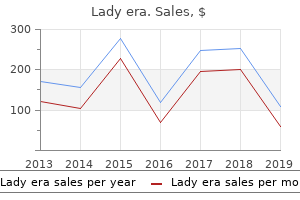
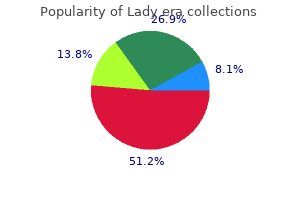
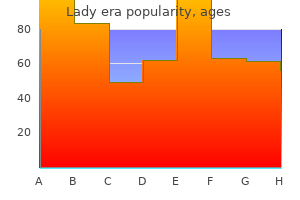
Lady era
Mark Stafford-Smith, MD, CM, FRCPC - Professor of Anesthesiology
- Director of Fellowship Education
- Director of Cardiothoracic Anesthesia and Critical Care
- Medicine Fellowship
- Division of Cardiothoracic Anesthesia and Critical Care Medicine
- Department of Anesthesiology
- Duke University Medical Center
- Durham, North Carolina
Cheap 100 mg lady era amexThe brachial plexus is the positioning of nearly all of intraoperative nerve injuries associated to the lateral position women's health clinic bendigo hospital proven lady era 100mg. Semiprone or semisupine repositioning after arm fixed to a help *Unfortunately menopause breast changes generic 100 mg lady era amex, this padding underneath the thorax is misnamed an "axillary roll" in some establishments menopause mood changes generic lady era 100mg visa. Dependent eye Dependent ear pinna Cervical backbone consistent with thoracic spine Dependent arm: (i) brachial plexus menstrual gas cramps quality lady era 100mg, (ii) circulation Nondependent arm*: (i) brachial plexus, (ii) circulation Dependent and nondependent suprascapular nerves Nondependent leg sciatic nerve Dependent leg: (i) peroneal nerve, (ii) circulation *Neurovascular accidents of the nondependent arm are extra likely to occur if the arm is suspended or held in an independently positioned arm rest. This two-point fixation, plus the intense mobility of neighboring skeletal and muscular structures, makes the brachial plexus extraordinarily liable to injury (Box fifty three. The affected person should be positioned with padding beneath the dependent thorax to keep the weight of the upper physique off the dependent arm brachial plexus. However, this padding will exacerbate the strain on the brachial plexus if it migrates superiorly into the axilla. Fortunately, the overwhelming majority of these nerve accidents resolve spontaneously over a interval of months. Anterior flexion of the arm at the shoulder (circumduction) throughout the chest or lateral flexion of the neck towards the alternative aspect may cause a traction damage of the suprascapular nerve. This malpositioning, which exacerbates brachial plexus traction, can cause a "whiplash" syndrome and may be tough to recognize from the head of the working desk, particularly after the surgical drapes have been placed. It is helpful for the anesthesiologist to survey the patient from the facet of the desk instantly after turning to make positive that the entire vertebral column is aligned properly. The dependent leg must be barely flexed with padding beneath the knee to protect the peroneal nerve lateral to the proximal head of the fibula. The nondependent leg is positioned in a neutral prolonged place and padding positioned between it and the dependent leg. Excessively tight strapping on the hip degree can compress the sciatic nerve of the nondependent leg. Other sites notably answerable for neurovascular harm within the lateral position are the dependent ear pinna and eye. A "head-to-toe" protocol to monitor for possible neurovascular accidents related to the lateral decubitus place is introduced in Box 53. These compliance changes are responsible for the ensuing differences in ventilation between the lungs that happen in the lateral place. Note: the compliance of the dependent lung is elevated when the nondependent hemithorax is open versus closed. Significant changes in air flow develop between the lungs when the affected person is positioned within the lateral place. Any factor that modifications the mechanics of both of these springs places the lung on a different compliance curve. Once the patient is anesthetized and paralyzed, the air flow of the dependent lung will then decrease 15%. These adjustments depend on the method used for ventilation in the particular person affected person. Thus the end-expiratory volume of each lung is immediately a function of the time allowed for expiration. The compliance of the entire respiratory system increases significantly as soon as the nondependent hemithorax is open. This atelectasis shall be evenly distributed within the dependent parts of both lungs. In the lateral place, the blood flow to the dependent lung is usually thought to be elevated by 10% in comparison with the same lung in the supine position. Pulmonary arteriovenous shunt during common anesthesia will normally enhance from roughly 5% in the supine position to 10% to 15% within the lateral position. First, paradoxical air flow (also known as "pendelluft") in which gasoline moves into the open-chest lung from the intact lung during expiration and then reverses circulate throughout inspiration. And second, because of the swinging movement of the mediastinum between the hemithoraces during the respiratory cycle, which interferes with cardiac preload and causes hemodynamic instability. In the early 1900s, a number of pioneers such as the New Orleans surgeon Matas advocated positivepressure air flow and a primitive form of endotracheal ventilation, which had been demonstrated to be safe in animal experiments, for thoracic anesthesia. Essentially any anesthetic method that gives protected and stable common anesthesia for main surgical procedure can and has been used for lung resection. Intravenous fluids are administered to substitute volume deficits and for upkeep solely during lung resection anesthesia. The poorly soluble nitrogen in the air/oxygen mixture delays collapse of the nonventilated lung. For intravenous induction of anesthesia, either propofol or ketamine may be expected to diminish bronchospasm. For maintenance of anesthesia, propofol and/or any of the risky anesthetics will diminish bronchial reactivity. This consideration shall be a