and proceed lively resuscitation with the intensive care unit and trauma group no matter physical location. The use of an upper belly retraction system significantly facilitates exposure of the liver. If further exposure is required, the incision may be extended laterally in a subcostal path or cephalad both partially or fully via the sternum. Although a median sternotomy may be required to management life-threatening bleeding, opening the sternum for a bicavitary process will increase evaporative heat loss and will worsen coagulopathy. The conduct of the operation might be determined to a considerable degree by the extent of hemoperitoneum encountered and the location of the presumed source of bleeding. If a big volume of free blood is encountered, packs must be positioned in the four quadrants of the abdomen in an attempt to decide the first site of bleeding. If liver bleeding could be controlled with packs initially, these can be left in place whereas different potential injuries are evaluated and addressed. A significantly injured spleen ought to be eliminated promptly and any concomitant gastrointestinal accidents quickly evaluated and managed. When addressing hemorrhage from the liver, a sequence of operative maneuvers could also be employed to acquire hemostasis. These injuries can normally be managed by compression and momentary packing alone or with electrocautery, argon beam coagulation, with adjunct use of topical hemostatic agents. Packing with temporary abdominal closure will not often be required for isolated low-grade accidents. In our follow, we usually initially carry out manual compression and perihepatic packing then permit resuscitation of the affected person and transfusion of blood products as wanted. Compression and packing often result in momentary hemorrhage control and allow definitive hemorrhage management. We sometimes transfuse in a balanced ratio of packed purple blood cells, plasma, and platelets (1: 1: 1) with minimal infusion of crystalloid, as this technique has been demonstrated to cut back mortality and morbidity from hemorrhage in trauma sufferers. The technique employed will depend on the geometry and depth of the wound in addition to the nature of the injured vessels. In basic, direct suture ligation of vessels is preferable to management with surgical clips due to the susceptibility of the latter to dislodge with manipulation of the liver. As wanted, use of the finger fracture technique can be used to expose and allow ligation of deeper vessels. We also discover the use of stapling units useful in the occasion that elimination of devitalized tissue is needed or to management hemorrhage with a restricted hepatic resection. We additionally discover that reapproximation of hepatic parenchyma with adjunct use of hemostatic brokers will lead to cessation of bleeding in plenty of accidents. This can then be exchanged for a mild, noncrushing fine vascular clamp or umbilical tape with a Rumel tourniquet to get hold of more secure control. The duration of protected occlusion of the porta hepatis within the setting of traumatic injury with concomitant hypotension and shock is unknown. Western Trauma Association critical determination in trauma: nonoperative management of blunt hepatic trauma. In the event of penetrating trauma to the liver with uncontrolled hemorrhage, balloon occlusion of the wound could additionally be lifesaving. This is passed by way of the trail of the projectile and then inflated till hemorrhage control is achieved. In most circumstances, the patient undergoes resuscitation and hepatic packing, adopted by selective angioembolization. There are additionally stories of the usage of in depth tractotomy for publicity of deep arterial bleeding. Hepatorrhaphy or reapproximation of the liver parenchyma may be useful for control of venous bleeding or bile leakage. Critics of the process argue that using massive sutures may cause necrosis of hepatic tissue, which could be minimized with management of pressure on the sutures. Attempting to management oozing from nonviable liver is an inappropriate use of hepatorrhaphy, as this tissue should be d�brided. However, small bleeding cracks can typically be closed with the arrest of hemorrhage by this method with out inflicting tissue necrosis or unnecessarily extending the wound by tractotomy or finger fracture. We have additionally encountered giant injuries with significant lacerations within the liver with little bleeding from the uncovered surfaces. After compression and control of larger vessels, hepatorrhaphy is performed with absorbable suture on a large blunt needle (right). This method may be augmented by an omental flap, packing with topical hemostatic brokers, or each. Omental pedicle flaps may be very helpful for prevention of diffuse oozing from uncooked surfaces of the liver. The omental flap is created in a regular style and is utilized in our practice to cover giant exposed liver surfaces. In the bizarre instance the place a subcapsular hematoma has ruptured or been surgically entered, diffuse bleeding from the exposed liver floor normally ensues. However, there are several situations the place a major hepatic resection is indicated: devitalizing injuries alongside anatomic planes, completion lobectomy when the harm has transected the liver alongside lobar anatomy, and for exposure of main venous bleeding associated with a significant hepatic parenchymal harm. The use of hepatic artery embolization has often resulted in lobar hepatic necrosis that requires a formal lobectomy for resolution. The use of techniques employed by elective hepatic surgeons similar to vascular and hepatic staplers is a helpful adjunct in such cases. Formal resection may be performed in delayed fashion at a re-assessment operation to delineate and d�bride necrotic hepatic tissue following the initial packing and correction of coagulopathy. Major hepatic venous injuries confined to the liver parenchyma can typically be efficiently managed by suture ligation. Once major bleeding has been lessened, packing could additionally be used to management the remaining bleeding.
