Kamagra Oral Jelly
Jennifer M. Kalish, M.D., Ph.D. - The Childrenĺs Hospital of Philadelphia
- Philadelphia, Pennsylvania
Purchase kamagra oral jelly 100mg mastercardParasympathetic preganglionic fibers arising from the sacral nerve roots follow the branches of the hypogastric vessels and synapse in the uterovaginal plexus erectile dysfunction breakthrough discount 100 mg kamagra oral jelly visa. As beforehand famous impotence caused by medication cheap kamagra oral jelly 100 mg fast delivery, the hypogastric plexus (nerves) descends into the pelvis over (anterior to) the aorta and the left widespread iliac vein 498a impotence purchase kamagra oral jelly 100mg overnight delivery, entering the presacral house erectile dysfunction caffeine kamagra oral jelly 100mg free shipping. Spinal wire segments and somatic motor neurons controlling perivesical muscle and parasympathetic preganglionic neurons are situated in S2, S3, and S4 segments. Sensory impulses (visceral sensory) return to the spinal twine by way of related pathways, transmitting via parasympathetic pathways and sacral wire segments. Some sensory fibers from the trigone and the urethrovesical junction transmit ache through the pudendal nerves. Clearly, some sensory afferents attain the spinal cord through the hypogastric nerve plexus. Contemporary neuroanatomy data suggest a sparse number of sympathetic nerves in the bladder musculature, aside from the trigone, the place larger numbers of sympathetic versus parasympathetic nerves are discovered. During the filling part, bladder volume will increase whereas parasympathetic output is inhibited. At the identical time, sympathetic discharge causes the urethral muscle to contract, thereby retaining a high-pressure gradient that favors the urethra over the bladder. When the extent of fullness transmits, via afferent sensors and fibers, a feeling of discomfort (associated with excessive bladder volume), the mind in turn dispatches a launch message, which triggers a parasympathetic discharge. Concurrently, sympathetic synapses in parasympathetic ganglia modulate ganglionic transmission, resulting in urethral muscle rest (by blocking contraction). The pressure gradient shifts in such a means that bladder pressure exceeds urethral stress, thereby allowing micturition. Numerous External anal afferent fibers are sphincter muscle carried centripetally through approximately the identical sympathetic splanchnic nerves that transmit preganglionic fibers. Somatic nerves that management voluntary muscle exercise, are shown in green; sensory (afferent) organs and muscles are black and may share pathways with autonomic and somatic nerves. Preganglionic fibers are proven as solid purple (sympathetic) or blue (parasympathetic) traces. Sympathetic nerves arise from the lower thoracic and lumbar cord segments and synapse in outlying ganglia on the aorta or its primary branches. Postganglionic fibers journey alongside the ovarian vessels or the uterovaginal vessels. Parasympathetic enter arises within the sacral twine and travels through pelvic splanchnic nerves to the assorted organs where synapses occur and brief postganglionic fibers transmit impulses. Parasympathetic preganglionic neurons are positioned in S2, S3, and S4 wire segments. Postganglionic parasympathetic neurons lie throughout the partitions of the bladder and the ureter, whereas preganglionic sympathetic fibers are found in the vesical plexus (pelvic plexus). The pelvic portion of the sigmoid colon, rectum, and anus receives sympathetic fibers via the superior and inferior hypogastric plexuses. The inferior hypogastric plexus receives parasympathetic fibers from S2, S3, and S4 nerve roots. The rectal plexus (pelvic plexus) is carefully utilized to the rectal connective tissue and carries sympathetic, parasympathetic, and afferent nerves. The pudendal nerve carries somatic efferent fibers to the levator ani and the external sphincter ani. Sympathetic preganglionic fibers are distributed from twine nuclei positioned at T8, T9, T10, T11, and T12, and at L1, L2, and L3; the latter relay throughout the ganglia of the sympathetic trunks and from there to plexuses, where synapses happen and postganglionic fibers distribute themselves to the intestines. Afferent and efferent somatic fibers, via the pudendal nerves, innervate voluntary (striated) muscles such because the levator ani and external sphincter ani. Pelvic Plexus the inferior mesenteric plexus receives fibers from the superior mesenteric plexus through the lumbar splanchnic nerves. Branches from the inferior mesenteric plexus accompany arteries to respective intestinal segments. This plexus receives parasympathetic preganglionic nerves, as nicely as somatic branches, from S2, S3, and S4 nerve roots via pelvic splanchnic nerves. The rectal plexus is a subdivision of the inferior hypogastric plexus and carries sympathetic preganglionic fibers, afferent sensory fibers, and parasympathetic preganglionic fibers. The inferior hemorrhoidal branches of the pudendal nerves receive sensory impulses from anal receptors positioned in the mucosa and the submucosa, especially in the anal valves. The inside anal sphincter is provided by sympathetic nerves originating in the L5 wire segment. The exterior anal sphincter is innervated by somatic efferent fibers by way of the inferior hemorrhoidal nerves and perianal branches (S4). Venous drainage is regularly missed in anatomic drawings of the feminine pelvis. This is rather unusual in that most bleeding encountered during surgical operations is venous in origin. Note the collateral circulation that exists between the inferior mesenteric vein (portal system) via the superior rectal vein and the interior iliac veins (systemic system) through the middle rectal and inferior rectal veins. Note the connectors between the internal pudendal veins via the inferior rectal veins and the middle rectal veins to the inner iliac veins. The help of the bladder neck can be readily seen in the anatomy laboratory by sawing via symphysis and tilting it ahead. The anterior pubourethral ligaments are less outstanding however attach the urethra as it emerges under the symphysis to the anteroposterior margin of the symphysis pubis. The posterior facet and bladder base are in close contact to the lower uterine corpus (anterior surface of the uterus) and are, in fact, connected to the cervix and vagina by the bladder pillars or vesicocervical and vesicovaginal pillars. The deeper parts of the cardinal ligaments are connected to the bladder base and the upper anterolateral vagina. The most substantial supporting buildings for the bladder base and the upper vagina are deep parametrial structures (deep cardinal ligaments). These substantial structures encompass fats, connective tissue (fibrous), and vascular channels. When these are severed, the bladder and the vagina could additionally be more or less totally mobilized. A not-uncommon location for ureteral harm is the ureterovesical junction, which is intrinsically throughout the substance of the bladder. This oblique course creates constriction and closure of the terminal ureter when the bladder contracts and empties. The ureteral closure aspect of bladder anatomy is necessary in that it prevents reflux of urine retrograde into the ureters when bladder stress rises. Sigmoid Colon the anatomic relationships of the sigmoid colon and the rectum to different pelvic viscera are critically essential to the gynecologist. Note that the sigmoid colon drapes over the left adnexa, nearly overlaying the tube and the ovary. The decrease sigmoid colon then may be positioned at least partially posterior to the ovary and broad ligament. The entire sigmoid colon is connected to a mesentery and due to this fact is an intraperitoneal structure. Within the hollow of the sacrum, the sigmoid colon joins to the brief straight rectum.
