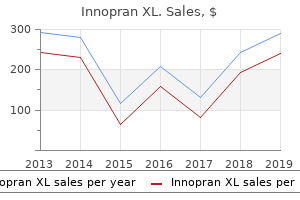
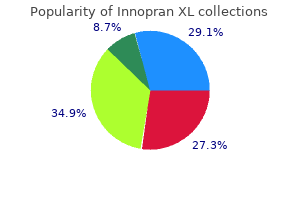
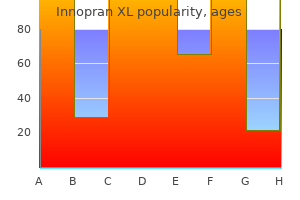
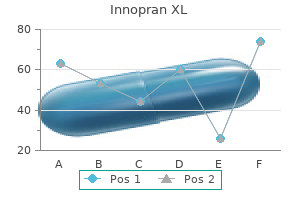
Innopran XL
Eloise J. Prijoles, M.D. - Greenwood Genetic Center
- Columbia, South Carolina
Discount 80mg innopran xl mastercardTogo S blood pressure medication morning or evening discount innopran xl 40 mg fast delivery, et al: Perioperative infection control and its effectiveness in hepatectomy sufferers arteria thoracica inferior innopran xl 80 mg mastercard, J Gastroenterol Hepatol 22(11):1942�1948 blood pressure factors discount 40mg innopran xl, 2007 blood pressure 7744 buy 80 mg innopran xl with amex. Togo S, et al: Usefulness of absorbable sutures in preventing surgical site infection in hepatectomy, J Gastrointest Surg 12(6):1041�1046, 2008. Uchiyama K, et al: Risk components for postoperative infectious issues after hepatectomy, J Hepatobiliary Pancreat Sci 18(1):67�73, 2011. Van Buren G 2nd, et al: A randomized prospective multicenter trial of pancreaticoduodenectomy with and without routine intraperitoneal drainage, Ann Surg 259(4):605�612, 2014. Wang A, et al: Analysis of surgical web site an infection fee in pancreas operation and its associated danger components, Zhongguo Yi Xue Ke Xue Yuan Xue Bao 29(4):562�565, 2007. Watanabe F, et al: Risk elements for intra-abdominal infection after pancreaticoduodenectomy-a retrospective analysis to consider the importance of preoperative biliary drainage and postoperative pancreatic fistula, Hepatogastroenterology 59(116):1270�1273, 2012. Yanaga K, et al: Intraperitoneal septic problems after hepatectomy, Ann Surg 203(2):148�152, 1986. Yang T, et al: Risk components of surgical website infection after hepatic resection, Infect Control Hosp Epidemiol 35(3):317�320, 2014. With the ease and availability of subtle high-resolution scanning, there may develop a tendency for the physician to "scan first, clinic later," and this have to be averted. A thorough scientific assessment will information the appropriateness and use of additional tests and should include a cautious balancing of potential danger versus advantage of any investigation or intervention in any particular individual, relying on their health, comorbidity, and private or family needs. Accurate recording of alcohol intake must be made, as a end result of ongoing heavy alcohol use impacts therapy for persistent liver or pancreatic diseases. Occasionally, patients attend the clinic smelling of alcohol of their breath, yet deny ongoing alcohol use, and this must be noted. A request for a blood alcohol degree might be made, supplied the affected person consents to it. A past medical historical past must be obtained to embrace any major diseases and any stomach surgical procedure. A document of comorbidities and train tolerance must be made, as this will guide the surgeon in assessing fitness for future intervention if required (see later). This must be followed by a household historical past, drug historical past, social circumstances, employment, and journey. Abdominal pain is usually a presenting symptom, and a detailed enquiry of the location, severity, radiation, and rapidity of onset will permit some clues to a differential diagnosis. Suddenonset severe higher abdominal ache radiating to the back is characteristic of acute pancreatitis (see Chapters fifty five and 56), whereas right-side upper quadrant pain may point out acute inflammation of the gallbladder (see Chapter 33). Any associated nausea and vomiting ought to be recorded along with a historical past of jaundice (sclerae), color of urine and stools, and any associated itching. A historical past of belly distension may point to an ileus in acute presentations and to ascites or bowel obstruction in persistent liver illness or a malignant course of. Steatorrhea is characterised by the passage of foul-smelling stools, which float on water and will point out pancreatic exocrine insufficiency (see Chapters fifty seven, 58, and 62). Full exposure of the abdomen in good mild is essential for an enough inspection. Particular attention ought to be paid to any scars from earlier abdominal surgery, stomach distension, and areas of discoloration. Palpation of the stomach should begin with a common mild palpation, in search of obvious masses or areas of tenderness. The healthy liver is normally impalpable; nonetheless, in very skinny people, the anterior edge may be palpable. A lobe might bear hypertrophy and turn into palpable, and this may occur in the presence of hemiliver atrophy or after liver resection. Reduction in liver size also is essential as a result of this will likely occur in cirrhosis and sure kinds of hepatitis. Rotation of the patient 45 levels to the right might help palpation, as a outcome of the spleen then falls onto the inspecting proper hand. During this maneuver, the left hand should assist the rib cage and relax the skin and abdominal musculature by drawing these all the way down to the best. Percussion could also be useful, and if ascites is present, the spleen may be ballotable. If the spleen is sufficiently enlarged, the notch on its anterior border may turn into palpable. The liver is examined using a mixture of palpation and percussion from above and beneath to delineate its borders. Dullness to percussion of the upper border extends so far as the fifth intercostal house. Auscultation can additionally be essential because a venous hum could also be heard with portal hypertension, and a bruit could also be heard in association with hepatocellular carcinomas. Portal Hypertension Portal hypertension is due to both intrahepatic or extrahepatic portal venous obstruction (see Chapters seventy six and 79). The extra common clinical site of portosystemic anastomosis is at the gastroesophageal junction, leading to esophageal varices; any evidence of upper gastrointestinal blood loss, whether or not hematemesis or melena, ought to be investigated with urgent endoscopy. Extrahepatic portal hypertension is normally as a end result of portal vein thrombosis, and as such you will need to establish any historical past of neonatal infection across the umbilicus, main intraabdominal sepsis or pancreatitis, pancreatic cancer, or a blood dysfunction that may lead to hypercoagulability. These sufferers almost invariably have splenomegaly, typically associated with pancytopenia. A palpable spleen within the upper left stomach associated with portal hypertension could also be discovered in the event of splenic occlusion attributable to tumor or chronic pancreatitis. Acute alcoholic hepatitis normally happens after a bout of ingesting and may be associated with liver tenderness, jaundice, pyrexia, and leukocytosis. These sufferers typically are seen recurrently with epigastric ache, which can be severe. They will usually admit to a bout of heavy ingesting, which precipitates their symptoms. Advanced alcoholic liver illness could also be related to different manifestations of hepatic impairment. Decompensated liver failure ends in the event of encephalopathy, jaundice, ascites, fatigue, polydipsia, easy bruising, temper fluctuation and infrequently is marked by nutritional depletion. Primary biliary cirrhosis, or continual nonsuppurative harmful cholangitis, often affects middle-aged women. The earliest symptom is often unrelenting pruritus, even earlier than medical jaundice is clear, but later the patient may expertise overt jaundice; hepatosplenomegaly; xanthelasma, particularly within the palms and around the eyes; vitiligo; and arthritis. Primary biliary cirrhosis is commonly present in affiliation with connective tissue disease (see Chapter 112). Primary Sclerosing Cholangitis Ulcerative colitis and Crohn illness are related to hepatobiliary disorders, especially main sclerosing cholangitis (see Chapter 41). It is necessary to embrace a detailed gastrointestinal methods review and investigations in any affected person with unexplained liver dysfunction.