Grifulvin V: 250 mg, 125 mg
Buy grifulvin v 250 mg with mastercardIf advanced liver illness exists anti fungal meds cheap 250mg grifulvin v overnight delivery, hepatic artificial perform could be impaired anti fungal shampoo discount grifulvin v 250 mg without a prescription, with lowered serum albumin and a prolongation of prothrombin time fungus gnats carnivorous plants effective 250 mg grifulvin v. After open cholecystectomy kaufmann antifungal diet order 250 mg grifulvin v with visa, only approximately 10% of postoperative strictures are actually suspected throughout the first week, however practically 70% are diagnosed within the first 6 months, and more than 80% are diagnosed within 1 yr of surgical procedure. In collection reporting bile duct injuries during laparoscopic cholecystectomy, the damage is normally acknowledged either in the course of the procedure (25% to 30%) or, more generally, in the early postoperative interval. Patients suspected of having a postoperative bile duct injury within days to weeks of initial operation often present in considered one of two methods. One presentation is the progressive elevation of liver perform check results, notably total bilirubin and alkaline phosphatase levels. These modifications can usually be seen as early because the second or third postoperative day. The second mode of early presentation is with leakage of bile from the injured bile duct. This presentation appears to happen most often in patients presenting with bile duct injuries after laparoscopic cholecystectomy. Bilious drainage from operatively placed drains or by way of the wound after cholecystectomy is abnormal and represents some type of biliary damage. In sufferers with out drains (including sufferers in whom the drains have been removed), the bile can leak freely into the peritoneal cavity or it could loculate as a group. Free accumulation of bile into the peritoneal cavity results in either biliary ascites or bile peritonitis. Similarly, a loculated bile assortment can lead to sterile biloma or in an infected subhepatic or subdiaphragmatic abscess. Patients with postoperative bile duct strictures who current months to years after the initial operation incessantly have proof of cholangitis. Less commonly, sufferers may current with painless jaundice and no proof of sepsis. Finally, sufferers with markedly delayed diagnoses might current with superior biliary cirrhosis and its issues. In patients who current within the early postoperative period with evidence of a bile leak or biliary sepsis, these research are helpful to rule out the presence of intraabdominal collections that might require drainage. Both research can confirm biliary obstruction by demonstrating a dilated biliary tree. In patients suspected of getting early postoperative bile duct damage, a radionucleotide biliary scan can verify bile leakage. In patients with postoperative external bile fistula, injection of water-soluble contrast media through the drainage tract/drain (sinography) can often define the site of leakage and the anatomy of the biliary tree. These catheters can be of assistance in surgical reconstruction and supply entry to the biliary tree for nonoperative dilation. This finding is frequently the case in patients with damage during laparoscopic cholecystectomy, when the distal bile duct is often clipped and divided. A surgical drain is in place, as well as a duodenal feeding tube (which crosses obliquely over the frequent hepatic duct). The administration of a suspected bile duct injury after laparoscopic cholecystectomy presenting with a bile leak deserves particular point out. Often, when bile leakage is suspected, the surgeon believes that pressing surgical exploration is important. Unfortunately, at laparotomy, the marked irritation associated with bile spillage and the small decompressed biliary tree that appears retracted excessive into the porta hepatis make recognition of the injury and repair virtually inconceivable. Delayed reconstruction, aided by percutaneous biliary catheters, then allows optimum surgical results. Biliary drainage is greatest accomplished by the transhepatic methodology, though profitable endoscopic stent placement may additionally be achieved. Parenteral antibiotics and biliary drainage should be continued until sepsis is managed. In sufferers who present with jaundice but with out cholangitis, cholangiography ought to be carried out to outline the anatomy. Preoperative biliary decompression in sufferers with out cholangitis has not been demonstrated to improve end result. This goal is best achieved with a tension-free anastomosis between wholesome tissues. A variety of surgical alternatives exist for primary restore of bile duct strictures, including end-to-end repair, Roux-en-Y hepaticojejunostomy or choledochojejunostomy, or choledochoduodenostomy. The alternative of repair is determined by a variety of factors, together with the extent and placement of the strictures, the experience of the surgeon, and the timing of the repair. Optimally, if a bile duct injury is recognized on the time of cholecystectomy, either quick reconstruction or "injury control" steps can be employed. Unfortunately, recognition of bile duct accidents on the time of laparoscopic cholecystectomy occurs in lower than half of all instances. Patients presenting within the early postoperative period may be septic with either cholangitis or intraabdominal bile collections. Sepsis must be managed first with broad-spectrum parenteral antibiotics, percutaneous biliary drainage, and percutaneous or operative drainage of biliary leaks. The combination of proximal biliary decompression and exterior drainage allows most biliary fistulas to be controlled or even to shut. The patient can then be discharged house to enable several weeks to elapse for decision of the inflammation within the periportal region and restoration of overall health. Unfortunately, recognition of a bile duct injury is unusual during either open or laparoscopic cholecystectomy. In common, this method is used for partial transections of the bile duct when there has been no related lack of ductal length. If a segmental or accent duct lower than three mm has been injured and cholangiography demonstrates segmental or subsegmental drainage of the injured ductal system, simple ligation of the injured duct is adequate. If the harm involves the common hepatic duct or the frequent bile duct, restore also needs to be performed at the time of harm. To accomplish these goals, all repairs at the time of preliminary operation ought to involve some type of external drainage. Generous mobilization of the duodenum out of the retroperitoneum (Kocher maneuver) may be useful to assist approximate the injured ends of the bile duct. An end-to-end repair, nevertheless, must be averted if the ductal harm is close to the hepatic duct bifurcation. Although seemingly an attractive possibility, end-to-end repair is commonly related to postoperative stricture. Fortunately, such strictures can typically be successfully managed with endoscopic dilation and stenting. For proximal injuries or if the injured segment of the bile duct is larger than 1 cm in size, an end-to-end bile duct anastomosis should be prevented due to the excessive rigidity that normally exists in these conditions. In these circumstances, the distal bile duct should be oversewn, and the proximal bile duct ought to be d�brided of injured tissue and anastomosed in an end-to-side style to a Roux-en-Y jejunal limb. The use of a Roux-en-Y jejunal limb is preferable to anastomosis to the duodenum as a outcome of, in the latter case, an anastomotic leak results in a duodenal fistula. A transanastomotic Silastic stent could be positioned retrograde via the transected duct and exiting the hepatic parenchyma to enable for postoperative external drainage.