important component in the selection of the anesthetic method for most thoracic sufferers. The anesthetic approach should optimize the myocardial oxygen supply/demand ratio by maintaining arterial oxygenation and diastolic blood pressure while avoiding unnecessary increases in cardiac output and coronary heart rate. Thoracic epidural anesthesia/analgesia might aid on this (see Postoperative Analgesia later). A saturation larger than or equal to 90% (PaO2 > 60 mm Hg) is usually accepted, and for temporary periods a saturation in the excessive 80%s may be acceptable in sufferers without vital comorbidity. However, the lowest acceptable saturation shall be higher in sufferers with organs at danger of hypoxia due to restricted regional blood flow. Reports for the interval between 1950 and 1980 describe an incidence of hypoxemia (arterial saturation < 90%) of 20% to 25%. The airway stress gradient between the ventilated and nonventilated thoraces tends to encourage blood circulate to the nonventilated lung. Surgery and cardiac output can have variable effects, either growing or lowering the proportional flow to the ventilated lung. The rapid-onset phase begins immediately and reaches a plateau by 20 to 30 minutes. This could contribute to increased desaturation in the course of the collapse of the second lung during bilateral thoracic procedures. Conversely, surgery can dramatically decrease blood flow to the nonventilated lung by deliberately or accidentally mechanically interfering with either the unilateral pulmonary arterial or venous blood flow. In a randomized examine evaluating sevoflurane to propofol for anesthesia in pulmonary resection, the sevoflurane group had significantly fewer postoperative pulmonary complications (14% vs. Increasing the cardiac output to supranormal levels by administering inotropes, similar to dopamine, tends to have an overall adverse effect on PaO2. As cardiac output falls under baseline, arteriovenous shunt (Qs/ Qt) falls, however the blended venous oxygen saturation (SvO2) also decreases, leading to a net fall in PaO2. Conversely, raising cardiac output above baseline tends to increase SvO2 but also enhance Qs/Qt and the net result again is a decrease in PaO2. It has been the practice of many anesthesiologists to use the same large tidal volume. And third, a ventilation sample that allows recurrent atelectasis and recruitment of lung parenchyma appears to be injurious. The Lower Inflection Point of the curve (functional residual capacity) was at 6 cm H2O.
Generic lady era 100 mg overnight deliveryDiuretics might go away patients in a chronically volume-contracted state that worsens anesthesia-related hypotension women's health center colorado discount lady era 100 mg online. Normalization of electrolytes is especially necessary in sufferers taking digoxin women's health clinic san antonio order 100 mg lady era with mastercard, in whom hypokalemia could potentiate digoxin toxicity pregnancy portraits lady era 100mg discount. The hypotension attributable to these should be handled appropriately by small doses of inotropes or vasopressors pregnancy 17 weeks discount lady era 100mg fast delivery, which can include vasopressin analogs. Patients with dialysis-dependent persistent kidney disease have multiple pathologic features that should be thought of in perioperative fluid remedy. Overall fluid stability may be disturbed by lowered or absent native urine production, with reliance on dialysis to achieve the target "dry" weight, representing estimated euvolemia. Organ O2 supply could also be impaired by varied components, including chronic anemia, endothelial dysfunction, and microvascular perfusion abnormalities. The frequent coexistence of coronary heart failure and systemic or pulmonary hypertension and the bleeding tendency caused by platelet dysfunction further enhance the perioperative threat. Surgery must be undertaken in a facility the place preoperative and postoperative dialysis or hemofiltration could be offered in case of intraoperative fluid overload or hyperkalemia. In elective surgery, preoperative dialysis should be timed such that the affected person enters the intraoperative part with a traditional blood quantity. Surgery in the presence of hypervolemia will increase the danger for pulmonary and peripheral edema, hypertension, and poor wound therapeutic, whereas hypovolemia will increase the danger for anesthesia-related hypotension and insufficient tissue perfusion. Practically, this implies performing dialysis the day earlier than surgery to enable for equilibration of fluid and electrolyte compartments and time for dialysis anticoagulants to be metabolized. Electrolytes should be checked on the morning of surgery; sampling too quickly after dialysis, before equilibration, could give an artificially low K+ result leading to pointless exogenous supplementation. Conversely, fasting may very well favor a hyperkalemic state because of the reduced presence of insulin; the perfect K+ value after dialysis is in the low-to-normal range. For emergency surgery, there will not be adequate time to safely dialyze patients preoperatively. In this case, electrolyte abnormalities must be managed conservatively, with explicit care paid to intraoperative fluid stability. The amount of fluid administered intraoperatively should be titrated to objective physiologic measurements, though the type of fluid given is open to debate. Large volumes of isotonic saline must be avoided, as a outcome of the induced acidosis favors extrusion of K+ from cells. Colloids could also be used for intravascular volume alternative, although owing to their predominantly renal excretion, the amount effect and potential toxicities could also be exaggerated in these sufferers. Liaising with the nephrologist is essential earlier than