Discount 80 mg innopran xl free shippingBacterial superinfection of Fasciola cysts is a complication of the chronic phase hypertension nursing teaching proven 40mg innopran xl. Recent research in a rat model have shown a considerably increased risk of bacterobilia in the persistent an infection (Valero et al blood pressure vision safe innopran xl 40 mg, 2006) and with concomitant gallstones (Valero et al arteriosclerotic heart disease purchase 40mg innopran xl, 2003) pulse pressure 15 cheap innopran xl 80 mg with visa. Even after successful therapy, abdominal ache and weight reduction should be present in approximately 2% to 4% of patients for several months (Rondelaud et al, 2006), which emphasizes the danger for morbidity even after eradication of the an infection. On admission to a tertiary health center, 47% of 277 sufferers with difficult disease had eosinophilia (Blancas et al, 2004). A related percentage was present in one hundred and one persistent cases from the Andean area and other endemic areas: 48% had eosinophilia above regular levels, and only 14% had more than a thousand eosinophils/mL (Alban et al, 2002). In one other examine, approximately half of a bunch of 61 youngsters in the Peruvian Altiplano with continual fascioliasis had eosinophilia (Marcos et al, 2002). In Turkey, only 11% of 18 patients with fascioliasis had eosinophilia (Turhan et al, 2006). Likewise, mild eosinophilia could additionally be present in a minority of fascioliasis sufferers (GilGil et al, 2006). Few sufferers in the chronic part have high-grade eosinophilia, in distinction with the acute section, which presents with hypereosinophilia in virtually all sufferers. A broad number of other infectious agents are associated with eosinophilia, corresponding to Strongyloides stercoralis, Ascaris lumbricoides, and hookworms or different helminths. Severe iron deficiency anemia has been regularly reported in patients with chronic fascioliasis (Cabada et al, 2014; Gabrielli et al, 2014; Tavil et al, 2014). A granulomatous persistent irritation may also be triggered by parasite ova within the liver or different locations (Marcos & Terashima, 2007; Naresh et al, 2006). In an animal mannequin, persistent immune suppression has been demonstrated in advanced chronic an infection (Giron�s et al, 2007), suggesting that the contaminated host may be vulnerable in the course of the persistent section to any Th2-suppression�dependent an infection. This chronic immunosuppression could predispose to bacterial infection that could be life threatening. It seems that hepatic fibrosis may evolve in some susceptible hosts, depending on the time and burden of infection. For instance, virtually 50% of cattle infected chronically by fascioliasis had cirrhosis (Marcos et al, 2007c). Data help that cathepsin L1 and its collagenolytic operate are related to tissue invasion within the pathogenesis of hepatic involvement related to F. However, few research have tried to determine components related to liver fibrosis, which is a vital clinical outcome of the an infection (Marcos et al, 2007c; Perez et al, 1999; Phiri et al, 2006; Shirai et al, 2006). In addition, liver cirrhosis has been reported in each youngsters and adults with fascioliasis (AlmendrasJaramillo et al, 1997; Heredia et al, 1984; Marcos et al, 2005a; Sanchez-Sosa et al, 2000). In an endemic country, preliminary research have shown that approximately 9% of cirrhotic sufferers have antibodies against Fasciola (Marcos et al, 2009b). In vitro and in vivo research have proven a significant correlation between fibrogenic gene expression and both intensity and length of infection, demonstrating that longer and higher burden of infection stimulates fibrogenesis within the infected liver (Marcos et al, 2011). Other findings are hepatomegaly, tractlike hypodense lesions with subcapsular location, subcapsular hematoma, and cystic calcifications (Loja et al, 2003; Marcos et al, 2008). Early an infection is associated with contrast enhancement of the Glisson capsule as a result of inflammation stimulated as the juvenile parasite penetrates the liver capsule. In the intermediate stage (after the first month), multiple hypodense nodular areas (abscesslike lesions) or low-density serpiginous, tortuous, tunnel-like branching lesions that vary from 2 to 10 mm are created by parasite migration via the liver and are usually visualized within the subcapsular region (Gonzalo-Orden et al, 2003; MacLean & Graeme-Cook, 2002). Although the characteristics of those cyst calcifications seem to be distinctive to fascioliasis, this discovering adds a new agent to the record of infectious ailments associated with tissue calcifications, corresponding to echinococcosis, paragonimiasis, histoplasmosis, and toxoplasmosis. Abdominal Ultrasound Findings within the acute phase of fascioliasis include focal areas of elevated echogenicity, a number of nodular or irregular lesions of variable echogenicity, or a single, complicated mass in the liver that resembles malignancy mimicking malignancy (Cosme et al, 2001, 2003). A T1-weighted three-dimensional gradient-echo picture displayed homogeneous contrast enhancement (Orlent et al, 2007). Diagnosis the analysis of the acute part of fascioliasis is confirmed mainly by serology, based on epidemiology, medical picture, and imaging results. In poor endemic areas, the analysis can be a challenge and sometimes a trial of antiparasitic drug could additionally be needed. Clinical enchancment and discount on the eosinophil counts after three to 5 days of triclabendazole can be utilized as a diagnostic criterion (Marcos et al, 2008). A sedimentation technique ought to be performed on serial stool specimens (at least three) from completely different days to increase the chance of detecting the eggs within the stools. The intermittent deposition of parasite ova in the biliary duct can decrease the sensitivity of the sedimentation approach, so frequent stool examinations may be considered. One technique is the speedy sedimentation technique described by Lumbreras and colleagues (Lumbreras et al, 1962) in Peru. This take a look at is inexpensive, straightforward to carry out, and sensitive, with a higher sensitivity than the ether-formalin focus method (Marcos et al, 2007a). Another method, the Kato-Katz methodology, can be utilized to measure the intensity of an infection (Katz et al, 1972). Diagnosis of Fascioliasis by Surgery In the instances reported within the literature, most sufferers who underwent a surgical or invasive process had chronic Fasciola an infection, and their initial clinical problem was biliary obstruction and choledocholithiasis (Kim et al, 2006; Mera y Sierra et al, 2011). However, the detection rate of the adult parasite during surgery of the biliary tract is low total. A delicate eosinophilia within the clinical setting of biliary obstruction in a traveler or immigrant from endemic areas ought to suggest fascioliasis. A single dose of triclabendazole ought to be given after the process to ensure elimination of any parasites missed by endoscopy or remaining in other locations. The adult parasite can be discovered by the way throughout an elective laparoscopic cholecystectomy (Bulbuloglu et al, 2007). Recognizing the medical state of affairs early could enable well timed and noninvasive identification of this infection. Chronic Phase the gold standard for the diagnosis of continual an infection is visualization of the eggs within the stool or bile or duodenal aspirates or recovery of the adult parasites during surgical procedure. Serology adverse and stool samples unfavorable - Stage: Early acute fascioliasis - Repeat serology in 1�2 weeks and proceed repeating stool exams - If persists negative: prognosis unlikely Case 3. Serology positive and stool samples optimistic - Chronic fascioliasis - Treatment Stages of the infection by diagnostic outcomes Case 2. Serology positive and stool samples negative - Acute fascioliasis - Treatment Case four. Serology unfavorable and stool samples constructive - Late persistent fascioliasis - Pseudofascioliasis is possible if patient consumed a poorly cooked or raw animal liver containing fasciola eggs. Biliary obstruction by Fasciola associated with cholangitis requires both surgical intervention and antiparasitic brokers. Patients could have surgical intervention to remove the pseudocyst of Echinococcus, when parasites of F hepatica had been inflicting an intrahepatic. In different conditions, grownup parasites have been discovered when trying to take away a potential malignancy or metastasis-like lesion from the colonic wall (Makay et al, 2007), neck (Marcos et al, 2009a), epidural house (Vatsal et al, 2006), eye (Dalimi & Jabarvand, 2005), and breast (Naresh et al, 2006).
Order innopran xl 40 mg with amexBile salts are amphipathic compounds that comprise both a hydrophilic and hydrophobic portion arrhythmia uk buy discount innopran xl 40 mg online. In aqueous options blood pressure 70 over 50 order 80 mg innopran xl with mastercard, bile salts are oriented with the hydrophilic portion outward prehypertension symptoms purchase innopran xl 40mg on-line. Phospholipids are integrated into the micellar construction blood pressure facts order 40mg innopran xl visa, allowing cholesterol to be added to the hydrophobic central portion of the micelle. Concentration of bile leads to net switch of phospholipids and cholesterol from vesicles to micelles. Phospholipids are transferred extra efficiently than cholesterol, leading to ldl cholesterol enrichment of the remaining (remodeled) vesicles. Aggregation of those cholesterolrich vesicles types multilamellar liquid crystals of ldl cholesterol monohydrate. Structurally, these vesicles are made up of lipid bilayers of ldl cholesterol and phospholipids. In their easiest and smallest type, the vesicles are unilamellar, but an aggregation might take place, leading to multilamellar vesicles. Bilirubin Secretion Heme is released at the time of degradation of senescent erythrocytes by the reticuloendothelial system. The remaining 15% to 20% is derived largely from the breakdown of hepatic hemoproteins. Both enzymatic and nonenzymatic pathways for the formation of bilirubin have been proposed. In this "unconjugated" form, bilirubin has a really low solubility and is sure avidly to plasma proteins, primarily albumin, before uptake and further processing by the liver. The liver is the only organ capable of removing the albumin-bilirubin complex from the circulation and esterifying the doubtless poisonous bilirubin to water-soluble, nontoxic, monoconjugated and deconjugated derivatives. In the hepatocyte, bilirubin binds to a driver of gluthathione-S-transferase and is catalyzed by bilirubin uridine-5-diphosphate glycosyltransferase to form bilirubin glucuronides. Most of the bile salts are reabsorbed within the terminal ileum and are returned to the liver to be extracted and reextracted. The complete amount of bile acids in the enterohepatic circulation is outlined because the circulating bile pool. Thus, of the total bile salt pool of 2 to four g, which recycles via the enterohepatic cycle 6 to 10 instances daily, only about 600 mg is definitely excreted into the colon. Bacterial action within the colon on the 2 main bile salts, cholate and chenodeoxycholate, ends in the formation of the secondary bile salts, deoxycholate and lithocholate. In reality, the bile acid signature of a person is very depending on intestine microbial modification (Swann et al, 2011). Bacterial enzymes modify major bile acids via deconjugation, dehydrogenation, dehydroxylation, and sulfation reactions. However, the physiology of bile salts, biliary lipids, bilirubin, bile circulate, and the enterohepatic circulation is dramatically altered when the bile ducts turn into obstructed. Bile Flow the bile ducts, gallbladder, and sphincter of Oddi act in concert to modify, store, and regulate the flow of bile. During its passage by way of the bile ductules, canalicular bile is modified by the absorption and secretion of electrolytes and water. Bicarbonate secretion by the bile ducts performs an necessary role in bile salt�independent bile move. The gastrointestinal hormone secretin increases bile move primarily by increasing the active secretion of chloride-rich fluid by the bile