Proven 250mg grifulvin vThe tail lies in the hilum of the spleen with the splenic artery fungus jock itch cure trusted grifulvin v 250mg, which is often tortuous fungus shampoo generic grifulvin v 250 mg line, operating along the superior border of the pancreas antifungal iv buy generic grifulvin v 250 mg. The main blood supply for the pancreas arises from a number of branches of the celiac trunk and superior mesenteric arteries forming arterial arcades inside the physique and tail of the pancreas antifungal medication for cats purchase grifulvin v 250mg with visa, with the inferior and superior pancreaticoduodenal artery working along the pinnacle of the pancreas. Approximately one in every 5 sufferers has major variations within the arterial anatomy, similar to having the best hepatic artery, which usually originates from the celiac trunk, arising from the superior mesenteric artery (also generally recognized as a changed right hepatic artery) touring posterior to the pancreatic head towards the liver. This regulation is delicately balanced through the actions of the hormones insulin and glucagon. Insulin is the hormone of vitality storage; it induces a rise in amino acid uptake and facilitates glucose uptake into cells, which will increase protein synthesis and decreases lipolysis and glycogenolysis, especially after a meal or in a hyperglycemic state. Glucagon, however, is seen because the hormone of vitality release; it stimulates larger blood glucose levels by stimulating hepatic gluconeogenesis, glycogenolysis, and lipolysis within the setting of hypoglycemia, and thus counteracts the consequences of insulin. The stimulus for insulin release into the bloodstream is far greater when glucose is ingested enterally compared to the parenteral route, indicating that a feed-forward mechanism within the digestive tract is activated, anticipating the rise in blood glucose. Both are secreted by endocrine cells located in the small intestinal epithelium when the luminal focus of glucose will increase in the digestive tract, and subsequently they stimulate the cells to secrete more insulin. Hence, the great interest within the pharmaceutical trade to develop incretin-based therapies to deal with diabetes, significantly type 2 diabetes, due to its potent secretagogue effect on cells. The exocrine function is historically divided into three phases: (1) the cephalic phase, which is triggered by the sight and smell of food, contains 10% to 20% of pancreatic excretion; (2) the gastric phase, which is triggered by food entering the abdomen and gastric distention, comprises 15% to 20% of enzyme excretion; and (3) the intestinal phase, which is triggered by acidification of the duodenum and proximal jejunum, comprises 60% to 70% of meal-stimulated pancreatic excretion. The bicarbonate is transported into the ductal space by a chloride/ bicarbonate exchanger. The passage of bicarbonate and chloride throughout the ductal cell membrane generates an ionic and osmotic gradient inflicting sodium and water to observe. Patients experience the lack of acinar cells, which are a essential nidus for pancreatitis, resulting in pancreatic insufficiency. Digestive enzymes are synthesized of their inactive form inside acinar cells and are packaged into zymogen granules. The granules migrate to the cell floor and fuse to the cell membrane releasing their contents in response to vagal stimulation, peptides, and fatty acids. The intestinal brush border enzyme, enteropeptidase, cleaves trypsinogen to its lively kind, trypsin. The mutations typically trigger the untimely activation of trypsinogen to trypsin, producing a situation characterized by recurrent episodes of pancreatitis ultimately leading to pancreatic insufficiency. However, the most important limitation of serum amylase measurement to diagnose pancreatitis is the lack of specificity as a end result of several scientific circumstances can lead to elevated amylase. Serum lipase levels, on the other hand, are believed to be extra particular in diagnosing pancreatic tissue damage because lipase is just produced in the pancreas. Lipase tends to be larger in alcoholic pancreatitis and the amylase degree greater in gallstone pancreatitis, therefore the lipase-to-amylase ratio has been advised as means to distinguish between the two. This stage entails the separation of islet progenitors beginning to differentiate and losing their attachments to the basement membrane. Gut rotation will deliver the ventral lobe dorsally, ultimately fusing with the dorsal pancreatic bud (this occasion corresponds to across the sixth to seventh week of gestation in people or E12 to E13 in mice) contributing to the formation of the uncinate process and inferior part of the top of the pancreas, while the relaxation of the pancreas arises from the dorsal pancreatic bud. The complete ventral pancreatic duct and the distal part of the dorsal pancreatic duct fuse together to kind the principle pancreatic duct of Wirsung. The remaining proximal part of the dorsal pancreatic duct is either obliterated or persists as a small accent pancreatic duct of Santorini. This exclusion of mesenchyme might affect epithelial-mesenchymal interactions and lineage selection. The pancreas then undergoes major amplification of the endocrine cell population via two distinct waves of differentiation inside the pancreatic epithelium during embryogenesis, an early main wave (pre E13. Sonic hedgehog (Shh), which is a potent intercellular patterning molecule, is expressed along the whole foregut, but is noticeably suppressed in the potential pancreatic endoderm. Deletion of the notochord in chick embryo cultures leads to ectopic Shh being seen in the pancreatic area of the foregut endoderm, with subsequent failure of the pancreas to develop. The homeobox gene Hlxb9, which is transiently expressed within the endoderm within the region of the dorsal and ventral pancreatic anlage, when inactivated in mice, solely dorsal pancreatic growth is blocked. Hex-null mutant embryos have particular failure of ventral pancreatic bud development, with the dorsal bud developing normally. Endodermal patterning is manifested by the regional expression of transcription elements within the primitive gut tube; for instance, Hex1 and Nkx2. When the pancreatic mesenchyme is removed from the pancreatic epithelium in explant cultures, it leads to disrupted pancreatic cell differentiation, with the endocrine lineage being favored over exocrine. The dorsal area of the definitive endoderm, on the other hand, contributes to the formation of