Cheap 100 mg kamagra oral jelly fast deliveryFinally erectile dysfunction diabetes qof cheap 100 mg kamagra oral jelly free shipping, the minimize edges of the perineum are approximated by a operating suture of 3-0 Vicryl erectile dysfunction newsletter purchase 100mg kamagra oral jelly otc. When the corpus is severed and faraway from the field erectile dysfunction prevalence kamagra oral jelly 100mg without a prescription, operative exposure is at all times positively affected erectile dysfunction medications causes symptoms order 100mg kamagra oral jelly with mastercard. The descending or cervical branch of the uterine artery is left intact if potential. If this department is clamped with the larger ascending branch, no issue relative to vascular supply to the cervix is encountered as a outcome of anastomotic branches of the vaginal artery present ample collateral circulation. Typically, the uterosacral and cardinal ligaments are intact; therefore no suspension is required. On completion of cervical closure, the wound is irrigated to examine for bleeding factors. I advocate, earlier than the top of the cervical stump is sutured, that the surgeon cut a thin disc from the uncovered cervix at the level of separation from the body of the uterus to ensure that no functioning endometrium remains. The intra-abdominal portion of the cervix is closed by a row of interrupted simple or figure-of-8 sutures. In this occasion, the utero-ovarian ligament and the oviduct are triply clamped close to the uterine fundus. The incision is made with scissors or knife between the clamp closest to the uterus and the second clamp. Transfixing suture ligatures of zero Vicryl are positioned behind the third (most distant from the uterus) and second clamps. On the left facet, three clamps have been positioned throughout the tube and utero-ovarian ligament. Although it bears an ingrained designation as minimally invasive, it clearly is invasive and falls into the class for a significant operation. Nevertheless the laparoscopic route and approach have certain advantages and drawbacks. The pure postoperative course or pathway might be certainly one of expected every day improvement. Limitation of angles to manipulate tissues, especially when adhesions are encountered 2. User issue in suturing tissues and limitations to needle size, thus resulting in a dependence on "crutches" for hemostasis. Injury threat peculiar to the laparoscopic approach above and past the actual operation; principally, the need of placing a trocar device into the belly cavity However when all features of route, advantages, and disadvantages are put apart, the operation of hysterectomy by laparotomy versus laparoscopy is in fact or at least should be roughly equivalent in approach. The peritoneum that mirrored off the dome of the urinary bladder onto the anterior floor of the uterus is dissected from the uterus. Next the posterior sheath of the broad ligament is opened, and a choice is required whether to retain or remove the ovaries. The bladder at this juncture may require further dissection to free it from the anterior wall of the vagina. Finally, the vagina is opened, and any vessels bleeding from the vaginal cuff are coagulated. If the surgeon has mastered laparoscopic suturing abilities the vaginal cuff is closed by suturing via the laparoscopic strategy. During the description of this operation, reference has been made to coagulation and slicing. The devices used within the operation pictured have been electrosurgical bipolar devices. Alternative tools could presumably be monopolar electrosurgical, harmonic scalpel, or laser gadgets. The left round ligament, tube, and utero-ovarian ligament have been coagulated and reduce. Another view of the utero-ovarian ligament being severed after intensive coagulation. The uterus has been completely freed, and the manipulating gadget within the vagina creates the bulge seen here. The expanse of the vagina is now in view; notice the anterior side of the cut vaginal cuff. The needle is viewed because it has been passed through the anterior and posterior vaginal cuff. In fact, radical hysterectomy and lymphadenectomy are workouts in anatomic dissection. Radical Hysterectomy and Pelvic Lymphadenectomy Radical hysterectomy and pelvic lymphadenectomy differ from easy stomach hysterectomy in two major aspects. This requires the ureter to be dissected free for its entire course throughout the pelvis to the purpose where the ureter enters the bladder. In addition, the bladder and the rectum should be separated from the vagina for a distance of 2 to 5 cm under the level of the cervicovaginal junction. Second, the tissues containing fat and lymph nodes are dissected and excised from the exterior iliac vessels, the obturator fossa, the interior iliac vessels, and the common iliac vessels to the extent of the aorta. On occasion, the nodal dissection might expand upward around the aorta to the level of the renal arteries. As with easy belly hysterectomy (described in Chapter 11), the round ligaments are clamped and divided, and a bladder flap is developed on either side. At this point, the peritoneum on the lateral aspect of the broad ligament is dissected further laterally to expose the psoas major muscle. Great care have to be taken to not tear or otherwise injure the tributaries of the internal iliac veins as a outcome of they bleed profusely and are very tough to safe. Next, the ureter is dissected inferiorly, with the encircling fibrofatty tissue removed and medially mirrored to be removed with the uterus. The uterine arteries and veins are clamped far laterally, simply distal to their origin from the anterior division of the hypogastric artery. The peritoneum between the uterosacral ligaments is divided and the rectouterine space is developed and dissected downward beneath the cervix. The scissors point to the stomach of the psoas main muscle, which is lateral to the external iliac artery. The external iliac artery has now been uncovered and lies above the unfold ideas of the scissors. The large vessels within the retroperitoneal house are properly visualized on this photograph. Removal of some fats and lymph nodes partially exposes the obturator nerve (white) and the obturator artery (pink). The tip of the scissors is simply beneath the junction of the hypogastric and external iliac veins. The lymph node´┐Żbearing fats is being dissected from the obturator fossa with the clamp.
Purchase kamagra oral jelly 100 mg free shippingBoth the afferent limb (which drains upstream pancreatobiliary secretions) and efferent limb (which permits meals and secretions to flow downstream) are visible here erectile dysfunction zinc deficiency 100mg kamagra oral jelly otc. Mallory´┐ŻWeiss tear in a 27-year-old man who introduced with emesis adopted by hematemesis erectile dysfunction pump order kamagra oral jelly 100 mg with amex. Mallory´┐ŻWeiss tears are longitudinal intramural mucosal lacerations occurring in the distal esophagus and proximal stomach erectile dysfunction sample pills buy kamagra oral jelly 100 mg mastercard. Biopsies revealed edematous gastric mucosa with foveolar hyperplasia and no evidence of malignancy confirming Menetrier disease; nevertheless impotence vacuum device buy 100mg kamagra oral jelly otc, years later he developed gastric leiomyosarcoma. A Dieulafoy lesion is an uncommon cause of upper gastrointestinal bleeding, ensuing from an aberrant dilated submucosal artery eroding via the mucosa within the absence of a major ulcer. These lesions could require repeated remedies with argon plasma coagulation or electrocautery to stop recurrent gastrointestinal bleeding. Endoscopic look of portal hypertensive gastropathy in a 55-year-old man with cirrhosis. Ectopic pancreatic tissue within the gastric antrum with characteristic apical dimpling. In this patient, markedly enlarged gastric folds in the cardia symbolize gastric varices. Endoscopic ultrasound can verify the presence of varices if the diagnosis is in question. This patient presented with bleeding, and hematin (altered blood) may be seen adjoining to the angioectasia. The adherent clot is an endoscopic finding related to an elevated risk of rebleeding. Biopsies from this ulcer revealed a signet ring cell adenocarcinoma with ulceration and candidal overgrowth. Multiple 3-mm to 15-mm sessile fundic gland-type polyps were found in the gastric body. No polyps were seen after a year follow-up with use of an H2 receptor blocker for gastroesophageal reflux illness symptoms. These small sessile polyps distributed in the body and fundus in a patient with a historical past of proton pump inhibitor therapy are characteristic of fundic gland polyps. A giant fungating and submucosal noncircumferential mass was found within the cardia on this affected person with a quantity of endocrine neoplasia type 1. An ulcerated mass in the antrum of the stomach seen right here in an 84-year-old Korean girl with iron deficiency anemia. Glomus tumors are benign lesions originating from