ducts. Bile duct secretion also is stimulated by different hormones, similar to cholecystokinin and gastrin. The major capabilities of the gallbladder are to concentrate and retailer hepatic bile during the fasting state and deliver bile into the duodenum in response to a meal. The enterohepatic circulation supplies an important adverse feedback system on bile salt synthesis. Should the recirculation be interrupted by resection of the terminal ileum or by major ileal disease, abnormally large losses of bile salts occur. This state of affairs increases bile salt production to maintain a normal bile salt pool. Similarly, if bile salts are misplaced through an exterior biliary fistula, increased bile salt synthesis is important. However, except for these unusual circumstances in which extreme losses occur, bile salt synthesis matches losses, sustaining a continuing bile salt pool dimension. During fasting, roughly 90% of the bile acid pool is sequestered within the gallbladder. Over the past forty years, vital advances have been made in our understanding of the pathophysiology, diagnosis, and management of the jaundiced affected person. Similarly, advances have been made in perioperative and operative administration which have resulted in improved survival of the jaundiced affected person. This part will review the causes, pathophysiology, and management of biliary obstruction. Overproduction, impaired uptake, and decreased conjugation of bilirubin all result in a predominantly unconjugated hyperbilirubinemia. For instance, secondary hepatocellular dysfunction might develop in a patient with biliary obstruction from a tumor. Therefore these classification methods may be simplifications of more complex disease processes. Diseases that cause bile duct obstruction may be further divided into conditions that trigger (1) full obstruction, (2) intermittent obstruction, (3) chronic incomplete obstruction, or (4) segmental duct obstruction (Box eight. Patients with complete biliary obstruction will have clinical jaundice, and those with intermittent obstruction could expertise signs (pain, pruritus, fevers) and biochemical changes with out necessarily experiencing scientific jaundice. Hepatic fibrosis can eventually develop in patients with continual incomplete obstruction (see Chapter 7) and biliary cirrhosis (see Chapter 76). Pathophysiology Biliary obstruction produces local results on the bile ducts, which lead to derangements of hepatic function and, ultimately, to widespread systemic effects. Jaundiced sufferers are at increased risk for hepatic dysfunction, renal failure, cardiovascular impairments, dietary deficiencies, bleeding issues, infections, and wound problems, and their perioperative mortality and morbidity are increased. Hepatobiliary Hepatocytes are arranged in plates along which blood flows from portal to central veins. Within these plates, the small apical domains of adjacent hepatocytes form a tubular lumen, the canaliculus, which is the site of primary bile formation. From the canalicular network, bile flows to the small ductules and subsequently to the bigger ducts. With biliary obstruction, the bile canaliculi turn into dilated, and the microvilli are distorted and swollen. In patients with long-standing obstruction, intrahepatic bile ductule proliferation happens with a rise in the length and tortuosity of the canaliculi. The biliary system usually has a low strain (5 to 10 cm H2O); nonetheless, in the setting of full or partial biliary obstruction, biliary pressure can strategy 30 cm H2O. While biliary strain will increase, the tight junctions between hepatocytes and bile duct cells are disrupted, leading to a rise in bile duct and canalicular permeability.
Cheap 80 mg innopran xl with amexTaken within the context of other modern literature on this subject arrhythmia in fetus purchase innopran xl 40mg online, one of the best method to peritoneal drainage stays unclear and should be individualized to the particular patient hypertension 140 90 purchase innopran xl 40mg visa. If placed on the time of pancreaticoduodenectomy heart attack or pulled muscle generic 80 mg innopran xl amex, the timing of drain elimination is also controversial pre hypertension nursing diagnosis discount 40mg innopran xl. Recent potential studies, together with a randomized trial, have advised that early drain elimination based on drain amylase levels can decrease the speed of postoperative problems, together with infectious ones (Bassi et al, 2010; Kawai et al, 2006). To summarize, danger mitigation at the operative stage for a pancreaticoduodenectomy or distal pancreatectomy consists of the efficient efficiency of the operation using careful operative approach in an effort to keep away from pointless blood loss. The pancreaticoenteric anastomosis throughout pancreaticoduodenectomy continues to be performed according to surgeon preference however must be carried out meticulously. With regard to distal pancreatectomy, stapled closure of the pancreas with bioabsorbable mesh buttress seems promising within the prevention of pancreatic fistula. Perioperative administration of pasireotide has demonstrated efficacy in reducing pancreatic fistula after pancreaticoduodenectomy and distal pancreatectomy. The use of intraperitoneal drains and the timing of their elimination remain controversial. Postoperative Risk Mitigation Postoperative blood glucose control is important after surgical procedures and has an impression on affected person outcomes, as discussed earlier. Synbiotic remedy has proven some promising results in mitigating infectious complications in hepatic resection sufferers (see section "Hepatic Resection"). Rayes and colleagues (2007) conducted a randomized, double-blind trial to evaluate the potential advantage of synbiotic therapy in patients undergoing pancreaticoduodenectomy with preservation of the pylorus. All sufferers were started on enteral nutrition immediately postoperatively by way of a nasojejunal tube placed at the time of the operation. The experimental group received enteral vitamin plus synbiotics, whereas the control group obtained enteral vitamin plus placebo. Ambiru S, et al: Poor postoperative blood glucose management will increase surgical website infections after surgery for hepato-biliary-pancreatic cancer: a potential examine in a high-volume institute in Japan, J Hosp Infect 68(3):230�233, 2008. The Veterans Affairs Total Parenteral Nutrition Cooperative Study Group, N Engl J Med 325(8):525�532, 1991. American Society of Health-System Pharmacists, Am J Health Syst Pharm 56(18):1839�1888, 1999. Arikawa T, et al: Risk factors for surgical site infection after hepatectomy for hepatocellular carcinoma, Hepatogastroenterology 58(105): 143�146, 2011. Bassi C, et al: Early versus late drain removing after standard pancreatic resections: outcomes of a prospective randomized trial, Ann Surg 252(2):207�214, 2010. Bilzer M, et al: Role of Kupffer cells in host protection and liver disease, Liver Int 26(10):1175�1186, 2006. Correa-Gallego C, et al: Operative drainage following pancreatic resection: analysis of 1122 sufferers resected over 5 years at a single establishment, Ann Surg 258(6):1051�1058, 2013. Cortes A, et al: Effect of bile contamination on instant outcomes after pancreaticoduodenectomy for tumor, J Am Coll Surg 202(1): 93�99, 2006. Emmrich J, et al: Secretory immunoglobulin A in pancreatic juice and pancreatic tissue of sufferers with continual pancreatitis, Gut 42(3): 436�441, 1998. Farges O, et al: Multicentre European examine of preoperative biliary drainage for hilar cholangiocarcinoma, Br J Surg 100(2):274�283, 2013. Ferrero A, et al: Preoperative biliary drainage will increase infectious complications after hepatectomy for proximal bile duct tumor obstruction, World J Surg 33(2):318�325, 2009. Finkelstein R, et al: Vancomycin versus cefazolin prophylaxis for cardiac surgical procedure in the setting of a high prevalence of methicillin-resistant staphylococcal infections, J Thorac Cardiovasc Surg 123(2):326�332, 2002. Fisette A, et al: High-dose insulin remedy reduces postoperative liver dysfunction and problems in liver resection sufferers via decreased apoptosis and altered irritation, J Clin Endocrinol Metab 97(1):217�226, 2012. Fong Y, et al: Drainage is unnecessary after elective liver resection, Am J Surg 171(1):158�162, 1996. Gerke H, et al: Complications of pancreaticoduodenectomy after neoadjuvant chemoradiation in patients with and with out preoperative biliary drainage, Dig Liver Dis 36(6):412�418, 2004. Harimoto N, et al: Prospective randomized controlled trial investigating the sort of sutures used during hepatectomy, World J Gastroenterol 17(18):2338�2342, 2011. Hirokawa F, et al: Evaluation of postoperative antibiotic prophylaxis after liver resection: a randomized controlled trial, Am J Surg 206(1): 8�15, 2013. Itoshima T, et al: Scanning electron microscopy of the bile ductule, Gastroenterol Jpn 12(6):476�482, 1977. Jagannath P, et al: Effect of preoperative biliary stenting on immediate end result after pancreaticoduodenectomy, Br J Surg 92(3):356�361, 2005. Kanazawa H, et al: Synbiotics reduce postoperative infectious complications: a randomized managed trial in biliary most cancers sufferers undergoing hepatectomy, Langenbecks Arch Surg 390(2):104�113, 2005. Kawai M, et al: Early removing of prophylactic drains reduces the danger of intra-abdominal infections in patients with pancreatic head resection: prospective examine for 104 consecutive patients, Ann Surg 244(1):1�7, 2006. Kitahata Y, et al: Preoperative cholangitis throughout biliary drainage will increase the incidence of postoperative extreme issues after pancreaticoduodenectomy, Am J Surg 208(1):1�10, 2014. Kobayashi S, et al: Risk factors of surgical site infection after hepatectomy for liver cancers, World J Surg 33(2):312�317, 2009. Konvalinka A, et al: Impact of treating Staphylococcus aureus nasal carriers on wound infections in cardiac surgery, J Hosp Infect 64(2): 162�168, 2006. Kurmann A, et al: Hepatic steatosis is related to surgical-site an infection after hepatic and colorectal surgery, Surgery 156(1):109� 116, 2014. Kurz A, et al: Perioperative normothermia to scale back the incidence of surgical-wound infection and shorten hospitalization. Study of Wound Infection and Temperature Group, N Engl J Med 334(19): 1209�1215, 1996. Lavu H, et al: Perioperative surgical care bundle reduces pancreaticoduodenectomy wound infections, J Surg Res 174(2):215�221, 2012. Lermite E, et al: Effect of preoperative endoscopic biliary drainage on infectious morbidity after pancreatoduodenectomy: a case-control research, Am J Surg 195(4):442�446, 2008. Surgical experience and evaluation of risk elements in 103 patients, Ann Surg 199(4):432�437, 1984. Limongelli P, et al: Correlation between preoperative biliary drainage, bile duct contamination, and postoperative outcomes for pancreatic surgery, Surgery 142(3):313�318, 2007. Liu F, et al: Preoperative biliary drainage before resection for hilar cholangiocarcinoma: whether or not or not Hospital Infection Control Practices Advisory Committee, Infect Control Hosp Epidemiol 20(4):250�278, quiz 279�280, 1999. A single establishment evaluation of 709 consecutive pancreaticoduodenectomies, J Am Coll Surg 216(4):635�642, discussion 642�634, 2013. Nakahira S, et al: Proposal for a sub-classification of hepato-biliarypancreatic operations for surgical web site infection surveillance following assessment of outcomes of prospective multicenter information, J Hepatobiliary Pancreat Sci 20(5):504�511, 2013. Nakayama H, et al: Subcutaneous drainage to forestall wound an infection in liver resection: a randomized managed trial, J Hepatobiliary Pancreat Sci 21(7):509�517, 2014. Nanashima A, et al: Associated components with surgical web site infections after hepatectomy: predictions and countermeasures by a retrospective cohort examine, Int J Surg 12(4):310�314, 2014. Okabayashi T, et al: Effect of intensive insulin remedy utilizing a closedloop glycemic management system in hepatic resection sufferers: a potential randomized scientific trial, Diabetes Care 32(8):1425�1427, 2009a. Okabayashi T, et al: Risk elements and predictors for surgical web site an infection after hepatic resection, J Hosp Infect 73(1):47�53, 2009b.