the esophagus, stomach, dorsal pancreas, duodenum, and intestines. The pancreas has been discovered to form because of the actions of some key particular transcription elements and signaling pathways. Another molecular pathway that has linked endodermal patterning to the initiation of pancreatic improvement is Wnt/-catenin signaling, as demonstrated in frog (Xenopus) research. Conversely, forcing excessive -catenin exercise within the posterior endoderm promotes intestinal improvement and inhibits foregut growth into liver and pancreas. Repressing -catenin in the posterior endoderm (future hindgut that usually expresses -catenin) induced ectopic liver and pancreas markers (hhex, Pdx1, elastase, and amylase) with subsequent ectopic liver bud initiation and pancreas improvement. These components promote growth and differentiation of the creating pancreas, particularly inducing progress of the endocrine cell inhabitants and speedy branching morphogenesis. These results suggest that the basement membrane has elements or elements that are conducive to ductal improvement. Impairing Notch signaling leads to premature differentiation of pancreatic progenitor cells into endocrine cells. However, the precise mechanism for Notch signaling in pancreatic lineage choice remains elusive, and ambiguity still surrounds the exact function of Notch signaling in pancreatic improvement. Shh signaling is crucial for foregut differentiation toward a gastrointestinal fate51 and its suppression within the potential pancreatic endoderm is a prerequisite for pancreas formation. There appears to be a hyperlink between aberrant Hh signaling and pancreatic exocrine neoplasia, with the upregulation of Shh ligand being noticed in noninvasive lesions previous pancreatic adenocarcinoma. However, beyond endodermal patterning, Wnt signaling has a quantity of pancreatic roles that depend on the time and place of Wnt signaling. Transgenic expression of Wnt1 or Wnt5a within the pancreatic epithelium results in pancreatic agenesis or severe hypoplasia, respectively, confirming that early Wnt signaling is detrimental to pancreatic development. Others found a job for Wnt signaling in promoting postnatal pancreatic growth,61 illustrating the complex and multiple roles that Wnt signaling performs in pancreatic development. Removal of the dorsal aorta from Xenopus embryos led to the absence of pancreatic endocrine development. Interestingly, ventral pancreas improvement appears to not be dependent on the endothelium, regardless of its close proximity to the vitelline veins. The patient lacked the pancreatic physique and tail, but not the top of the pancreas, with the latter arising from the ventral bud, which develops independently of the aortae. Islet transplantation entails an enzymatic digestion course of that additionally removes some intraislet endothelial cells. Recently it has been demonstrated that cells could be reprogrammed to form new cells during regeneration after ablating practically 99% of the present cells. However, how exactly Ngn3 controls the next specification of different endocrine subtypes stays to be fully elucidated.
Bergwohlverleih (Arnica). Grifulvin V. - Reducing pain, swelling, and complications of wisdom tooth removal.
- Bruises, aches, sprains, insect bites, and sore throats.
- Are there safety concerns?
- What is Arnica?
- Dosing considerations for Arnica.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96706
Cheap grifulvin v 250 mg lineThe innermost layer is the epithelium antifungal wash grifulvin v 250mg lowest price, and the opposite layers are the lamina propria fungus nail polish cheap 250mg grifulvin v visa, clean muscle fungal sinus buy grifulvin v 250 mg on-line, perimuscular subserosal connective tissue anti fungal gel generic grifulvin v 250mg online, and serosa. Most cells in the mucosa are columnar cells, and their main perform is absorption, however additionally they are capable of lively secretion. The lamina propria contains nerve fibers, vessels, lymphatics, elastic fibers, loose connective tissue, and occasional mast cells and macrophages. The muscle layer is a free arrangement of round, longitudinal, and oblique fibers with out well-developed layers. The subserosa is composed of a free association of fibroblasts, elastic and collagen fibers, vessels, nerves, lymphatics, and adipocytes. Rokitansky-Aschoff sinuses are invaginations of epithelium into the lamina propria, muscle, and subserosal connective tissue. These sinuses are current in roughly 40% of normal gallbladders and are present in abundance in virtually all infected gallbladders. The ducts of Luschka are tiny bile ducts found across the muscle layer on the hepatic aspect of the gallbladder. During performance of a cholecystectomy, clear visualization of the hepatocystic triangle is essential with correct identification of all buildings within this triangle. It regulates the bile and pancreatic juice circulate in path of the duodenum, preventing the regurgitation of duodenal content into the biliary tree and also diverts bile into the gallbladder leading to its distention. This term is imprecise because the sphincter is subdivided into a quantity of sections and incorporates both round and longitudinal fibers. In greater than 90% of the inhabitants, the frequent channel, the place the biliary and pancreatic ducts be a part of, is lower than 1. The 4 sphincters are the superior and inferior sphincter choledochus, the sphincter pancreaticus, and the sphincter of the ampulla. The common hepatic and the best or left hepatic arteries could come up from vessels aside from the celiac trunk. The supraduodenal bile duct is equipped by arterial branches from the right hepatic, cystic, posterior superior pancreaticoduodenal, and retroduodenal arteries. The axial blood supply of the supraduodenal bile duct has been emphasized by Terblanche et al. Injury to this important axial blood supply may end result within the formation of an ischemic ductal stricture. The proximal or hilar ducts and the retropancreatic bile duct receive a wealthy blood supply. The supraduodenal bile duct supply is axial and tenuous, with 60% from below and 38% from above. Only 2% of the arterial blood provide to the supraduodenal bile duct is segmental (nonaxial). The blood provide to the retroduodenal and intrapancreatic bile duct is from the retroduodenal and pancreaticoduodenal arteries. However, this relation is way from constant; if the artery arises from the proximal proper hepatic artery or from the frequent hepatic artery, it could lie near the