the modified smooth muscle cells of the glomus body and are not often seen within the abdomen. These submucosal lesions could current with overlying mucosal ulceration, as seen here. The first portion of the duodenum, simply after the pylorus, is referred to because the duodenal bulb. A large duodenal diverticular cavity could be seen in the lower left side of the image. A duodenal ulcer with a pulsatile seen vessel was discovered within the duodenal bulb in a affected person who presented with melena. The white papules arising from the duodenal mucosa symbolize lymph in dilated lacteals in the mucosa. Endoscopic view of a big periampullary mass with clear yellow bile draining from the central portion of the lesion. Duodenal mucosa within the bulb with a scalloped mosaic look in a affected person with celiac disease. This patient had a excessive titer of antiendomysial and tissue transglutaminase antibodies. Small bowel biopsies confirmed villous blunting, crypt hyperplasia, and markedly increased intraepithelial lymphocytes. A large fungating pigmented mass with minimal bleeding may be seen right here involving the second portion of the duodenum. This patient had a history of kidney transplant and biopsies confirmed a diffuse massive B-cell lymphoma. Capsule endoscopy includes ingestion of a capsule-sized gadget that obtains photographs of the gastrointestinal tract and transmits data to a recorder worn by patients through the examine. This picture reveals the everyday look of the conventional small bowel folds and villi. Capsule endoscopy in a patient with celiac illness reveals scalloping of the small intestinal mucosa. Capsule endoscopy may be indicated in some sufferers with obscure gastrointestinal bleeding. The duodenum is essentially the most proximal and shortest segment of the small bowel, with a mean size of 25 cm. It consists of the duodenal bulb and the second, third, and fourth parts, and it extends up to the ligament of Treitz. The proximal 40% of this portion is the jejunum and the remaining distal 60% is the ileum. The luminal floor of the small bowel has quite a few folds referred to as the plicae circulares. The plicae are most outstanding within the proximal small bowel, and reduce in number distally. Historically, suspected small bowel illness was categorised as proximal and distal to the ligament of Treitz. Since the introduction of capsule endoscopy and deep enteroscopy, the small bowel is now divided into three segments: the higher tract proximal to the ligament of Treitz, the decrease tract distal to the ileocecal valve, and the midgut, which refers to the portion of the small bowel located between the ampulla and the ileocecal valve that can be identified more definitively using these new imaging strategies. The complete small bowel can now be visualized in a noninvasive manner using capsule endoscopy. Therapeutic management of small bowel lesions is now potential with deep enteroscopy methods, together with balloon-assisted and spiral enteroscopy. Each of those gadgets has unique advantages and disadvantages that ought to be taken into consideration throughout number of the suitable modality. As a result, capsule endoscopy and deep enteroscopy techniques are often complementary and utilized collectively in the evaluation of suspected small bowel issues. Literature evaluate and recommendations for clinical utility of small-bowel capsule endoscopy, primarily based on a panel dialogue by international experts: consensus statements for small-bowel capsule endoscopy, 2006/2007. The Agile Patency System (Given Imaging Ltd, Yoqneam, Israel) contains a radiofrequency identification tag lined with a dissolvable physique of lactose and barium with a timer plug at both finish. This 54-year-old girl had an elevated immunoglobin A tissue transglutaminase antibody titer of seventy five U/mL. A polypoid hemangioma was additionally discovered in the 61-year-old patient with hematochezia in whom capsule endoscopy beforehand confirmed a polypoid lesion with lively bleeding within the midjejunum. Upper endoscopy and colonoscopy have been normal, but capsule endoscopy confirmed a quantity of angioectasias within the proximal small bowel. This 72-year-old lady with a historical past of alcoholic cirrhosis introduced with maroon stools.
Buy kamagra oral jelly 100mg visaA metastasis positioned within the cerebellum has been perceived as an isolated unfavorable prognostic marker for survival (Wronski and Arbit erectile dysfunction email newsletter discount 100mg kamagra oral jelly with visa, 1999 erectile dysfunction vacuum device order 100mg kamagra oral jelly overnight delivery, 2000) erectile dysfunction on prozac discount 100 mg kamagra oral jelly fast delivery. In common yohimbine treatment erectile dysfunction cheap kamagra oral jelly 100 mg amex, infratentorial tumors are considered extra life-threatening than supratentorial ones, as tumors within the confined space of the posterior fossa may find yourself in hydrocephalus, brainstem compression, and tonsillar herniation (Fadul et al. Gradual onset headache, nausea, and gait instability are the most typical presenting symptoms, but some sufferers may deteriorate rapidly, requiring instant neurosurgery to stop a neurological reason for dying (Fadul et al. The data had been restricted to one well being heart, thereby reducing the possible confounding impact of variations within the entry to well being care providers between well being centers and avoiding the selection bias inherently current in giant multicenter research. Furthermore, the info were prospectively registered and included all craniotomies performed for a histologically verifiable brain tumor, leaving no selection bias. The study is contemporary, thereby reflecting present neurosurgical follow and was I. From January 2003 until January 2011, primary surgical procedure for parenchymal supratentorial and cerebellar metastases was performed 627 times. Among these, surgery for cerebellar metastases was undertaken in one hundred forty patients (22% of total), constituting the first study inhabitants. Vital standing (deceased/alive) and time of death had been retrieved from the Norwegian inhabitants registry (Folkeregisteret) at October 15, 2012, hence all sufferers have been noticed for at least 9. Median overall survival was calculated from the time of surgery until the time of death. Statistics To visualize the relative propensity of various main cancer varieties to metastasize to the brain, we retrieved the typical annual incidence of every major most cancers type for the south-eastern population of Norway between 2003 and 2011 from the Norwegian Cancer Registry. For each main most cancers type, the number of patients present process surgery for a cerebellar metastasis was divided by the incidence of that specific main most cancers kind in our catchment space population within the examine interval. For comparability, this calculation was additionally made for all of the supratentorial metastases operated within the similar time period. In order to consider whether or not metastases from totally different major most cancers varieties were significantly over- or underrepresented within the cerebellum, we calculated if the proportion of cerebellar metastases have been significantly totally different from the general proportion of cerebellar metastases present process surgery at our division (140/627 = zero. Origin of Primary Tumor the origin and histology of a primary tumor are necessary predictors of the incidence and sample of intracranial metastasis (Suki, 2004). By retrieving the incidence of main tumors from the Norwegian Cancer Registry, we had been able to show that the danger of present process craniotomy for a mind metastasis was highest (>1%) for melanomas and lung cancers, in contrary to a particularly low danger (<0. However, it is essential to notice that brain metastases from sure main tumor sites, corresponding to testicular cancer and hematologic malignancies, are systematically excluded from surgical collection as they primarily are enrolled for different therapy modalities. This proportion is greater than the anticipated 15% based mostly on the regional blood move to and tissue volume of the cerebellum (Gavrilovic and Posner, 2005), which could be defined by a more aggressive surgical strategy toward cerebellar lesions to prevent potential life-threatening problems. Incidence of Cerebellar Malignant Melanomas Metastases Malignant melanomas have the best propensity for present process craniotomy for a mind metastasis (Rogne et al. Nevertheless, we observed that cerebellar melanoma metastases were exceedingly uncommon. A larger cohort was subsequently constructed to consider whether these observations were random, or a sample of metastasis for melanomas (Rogne et al. We have confirmed that melanoma metastases had been considerably underrepresented in the cerebellum (5%) compared to the general proportion of cerebellar metastases surgically resected (22%) at our division (P < zero. Our findings are statistically well-founded, as we included 140 instances and the pattern size wanted was 23 for a power of zero. To further substantiate our findings, we conducted a post hoc one-sample take a look at of proportion to verify that the proportion of cerebellar melanoma metastases also was significantly underrepresented in comparability with 15%, the general anticipated share in accordance to regional blood flow (Gavrilovic and Posner, 2005). Currently, the mechanism driving this attainable predilection is unknown, and addressing potential biological interactions based on up to date molecular biology lies past the scope of this surgical thesis. The interpretation of our findings could also be challenged by the inherent selection bias of sufferers to surgical intervention. Patients with multiple tumors, poor performance standing and superior systemic disease with a limited life expectancy are most probably not thought of surgical candidates and referred to different remedy modalities. We contemplate our findings strong, as the share of cerebellar melanoma metastases is low (5%), the total pattern measurement is massive (n = 140) and similar observations can be present in prior literature to assist our claim. It is, nonetheless, only an estimate of the relative biologic propensity of melanomas to metastasize to the supratentorial versus infratentorial compartment in surgical candidates. Incidence of Cerebellar Colorectal Cancer Metastases Colorectal cancers had an intermediate risk (0. For every main most cancers group, the figure illustrates if the metastases had been considerably over- or underrepresented in cerebellum compared to zero. Distribution of brain metastases as a outcome of blood provide and mechanical tumor cell arrest, was first proposed by Ewing in 1928 (Gavrilovic and Posner, 2005). An statement supportive of this speculation is that metastatic cells are seen to ideally embed in watershed areas and gray-white matter interfaces, areas where arterioles slim, leading to attainable mechanical entrapment of metastatic cells. Moreover, parenchymal mind metastases are reported to be positioned in the cerebellum in about 15%, cerebral hemispheres in 80%, and brain stem in 3´┐Ż5%, a distribution comparable to the regional blood move. Virtually any systemic cancer has the flexibility to metastasize to mind parenchyma, but the propensity for creating mind metastases varies significantly amongst totally different major cancer sorts (Suki, 2004). In absolute numbers, the most common main tumors giving rise to brain metastases are lung, breast, malignant melanoma, colorectal, and kidney cancer (Suki, 2004). The variable relative frequency of brain metastases from completely different primaries can in part be defined by the "seed and soil" hypothesis first proposed by Paget in 1887 (Paget, 1989). The concept of this speculation is that metastasis of cancers is dependent upon cross-talk between tumor cells ("seed") and particular host microenvironment ("soil") (Fidler, 2003). In conclusion, both the mechanical and the "seed and soil" hypothesis may be of significance for the distribution of brain metastases (Gavrilovic and Posner, 2005). In our neurosurgical practice, mind metastases had been located in the cerebellum in 22% of cases. This is larger than the anticipated 15% of circumstances and might replicate a extra aggressive neurosurgical strategy toward these lesions, as tumor location in posterior fossa is thought to represent a better danger of creating hydrocephalus, brain stem compression, and herniation than a supratentorial counterpart (Fadul et al. Malignant Melanomas Up to 75% of melanoma sufferers with metastatic illness develop brain metastases (Hofmann et al. However, in our cohort, cerebellar melanoma metastases were uncommon with solely seven resected lesions, accounting for only 5% of all of the I. A one-sample check of proportions analysis conducted post hoc confirmed that the incidence of cerebellar melanoma metastases in our cohort was also significantly decrease than 15%, which is the expected total proportion of cerebellar metastases in accordance with regional blood flow. An apparent aversion of melanomas to metastasize to cerebellum can be observed in former published sequence, but has not been explicitly pointed out previously. In series exclusively reporting on cerebellar metastasis, melanomas have accounted for two. In series reporting solely on melanoma metastases however addressing completely different treatment modalities, I. In two sequence, melanomas were located both supra- and infratentorially in an extra 15´┐Ż30% of sufferers (Hofmann et al. Our surgical collection consists of a particular group of sufferers with mind metastases discovered eligible for surgical therapy. Patients with a number of intracranial metastases with superior systemic disease and a poor performance status are normally not provided surgery. As many sufferers with malignant melanoma present with multiple metastases, a surgical series may be topic to a negative selection bias. However, in the case of cerebellar melanomas, the choice bias might as properly be in favor of surgical procedure.

100 mg kamagra oral jelly free shippingA case of a 59-year-old man with historical past of orthotropic liver transplant sophisticated with a hepatic artery stenosis on the anastomosis bisoprolol causes erectile dysfunction cheap kamagra oral jelly 100mg with visa. An 80-year-old man with the history of episodic bleeding of the proper colon requiring blood transfusion and with present rebleeding erectile dysfunction doctor in atlanta cheap kamagra oral jelly 100mg fast delivery. A case of a 79-year-old lady with a history of chronic epigastric ache and weight loss erectile dysfunction pump on nhs cheap 100 mg kamagra oral jelly otc. A naked metal stent was deployed across the stenosis and a balloon dilatation of the stent was carried out erectile dysfunction morning wood order 100mg kamagra oral jelly with mastercard. This was a case of a 29-year-old man with a historical past of intravenous drug abuse and endocarditis. This was a case of a 56-year-old girl with superior liposarcoma who presented with subcutaneous belly edema and decrease extremity edema. Hepatic venogram displaying the classic "cobweb" look of chronically occluded hepatic veins. A combination of glide wire (not shown) and 5 Fr catheter (arrowhead) had been used to cross the stricture. Triangulation and fluoroscopy were then used to goal a posterior duct in the proper hepatic lobe with a 21-gauge trocar needle, through which a 0. A clamp was positioned left of the left vertebral body and projecting over the gastric bubble. Celiac trunk angiography reveals traditional three vessel branching sample of the celiac trunk including the common hepatic, left gastric and splenic arteries. In this case of blunt splenic pseudoaneurysms, arteriovenous fistulas and petechial hemorrhage may be seen within the splenic parenchyma. A forward directing catheter is positioned in an accessory hepatic vein and contrast is injected. Fluoroscopic images obtained immediately after a needle was passed from the hepatic vein, via the liver parenchyma and into the portal vein. This is frequently performed in sufferers present process a liver embolization process. Although some histological prognosis can be made without the assistance of the scientific or laboratory information, most significant data is obtained with a correct clinical´┐Żpathological correlation. Special stains, similar to Masson trichrome, reveal fibrosis or cirrhosis of the liver, a sign of a persistent course of. Other routine stains embody stains for iron, reticulin, and diastase-resistant periodic acid Schiff-positive materials. Granulomas of the liver require special stains for the etiological agent such as acid-fast organisms and fungi. Shikata or orcein stain identifies hepatitis B surface antigen in addition to copper-binding protein, metallothionein. Immunoperoxidase stains detect viral and nonviral protein in the biopsy material utilizing specific antibodies directed towards the proteins. Routine hematoxylin and eosin stained sections are probably the most useful tools in the analysis. Well-embedded (3-m) sections with good hematoxylin and eosin stain will present great mobile particulars of hepatocytes, similar to inclusions in the cytoplasm or the nuclei, in addition to options corresponding to fats, cholestasis, or dysplasia. Initial evaluation of the architecture is adopted by a more in-depth evaluation of the portal tract or the fibrous septa if cirrhosis is present. The portal tracts or the fibrous septa must also be examined under polarized mild for foreign materials within the macrophages, which is often seen in patients with a history of intravenous drug addiction. The parenchyma is examined for cord sinusoidal sample; regular one-cell thickness is altered in hepatocellular carcinoma to three to four or more cells that thicken the trabeculae. Parenchymal cytoplasmic