Buy innopran xl 40 mgIn addition to washout blood pressure medication post stroke innopran xl 80mg without prescription, peritumoral capsules arrhythmia uk generic innopran xl 40mg free shipping, that are low in signal intensity on the arterial dominant section and enhance later prehypertension for years 80mg innopran xl with visa, are also related to microvascular invasion blood pressure medication propranolol 40mg innopran xl free shipping, an necessary characteristic with clinical significance (Witjes et al, 2012). Although dysplastic nodules may also hyperenhance, they have a tendency to be extra homogeneous and isointense to background liver parenchyma during the equilibrium part, typically present low T2 signal, and are variable on delayed hepatobiliary part imaging (Cruite et al, 2010). Due to the complexity of imaging options and overlap, as nicely as multimodality availability, there have been organized efforts to improve report standardization and communication regarding imaging findings, as nicely as recommendations relating to surveillance imaging and screening. Although continued revisions are inevitable, consensus pointers will encourage report standardization, enhance communication, and in the end enhance choice making. Agreement among readers utilizing newer algorithms tends to be average to substantial for professional readers however decrease among novices, suggesting implementation of criteria may require a studying curve (Davenport et al, 2014). Furthermore, pathologic evaluation remains important for diagnostic affirmation; immunohistochemical stains for markers could supply increased accuracy (Du et al, 2012). The average age at presentation is 25 years, and the presence of nodal metastases is common (Ganeshan et al, 2014). Metastatic disease can be widespread at presentation, each in the stomach and chest, with adenopathy being distinguished (>2 cm) in a majority of circumstances (Do et al, 2014). They additionally could show a distinct target sign on T1- and T2-weighted images (Economopoulos et al, 2008). This difference in signal depth makes it comparatively easy to determine the malignant nature of the lesion but not the precise tumor kind. Lymphoma could additionally be relatively hypoenhancing in early dynamic phases, with isointensity in later phases (Coenegrachts et al, 2005). The imaging characteristics of lymphoma overlap with different malignant hepatic lesions. B,T1-weightedout-of-phase picture shows low signal at its margin as a result of chemical shift artifact between the mass and surrounding liver, confirming the presence of bulk fat. Communication with the biliary ductal system on delayed hepatobiliary part imaging with hepatocyte distinction brokers has been reported, serving to to differentiate these tumors from nonneoplastic easy hepatic cysts. Infectious cysts may also communicate with the biliary tree, nonetheless, similar to with advanced cysts from echinococcal illness. However, its differentiation from inflammatory circumstances, which may occur concurrently, may be troublesome (see Chapters 33 and 49). As against the inflammatory related wall thickening with maintained mucosal and submucosal layers, with differential enhancement, gallbladder most cancers typically shows irregular intermediate to excessive T2 sign thickening of the gallbladder wall, with early and extended heterogeneous enhancement, typically in patients with a number of gallstones (Tan et al, 2013). Tumors may present focal nodular thickening along ductal partitions or be discrete intrahepatic masses. Focused assessment of ductal, portal venous, and hepatic arterial involvement is carried out in staging and preoperative imaging. Satellite lesions are common throughout the liver, and these lesions tend to show low sign depth on delayed hepatocyte imaging part (Chung et al, 2009; Kim et al, 2011; Peporte et al, 2013). Intrahepatic cholangiocarcinomas may show adjoining capsular retraction in addition to vascular encasement, sometimes with out tumor thrombus (Chung et al, 2009). Smaller tumors might present early, more uniform arterial enhancement, significantly when less than four cm in measurement (Kim et al, 2011). Intraductal papillary neoplasm of the bile duct is an uncommon subtype of bile duct cancer with traits just like pancreatic intraductal mucinous neoplasms. The majority of tumors occur near the hilum or in extrahepatic ducts, and the scientific outcomes are better than conventional bile duct cancers (Rocha et al, 2012). They often appear as low sign depth buildings in a fluid-filled gallbladder. Choledochal Cysts Choledochal cysts (see Chapter 46) symbolize dilatation of the extrahepatic bile ducts with potential associated intrahepatic biliary duct dilatation. This entity is a comparatively unusual congenital anomaly that usually presents before 10 years of age. Cysts could additionally be related to chronic irritation and increase the chance for cholangiocarcinoma. Recently, there have been advocates for dropping the numeric classification system, as a substitute utilizing a extra descriptive, clinically significant nomenclature (Visser et al, 2004). A, T1-weighted in-phase gradient-echo image shows a peripheral hypointense mass(m)withcapsularretraction. Imaging characteristics mixed with medical presentation and demographic knowledge typically information therapy and predict the analysis. Neoplastic etiologies include tumors arising in the pancreas, such as adenocarcinoma, solid pseudopapillary tumor, neuroendocrine tumors, or pancreatic lymphoma. Metastases, lymphomas, and other uncommon tumors could contain the pancreas (Low et al, 2011). In addition to enhancement traits, such as early arterial enhancement in neuroendocrine tumors, precontrast sign traits, corresponding to hemorrhage with elevated T1 sign in strong pseudopapillary tumors, might provide clues to the diagnosis. Nonneoplastic etiologies embrace focal pancreatitis, accessory spleen, focal fats, congenital anomalies, and other uncommon etiologies. Focal pancreatitis can also cause irregular narrowing of the primary pancreatic duct, as opposed to the abrupt cutoff and upstream dilatation with associated parenchymal atrophy famous in adenocarcinoma (Low et al, 2011; Siddiqi et al, 2007). A, Coronal T2-weighted sequence in a affected person after pancreaticoduodenectomy for pancreatic carcinoma. Bile duct accidents after surgical procedure could be attributable to numerous things, however these could all result in the same result-a stricture on the anastomotic website. Preliminary data counsel grade of tumor enhancement could correlate with tumor grade in adenocarcinomas (Lauenstein et al, 2010). Cystic Lesions of the Pancreas Detection of pancreatic cystic lesions (see Chapter 60) has elevated lately with elevated imaging and improved spatial decision. Diagnostic possibilities embody benign lesions, similar to pseudocysts, serous cystadenomas, and true epithelial cysts; to Chapter 19 Magnetic resonance imaging of the liver, biliary tract, and pancreas 377 benign lesions with potential for malignant degeneration, similar to intraductal mucinous or parenchymal mucinous cystic neoplasms; to malignant lesions, similar to uncommon cystic or necrotic adenocarcinomas or cystic neuroendocrine tumors (Kucera et al, 2012). Evaluation after contrast administration helps assess cyst wall irregularity or enhancement of soft tissue elements. The International Association of Pancreatology stratifies sufferers primarily based on "excessive threat" or "worrisome" features, with pointers regarding resection, endoscopic ultrasound, and imaging follow-up (Tanaka et al, 2012). A recent revision consists of primary duct dilatation greater than 5 mm (without obvious cause) as a worrisome characteristic, but also downgraded size higher than or equal to three cm from high threat to worrisome (Tanaka et al, 2012). The single-shot fast spin-echo T2-weighted sequence is particularly useful, as cystic lesions are excessive in T2 signal and brilliant on these sequences, and communication with the main duct could additionally be more evident (Acar et al, 2011; Campbell et al, 2015). Imaging options could recommend the analysis and are correlated with medical options, including elevated serum immunoglobulin G4, comparatively indolent medical presentation, and response to corticosteroid therapy. Autoimmune pancreatitis could also be diffuse, focal, or multifocal, and often reveals heterogeneous T1 hypointensity, slight T2 hyperintensity, and delayed enhancement as a outcome of associated fibrosis. Diffuse main pancreatic ductal narrowing or irregularity, and upstream common bile duct dilatation or wall thickening, could also be present. There may also be a peripancreatic halo, which seems hypointense on T1- and T2-weighted imaging postcontrast (Heyn et al, 2012). Focal illness, particularly when involving the pinnacle with associated upstream pancreatic and major bile duct dilatation, could mimic ductal adenocarcinoma. Extrapancreatic manifestations can also be current inside the spectrum of immunoglobulin G G4related sclerosing illness, together with bile duct, renal, and retroperitoneal involvement (Kim et al, 2013). Chapter 19 Magnetic resonance imaging of the liver, biliary tract, and pancreas 377.