hepatic duct, which can be injured when the artery is ligated. Lymphatic vessels from the hepatic surface of the gallbladder may communicate with lymphatic vessels within the liver. Sympathetic fibers originating from the fifth to the ninth thoracic segments pass through the larger splanchnic nerves to the celiac ganglion. Postganglionic sympathetic fibers travel along the hepatic artery to innervate the gallbladder, bile duct, and liver. Visceral afferent nerve fibers from the liver, gallbladder, and bile duct travel with sympathetic afferent fibers by way of the greater splanchnic nerves to enter the dorsal roots of the fifth via ninth thoracic segments. Sensory fibers from the best phrenic nerve additionally innervate the gallbladder, presumably via the communications between the phrenic plexus and the celiac plexus. This innervation may explain the phenomenon of referred shoulder pain in patients with gallbladder disease. The subserous plexus ganglia are bigger and spaced farther apart, unlike the myenteric plexus of the gut. The venous drainage from the hepatic ducts and hepatic floor of the gallbladder is through small vessels that empty into branches of the hepatic veins within the liver. A small venous trunk ascending parallel to the portal vein receives veins draining the gallbladder and bile duct before getting into the liver, separate from the portal vein. Lymph from the decrease bile duct drains into the lower hepatic nodes and the higher pancreatic lymph nodes. A thorough knowledge of this variable anatomy is necessary as a result of failure to acknowledge the frequent anatomic variations may result in important ductal damage. Accessory hepatic ducts often course through Calot triangle and may be injured during dissection in this space. Cholecystohepatic ducts are small biliary ducts that emerge from the liver to enter the hepatic surface of the gallbladder immediately. Cystic Duct In 1976 Benson and Page described five ductal anomalies of scientific significance to the surgeon during performance of a cholecystectomy. A sensible reappraisal of the anatomy of the extrahepatic bile ducts and arteries. These anomalies vary in their medical significance: Some are only medical curiosities and require no try at correction, whereas others require surgical intervention. The gallbladder anomalies may be divided into three groups based on formation, quantity, and place (Box 106. Boyden found that this anomaly was current as confirmed by oral cholecystography in 18% of sufferers with a functioning gallbladder. These diverticula are clinically insignificant unless they become the site of illness, during which case they may include stones, become acutely infected, and even perforate. Hartmann pouch is associated with pathologic situations of the gallbladder, especially those involving extended obstruction to gallbladder emptying. When found in infants and children, a rudimentary gallbladder is believed to be caused by congenital hypoplasia and normally requires no treatment. In an older grownup, this case could additionally be the outcomes of fibrosis from cholecystitis and will require elimination if inflicting biliary signs. Absence of the Gallbladder (Agenesis) More than 200 circumstances of absence of the gallbladder have been reported. Most circumstances are related to different biliary abnormalities, and most of the patients died earlier than 6 months of age. In this sequence, 70 (38%) have been completely absent, 60 (32%) have been rudimentary, and fifty five (30%) were a fibrous structure. There have been circumstances the place two gallbladders had been present in a single patient and just one eliminated leaving the second behind. The gallbladder itself may be seen as two distinct organs at variable distances aside or may outwardly have the looks of a single organ.
Cheap grifulvin v 250mg on-lineThis additionally allows for histologic affirmation of the diagnosis and molecular profiling as a information to further systemic therapy pyrithione zinc antifungal grifulvin v 250 mg mastercard. Nuclei are spherical to oval with minimal pleomorphism and a single distinguished nucleoli antifungal essential oils list buy grifulvin v 250 mg amex. As the stable papillary vascular stalks inside the tumor slough and hemorrhage club fungi definition biology cheap grifulvin v 250 mg amex, central necrosis can happen fungus gnats remedy buy discount grifulvin v 250 mg line, resulting in cystic degeneration. Although these tumors could additionally be extremely large and might invade important vasculature, most lesions are normally amenable to full resection. Pancreaticoduodenectomy or distal pancreatectomy may be performed with en bloc resection of involved adjacent organs when indicated. If metastatic disease occurs, the commonest websites embrace liver, mesentery, and peritoneum. Jaundice has been reported in as much as 70% to 80% of patients and is in all probability going as a outcome of irritation and narrowing or stricture of the distal common bile duct. Immunostaining usually demonstrates ample (>10 cells/ high-power field) IgG4-positive cells. Diagnostic standards rely on a combination of histology, cross-sectional and endoscopic imaging, serologic findings, and an in depth scientific history. The International Consensus Diagnostic Criteria for Autoimmune Pancreatitis recommends a trial of zero. With scientific and radiologic improvement, the prednisone can be tapered by 5 mg/week. Because scientific relapse can occur in as a lot as 30% of sufferers, some investigators have advocated the administration of low-dose upkeep prednisone. Common presenting symptoms include abdominal ache (67% to 73%), B signs such as fever, night sweats, chills, weight reduction (38% to 58%), jaundice (33% to 42%), and gastric or duodenal outlet obstruction (2% to 26%). Cytopathologic features include giant malignant lymphocytic nuclei, prominent nucleoli, abundant karyorrhexis, and a background of necrosis. Note the hypodense look of the mass (arrowheads) and the adjoining abutment of the superior mesenteric vein (long arrow) and proximity to the superior mesenteric artery (short arrow). Complete remission can be anticipated with multidrug therapy in 63% to 77% of sufferers with large B-cell lymphoma. Note the characteristic enhancement of the metastatic lesion (arrow) on arterial phase imaging, in addition to the posterior displacement of the pancreas (arrowheads) due to the absence of the left kidney. The imaging characteristics can be just like pancreatic neuroendocrine neoplasms, and these lesions ought