considering blood transfusion; if the patient is awaiting renal transplantation, human leukocyte antigen-matched blood may be required to reduce antibody formation and future difficulties with blood and tissue matching. Large volume gastric fluid loss could also be attributable to congenital or acquired gastric outlet obstruction and lead to a definite sample of fluid and acid-base abnormalities. However, progressive dehydration leads to elevated aldosterone secretion, geared toward retaining Na+ and water. Na+ is retained on the expense of K+ and H+ ions, leading to hypokalemia, and worsening metabolic alkalosis with a paradoxically acid urine. Correction ought to include gradual rehydration with isotonic saline and K+ supplementation, changing to dextrose-containing saline solutions depending on electrolyte analysis. Any surgical procedure required to treat gastric outlet obstruction must be scheduled after correction of the volume and acid-base standing. Patients with an infection and sepsis syndromes may be encountered early in their presentations, as surgical supply control of an infection (drainage of abscesses, debridement of necrotic tissues, removal of contaminated devices) forms a key a part of early sepsis remedy. Fluid resuscitation, with the goal of maintaining sufficient end organ perfusion, has traditionally been a key a half of the primary six hours of sepsis remedy, which may symbolize the perioperative period for some patients. This evaluation may incorporate more detailed measurements corresponding to cardiac output, along with routinely obtainable physiological variables (heart fee, blood pressure, urine output). These pointers are based on a limited proof base and additional research is needed to refine this space. For example, some trials have suggested that a fluid bolus technique may not be helpful achieve hemodynamic targets174 or might even be harmful in some settings. Here the focus of fluid remedy is the fantastic steadiness between avoiding an increase in lung edema while maintaining adequate tissue perfusion. The consequences are interstitial and alveolar edema, lowered pulmonary compliance, increased pulmonary artery pressures, and hypoxemia. Meanwhile, organ perfusion could also be impaired by increased intrathoracic pressures and decreased cardiac filling pressures. Extensive burns create a situation of copious fluid loss from the circulation mixed with specific sensitivity to the results of excess fluid administration. Thermal harm creates an space of necrotic tissue with surrounding ischemic areas. The mixture of lifeless tissue with areas undergoing ischemia and subsequent reperfusion causes localized and systemic inflammatory reactions via histamine, prostaglandin, reactive O2 species, and cytokine launch. Local impairment of endothelial barrier perform leads to the loss of oncotically active plasma constituents, elevated capillary filtration into the interstitial compartment, and evaporative transcutaneous fluid loss as a result of lack of pores and skin integrity. Through similar mechanisms, extensive burns may lead to the systemic inflammatory response syndrome, with its well-recognized effects on fluid compartments outlined beforehand. The deleterious position of this inflammatory response is underlined by the discount in mortality seen with early burn excision compared with conservative care. Fluid administration is basically nonetheless based mostly on formulas such as the Parkland formulation (Box forty seven. Although these have given a place to begin for resuscitation volumes based mostly on patient weight and extent of burn, myriad other affected person and pathologic components put such a recipe-based approach at odds with modern perioperative fluid remedy based on goal physiologic objectives. Although the approaches primarily based on these formulation advocate down-titration of administered fluid volumes if urine output is sufficient (0. Indeed, massive research have proven that the majority of burn patients receive fluid volumes in extra of these predicted by the Parkland formula, with a imply of 6 mL/kg/% burn in contrast with 4 mL/kg/% burn in 24 hours predicted by the method. As in all conditions typified by systemic inflammation, extra administered fluid will gather in compliant compartments. Pulmonary edema requiring ventilatory support, fasciotomies in muscle compartments, raised intraocular stress, and conversion of superficial to deep burns have been observed and attributed to fluid resuscitation. A mixture of crystalloids and colloids may be used to cut back the total fluid quantity administered,192 though the early use of colloids is controversial as a result of the perceived risk of extravasation of oncotically active molecules within the presence of extreme capillary leak. In addition, sufferers with burns have been included in current license restrictions on the use of starches. Perioperative fluid remedy in pediatric patients has for a couple of years been based mostly on traditional approaches that are increasingly being reexamined. Holliday and Segar138 proposed a quantity and composition of maintenance fluid in hospitalized children in 1957 based mostly on water necessities to sustain average metabolic activity and the electrolyte composition of milk. This developed into the 4-2-1 quantity calculation for upkeep fluid requirements aimed at replacing insensible and urinary losses with hypotonic crystalloids containing glucose to keep isoosmolality. These concepts had been translated into the perioperative part and glucose-based options were administered intraoperatively to cut back the apparently excessive risk for preoperative hypoglycemia after extended fasting,193 and postoperative maintenance fluids had been prescribed based on the 4-2-1 calculation using hypotonic crystalloids.