Boneset. Innopran XL. - How does Boneset work?
- What is Boneset?
- Are there safety concerns?
- Constipation, causing vomiting, fluid retention, aching muscles, reducing inflammation, and stimulating the immune system.
- Dosing considerations for Boneset.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96589
Purchase 40 mg innopran xl amexThis cause is now much much less frequent because of efficient medical therapy with antacid medication blood pressure zebrafish cheap 80mg innopran xl mastercard. Other blood pressure medication iv cheap innopran xl 40 mg free shipping, less widespread causes of choledochoduodenal fistula embody cholelithiasis (see Chapter 32) arrhythmia questions cheap 80 mg innopran xl visa, operative trauma blood pressure chart download generic innopran xl 40mg amex, duodenal diverticula, echinococcal an infection (see Chapter 74), B. The incidence of distal choledochoduodenal fistula secondary to cholelithiasis or operative trauma is variable in numerous components of the world. Large sequence from Argentina reported the incidence of distal choledochoduodenal fistula to be zero. Additionally, there are 2 case reports of choledochoduodenal fistula occurring after blunt abdominal trauma (Chao et al, 2008; Tan et al, 2011). This study also discovered an intriguing association between peripapillary fistula with widespread duct stones and problems of cholangitis. Spontaneous fistula formation between the common duct and the colon has been recorded solely five occasions in the English literature (Bannister et al, 1984; Bose & Sastry, 1983; Guitron-Cantu et al, 2001; Rawas et al, 1987). We are also aware of 1 case of a choledochocolonic fistula that developed after blunt belly trauma (Benson et al, 2001) (see Chapter 122) and another that developed as a complication from diverticulitis (BlancoBenavides & Rodriguez-Jerkov, 1992). Peptic ulcer disease has rarely produced fistulae between the widespread duct, duodenum, and pancreas (Aitken et al, 1986). More lately, a bile duct stricture related to a choledochocolonic fistula was reported following an uncomplicated open cholecystectomy 4 months prior (Munene et al, 2006). Fistulae Involving the Intrahepatic Ducts, Liver, and Lung Thoracobiliary and bronchobiliary fistulae are uncommon (Boyd, 1977; Chan et al, 1984; Cleve & Correa, 1958) and refer to communications between the biliary tree and the pleural cavity or bronchial tree. The three main categories of bronchobiliary fistula are these ensuing from (1) an infection, (2) trauma, and (3) congenital causes (Liao, 2011; Sane, 1971). Worldwide, the principal explanation for bronchobiliary fistula in adults is parasitic disease of the liver, either echinococcal (see Chapter 74) or amebic (see Chapters forty five and 73). In developed countries, iatrogenic harm to the biliary system is the most frequent trigger. The hallmark symptom of a bronchobiliary fistula is biliptysis along side other pulmonary complaints, jaundice, cholangitis, and external biliary fistula or subphrenic abscess. In the presence of an external fistula, injection of distinction answer is probably the most facile and direct strategy. Bronchobiliary fistulae also have been shown by cholescintigraphy (Annovazzi et al, 2008; Andalkar et al, 2004; Gunlemez et al, 2009; Santra et al, 2009; Savitch et al, 1983; Uramoto et al, 2008; Velchik et al, 1991). The surgical therapy of parasitic illnesses of the liver is discussed elsewhere on this guide (see Chapters forty five, 73, and 74). In large series of surgically treated cases of hepatic echinococcal illness in Greece and Turkey, only 2% have been difficult by rupture into the lung or bronchi (Alestig et al, 1972). Amebic abscess of the liver has been reported in affiliation with bronchobiliary fistula in 8% of cases (Razemon et al, 1963). The successful remedy of these fistulae depends on the usage of applicable surgical drainage or resection along side applicable drug therapy (Tuxun et al, 2014). The incidence of bronchobiliary fistula as a consequence of surgically handled calculous or neoplastic disease of the hepatobiliary tract and adjacent structures has been lowering, as sufferers are operated on earlier in the course of their illness and by better-trained surgeons (Ramesh et al, 1991; Warren et al, 1983). Reports of bronchobiliary fistula brought on by more lately developed liver tumor ablative therapies, similar to radiofrequency ablation, are beginning to emerge (Kim et al, 2005; Tran et al, 2007; Yoon et al, 2009). The incidence of bile duct harm in the midst of cholecystectomy has increased with the appearance of laparoscopic cholecystectomy (Davidoff et al, 1992) (see Chapter 35 and 38). Bronchobiliary fistulae secondary to bile duct harm are a late consequence of the occasion in sufferers with uncared for or recurrent strictures after unsuccessful operations. Untreated choledocholithiasis difficult by repeated episodes of biliary obstruction and cholangitis is another, albeit infrequent, reason for bronchobiliary fistula. Brem and colleagues (1990) reported the profitable treatment of an 87-year-old affected person with this medical scenario by endoscopic papillotomy alone. Bronchobiliary fistulae should be handled by transampullary biliary decompression to reduce the fistula tract stress. Some patients with a persistent fistula or infection would require transthoracic debridement and drainage. Posttraumatic thoracobiliary fistulae are extremely rare (Oparah & Mandal, 1978) (see Chapter 122). Ivatury and colleagues (1984) reported on 3 sufferers and reviewed 32 beforehand reported circumstances. All patients had pleural effusion in the end proven to be bilious after aspiration. Historically, successful remedy required pulmonary decortication, restore of the diaphragm, and adequate drainage above and below the diaphragm. More latest publications have described profitable remedy via endoscopic decompression of the biliary system and pleural drainage. Although the optimal administration strategy remains undefined, current reports suggest aggressive surgical intervention may be reserved for instances that fail conservative administration (Ball et al, 2009; Eryigit et al, 2007; Gandhi et al, 2009; Navsaria et al, 2002; Singh et al, 2002). Neuhauser and colleagues (1952) first described congenital bronchobiliary fistula in an infant with a tract speaking between the best primary stem bronchus and the hepatic duct that passed by way of the posterior mediastinum. There are a number of choices for reestablishing communication with the intestinal tract, together with Roux-en-Y cholodochojejunostomy, fistula enteric anastomosis, and portoenterostomy in instances of extrahepatobiliary atresia (Croes et al, 2010). Yamaguchi and colleagues (1990) reported one adult affected person with a congenital bronchobiliary fistula and summarized the information of sixteen previously reported cases, 4 of them adults. The only congenital bronchobiliary fistula in an aged individual was reported recently by Uramoto (2008). On microscopic examination, the proximal portion of the fistula in most sufferers resembles the bronchus, and the distal segment resembles the esophagus; the embryologic explanations for this anomaly are conjectural (Dyon et al, 1978; Sane et al, 1971). Transthoracic excision of the fistula and surgical correction of related biliary anomolies is often curative. Diagnostic Tests Laboratory Testing Sputum evaluation for bilirubin and viable scolices or membranes can be utilized as laboratory proof to set up the prognosis of bronchobiliary fistulae secondary to echinococcosis (Gerazounis et al, 2002). Although no particular blood exams for biliaryenteric fistula can be found, serum liver function tests, electrolytes, and blood counts are helpful in the evaluation and administration of a affected person with a symptomatic biliary fistula. Hricak and Vander Molen (1978) instructed that the comparatively low incidence of pneumobilia in gallstone ileus is due to the cystic duct obstruction-preventing retrograde passage of air into the biliary tree. Direct Cholangiography Direct injection of contrast materials is one of the only ways to outline the normal and pathologic anatomy of the biliary tract (see Chapter 20). Intraoperative cholangiograms are another technique of instantly imaging the biliary tree. Endoscopically, the alimentary facet of a fistula itself of the ampulla of Vater can generally be cannulated to obtain a high-quality radiograph of the speaking biliary anatomy (Chatzoulis et al, 2007; Moreira et al, 1984; Stempfle & Diamantopoulos, 1976; Watkins et al, 1975). Similarly, the largely unappreciated and frequently asymptomatic parapapillary choledochoduodenal fistula has been found to be fairly frequent (Hunt & Blumgart, 1980; Karincaoglu et al, 2003b; Kuroki et al, 2005; Tanaka & Ikeda, 1983). B, Plain radiograph reveals a number of dilated loops of small bowel (black arrowheads), a number of calcified gallstones (white arrowheads), three gallstones positioned in small bowel in the upper abdomen, and one obstructing gallstoneinthepelvis.