to be included in the differential diagnosis. In contrast, the hypervascularity of the tumor is inconsistent with pancreatic ductal adenocarcinoma. The majority of patients have solitary metastases, which are normally asymptomatic (>50%) and recognized by the way or during follow-up surveillance. Among those that are symptomatic, stomach pain, weight reduction, jaundice, or gastrointestinal hemorrhage may be the presenting criticism. This is best achieved by a coordinated method involving a multidisciplinary staff of physicians, with explicit attention to radiographic and pathologic evaluation. Clinical traits and outcomes from an institutional collection of acinar cell carcinoma of the pancreas and related tumors. Acinar cell carcinoma of the pancreas: an institutional series of resected patients and evaluate of the present literature. Acinar cell carcinoma of the pancreas: scientific and computed tomography manifestations. Cytomorphologic and immunophenotypical options of acinar cell neoplasms of the pancreas. Acinar cell carcinomas of the pancreas: a molecular evaluation in a collection of 57 instances. Neurogenin 3-directed cre deletion of Tsc1 gene causes pancreatic acinar carcinoma. Acinar cell carcinoma of the pancreas in the United States: prognostic factors and comparability to ductal adenocarcinoma. Acinar cell carcinoma of the pancreas: new genetic and remedy insights right into a uncommon malignancy. Aggressive method to acinar cell carcinoma of the pancreas: a single-institution expertise and a literature review. Pancreatic solid-cystic papillary tumor: medical features, imaging findings and operative management. Note the stable sheets of tumor cells which may be separated into acini by vascular septae. Solid pseudopapillary tumor of the pancreas: a single-institution 20-year sequence of pediatric patients. Solid pseudopapillary neoplasm of the pancreas: a single institution expertise of 14 instances. Solid pseudopapillary tumors of the pancreas: evaluate of 718 patients reported in English literature. Institutional expertise with solid pseudopapillary neoplasms: concentrate on computed tomography, magnetic resonance imaging, typical ultrasound, endoscopic ultrasound, and predictors of aggressive histology. Solid-pseudopapillary tumor of the pancreas: a usually cystic carcinoma of low malignant potential. Clinical and pathological options of stable pseudopapillary neoplasms of the pancreas at a single establishment. Alpha-methylacyl-CoA racemase (P504S) is a useful marker for the differential analysis of stable pseudopapillary neoplasm of the pancreas. The prognosis and scientific characteristics of superior (malignant) solid pseudopapillary neoplasm of the pancreas. Recurrence of stable pseudopapillary neoplasms of the pancreas: outcomes of a nationwide research of risk factors and treatment modalities. A mixture of molecular markers and scientific options improve the classification of pancreatic cysts. Solid-pseudopapillary tumors of the pancreas are genetically distinct from pancreatic ductal adenocarcinomas and nearly at all times harbor beta-catenin mutations. Identification of potential biomarkers to differentially diagnose solid pseudopapillary tumors and pancreatic malignancies through a gene regulatory community. Characterization of gene expression and activated signaling pathways in solid-pseudopapillary neoplasm of pancreas. Surgical management of solid-pseudopapillary neoplasms of the pancreas (Franz or Hamoudi tumors): a big single-institutional sequence. Resection of a solid and papillary epithelial neoplasm of the pancreas following remedy with cis-platinum and 5-fluorouracil: a case report. Preoperative gemcitabine for unresectable, solid pseudopapillary tumour of the pancreas.
Purchase grifulvin v 250mg fast deliveryThe splenic artery and vein can be suture ligated or stapled utilizing a vascular load on a linear stapler antifungal pregnancy grifulvin v 250 mg without prescription. Postoperative pancreatic fistula is the most common complication after distal pancreatectomy fungus gnats forum generic 250mg grifulvin v with mastercard. Numerous strategies of pancreatic transection and administration of the pancreatic remnant have been reported antifungal extra thick discount grifulvin v 250 mg otc, including utilizing linear stapling devices across the pancreas antifungal medication for ringworm discount grifulvin v 250 mg with visa, direct duct ligation, fibrin glue utility, and enteric drainage. Prior to dividing the pancreas, four keep sutures may be positioned alongside the inferior and superior border of the pancreatic transection line. The neck of the pancreas is oversewn with overlapping "U" stitches, and the duct is directly ligated when it could be identified. One or two 19-French drains are placed in the left upper quadrant and along the sting of the pancreatic remnant. The drain output is monitored for proof of pancreatic leak, and drain amylase levels are measured as indicated. Postsplenectomy vaccines for Neisseria meningitidis, Streptococcus pneumoniae, and Haemophilus influenzae are given preoperatively or on the day of discharge. Splenic Preservation Mallet-Guy and Vachon first described a spleen-preserving distal pancreatectomy in 1943. Some reports reveal fewer postoperative issues and improved survival with spleen-preserving distal pancreatectomy in contrast with distal pancreatectomy and splenectomy. Splenic preservation is extra appropriate in circumstances of benign disease or tumors with low malignant potential. Splenic preservation could be performed by either preserving the splenic vessels or the Warshaw technique,39 by which the splenic vessels are ligated but the quick gastric are preserved. Outcomes appear comparable with each approaches; nonetheless, splenic infarcts and secondary splenectomies occur more regularly with the Warshaw method. This requires mobilizing the pancreatic tail and cautious dissection of the assorted pancreatic branches from the splenic artery and vein from proximal to distal on the pancreas. Appleby Procedure the Appleby procedure was first described in 1953 and includes en bloc resection of the celiac axis, distal pancreatectomy with splenectomy, and complete gastrectomy. The Appleby procedure has been gradual to achieve reputation; nonetheless, there are an increasing variety of collection in the literature reporting either the Appleby or modified Appleby procedure for locally superior pancreatic adenocarcinoma. A Penrose drain has been positioned across the underside of the pancreatic neck, anterior