Syndromes - Within 24 hours of quitting: Your risk of a sudden heart attack goes down.
- Loss of ability to interact
- The sperm count varies from 20 to 150 million sperm per milliliter.
- Rectal pain while having a bowel movement (tenesmus)
- High serum osmolality
- Swelling of the cornea
- Avoid alcohol and sleep aids
- Get more exercise.
- In the Cotrel-Dubousset instrumentation (CDI), instruments are placed in each part of the spine that needs straightening. Your child may go home in about 5 days and may return to school in about 3 weeks.
- Delivery by c-section
Purchase 100 mg lady era with amexThe convention of onesixth unit of platelets outcomes from the frequent allocation of platelet merchandise in 1 unit (apheresis) from a single donor or 1 pool (pooled) from six donors in a "six pack menstruation 6 days early discount 100mg lady era visa. Holcomb and associates134 concluded that elevated platelet ratios were associated with improved survival after massive blood transfusions 1st menstrual period after pregnancy discount lady era 100 mg without a prescription. The first approach uses linear binding kinetics the women's health big book of yoga download 100mg lady era with amex, unlike the nonlinear binding of Hb menopause las vegas lady era 100mg cheap. A number of approaches have been used, together with crosslinking, pyridoxylation and polymerization, and conjugation and encapsulation to accomplish this. Natanson and colleagues146 performed a cumulative meta-analysis on sixteen trials involving 5 different merchandise and 3711 patients. An accompanying editorial concluded that a 30% increased threat for death and a threefold improve in the threat for myocardial infarction ought to preclude any extra research. Evidence of an infection and danger of bacteremia Scheduled surgical procedure to appropriate aortic stenosis Unstable angina Active seizure dysfunction Myocardial infarction or cerebrovascular accident inside 6 months of donation 6. Although the benefits and disadvantages vary with every method, autologous transfusion goals to decrease the incidence and severity of problems related to allogenic transfusions and preserve the provision of banked blood. Autologous blood can also be an acceptable resolution in patients with rare blood phenotypes or alloantibodies. Blood is collected in commonplace blood bags containing citrate anticoagulant and maintained at room temperature within the operating room for as much as 8 hours or at 4�C for twenty-four hours. However, as blood security has improved with a marked decrease in infectivity from allogeneic blood, the distinction in safety compared with autologous blood is far less. Not surprisingly, the proportion of autologous blood collected has considerably decreased since the peak in the mid-1990s. Repeated donations ought to be separated by every week with seventy two hours between the final donation and the time of surgical procedure. The latter suggestion is to guarantee restoration of intravascular volume and acceptable testing and preparation of the donated blood. Acute preoperative hemodilution in patients present process radical prostatectomy: a case study evaluation of efficacy. Another metaanalysis demonstrated related findings in a broader affected person inhabitants that included multiple surgical specialties, however the findings have been criticized because of the heterogeneity of the research included and the potential for publication bias, which might doubtless overestimate any true profit. These effects included the development of bronchoconstriction and acute lung damage as a end result of extravasation of fluid and deterioration of cardiopulmonary hemodynamics. It is a perioperative blood conservation method to reduce use of allogenic blood and the risks associated with allogeneic blood publicity. This approach ought to be discussed with such patients and acceptability must be decided on a case-by-case foundation. Patient is unwilling to settle for allogeneic blood however will consent to receive blood from intraoperative blood salvage. Blood from the surgical subject is collected in a reservoir till enough fluid accumulates for processing. Microaggregate filters (40 m) are most often employed during reinfusion as a result of recovered and processed blood might include tissue particles, small blood clots, or bone fragments. Some techniques are in a place to regularly course of blood and may present the equal of 12 units/h of banked blood to a massively bleeding patient. If collected under aseptic conditions with a saline-wash gadget and if correctly labeled, blood may be stored at room temperature for as much as four hours or at 1�C to 6�C for up to 24 hours, supplied storage at 1�C to 6�C is begun within four hours of ending the collection. Storage times are the same for recovered blood regardless of whether unwashed or washed. Collection methods that neither concentrate nor wash shed blood before reinfusion enhance the chance of opposed results. If not transfused immediately, items collected from a sterile operating subject and processed with a tool for intraoperative blood collection that washes with 0. At 1�C-6�C for as a lot as 24 h, supplied storage at 1�C-6�C is begun within four h of ending the gathering 2. Transfusion of blood collected intraoperatively by different means should start inside 6 h of initiating the gathering. If stored within the blood financial institution, the unit must be handled like any other autologous unit. The transfusion of shed blood collected underneath postoperative or posttraumatic circumstances should begin inside 6 h of initiating the collection. The high suction pressure and floor