Syndromes - Ages 40 - 49: 95 - 530 ug/dL
- If you have ever had any bleeding problems
- Bronchoscopy -- camera down the throat to see the airways and lungs
- Metallic taste in the mouth
- Emphysema, which involves destruction of the lungs over time
- Diarrhea
- Decreased urine
- Childhood infections, such as meningitis, mumps, scarlet fever, and measles
- Type 1 or type 2 diabetes
- Kidney dialysis
Buy innopran xl 40 mg low priceVirani S pulse pressure normal rate cheap innopran xl 40 mg with mastercard, et al: Morbidity and mortality after liver resection: results of the patient security in surgery research prehypertension medicine buy innopran xl 80 mg with mastercard, J Am Coll Surg 204(6):1284�1292 heart attack enzyme cheap 40mg innopran xl with amex, 2007 blood pressure facts 80mg innopran xl with amex. Wehry J, et al: Restrictive blood transfusion protocol in liver resection patients reduces blood transfusions with no enhance in affected person morbidity, Am J Surg 209(2):280�288, 2015. Wijeysundera D, et al: Epidural anaesthesia and survival after intermediate-to-high non-cardiac surgery: a population-based cohort study, Lancet 372(9638):562�569, 2008. Although this chapter mainly focuses on the particular perioperative issues of patients with cirrhosis and continual liver disease, a brief dialogue of the preoperative evaluation and perioperative problems that may happen in patients undergoing pancreaticoduodenectomy is presented. When evaluating perioperative risks for sufferers with continual liver diseases, three main elements must be thought of: hepatic reserve, comorbid conditions, and the complexity of the planned surgical process. In sufferers with persistent hepatitis C infection and cirrhosis, diabetes will increase the danger for the development of ascites, renal dysfunction, and bacterial infections (Elkrief et al, 2014). In instances of autoimmune and infectious hepatitis, immunomodulation and antiviral therapies are useful in the preoperative interval, and the doses of steroids are often elevated to mitigate adrenal insufficiency (Chan, 2005; Hadziyannis, 2006; Keeffe et al, 2008; Lau et al, 2005; Marcellin et al, 2008). Class A (5 to 6 points) refers to well-compensated cirrhosis; class B (7 to 9 points) and sophistication C (10 to 15 points) describe cases of cirrhosis that are in a state of mild and extreme decompensation, respectively. The mortality rates for elective or emergent extrahepatic surgery range from 0% to 7. Preoperative cholestasis and hepatic steatosis are vital threat elements for major issues together with mortality (McCormack et al, 2007). Nutrition Malnutrition is often underappreciated in cirrhotic sufferers as a end result of the frequent parameters of dietary status (body weight, body mass index, and albumin level) are unreliable (Juakiem et al, 2014). Up to 40% of cirrhotic patients undergo from extreme malnutrition, a comorbid condition that confers the next danger of perioperative morbidity and mortality (Sam & Nguyen, 2009) (see Chapter 26). Combined with diabetes mellitus, malnutrition in cirrhotic patients increases the risk of hepatic encephalopathy (Kalaitzakis et al, 2007). Enhancing the nutritional standing of cirrhotic patients could also be related to improved outcomes. Oral diet and enteral feeding by way of a nasogastric tube are preferred and can safely be used in patients with esophageal varices (Hebuterne & Vanbiervliet, 2011). Branched-chain amino acids are advocated as a end result of they could reduce the chance of hepatic encephalopathy, but their actual benefit is marginal (Harrison, 2006; Marchesini et al, 2003). Adequate management of ascites might require several months and could be achieved with a low-sodium food plan, judicious use of diuretics, and/or giant quantity paracentesis. Portal hypertension can be recognized early by transient elastography, and this analysis confers a higher risk of hospital mortality (Berzigotti et al, 2013; Bureau et al, 2008; Nguyen et al, 2009). Ascites and varices related to portal hypertension are related to elevated dangers of variceal hemorrhage, bacterial peritonitis, and hospital mortality in cirrhotic patients present process varied surgical procedures, similar to cholecystectomy, coronary artery bypass grafting, abdominal aortic aneurysm restore, and colorectal surgical procedure (Csikesz et al, 2009; Nguyen et al, 2009) (see Chapter 77). Abnormal blood move in the portal venous system can be easily demonstrated by Doppler ultrasound and correlates nicely, when present, with increased mortality (Harrod-Kim & Waldman, 2005). Preoperative interventions ought to be initiated to reduce hepatic venous strain and the risks of variceal bleeding. The mixture of octreotide and diuretics can lead to improvement in portal and systemic hemodynamics (Kalambokis et al, 2006). Anemia Anemia is a typical complication of liver diseases that often develops roughly 40 months after the onset of cirrhosis, even within the absence of decompensation or esophageal varices (Qamar et al, 2009). Anemia is as a outcome of of many components, including bleeding, hemolysis, splenic sequestration, hepatic dysfunction, malnutrition, and iron and vitamin deficiency. Iron supplementation should be administered only within the presence of documented deficiency. Autologous blood transfusion and administration of erythropoietin have been used efficiently to mitigate the need for red blood cell transfusions (Kato et al, 2009; Silver et al, 2006). Coagulopathy Similar to anemia, coagulation abnormalities are frequent in cirrhotic sufferers and are because of many causes, including decreased hepatic synthetic operate, irregular synthesis of coagulation factors, malnutrition, vitamin K deficiency, thrombocytopenia, and dysfibrinogenemia (Qamar et al, 2009). Administration of cryoprecipitate is advocated when serum fibrinogen levels are less than a hundred mg/dL in the presence of bleeding (Anderson et al, 2013). Data on the advantages of fibrinogen concentrates are limited to trauma and big hemorrhage (Fenger-Eriksen et al, 2008). Transfusion of platelets is really helpful earlier than invasive procedures for average thrombocytopenia of less than 50,000/�L (Johansson, 2009; Rebulla, 2001). A preoperative partial stress of oxygen in arterial blood (PaO2) of 50 mm Hg or a macroaggregated albumin scan quantification shunt fraction of 20% or higher is related to prohibitive mortality rates from cardiorespiratory problems (Arguedas et al, 2003). Mortality of portopulmonary hypertension is high, with 1- and 5-year survival rates of 54% and 14%, respectively (Swanson et al, 2008). Right aspect of the guts catheterization helps to determine the various causes of pulmonary hypertension and is the most effective diagnostic software for portopulmonary hypertension (Krowka et al, 2006). Electrolytes Electrolyte abnormalities are frequent in sufferers with energetic alcohol use and persistent liver diseases. The causes of hyponatremia ought to be elucidated and addressed through various strategies, such as correction of fluid deficit or fluid restriction, and cautious and transient use of vasopressin-2 (V2)-receptor antagonists, such as conivaptan, satavaptan, and lixivaptan (Kwo, 2014). Other electrolyte imbalances (hypokalemia, hypomagnesemia, and hypophosphatemia) can result from using loop diuretics, persistent respiratory alkalosis, or malnutrition and must be corrected earlier than surgery to limit cardiac arrhythmias, peritonitis, and hepatic encephalopathy. Cardiovascular and Respiratory Parameters Repiratory alkalosis tends to develop in sufferers with continual liver illness. Patients with cirrhosis also are at risk for coronary artery illness due to a excessive prevalence of cigarette smoking and diabetes mellitus (Dam et al, 2013; Hickman & MacDonald, 2007). Patients with alcoholic liver illness and iron overload are predisposed to cardiomyopathy and cardiac arrhythmias (Moller & Henriksen, 2008). In sufferers with cirrhosis, infections increase mortality fourfold with a median mortality rate of 38% (30% inside 1 month after infection, whereas one other 30% die within 1 year) (Arvaniti et al, 2010). General anesthesia for hepatic and Surgical Procedures the complexity of the surgical process influences outcomes (see Chapters 24, seventy seven, and 103D). Emergent surgical procedure and unscheduled laparotomy for trauma carry a excessive mortality (Demetriades et al, 2004; Georgiou et al, 2009). Cholecystectomy and surgical repair of umbilical and inguinal hernia have been associated with the lowest morbidity and mortality threat, whereas pancreatic surgical procedure, cardiovascular, and trauma surgical procedure correlated with the very best (De Goede et al, 2012). The morbidity and mortality rates of cardiovascular operations, open cholecystectomy, hysterectomy, nephrectomy, and transurethral resection of the prostate are also greater in comparison to laparoscopic and elective interventions (Csikesz et al, 2009; Filsouf et al, 2007; Pavlidis et al, 2009; Shaheen et al, 2009). Assessment for Pancreatobiliary Surgery Surgery for gallbladder bile duct, and pancreatic cancer remains very difficult and requires skilled surgical and anesthesiology teams. During the past four many years, the mortality associated with standardized Kausch-Whipple pancreaticoduodenectomy for adenocarcinoma of the pancreatic head has dramatically improved (Richter et al, 2003) (see Chapters sixty six and 67). However, postoperative problems are frequent and embody cardiopulmonary occasions, fistula, delayed gastric emptying, sepsis, and bleeding (Schmidt et al, 2004). Predictive fashions of postoperative morbidity based mostly on the estimation of physiologic capability and surgical stress rating in pancreatic surgical procedure are associated with combined outcomes (Deyle et al, 2011; Hashimoto et al, 2010). Other scoring techniques enable preoperative danger stratification, prediction of major issues associated with pancreaticoduodenectomy, and careful patient selection.