inclusions similar to Mallory our bodies, mega-mitochondria, l-antitrypsin, or of ground-glass cytoplasmic appearance are recognized under greater magnifications within the evaluation process. Areas of hepatocytolysis typically seem as focal punched-out or spotty necrosis with an accumulation of Kupffer cells and lymphocytes, or as large areas of collapsed reticulin with loss of hepatocytes. Attention additionally must be paid to the sinusoidal lining cells, Ito cells, and the house of Disse. Amyloid can also be seen in this area, either as reticular or globular kind, and is demonstrated by Congo red stain. In addition to the histological diagnosis to affirm the clinical analysis, the liver biopsy has turn into a very important prognostic software to assess the responses to remedy of chronic viral hepatitis B and C. This quantitative measurement of necroinflammation and fibrosis either by Knodell or Ishak scoring Table ninety two. Standardization of the scoring has been helpful in studies that examine completely different treatment modalities. Its application for particular person circumstances additionally helps the clinician with patient follow-up and monitoring of different serological viral markers. Standard protocols of liver biopsies help verify the medical diagnoses from rejection to opportunistic infections. Post-liver transplantation management of sufferers is basically dependent on the liver biopsy interpretations at the facet of the other laboratory studies. With correct indications and carefully chosen technique, a needle biopsy of the liver is a useful software. Most typically, the biopsy offers the final prognosis when the pathology interpretation is made utilizing the combined expertise of the pathologist and the hepatologist. Periportalpiecemealnecrosis Absent Mild (focal, few portal areas) Mild/moderate (focal, most portal areas) Moderate (continuous around <50% of tracts or septa) Severe (continuous round >50% of tracts or septa) B. Confluentnecrosis Absent Focal confluent necrosis Zone three necrosis in some areas Zone three necrosis in most areas Zone three necrosis + occasional portal´┐Żcentral (P´┐ŻC) bridging Zone 3 necrosis + a number of P´┐ŻC bridging Panacinar or multiacinar necrosis C. Correlating endoscopic imaging with histopathological findings may be crucial in establishing appropriate clinical analysis. There is extensive squamous epithelial apoptosis such that the nuclei resemble specks of dust. This field shows distinguished intraepithelial lymphocytosis and necrotic squamous cells. This is a transient prevalence and disappears with continued remark, as shown in the best panel. Eosinophilic esophagitis can current with a similar appearance however the rings persist with air insufflation and are less tightly spaced apart (right panel). Esophageal narrowing and deep sinus tracts again noted (d), and on barium swallow, the barium pill becomes lodged within the proximal esophagus (e). This entails staining the gastrointestinal mucosa for higher endoscopic visualization, usually for the detection of malignant or premalignant lesions. In this image, the mass can be seen extending from the gastroesophageal junction in a retroflexed view. In this biopsy, the lesion has invaded the muscularis mucosae, seen as slender pink strips. A DiffQuik stain highlights the organisms, seen as curved bacilli in the gland at the center of the sector. Biopsy confirmed continual antral gastritis with marked intestinal metaplasia consistent with atrophic gastritis. In this affected person, a number of bleeding angioectasias can be seen within the gastric antrum.
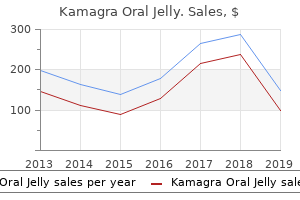
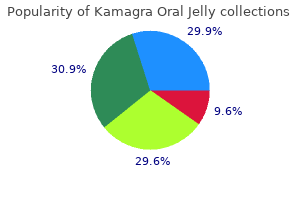
Flax (Flaxseed). Kamagra Oral Jelly. - Relieving mild menopausal symptoms.
- Dosing considerations for Flaxseed.
- Improving kidney function in people with lupus.
- Lowering cholesterol levels in people with high cholesterol.
- How does Flaxseed work?
- Osteoporosis.
- What is Flaxseed?
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96952
Purchase kamagra oral jelly 100 mg on lineBecause roughly 50% of cases are done in conjunction with a prolapse restore erectile dysfunction doctor in hyderabad cheap 100 mg kamagra oral jelly overnight delivery, all surgeons must erectile dysfunction causes alcohol buy cheap kamagra oral jelly 100mg line be well versed at tensioning strategies beneath general anesthesia erectile dysfunction vascular disease kamagra oral jelly 100mg with mastercard. The anterior vaginal wall is hydrodistended with a combination of lidocaine and epinephrine erectile dysfunction statistics canada discount 100mg kamagra oral jelly free shipping, with the goal of completely blanching the anterior vaginal wall at the stage of the mid to distal urethra. A scalpel blade is used to make an incision from slightly below the exterior urethral meatus to the extent of the mid urethra. The vaginal wall is sharply dissected with Metzenbaum scissors off the posterior urethra, creating small tunnels to the inferior pubic ramus. Some physicians favor to hydrodissect the trocar trajectory bilaterally earlier than passing the trocars through the use of a spinal needle, injecting fluid alongside the back of the pubic bone. A catheter information is positioned in the indwelling Foley catheter in order that the urethra and bladder neck may be displaced away from where the trocar is inserted. The trocar tip is inserted into the previously dissected tunnel on each side lateral to the urethra and superior to the undersurface of the pubic bone. The tip of the needle is fastidiously superior through the endopelvic fascia into the retropubic area. When the resistance of the endopelvic fascia is overcome and the tip of the needle is within the retropubic area, the handle of the trocar is dropped and the needle is advanced through the retropubic space as it hugs the back of the pubic bone. Cystoscopy is carried out with a 30- or 70-degree scope to evaluate the bladder for inadvertent trocar damage with the trocar in place. During repassing of the trocar, nice care ought to be taken to hug the again of the pubic bone. In such cases, the patient should proceed with the voiding trial postoperatively without the need for discharge with an indwelling catheter because the bladder perforation may be very small and is normally in a excessive, nondependent portion of the bladder. If extreme hematuria is current or the perforation is in the base or trigone of the bladder, continuous postoperative bladder drainage ought to be undertaken. The size of drainage should be decided on the idea of the type and extent of the bladder damage. As the ends of the mesh gadget are hooked up to the trocars on all sides, the mesh with its plastic sheath is pulled up by way of the suprapubic stab wound along the trocar trajectory. Some surgeons choose to perform the procedure underneath native anesthesia and use a cough stress test. In such situations the sling is tensioned to the purpose at which minimal leakage occurs during coughing. Regardless of tensioning approach, the last word endpoint is to create a laxity within the mesh manifested by a ricochet of the mesh again toward the urethra if pulled on vaginally with a right-angle clamp while additionally avoiding direct mesh contact with the underside of the urethra. After, the plastic sheaths covering the mesh are eliminated, and rigidity of the mesh is rechecked. The vaginal wound is copiously irrigated and closed with a operating 3-0 polyglycolic acid suture. The suprapubic stab wounds are closed with absorbable suture or liquid tissue adhesive. Vaginal packing may be inserted quickly on the completion of the case if the affected person is bleeding or concurrent prolapse procedures are being performed. The catheter may be removed together with the vaginal packing within the restoration room, and the affected person is discharged after confirming voiding effectivity. Mayo or Metzenbaum scissors are used to create a tunnel to the inferior pubic ramus. The tip of the needle is positioned within the small tunnel that has been created and will come into direct contact with the inferior pubic ramus, pointing toward the ipsilateral shoulder. With the index finger of the nondominant hand in the vagina and the thumb on the shaft of the needle, the tip is pushed through the urogenital diaphragm. Once the resistance of the urogenital diaphragm is overcome, the handle is dropped and the needle is moved in a medial and superior direction, whereas direct contact with the again of the pubic bone is maintained. The tip of the needle is then palpated suprapubically and is guided to exit via the previously created stab incision. Leakage of urine during a coughing stress test signifies the need for adjustment of the sling materials. Tunnels are created bilaterally to permit trocars to come into direct contact with the inferior pubic ramus. At the beforehand marked puncture websites within the suprapubic region, a stab incision is made on all sides. A trocar