skimming throughout aspiration and the turbulence or mechanical compression that occurs in roller pumps and plastic tubing make some extent of hemolysis inevitable. Adverse reactions related to autologous blood transfusion: analysis and incidence at a big educational hospital. Many packages limit the amount of recovered blood that could be reinfused without processing. To reduce hemolysis, the vacuum degree should ordinarily not exceed one hundred fifty mm Hg, although larger ranges of suction could often be wanted during periods of speedy bleeding. One study discovered that vacuum settings as high as 300 mm Hg might be used, when necessary, with out inflicting excessive hemolysis. Other situations that will preclude use of cell savage include: use of parenterally incompatible chemicals. Intra-operative cell salvage: a recent look at the indications and contraindications. In some instances, the worth of blood salvage will not be by way of affected person consequence or discount of transfusion necessities, however instead in price financial savings. The value of intraoperative blood collection was recently demonstrated for high-risk cesarean surgeries however not for routine procedures. Recovered blood is dilute, is partially hemolyzed, and will contain excessive concentrations of cytokines. These exams had been designed to show dangerous antigen-antibody interactions in vitro so that harmful in vivo antigen-antibody interactions may be prevented. Donor blood used for emergency transfusion of type-specific blood must be screened for hemolytic anti-A and/or anti-B antibodies, and Rh antibodies. All approved blood banks have redundant processes in place to ensure that the affected person receives the right unit of blood. Most would require a second confirmatory specimen drawn on a separate occasion from the first kind and screen to cut back the chance of a crossmatch error and a hemolytic blood transfusion reaction. In fact, 15% of all transfusionrelated deaths are related to hemolytic reactions because of antibody incompatibility. Anti-A or anti-B antibodies are formed every time the person lacks either or each of the A and B antigens. Antigen D is quite common, and, except for the A and B antigens, the one more than likely to produce immunization.
Cheap lady era 100mg overnight deliveryIn addition to hypovolemia breast cancer 2014 game order lady era 100mg without prescription, chest closure is essential in regard to inflicting ischemic modifications by impinging on a venous or arterial graft that lies in a susceptible position on or around the heart cascade women's health yakima purchase lady era 100 mg without prescription. Inotropes � vasopressors � Dobutamine or epinephrine � norepinephrine Or levosimendan (or milrinone) + norepinephrine 2 menstruation questions generic 100 mg lady era with mastercard. Preparation for transportation of a postcardiac surgical affected person should begin with evaluation of the stability of the affected person in the working room menopause weight loss diet quality lady era 100 mg. Electromechanical Support Biventricular pacing Intraaortic balloon pump Extracorporeal membrane oxygenation Ventricular help device Vasoplegic Syndrome 1. The best transport monitoring system has a "brick" that may be ejected from the operating room monitor and is appropriate with the transport monitor. A cardiac anesthesiologist ought to make positive that the pumps used for infusions in cardiac surgery are adequately useful. It is an effective practice to unplug infusion pumps a couple of minutes before leaving the operating room to test the battery life for transport. It is recommended that the anesthesiologist carries no less than one round of "code medication" to assist in the occasion of cardiac arrest during transportation. Handoff failures have been identified as a significant source of medical errors, each between and inside groups. The course of is intended to be strictly sequential: monitoring ought to be transferred earlier than ventilator transfer, and all phase 1 gadgets must be accomplished before information transfer. Vital indicators confirmed to be steady, ventilator functioning well, infusions operating appropriately 6. Patient-specific info (age, weight, medical and surgical historical past, allergy status, baseline very important signs, pertinent laboratory results, analysis, present situation, and vital signs) b. Anesthetic data (intraoperative course and any problems, traces present, blood transfusion or fluid totals, paralytics or opioids, antibiotics, present infusions, very important signal parameters or limits, pain relief plan, laboratory values) 2. Surgeon presents: surgical course (diagnosis, operation performed, surgical findings, issues, blood loss, drains, antibiotic plan, deep vein thrombosis prophylaxis, medicine plan, checks to be done, diet, key targets for the next 6 to 12 hours) Phase 3: Questions and Discussion In all instances, the anesthesiologist ought to stay with the affected person until hemodynamic stability and general stability are ensured. The incidence of this distressing complication is more frequent in cardiac operations than in different cases. Consideration must be given to persevering with to administer a risky anesthetic agent as soon as pulmonary air flow is reestablished and to administering extra sedative-hypnotic doses, an opioid, or each. Use of a peripheral nerve stimulator might facilitate this decision (see additionally Chapter 43). Because shivering can increase oxygen demand by 300% to 600%, it must be prevented by administering a neuromuscular blocking drug. Prolonged aortic crossclamp time, incomplete