Discount innopran xl 80 mgThe simultaneous administration of ascorbate and -tocopherol is more practical in inhibiting oxidation than either alone (Niki et al pulse pressure vs heart rate cheap innopran xl 40 mg otc, 1995) arteria espinal anterior cheap innopran xl 40 mg with amex. The synergistic protecting results of vitamin C and vitamin E in preventing lipid peroxidation and cellular damage counsel that these vitamins ought to be administered collectively for maximal potential benefit (Bulger & Helton heart attack zippy buy innopran xl 80mg with mastercard, 1998) prehypertension kidney disease purchase 80mg innopran xl. A prospective randomized study in sufferers undergoing liver resection by utilizing an infusion containing 10 mg -tocopherol acetate and 1 g ascorbate administered before reperfusion demonstrated much less plasma lipid peroxidation and acute liver damage and fewer postoperative problems (Cerwenka et al, 1999). Cirrhosis and Liver Failure Patients with cirrhosis have a quantity of hormonal and metabolic alterations (see Chapter 79). These changes cause loss of fats and muscle mass, development failure, glucose intolerance, hyperinsulinemia, insulin resistance, increased plasma glucagon and catecholamines, elevated serum free fatty acids, elevated glycerol, hypoproteinemia, hyperammonemia, hypophosphatemia, and alterations in plasma and cerebrospinal fluid amino-acid profiles (Achord, 1987; Henriksen et al, 1985; Petrides & De Fronzo, 1989; Riggio et al, 1984). These metabolic aberrations result in altered metabolism of fat, protein, and carbohydrate. In addition, there is a rise in skeletal muscle proteolysis for vitality provision, which finally ends up in eventual muscle losing. Compounding the metabolic alterations of cirrhosis are points that predispose patients with cirrhosis to malnutrition, together with decreased dietary intake because of anorexia, nausea and vomiting, and the widespread practice of imposing protein restriction in an effort to stop encephalopathy. The practice of routine protein restriction should be abandoned in an already malnourished affected person because it exacerbates the problems inherently related to malnutrition and prohibits the objective of liver regeneration (Box 26. This reality supports the argument that enteral administration of glucose is the preferred route of feeding because of the impact on insulin release, which is vital to the operate of the regenerating liver (Ozawa, 1992). Transplantation In the first 6 hours after liver transplantation, glucose use by the transplanted liver is impaired until the redox state of the mitochondria improves (Ozaki et al, 1991) (see Chapter 113). After 6 hours, normally functioning liver allografts shift substrate use from fat to glucose, whereas failing livers continue to use fats. This shift in metabolism may be followed by measuring the plasma focus of complete ketone bodies and arterial ketone body ratio (Takada et al, 1993). Based on these observations, Takada and colleagues advised that glucose must be administered in small portions within the instant postoperative period with out insulin to keep away from suppressing peripheral fat mobilization. Glucose infusion ought to be increased slowly while mitochondria respiration recovers and the Krebs cycle turns into active. When the redox state of mitochondria is sufficiently improved, amino acids and increased amounts of glucose could be administered. It has been demonstrated that intraportal insulin administration augments liver regeneration during the first postoperative transplant week by enhancing hepatic perform in live-donor liver transplant recipients (Xu et al, 2009). The nutritional standing of the donor liver could also be an essential factor affecting posttransplant allograft function. Initially, it was believed that liver allografts obtained from fasted donors were more susceptible to anoxic liver damage than allografts obtained from donors being administered glucose till the time of liver donation because of an absence of glycogen as a supply of glucose from glycolysis in the fasted group (Bradford et al, 1986). Liver Resection Numerous metabolic alterations happen within the regenerating liver after liver resection (see Chapter 6). Krebs cycle exercise is depressed, as is the reduction-oxidation state of the hepatic mitochondria, with a swap from the usage of glucose to fat as the popular source of power by the use of -oxidation (Nakatoni et al, 1981). Because hyperglycemia and hyperinsulinemia suppress the release of fatty acids from adipose tissue and reduce ketone body manufacturing by the liver (Riou et al, 1986), hypertonic glucose infusions and insulin administration ought to be avoided in the instant (<6 hours) postoperative period (Ozawa, 1992). These metabolic alterations emphasize the importance of glycemic control earlier than, during, and instantly after operation, such as with preoperative carbohydrate loading. The regenerating liver has an increased demand for particular amino acids, and provision of those within the food plan accelerates regeneration. A detailed discussion of nutritional support for sufferers with acute pancreatitis is covered in Chapter 54. Cirrhosis can result in inefficient vitality expenditure resulting from increased Cori cycle exercise, elevated protein turnover rates with altered amino-acid profiles, elevated gluconeogenesis, and elevated lipid oxidation (Holroyde & Reichard, 1981). This syndrome is related to anorexia, tissue losing, malnutrition, weight reduction, and a lack of compensatory improve in feeding. The pathogenesis relies on disorders of carbohydrate, protein, lipid, and vitality metabolism mediated by proinflammatory cytokine elaboration and an total increase in leptin (Bruera et al, 2000; Tisdale, 2003; Walker, 2001;). Nutritional deficits can also arise solely after a very lengthy time or seem abruptly in response to acute illness or treatment-related complications. For instance, sufferers with persistent pancreatitis and belly pain may have profound malnutrition due to meals avoidance, dietary restriction, exocrine or endocrine insufficiency, pancreatic and/or biliary duct obstruction, and continual malabsorption (see Chapters fifty seven and 58). Patients with severe acute pancreatitis, and notably these with acute superimposed Pancreatic Exocrine Insufficiency Patients with benign and malignant circumstances of the pancreas can expertise biliary and/or pancreatic duct obstruction, which may lead to malnutrition attributable to maldigestion and malabsorption. The majority of patients with pancreatic carcinoma are seen with malnutrition and weight loss at the time of diagnosis. Fourth, pancreatitis develops in plenty of patients with pancreatic duct obstruction, which can scale back exocrine perform. Multiple research have reported that patients with persistent pancreatitis and pancreatic cancer are additionally vitamin D poor (Cho et al, 2013; Klapdor et al, 2012). Pain Patients with pancreatic disease usually experience extreme abdominal ache due to involvement of the celiac plexus by tumor, pancreatic duct obstruction, and/or pancreatitis. When abdominal ache is exacerbated by oral consumption, patients will avoid food consumption or modify their food plan, which contributes to a malnourished state (Rasmussen et al, 2013). In many cases, patients unconsciously keep away from certain foods, corresponding to those containing fat, which during time leads to weight reduction. Biliary Obstruction Biliary obstruction in patients with pancreatic head illness could be associated with nutritional deficits, that are corrected once obstruction is relieved either surgically or by nonoperative means, such as endoscopic stenting or percutaneous drainage (see Chapter 8). On the other hand, patients with long-standing obstructive jaundice related to profound malnutrition will more than likely benefit from a period of dietary repletion before present process main belly surgery. Refeeding bile into the small bowel improves the digestion and absorption of fats and reduces the amount of hepatic bile output via the enterohepatic recirculation of bile salts. Most patients can tolerate bolus infusion of bile into their small bowel of a hundred and fifty mL or less each four hours, and they are often taught to do that on their own at house. An different to enteric bile refeeding is to provide oral bile salts in the form of ursodeoxycholic acid (300 mg, 4 occasions daily) to kind micelles for fats absorption (Tripathy et al, 1996). Malnourished patients with full biliary obstruction or disconnection might require specialised semielemental diets to avoid fats malabsorption. These sufferers are also in danger for fat-soluble vitamin deficiency and must be offered water-soluble forms Cancer-Related Effects on Metabolism Direct adverse results of cancers on nutrition and metabolism have been identified to exist for years but are poorly understood. The mechanism(s) by which pancreatic cancer induces cachexia are largely unknown however believed to be modulated, partially, by way of activation of proinflammatory mediators that stimulate systemic inflammation, the magnitude of which is related to poor prognosis (Fearon et al, 2006; McMillan et al, 2009, 2013) (see Chapter 11). A combination of factors-exocrine insufficiency, tumor results, ache, alcohol use-leading to malnutrition in patients with pancreatic disease has a detrimental effect on affected person outcomes and treatment. The diploma of malnutrition, as measured by weight alone, is commonly greater than 25% of preillness weight (Wigmore et al, 1997). Others have noticed that more than 80% of sufferers are cachectic at diagnosis; this proportion increases whereas the disease progresses (Tisdale, 2003) and is related to poor prognosis (Bachmann et al, 2008). These metabolic and nutritional responses negatively influence remedy plans and might often delay resection, chemotherapy, and result in progressive deterioration in efficiency status.