is inserted into the primary of the suprapubic incisions whereas aligning with the sagittal axis of the physique after which rigorously puncturing via the anterior rectus sheath. Angling caudally and "strolling off" the superior posterior fringe of the pubic bone, the trocar is advanced into the retropubic house sustaining shut contact with the posterior surface of the pubic bone. In a managed method, the trocar is progressively advanced till the tip is seen in the vaginal incision. The mesh is hooked up to the trocars, and the trocars are withdrawn via the suprapubic stab wounds. These slings are passed via a group of internal thigh muscular tissues, particularly the gracilis tendon, adductor brevis, and obturator externus. Both strategies involve specifically designed needles which are passed from the obturator area into the vagina or from the vagina into the obturator region. When handed from outside-in, the sling is directed from a small incision lateral to the clitoris at the inferior fringe of the adductor longus tendon, via the obturator foramen, around the ischiopubic ramus, and into the anterior vagina at the level of the midurethra. It passes so as via the following structures: gracilis tendon, adductor brevis muscle, obturator externus muscle, obturator membrane, and beneath or through the obturator internus muscle and periurethral endopelvic connective tissue; it finally exits into the opened vagina. In the approach used for the inside-out approach, the same buildings are handed via in the opposite direction. The adductor brevis muscle is displaced to reveal the location of the obturator externus muscle, the site of which lies instantly on the obturator membrane. The anatomic location of a transobturator suburethral sling is drawn on the cadaver. Average distance from the Monarch system to the obturator vessels in six fresh-frozen cadavers. Average distance from Monarch gadget to obturator nerves in six fresh-frozen cadavers. The clamp is pointing to the arcus tendineus fascia pelvis and the obturator internus muscle. This space has been opened as much as reveal the conventional anatomic location of a transobturator sling. It ought to remain deep to the arcus tendineus fascia pelvis and the obturator internus muscle. Appropriate positioning of the nondependent hand on the curvature of the needle in order that downward strain can be utilized to facilitate penetration of the needle via the obturator membrane. The needle has been handed by way of the obturator membrane around the ischiopubic ramus and is shown exiting into the lateral a half of the vaginal incision. The sling has been placed, and a right-angle clamp is used to stabilize the sling while the plastic sheath is eliminated.
Syndromes - You may be told to drink only clear liquids such as broth, clear juice, and water after noon.
- Ask that the provider who has spent the most time with your child be present during the procedure.
- Dialysis
- You have one of these cysts and develop a fever higher than 100.4 degrees Fahrenheit
- Moth repellant
- Be given medicines to thin your blood
- Name of product (as well as the ingredients and strength if known)
- A long, thin tube with a camera on the end is placed through this cut. This is called an arthroscope. The camera is attached to a video monitor in the operating room. This tool lets the surgeon to look inside your knee area and work on the joint.
- Time between periods changes each month
Purchase 100mg kamagra oral jelly otcA magnified view of D exhibits the multinucleated cell with viral inclusions (arrow) erectile dysfunction journal best 100 mg kamagra oral jelly. A high-power colposcopic view of the herpes simplex ulcers shown in C exhibits their sharp impotence by age discount 100mg kamagra oral jelly with amex, red define erectile dysfunction vacuum pump reviews order 100 mg kamagra oral jelly otc. A cytologic preparation obtained from a herpes ulcer shows a bizarre what std causes erectile dysfunction kamagra oral jelly 100 mg with visa, enlarged cell that has 4 nuclei. Massive development of condylomata acuminata occurs during being pregnant on account of immune compromise. The discovering of perianal warts virtually ensures that warts will be current within the anus. An anoscopic speculum, coupled with the colposcope, facilitates the diagnosis of rectal, or anal, warts. This strip of epithelium reveals acanthosis, parakeratosis, and extensive koilocytosis. The section was obtained from a biopsy specimen of the vulva of the affected person seen in G. It shows the traditional findings of condylomata acuminata, including papillomatosis, acanthosis, and hyperkeratosis or parakeratosis, as well as neoplastic mobile changes (left). This patient has a ragged ulcer, a swollen vulva, and unilateral enlargement of the groin lymph nodes. These flat, warty lesions are consistent with condylomata lata, or secondary syphilis. Multiple, nonindurated chancroid ulcers have to be differentiated from ulcers brought on by herpes simplex and syphilis. Chancroid ulcers trigger discomfort and could also be associated with inguinal lymphadenopathy. Multiple biopsies may be necessary to distinguish this condition from invasive carcinoma. A magnified view of D exhibits large cells that include red-staining Donovan our bodies (red dots). Lymphopathia venereum, or lymphogranuloma inguinale, causes painless vulvar ulcers. A giant ulcer is seen in the proper labium majus, and a smaller lesion is seen within the left labium majus. Lymphopathia venereum additionally causes enlarged inguinal lymph nodes that ulcerate and drain pus (buboes). The continual section is characterized by vulvar deformities that include fenestrations, elephantiasis, and systemic sequelae, corresponding to rectal strictures. Invasive squamous cell carcinoma of the vulva may coexist with lymphopathia venereum. Patients initially have pruritus that progresses to burning discomfort within the vestibule and is described as rawness, dryness, and irritation. Initially, pain is caused principally by coitus and its attendant rubbing on the hymenal ring. Traction on the Bartholin glands is the source of ache attributable to tight denims, pantyhose, wiping, or sexual intercourse. Contact dermatitis is related to chemical, drug, or cosmetic publicity and causes itching, irritation, and erythema. This abnormality was the outcomes of vaginal deodorant allergy, or contact vestibulitis. Other mucous glands inside the vestibule might show dysfunction that includes the paraurethral and Skene ducts. Light pressure with a cotton-tipped applicator produced a digital pain rating of 10/10. Vascular ectasia in the Bartholin duct area is a consistent finding in vulvar vestibulitis syndrome. The lesion was brought on by daily use of a sanitary pad due to vaginal discharge. G Lichenification Disorders the most typical lichen disorder of the vulva is lichen sclerosus, previously known as lichen sclerosus et atrophicus. When skin stretch is important to operate, the affected pores and skin splits, creating painful fissures. The reticular help buildings are broken, and the framework for repair is lost. Because this situation is so painful, nothing may be positioned into the vagina without eliciting a digital pain score of 10/10. Similar spotty lesions could additionally be seen in the mouth, particularly on the buccal mucosa. Microscopically, thick layers of keratin dominate the part and levels of acanthosis are seen. Areas of thickened, hyperkeratic pores and skin are interspersed with normal-appearing skin. Long-standing, poorly handled lichen sclerosus caused adhesions of the entire vulvar parts. The patient experienced leakage of urine because of urine pooling within the vagina. Several features of lichen sclerosus are seen: white plaques (lichenification); thin, atrophic pores and skin; and cigarette paper pores and skin modifications (wrinkling). As a result, she has scratched at her vulva, especially at night, and the scratching has brought on ulceration and a superficial bacterial an infection. A magnified view of F exhibits ulceration, fissure formation, and tearing of the inflamed, scarred tissue. Lichen sclerosus could contain the perineum and perianal skin, as well as the vestibule, labia, and clitoral and periclitoral tissues. The microscopic standards embody thinning and atrophy of the vulvar epidermis; fracture, or dishevelment of the basal cell layer; collagenation of the underlying dermis; and hyperkeratosis. In this affected person with erosive lichen planus, the surface dermis is thin or gone. A higher-magnification view of the vulva seen in B exhibits the sharp contrast between the erosion zone and the thin squamous zone of metaplasia. A microscopic part of lichen planus reveals thinning of the epidermis and an intense inflammatory response. The underlying papillary dermis and upper reticular dermis present an intense mononuclear inflammatory response. Extensive hyperkeratosis related to itching is characteristic of lichen simplex chronicus.