revascularization, or poor myocardial preservation adds additional threat. Both tachycardia and bradycardia should be avoided, and postoperative arrhythmias ought to be handled. In addition, shivering must be prevented because it raises the heart rate by rising oxygen demand. The predominant hemodynamic effect of a particular catecholamine depends upon the degree to which the, 1, 2, and dopaminergic receptors are stimulated. Although not but obtainable within the United States, a newer class of drugs-the calcium sensitizers-exhibit potent inodilatory properties. Its mechanism of motion is that it will increase myocyte sensitivity to calcium by stabilization of the calcium binding to troponin C, thus enhancing actin-myosin cross-bridging and increasing contractility. Like phosphodiesterase inhibitors, levosimendan might augment inotropy without considerably increasing myocardial oxygen consumption. Afterload reduction with agents efficient within the pulmonary circulation is useful. With the development of new imaging modalities, it has turn into easy to accurately consider the proper coronary heart for administration purposes. Fluid administration in these patients should be very even handed as they could already be congested. Finally, mechanical help for the failing proper coronary heart is available and has seen significant advancement in the earlier few years. Depending on the scenario of the affected person, these units can be either temporary or permanent in nature. Other pharmacologic drugs often used to induce pulmonary vasodilation embrace nitroglycerin and nitroprusside. Inhaled medicine such as nitric oxide, epoprostenol (Flolan), and inhaled iloprost are thought of in refractory instances. Treatment with infusion of a vasoconstrictor drug corresponding to phenylephrine, norepinephrine, vasopressin, or, not often, methylene blue or B12 is normally successful. Dysrhythmias Normal sinus rhythm is ideal because it provides an atrial contribution to ventricular filling and a standard synchronized contraction of the ventricle. However, both supraventricular or ventricular arrhythmias can occur in the immediate postbypass period. With advancing age, dilatation of the atrium interrupts cell-to-cell electrical coupling between atrial muscle fibers. Perioperative factors embody insufficient atrial safety during surgery, pericardial irritation, autonomic imbalance in the course of the postoperative period, change in atrial size with fluid shifts, electrolyte (potassium and magnesium) abnormalities, and excessive manufacturing of catecholamines. Many studies have proven that blockade considerably reduces the incidence of postoperative atrial fibrillation and that withdrawal of -blockers will increase threat. Drugs often employed for this purpose embody calcium channel blockers, -blockers, magnesium, and amiodarone. Expert session must be obtained earlier than remedy is initiated, especially in a stable patient. Although ventricular arrhythmias occur after cardiac surgical procedures, sustained ventricular arrhythmias are relatively uncommon. Associated elements could embrace hemodynamic instability, electrolyte abnormalities, hypoxia, hypovolemia, ischemia or infarction, acute graft closure reperfusion, and using inotropic brokers. A examine of 126 patients with postoperative complicated ventricular ectopy discovered a mortality rate of 75%. Ventricular fibrillation ought to be treated promptly with electrical defibrillation. Multiple elements dictate which particular gadget would most benefit a person affected person. However, arterial vasoconstriction usually plays a central position in acute postoperative hypertension. In the postoperative interval, deepening sedation to management a hypertensive episode will not be the best or the one potential strategy, notably if early extubation (fast tracking) is fascinating. Sodium 54 � Anesthesia for Cardiac Surgical Procedures 1745 nitroprusside, a nonspecific venous and arterial vasodilator, is a typical choice. Fenoldopam is a short-acting dopamine agonist that causes arterial-specific vasodilation by stimulating D1-receptors. Unlike sodium nitroprusside, fenoldopam will increase renal blood circulate to produce diuresis and natriuresis. In addition, severe hypertension may require larger doses of fenoldopam, which may be associated with undesirable increases in coronary heart rate. Dihydropyridine-type calcium channel blockers, similar to nicardipine and clevidipine, selectively chill out arterial resistance vessels without unfavorable inotropic or dromotropic (conduction) results and cause generalized vasodilation of the renal, cerebral, intestinal, and coronary vascular beds.
Lady era: 100 mg
Lady era 100 mg fast deliveryClonidine as an adjuvant to intrathecal local anesthetics for surgery: systematic evaluation of randomized trials women's health clinic yeovil discount 100 mg lady era amex. Spinal antinociception by dexmedetomidine womens health 2 skincare secret report generic 100mg lady era mastercard, a extremely selective alpha 2-adrenergic agonist menstruation weight gain 100mg lady era sale. Effect of low-dose dexmedetomidine or clonidine on the traits of bupivacaine spinal block women's health clinic port adelaide discount 100mg lady era amex. The facilitatory effects of perineural dexmedetomidine on neuraxial and peripheral nerve blockade: a scientific evaluate and meta-analysis. Dose-response effects of spinal neostigmine added to bupivacaine spinal anesthesia in volunteers. Phase I human safety evaluation of intrathecal neostigmine containing methyl- and propylparabens. Use of neostigmine within the management of acute postoperative pain and