to the portal vein�superior mesenteric vein confluence to help in elevating the pancreatic neck during transection. In select instances, arterial reconstruction, most often common hepatic artery to aorta, could also be used. One indication for multivisceral resection in pancreatic cancer is an advanced tumor invading the hepatic flexure or transverse colon requiring a hemicolectomy. The good factor about multivisceral resection in pancreatic cancer is to obtain a curative resection with unfavorable margins. Patients requiring multivisceral resection typically current with bigger, more locally advanced tumors needing prolonged resection for contiguous organ involvment. Appropriate affected person choice and performance by an experienced surgeon in specialized pancreatic cancer centers are essential. A more radical resection was thought to potentially improve outcomes by utterly eradicating all of the gland in danger, in addition to reducing morbidity and mortality because of the lack of a pancreaticoenteric anastomosis. Outcomes following whole pancreatectomy had been initially poor with increased postoperative morbidity and no enchancment in long-term disease-free or general survival. More just lately, with improved operative method and better perioperative care, outcomes following whole pancreatectomies have improved and the number of whole pancreatectomies for pancreatic cancer has increased. However, modern-day, long-acting insulin analogues and pancreatic enzyme supplementation have improved the administration of these issues. Typically, the top or tail has been mobilized, and a total pancreatectomy turns into necessary because of a persistently positive margin. The technique for total pancreatectomy in pancreatic most cancers therefore consists of mobilization of the remnant pancreas. In circumstances by which the pancreatic head has been resected, the remnant pancreas should then be excised along with the spleen. The remnant pancreas and spleen are then mobilized in a medial to lateral style. Both techniques have demonstrated acceptable early outcomes and likely equivalent oncologic outcomes compared with open resection, significantly in the hands of skilled pancreatic surgeons. Potential advantages embrace decreased wound complications and postoperative pain, in addition to shortened size of keep. Most of the perceived advantages are derived from retrospective sequence as a result of no randomized managed trials have been carried out. Laparoscopic distal pancreatectomy has gained widespread acceptance in the therapy of benign pancreatic illness. More recently, numerous sequence have reported on the use of laparoscopic distal pancreatectomy for pancreatic ductal adenocarcinoma and noted equivalent oncologic outcomes, fewer issues, and shorter size of keep compared with open distal pancreatectomy. Three more ports are typically used, one in the left decrease quadrant and two additional ports along the upper midline. The dissection begins with taking down the gastrocolic ligament and brief gastric vessels utilizing an digital dissector. The pancreas is mobilized by incising the peritoneum overlying its inferior border, and dissection continues till the splenic vessels are visualized. The pancreatic tail can be suspended by an instrument to permit higher visualization of the splenic vessels. The splenic artery is confirmed by tracing it proximally to the celiac axis if essential. Both the splenic artery and vein are ligated using a linear stapler with a vascular (white) load. The spleen is then mobilized from its retroperitoneal attachments, and the specimen is delivered through an Endo Catch bag. Laparoscopic Pancreaticoduodenectomy the primary laparoscopic pancreaticoduodenectomy was reported by Gagner and Pomp in 1994. As such, laparoscopic pancreaticoduodenectomies are at present performed in facilities all through the world. A tunnel beneath the neck of the pancreas is created, and an umbilical tape is positioned around the pancreas for retraction. The gallbladder is mobilized, and the frequent bile duct is encircled and subsequently divided. A wide Kocher maneuver is performed, and the jejunum is divided with a stapler 10 cm from the ligament of Treitz. Finally, the pancreatic neck is transected utilizing an energy gadget, and the uncinate is then taken off of the superior mesenteric artery in an analogous fashion. The jejunum is introduced into the proper upper quadrant by way of the ligament of Treitz defect. Reconstruction is carried out in a similar way to the open technique, consisting of an end-to-side, duct to mucosa, 1- or 2-layer pancreaticojejunostomy, a single layer end-to-side hepaticojejunostomy, and an end-to-side, antecolic duodenojejunostomy. This ultimate anastomosis is usually stapled, although a sewn 2-layer anastomosis is suitable.
Cheap grifulvin v 250mg fast deliveryIt is troublesome to know the percentage of sufferers with a diaphragmatic hernia and intrathoracic abdomen who will progress to acute gastric strangulation antifungal and antibacterial cream buy grifulvin v 250 mg overnight delivery. However anti fungal toe medication discount grifulvin v 250 mg with visa, the high morbidity and mortality associated with strangulation justify expeditious restore antifungal over the counter pill buy grifulvin v 250mg without a prescription, even in asymptomatic sufferers fungus nail turning black buy discount grifulvin v 250 mg on line. After the stomach has been reduced, gastropexy can be achieved by placement of a percutaneous endoscopic gastrostomy tube. Laparoscopic and combined laparoscopic and endoscopic approaches have the potential to combine minimally invasive techniques with repair of the diaphragmatic defect. Small bowel volvulus within the adult populace of the United States: results from a population-based examine. Wandering spleen with gastric volvulus and intestinal non-rotation in an adult male affected person. Rare persistent gastric volvulus related to left atrial and mediastinal compression. Gastric wall necrosis from organo-axial volvulus as a late complication of laparoscopic gastric banding. Gastric volvulus as a complication within the recipients after adult dwelling donor liver transplantation. Chronic and recurrent volvulus of the abdomen with late results of "colonic displacement". Acute and persistent gastric volvulus in infants and kids: who should be treated surgically Laparoscopic gastropexy relieves signs of obstructed gastric volvulus in excessive operative threat patients. Acute gastric volvulus handled with laparoscopic