Order kamagra oral jelly 100 mg with mastercardClinical pharmacogenetics implementation consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing: 2013 replace erectile dysfunction young age treatment generic kamagra oral jelly 100 mg without a prescription. Traditional Chemotherapy ´┐Ż Renally modify for capecitabine (contraindicated if creatinine clearance 30 mL/min) Are there drug interactions with any of the fluoropyrimidine analogues Traditional Chemotherapy What are the widespread dose ranges for each deoxycytidine analogue Traditional Chemotherapy What is the emetogenicity degree of the deoxycytidine analogues Target/ disease class -tu- erectile dysfunction otc purchase 100 mg kamagra oral jelly overnight delivery, -t- = tumor -so- erectile dysfunction treatment psychological discount 100mg kamagra oral jelly mastercard, -s- = bone -gro- erectile dysfunction caused by nicotine order kamagra oral jelly 100mg amex, -gr- = development issue 3. Antibody source -o- = mouse (100% foreign) -li-, -l- = immunomodulator -ci-, -c- = circulatory system -tox-, -toxa- = toxin -xi- = chimeric (~75% human/~25% foreign) -ki-, -k- = interleukins -vi-, -v- = antiviral -fu-, -f- = fungus -zu- = humanized (~95% human/~5% foreign) -u- = human = absolutely human (100% human) -ne-, -n- = neurons as goal -ba-, -b- = bacterial four. Next-Generation Antineoplastics What are the most common antagonistic results of ziv-aflibercept This prevents tyrosine kinase autophosphorylation and phosphorylation of downstream signaling pathways that promote leukemogenesis. Ponatinib is structurally designed to include a carbon-carbon triple bond linkage to keep away from steric hindrance from the isoleucine residue, making it the only agent with activity in opposition to the T315I mutation. Tyrosine kinase inhibitors act intracellularly to inhibit tyrosine kinase signaling. The B-cell receptor is activated by both antigen-dependent and antigenindependent signaling. As a end result, many cellular processes occur such as proliferation, motility, homing, adhesion, chemotaxis, and survival. Use caution when coadministering ibrutinib with substrates of P-gp with a narrow therapeutic index (eg, digoxin) eight. Normal cells have intact homologous recombination; nonetheless, a subset of tumor cells are deficient in homologous recombination. Next-Generation Antineoplastics ´┐Ż Crizotinib, ceritinib, lapatinib, and vismodegib are P-gp substrates; crizotinib and lapatinib are inhibitors of P-gp. Crizotinib, ceritinib, lapatinib, vismodegib, palbociclib, and sonidegib concentrations could be reduced with the coadministration of antacids What are the most typical adverse results of every agent Proteasome inhibitors result in the accumulation of ubiquitinated protein aggregates, which contribute to cell demise. Next-Generation Antineoplastics pegylation of pegaspargase is also thought to reduce immunogenicity compared to the historic, non-pegylated, E. Because of hepatotoxicity with asparaginase, warning is warranted in these with preexisting liver dysfunction. The precise value is controversial; nevertheless, targeting nadir serum asparaginase exercise ranges of 0. Next-Generation Antineoplastics What is the emetogenicity stage of the asparaginase enzymes Consider plastic surgery skilled session relying on severity and agent extravasated Specific Extravasation Interventions 1. Administer subcutaneously with a small needle (eg, 25 gauge), distributing dose around the perimeter of the extravasation site in four or more equal injections, pointing the medicine inward toward the center of the extravasated web site ii. Dose: 10% answer, 4 mL diluted with 6 mL sterile water; 2 mL of a solution for: i. The strongest predictive options of cardiac ache are an affiliation with exercise and radiation to the shoulders or arms. Pericardial ache is exacerbated by inspiration (like pleuritic chest pain) and could additionally be relieved by sitting upright or leaning ahead. Timing and frequency of episodes: ask about precipitating elements (exercise, stress, caffeine consumption, smoking and alcohol) or any methods used to terminate palpitations. Association with palpitations, train or current alterations in drug prescription. Previous cardiac investigations such as echocardiograms, perfusion scans and angiograms. History of situations that are risk components for ischaemic coronary heart illness such as diabetes, hypertension and hypercholesterolaemia. A history of abdomen ulcers or extreme gastritis could require warning in the use of anti-platelet medications, particularly aspirin. Consider the possible cardio-toxic profile of certain medications: ´┐Ż Anti-neoplastic agents. Enquire about a household history of sudden cardiac dying, unexplained dying or cardiac defibrillator insertions which will suggest inherited channelopathies corresponding to Brugada syndrome or hypertrophic obstructive cardiomyopathy. Does the affected person appear breathless or cyanosed: verify use of oxygen (type of mask; percentage oxygen), is the patient propped up on pillows Capillary refill time: raise hand to the level of the guts, press for 5 seconds, launch and depend time to refill. Brachial or carotid pulse Volume ´┐Ż ´┐Ż ´┐Ż ´┐Ż ´┐Ż ´┐Ż ´┐Ż Variation in pulse volume and blood stress is seen with respiration (increases in expiration and decreases in inspiration as a result of an increase and fall in intrathoracic pressure, respectively). Low quantity pulse is caused by hypovolaemia, peripheral vascular illness or a decreased pulse pressure as occurs in mitral and aortic stenosis. Hyperdynamic pulse is a large-volume bounding pulse seen in anaemia, sepsis, thyrotoxicosis and being pregnant. Slow-rising pulse (pulsus parvus et tardus) is a pulse growing gradually in quantity that occurs with aortic stenosis. Bisferiens pulse is a slow-rising pulse with two systolic peaks, felt in aortic stenosis combined with aortic regurgitation. Pulsus alternans alternates between normal and low volume and happens in circumstances such as mitral or aortic valve stenosis, severe ventricular failure or effusive pericarditis. Collapsing pulse (water hammer) has an early peak with a speedy lower in quantity that could be exaggerated by elevating the arm above the extent of the center (occurs in severe aortic regurgitation). Palpate the chest for heaves parasternally (right ventricular hypertrophy), heaves at the apex (left ventricular hypertrophy) and thrills (palpable murmurs). Pericardial rub is a harsh sound heard in pericarditis ´┐Ż characteristically scratchy and heard each in systole and diastole. Volume change ´┐Ż ´┐Ż ´┐Ż ´┐Ż ´┐Ż ´┐Ż ´┐Ż Systemic and pulmonary hypertension enhance the quantity of the aortic and pulmonary coronary heart S2 sounds, respectively (often termed a loud A2 and a loud P2, respectively). A calcific or motionless valve may shut quietly or silently, while a click on could also be heard with a cell valve leaflet. Quiet heart sounds could occur in the presence of a reduced cardiac output, pericardial effusion or emphysema. Delay in left ventricular emptying reverses the splitting of S2 so splitting occurs in expiration.