labour ache: a review. A multi-center study of intrathecal neostigmine for analgesia following vaginal hysterectomy. Comparison of efficacy and issues of 27G and 29G Sprottte needles for subarachnoid anesthesia. Practice advisory for the prevention, prognosis, and management of infectious issues related to neuraxial strategies: an updated report by the American Society of Anesthesiologists Task Force on Infectious Complications Associated with Neuraxial Techniques and the American Society of Regional Anesthesia and Pain Medicine. Antiseptic solutions for central neuraxial blockade: which concentration of chlorhexidine in alcohol ought to we use Ultrasonography of the adult thoracic and lumbar spine for central neuraxial blockade. Comparison of three catheter units for continuous spinal anesthesia in patients undergoing whole hip or knee arthroplasty. Minimal efficient dose of spinal hyperbaric bupivacaine for grownup anorectal surgical procedure: a doubleblind, randomized study. Differential spread of blockade of contact, chilly, and pinprick during spinal anesthesia. Sensory evaluation of regional analgesia in humans: a evaluation of methods and purposes. A comparability of the hydrochloride and carbon dioxide salts of lidocaine and prilocaine in epidural analgesia. Extradural block with bupivacaine: affect of dose, volume, focus and affected person characteristics. Continuous constructive airway stress respiratory will increase the spread of sensory blockade after low-thoracic epidural injection of lidocaine. Continuous constructive airway stress respiration increases cranial spread of sensory blockade after cervicothoracic epidural injection of lidocaine. Extension of sensory blockade after thoracic epidural administration of a test dose of lidocaine at three totally different levels. The Trendelenburg position will increase the spread and accelerates the onset of epidural anesthesia for cesarean part. A survey and a double-blind investigation comparing carticaine with lidocaine in epidural analgesia. Comparison of prilocaine 2% versus lidocaine 2% with adrenaline in peridural anesthesia. Cardiovascular and central nervous system results of intravenous levobupivacaine and bupivacaine in sheep. Cardiac electrophysiologic properties of bupivacaine and lidocaine in contrast with these of ropivacaine, a model new amide local anesthetic. The relative motor blocking potencies of epidural bupivacaine and ropivacaine in labor. Neurological features of issues of spinal anesthesia, with medicolegal implications. Epinephrine markedly improves thoracic epidural analgesia produced by a small-dose infusion of ropivacaine, fentanyl, and epinephrine after main thoracic or stomach surgical procedure: a randomized, double-blinded crossover research with and with out epinephrine. Epidural and intravenous fentanyl infusions are clinically equal after knee surgical procedure. A potential, randomized, double-blind comparability of epidural and intravenous sufentanil infusions. Evaluation of a single-dose, extended-release epidural morphine formulation for pain after knee arthroplasty. Clonidine prolongation of lidocaine analgesia after sciatic nerve block in rats is mediated through the hyperpolarization-activated cation present, not by alphaadrenoreceptors. Improved analgesia with clonidine when added to native anesthetic during mixed spinal-epidural anesthesia for hip arthroplasty: a double-blind, randomized and placebo-controlled study. The efficacy and security of epidural infusions of levobupivacaine with and with out clonidine for postoperative ache relief in sufferers present process complete hip substitute. The analgesic impact of epidural clonidine after spinal surgery: a randomized placebo-controlled trial. The impact of epidural clonidine on perioperative cytokine response, postoperative pain, and bowel operate in patients undergoing colorectal surgical procedure. The impact of extradural ketamine on onset time and sensory block in extradural anaesthesia with bupivacaine. Smalldose S(+)-ketamine reduces postoperative pain when utilized with ropivacaine in epidural anesthesia for whole knee arthroplasty. Epidural administration of neostigmine and clonidine to induce labor analgesia: analysis of efficacy and local anesthetic-sparing impact. Comparison of lidocaine hydrocarbonate with lidocaine hydrochloride for epidural anesthesia. Superiority of multi-orifice over singleorifice epidural catheters for labor analgesia and cesarean delivery. A systematic evaluate of randomized managed trials that consider methods to avoid epidural vein cannulation during obstetric epidural catheter placement. Which is a better position for insertion of a high thoracic epidural catheter: sitting or lateral decubitus Recordings of, and an anatomical clarification for, false positive lack of resistance throughout lumbar extradural analgesia. Epidural house identification: a meta-analysis of complications after air versus liquid because the medium for lack of resistance. Cervical epidural stress measurement: comparability within the susceptible and sitting positions. Complications of obstetric epidural analgesia and anaesthesia: a potential evaluation of 10,995 instances. Appropriate length of epidural catheter within the epidural area for postoperative analgesia: evaluation by epidurography. The optimal distance that a multiorifice epidural catheter ought to be threaded into the epidural house. The impact of the Lockit epidural catheter clamp on epidural migration: a controlled trial. Subcutaneous tunnelling of epidural catheters for postoperative analgesia to forestall accidental dislodgement: a randomized controlled trial.