discount and percutaneous endoscopic gastrostomy. The analysis is made with a history of nausea, vomiting, abdominal pain, signs of stomach distention and tenderness, and imaging displaying dilated bowel with air-fluid ranges. Adhesive disease is the etiology of roughly 50% to 75% of small bowel obstructions, with Crohn obstruction, neoplasm, and stomach wall hernia finishing the differential analysis in most cases. Internal hernias, defined as a protrusion of viscus via an intraabdominal aperture without traversing fascial planes, cause zero. This article will focus on acquired and congenital forms of internal hernias, their prognosis, and administration. These embody the mesenteric defect created in a bowel anastomosis, hepaticojejunostomy throughout liver transplantation or Whipple procedures, and even ostomy formation. The commonest site for inner hernia after liver transplantation is through the transverse mesocolon. The drawback of the laparoscopic approach is the elevated incidence of gastrojejunal anastomotic stricture and inner hernia. The increased incidence of inner hernia after laparoscopic bypass is due to the dearth of adhesion formation and the ensuing mobility of the bowel. A comparable increased incidence of inner hernia is seen in immunosuppressed sufferers, and is also thought to be due to decreased adhesion formation. The most typical secondary operations are cholecystectomy, lysis of adhesions, liver biopsies, and umbilical hernia repairs. Early operation, outlined as within ninety days of the preliminary operation, accounts for 18% of all reoperations. Late reoperation, occurring after ninety days, is most commonly done for exploration secondary to ache, nausea, or vomiting of unclear etiology, but can be due to adhesive obstruction or inside hernia. Incidence of acquired inner hernias is rising secondary to elevated use of laparoscopic Roux-en-Y gastric bypass for weight loss and management of obesity-related morbidities. Knowledge of congenital forms of internal hernia is essential in recognizing acutely life-threatening obstructions or diagnosing the etiology of persistent belly ache. Regardless of etiology, consolation in administration of each acquired and congenital internal hernias is prime for the general surgeon. The lack of overt visual cues makes the analysis tough, so suspicion have to be high. Roux limb obstruction most commonly ends in ill-defined epigastric and left higher quadrant ache quickly relieved with emesis. Signs of high-grade obstruction might be present in 50% of sufferers, and 40% of sufferers may have stomach ache. Finally, herniation of the biliopancreatic limb, a uncommon occasion, could end in pain, remnant gastric distention, tachycardia, and hiccoughs. Laboratory examinations are typically nondiagnostic, but sufferers with internal hernia could current with amylasemia and leukocytosis. B, Space between the Roux limb mesentery and the transverse mesocolon (Petersen hernia). The biliary limb consists of the size of the duodenum and approximately 30 cm of jejunum measured from the ligament of Treitz. Retrocolic passage of the Roux limb on the index operation creates a 3rd potential aperture in the transverse mesocolon, the place bowel may herniate alongside the Roux limb. Closure or nonclosure of all of those defects on the index operation has been described. There is proof of decreased incidence of inside hernia with closure of each defect at preliminary operation. The retrocolic method was initially favored because of concern of excess stretch on the gastrojejunal anastomosis with an antecolic strategy. Most research report an increased incidence of inner hernia within the retrocolic strategy compared to the antecolic approach of 2. The variability in these research is likely because of the variability in time to follow-up. The elevated incidence of internal hernia with the retrocolic strategy appears to be as a result of herniation through the transverse mesocolic defect. Routine closure of this defect significantly reduces the incidence of herniation to zero. Data are conflicting, however there appears to be a pattern towards decreased incidence of inside hernia with routine closure of the Petersen house as nicely. Because inner hernias typically spontaneously reduce, you will want to image the symptomatic patient with indicators of inside hernia. Oral contrast might assist elucidate the etiology of obstruction; however, inside hernias in this setting are sometimes proximal obstructions with no pylorus to sluggish filling of the small bowel. Simply having the patient swallow a tolerable quantity of distinction on the desk immediately before scanning is adequate. Medical centers with skilled radiologists with a suspicion for inside hernia will be unable to diagnose inner hernia on imaging in 16% to 20% of circumstances. A swirl signal happens when tension on the small bowel mesentery causes the mesenteric vessels to twist around in a whorl-like fashion and occurs in 55% of sufferers with inner hernia. Any abrupt adjustments within the path of mesenteric vessels or vascular engorgement are additionally regarding findings. Specifically, clustering of bowel loops in aberrant places is indicative of obstruction. Small bowel dilation is found in 25% of sufferers, and mesenteric edema and free fluid are found in 11%.
References - Simbre VC, Duffy SA, Dadlani GH, Miller TL, Lipshultz SE. Cardiotoxicity of cancer chemotherapy: implications for children. Paediatr Drugs 2005;7:187- 202.
- Weinblatt ME, Kavanaugh A, Genovese MC, et al. An oral spleen tyrosine kinase (Syk) inhibitor for rheumatoid arthritis. N Engl J Med 2010;363(14):1303-1312.
- Zoghbi WA, Enriquez-Sarano M, Foster E, et al: Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography, J Am Soc Echocardiogr 16:777-802, 2003.
- Centers for Disease Control and Infection (CDC): Provisional CDC guidelines for the use and safety monitoring of bedaquiline fumarate (Sirturo) for the treatment of multidrug-resistant tuberculosis, MMWR Recomm Rep 62(RRn09):1n12, 2013.
- Wheller JJ, Reiss R, Allen HD: Clinical experience with fetal echocardiography. Arch Pediatr Adolesc Med 1990; 144:49-53.
- Tsakiris AG, Von Bernuth G, Rastelli GC, et al: Size and motion of the mitral valve annulus in anesthetized intact dogs, J Appl Physiol 30:611-618, 1971.
- Kormann MS, Depner M, Hartl D, et al. Toll-like receptor heterodimer variants protect from childhood asthma. J Allergy Clin Immunol 2008; 122: 86-92.
- Gottlieb AG, Galan HL. Shoulder dystocia: an update. Obstet Gynecol Clin N Am 2007;34:501-31.
|