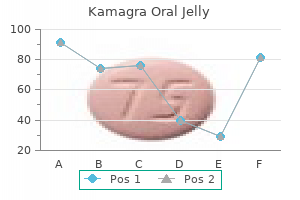
Kamagra Oral Jelly: 100 mg
Order kamagra oral jelly 100mg with mastercardAt the same time erectile dysfunction at 17 order 100 mg kamagra oral jelly with visa, the vaginal inlet has been reshaped and widened to allow two finger widths (2 erectile dysfunction 16 years old cheap kamagra oral jelly 100mg visa. The medical area is dominated above (superiorly) by the vestibular bulb and the vaginal wall sinuses erectile dysfunction yoga exercises buy kamagra oral jelly 100mg online. The lateral house accommodates a couple of small arteries and veins impotence pregnancy kamagra oral jelly 100 mg without a prescription, but principally fatty tissue. A doubly gloved finger is placed in the anus to confirm its location relative to the operative subject, as nicely as its integrity. This drawing illustrates the topographic anatomy of the vestibule and Bartholin glands/ducts. Noteworthy is the relationship of the anus to the posterior side of the vestibule and lower vagina. A deep dissection of the vestibule (left) and a superficial dissection (right) are proven here. The vessel enters the perineum with the pudendal nerve medial to the ischial tuberosity. The bulbocavernosus muscle overlies the Bartholin gland; lateral to the gland is the fats of the labium majus and ischiorectal fossa. Preoperative view of the vestibule in a girl afflicted with vulvar vestibulitis syndrome. Note the erythema across the Bartholin ducts, as well as the vascular ectasia (punctation). Via a tightly targeted laser beam, the dots are related and a deeper incision is accomplished (C) with Stevens scissors. The labia are sutured again for retraction and steady exposure of the vestibule. A 2-cm bloodless incision is made immediately lateral to and above and below the right Bartholin duct opening. A mosquito clamp dissects the house between the bulb, Bartholin gland, and inside wall of the vagina. This house is dissected into the fats of the labium majus and the ischiorectal fossa. The lateral fringe of the incision is pulled with an Allis clamp to provide publicity. The Bartholin gland is cut free from the encircling tissue with Stevens scissors. The lower vagina, hymen, and medial side of the vestibule are excised with a sharp scalpel. The lateral side of the vestibule (abutting Continued the labium majus) is excised. The excised vestibular tissue is distributed to the pathology laboratory in a separate container from that used for the excised Bartholin gland. Therefore specs for therapy required excision to a depth of 1 to 3 mm for labia majora and perineal and perianal pores and skin; a depth of not extra than 1 mm for the labia minora and periclitoral pores and skin; and a peripheral margin of three. A primary tenet for surgical remedy of the vulva is limitation of deep tissue devitalization by power units. After the excision is completed, adequate time and effort must be expended to get hold of vigorous hemostasis. When the latter is accomplished, the operative web site is irrigated with normal warm saline. If the skin is tightly stretched to acquire closure, the edges might bear necrosis and separate. Alternatively, wounds that are closed underneath pressure are weak to suture tear-out when inevitable postoperative tissue edema develops. The precept of the pedicle graft involves preservation of a plentiful blood supply to the graft. Therefore the surgeon must know the supply and path of the blood vessels to avoid cross-cutting them. Second, the length of the graft must be approximately onehalf the width of the base. Finally, a split-thickness graft from the thigh or buttock may be obtained preoperatively after which grafted onto the wound. In actuality, that is the preferred method of remedy for big defect protection. When a large, deep resection or earlier iatrogenic scar formation has compromised the blood provide and created large tissue loss in the vulva or vagina, a myocutaneous graft must be thought of. This type of graft supplies tissue substance, in addition to a blood supply to the graft. The interlabial sulcus pores and skin and the skin at the lateral margin of the labium majus have been approximated with out excessive tension on the suture line. On the working table, the extent of the realm to be resected is sketched with a sterile marking pen. The correct depth of excision is maintained by the operator by stretching the skin inferiorly and pushing up on the skin with the index finger on the line of resection. Only a portion of the best labium minus (including the clitoris and its hood) stays. The pores and skin is carefully defatted, moistened, and held in a sterile sponge until its use is required. A split-thickness graft was utilized to the proper side, whereas a pedicle graft was needed on the left. The graft shall be cut and freed from the underlying fats and rotated posteriorly (inferiorly) and medially. Xeroform gauze is applied to the graft, and that is adopted by the applying of a stress dressing. The muscle, along with the overlying pores and skin and subcutaneous tissue, constitutes the pedicle graft. This graft is rotated and delivered through a tunnel through the thigh to the labial area. The graft is then sutured into place after testing for the adequacy of blood circulate (using Doppler sonography). The left wall of the vagina and the perineum have been changed and repaired with a gracilis myocutaneous flap. For acquiring a tissue specimen, laser excision is preferable to ablative strategies. Ocean) twice every day and to apply silver sulfadiazine (Silvadene) cream to the wound site 3 instances per day. The laser locations multiple impression spots, a lot in the method of marking the lesion with a pen. Laser energy is turned up to 30 to forty W, and the complete zone is vaporized to a uniform 2-mm depth (note that vaporization between zero. Laser Excision by Thin Section the laser "thin part" has three advantages: It (1) requires neither closure nor grafting, (2) heals quickly without gross scar formation, and (3) supplies a specimen for pathologic examination. Next, laser energy is elevated to 15 to 20 W, and, with a tightly centered beam, a aircraft is created parallel to the floor of the skin.
References - Dogra PN, Nabi G: Laser welding of vesicovaginal fistula, Int Urogynecol J Pelvic Floor Dysfunct 12(1):69n70, 2001.
- Madsen BL, Noer HH. Simultaneous rupture of both peroneal tendons after corticosteroid injection: operative treatment. Injury .1999;30(4):299- 300.
- Spinetta JJ, Swarner JA, Sheposh JP. Effective parental coping following the death of a child from cancer. J Pediatr Psychol. 1981;6:251-63.
- Poppas DP, Uzzo RG, Britanisky RG, et al: Laparoscopic laser assisted autoaugmentation of the pediatric neurogenic bladder: early experience with urodynamic followup, J Urol 155(3):1057-1060, 1996.
- Polascik TJ, Amin MB: Surveillance after focal therapy. In Sanchez-Salas R, Desai M, editors: Image-guided therapy in urology. SIU-ICUD Joint Consultations, Melbourne, Australia, 2015, Societe Internationale diUrologie;. Polascik TJ, Mayes JM, Schroeck FR, et al: Patient selection for hemiablative focal therapy of prostate cancer: variables predictive of tumor unilaterality based upon radical prostatectomy, Cancer 115(10):2104n2110, 2009.
- Sheridan P, Blain R, Vezina D, Bleau G: Prospective evaluation of the safety of heparin reversal with protamine in vasectomized patients after cardiopulmonary bypass. In Proceedings of the 10th Annual Meeting of the Society of Cardiovascular Anesthesiologists, New Orleans, 1988, p 140.
- Francis GS, Tang WH, Sonnenblick EH: Pathophysiology of heart failure. In Furster V, Alexander RW, O'Rourke RA, et al: Hurst's the heart, ed 11 New York, 2004, McGraw-Hill, pp 697-722.
- Haimovici H, Steinman C, Karson IH: Evaluation of lumbar sympathectomy. Advanced occlusive arterial disease, Arch Surg 89:1089-1095, 1964.
|