Innopran XL: 80 mg, 40 mg
Buy innopran xl 80mg visaIn a couple of hours heart attack 90 blockage innopran xl 40mg line, catabolism of Biliary Atresia Biliary atresia is a typical reason for neonatal cholestasis and occurs in 1 in 8000 to 15 blood pressure medication sleepy discount 40 mg innopran xl,000 newborns (Sokol et al arteria vesicalis order 40mg innopran xl with mastercard, 2003) (see Chapter 40) prehypertension and anxiety purchase innopran xl 40 mg online. Biliary atresia develops both during embryogenesis or the perinatal period, and completely different subgroups have been postulated, with ongoing analysis efforts to establish underlying causes (Davenport, 2005; Mack & Sokol, 2005) (see Chapter 1). Pathologic traits embrace progressive inflammatory modifications, subsequently leading to obliteration of intrahepatic and extrahepatic biliary ducts. Treatment is predicated on surgical procedures, largely Kasai, and infrequently liver transplantation. Cholescintigraphy is effective as a way to exclude biliary atresia, however not as a way to positively diagnose biliary atresia. If excreted biliary tracer is detected scintigraphically within the gallbladder or bowels, biliary atresia is successfully excluded (Ziessman, 2014). Biliary atresia does manifest on scintigraphy as a lack of tracer passage into gallbladder or bowels, so the end result may be brought on by biliary atresia. However, irregular lack of excreted biliary tracer passage into the gallbladder or bowels additionally might be brought on by severe hepatocellular dysfunction from hepatitis or different etiology (without biliary atresia), or with an related absence of bile manufacturing and (nonobstructive) halt of biliary flow, or from interlobular bile duct paucity. Given this risk of extreme hepatocellular dysfunction leading to nondiagnostic cholescintigraphy, two methodologic approaches are frequent: (1) pediatric sufferers are normally pretreated with phenobarbital (5 mg/kg/day) for as long as 5 days before cholescintigraphy, and (2) cholescintigraphy imaging typically continues at multiple time points as long as 24 hours after tracer injection, to enable for attainable markedly slow biliary circulate. Phenobarbital earlier than the scan ends in activation of liver enzymes and elevated bile manufacturing, enhancing specificity. Its near-perfect sensitivity for biliary atresia makes cholescintigraphy an efficient assay for excluding biliary atresia. Its restricted specificity demonstrates that a scarcity of biliary tracer transit into gallbladder or bowel, as a scintigraphic biomarker, has insufficient specificity to positively diagnose atresia and information choice making on whether or not surgical intervention is important (Kianifar et al, 2013). Cholescintigraphy is diagnostically helpful as a means to "rule out" biliary atresia. Sulfur colloid tracer accumulation in vertebral marrow is typically faintlydetectable,althoughnotinthispatient. Broad examples of etiologies associated with low hepatic uptake include diffuse hepatic diseases corresponding to advanced cirrhosis and extreme hepatitis. With such associations noticed, investigators have explored whether hepatic colloid uptake may offer a semiquantitative biomarker of hepatic perform. In at least one study (Esmaili et al, 2008), no correlation was discovered between scintigraphic semiquantitative uptake measurements and Child-Pugh classification, an index of liver perform. The finding of diminished colloid uptake in the best and left liver lobes, together with sparing of the caudate lobe, has been related to Budd-Chiari syndrome (hepatic vein thrombosis) (Oppenheim et al, 1988). Various causes of hypersplenism can manifest as abnormally high splenic uptake (Rutland, 1992). The differential for "chilly defects" or photopenic defects- foci of absent or comparatively low colloid uptake-within the liver parenchyma is extensive(Oppenheim et al, 1988), together with hepatoma, metastases, and many different pathologic entities. Clinical studies reveal that arterial infusion improves tumor uptake of sure chemotherapeutic agents in contrast with portal venous or systemic venous infusion (Callahan & Kemeny, 2010). Cancerous liver tumors derive/stimulate a nutrient blood supply from the arterial system (by tumor neoangiogenesis). Catheters could hook up with a subcutaneously implanted port or an infusion pump system. Pumps allow slow, steady drug infusion, typical of hepatic arterial chemotherapy; such techniques are more typically found within the United States. In a port-catheter system, the implanted port could accessed for connection to an external pump system. In Europe, transiently placed catheters and port-catheter methods are extra frequent. The tracer infusate, followed by a saline flush, traverses the connected catheter into the bloodstream of the hepatic artery or accessed branch. Hepatic arterial blood circulate is laminar, significantly alongside straighter lengths of the artery. Extrahepatic tracer accumulations, when tracer is infused slowly, are normally attributable to variant hepatic arterial anatomy, similar to branches supplying extrahepatic viscera. When the tracer is bolused, however, such extrahepatic tracer accumulations could be mere artifact of bolus technique. In our experience, mere heterogeneity of intrahepatic uptake is relatively common and not clearly associated with adverse outcomes. Chapter 17 Role of nuclear drugs in prognosis and administration of hepatopancreatobiliary illness 315. Akhurst T, et al: Recent chemotherapy reduces the sensitivity of [18F] fluorodeoxyglucose positron emission tomography within the detection of colorectal metastases, J Clin Oncol 23:8713�8716, 2005. Annunziata S, et al: Diagnostic accuracy of fluorine-18-fluorodeoxyglucose positron emission tomography in the analysis of the first tumor in sufferers with cholangiocarcinoma: a meta-analysis, Biomed Res Int 2014:247693, 2014. Baillie J: Sphincter of Oddi dysfunction, Curr Gastroenterol Rep 12: 130�134, 2010. Bang S, et al: the medical usefulness of 18-fluorodeoxyglucose positron emission tomography within the differential diagnosis, staging, and response evaluation after concurrent chemoradiotherapy for pancreatic most cancers, J Clin Gastroenterol 40:923�929, 2006. Bar-Meir S, et al: Frequency of papillary dysfunction among cholecystectomized sufferers, Hepatology four:328�330, 1984. Boulahdour H, et al: the hot spot hepatobiliary scan in focal nodular hyperplasia, J Nucl Med 34:2105�2110, 1993. Brunot B, et al: Biopsy and quantitative hepatobiliary scintigraphy in the evaluation of liver transplantation, J Nucl Med 35:1321�1327, 1994. Cicala M, et al: Quantitative cholescintigraphy within the assessment of choledochoduodenal bile move, Gastroenterology 100:1106�1113, 1991. Cicala M, et al: Outcome of endoscopic sphincterotomy in submit cholecystectomy sufferers with sphincter of Oddi dysfunction as predicted by manometry and quantitative choledochoscintigraphy, Gut 50: 665�668, 2002. Davenport M: A challenge on the use of the phrases embryonic and perinatal within the context of biliary atresia, Hepatology forty one:403�404, writer reply 404-405, 2005. Dimitroulopoulos D, et al: Long acting octreotide within the treatment of superior hepatocellular cancer and overexpression of somatostatin receptors: randomized placebo-controlled trial, World J Gastroenterol 13:3164�3170, 2007. Eppard E, et al: Ethanol-based post-processing of generator-derived sixty eight Ga toward kit-type preparation of 68Ga-radiopharmaceuticals, J Nucl Med fifty five:1023�1028, 2014. Esmaili J, et al: Correlation of liver-spleen scan findings with modified Child-Pugh classification, Rev Esp Med Nucl 27:99�102, 2008. Herman P, et al: Hepatic adenoma and focal nodular hyperplasia: differential diagnosis and treatment, World J Surg 24:372�376, 2000. Kaemmerer D, et al: Neoadjuvant peptide receptor radionuclide therapy for an inoperable neuroendocrine pancreatic tumor, World J Gastroenterol 15:5867�5870, 2009. Kaltsas G, et al: Recent advances in radiological and radionuclide imaging and remedy of neuroendocrine tumours, Eur J Endocrinol 151:15�27, 2004. Kennedy A, et al: Radioembolization for the treatment of liver tumors: common rules, Am J Clin Oncol 35:91�99, 2012.
References - Moore KN, Jensen L: Testing of the Incontinence Impact Questionnaire (IIQ-7) with men after radical prostatectomy, J Wound Ostomy Continence Nurs 27(6):304-312, 2000.
- Bussani R, Silvestri F. Images in cardiovascular medicine. Sudden death in a woman with fibroelastoma of the aortic valve chronically occluding the right coronary ostium. Circulation 1999;100:2204.
- Redline S, Yenokyan G, Gottlieb DJ, et al. Obstructive sleep apnea hypopnea and incident stroke. Am J Respir Crit Care Med 2010; 182: 269-277.
- Jones CE, Liang IYS, Gwirtz PA: Effects of alpha-adrenergic blockade on coronary autoregulation in dogs, Am J Physiol 253:H365, 1987.
|