Cheap lady era 100mg with amexLarge defects with associated low-pressure gradients across them have nonrestrictive flow menstrual orange blood generic lady era 100mg otc. In addition menopause kits boots order 100mg lady era overnight delivery, bigger defects may be anticipated to have a higher effect on downstream buildings and pressures menopause night sweats generic lady era 100 mg on-line. The mainstays of the anesthetic administration of shunt lesions are understanding and controlling components that may influence the path and magnitude of the shunt menstruation y sus sintomas buy lady era 100mg without a prescription. If the clinical downside is luxuriant pulmonary blood circulate, a excessive Fio2 must be prevented. Similarly, the path and magnitude of the shunt flow decide whether one should hyperventilate a patient to achieve a low Paco2 or tolerate a high-normal Paco2. In the presence of a shunt, the potential dilation of the cardiac chambers and resultant enhance in chamber volume and strain are important. These situations cause hyperviscosity, which could be associated with hemostatic abnormalities. Many sufferers with congenital repairs that include a conduit or graft are maintained on antiplatelet drugs, and this ought to be famous. Intracardiac shunts are classically positioned at the degree of the atria or ventricles. The magnitude of the shunt is commonly expressed in phrases of the ratio of pulmonary blood circulate (Qp) to systemic blood move (Qs): Qp/ Qs. A Qp/Qs ratio higher than 1 is generally in preserving with acyanotic coronary heart disease and luxuriant pulmonary blood move. Intracardiac shunts and the Qp/ Qs are often bidirectional, depending on situational physiology, and subsequently must always be thought-about to be a risk for systemic embolization. Special point out of sure aortopulmonary shunts, used commonly prior to now to palliate some forms of cyanotic coronary heart disease, is warranted. The proximal connection may be to the ascending aorta, brachiocephalic trunk, or subclavian artery. Because blood move via this sort of shunt depends on systemic blood strain, systemic hypotension could result in worsening hypoxemia. Furthermore, long-term publicity to these extracardiac shunts may end up in left-sided chamber enlargement and dysfunction secondary to continual quantity overload. This is related to train intolerance and decreased practical capacity, which appear to have important prognostic implications. Regional anesthesia may be used for acceptable procedures, but neuraxial blocks ought to be administered with caution because of the sympathetic blockade produced. Patients with significant pulmonary hypertension are very delicate to preload; subsequently, hypovolemia, must be handled immediately and aggressively. As in adult sufferers with acquired coronary heart illness, the presence of ventricular dysfunction is an important danger factor for morbidity and mortality, both in the perioperative interval and in the lengthy term. Additionally, atrial fibrillation causes 24% of strokes in sufferers older than eighty years old. The transition of the electrical sign from one type of tissue to the opposite might be liable for this arrhythmia. The traditional Maze procedure is currently the most effective healing therapy for atrial fibrillation. A commercially out there bipolar instrument permits the operator to assess transmurality. Currently, newer applied sciences allow the fast creation of traces of conduction blockade, which surgeons use to ablate atrial fibrillation in patients present process concomitant cardiac surgical procedures. These applied sciences include alternate vitality sources similar to radiofrequency and microwave vitality, ultrasound, cryotherapy, and laser (Table fifty four. These technologies are additionally used in minimally invasive surgical ablation procedures to remedy isolated atrial fibrillation. Because cardiac constructions can be visualized directly during open surgical procedures, ablation lines could be created safely, thus avoiding the complication of pulmonary vein stenosis. The pericardial sac has two layers: the outer, parietal pericardium; and the inside, visceral pericardium (epicardium), which is instantly adherent to the surface of the guts. As a result, the atrial and ventricular diastolic transmural pressures are essentially zero, a trademark of pericardial tamponade. Pulsus paradoxus is outlined as a drop in systolic blood pressure exceeding 10 mm Hg throughout inspiration. Wide swings in intrathoracic strain and circumstances such as pulmonary embolism or hypovolemic shock also can give rise to the phenomenon. Pericardial pressure-volume (or strain-stress) curves are shown during which the quantity increases slowly or rapidly over time. On the left, quickly growing pericardial fluid first reaches the restrict of the pericardial reserve quantity (the preliminary flat segment) and then shortly exceeds the restrict of parietal pericardial stretch, thus causing a steep rise in strain, which turns into even steeper as smaller increments in fluid trigger a disproportionate increase in the pericardial pressure. On the proper, a slower price of pericardial filling takes longer to exceed the restrict of pericardial stretch as a end result of extra time is available for the pericardium to stretch and for compensatory mechanisms to turn out to be activated. Patients with pericardial tamponade might present with pain or feelings of fullness in the chest, dyspnea, lethargy, fever, cough, weakness, fatigue, anorexia, or palpitations. However, sufferers whose tamponade develops secondary to a continual medical condition. The timing of the collapse of the two chambers is related to the bottom intracavitary pressures in those chambers. However, in sufferers with very giant effusions, fluid does accumulate behind the left atrium and ultimately collapses this chamber. Indications for pericardiocentesis (surgical drainage of the pericardial effusion) have been summarized by Soler-Soler and colleagues (Box fifty four. If common anesthesia is deliberate, the watchwords within the administration of cardiac tamponade are fast, full, and robust. Intravenous fluids must be administered earlier than induction of anesthesia to optimize preload. Increasing intravascular quantity helps to increase the efficient filling pressures of the guts, restore the gradient between the chambers, and increase arterial pressure. Another possibility is to induce general anesthesia however to permit the patient to breathe spontaneously, avoiding constructive intrathoracic pressure, till the pericardial sac is opened. Drugs that may cause myocardial depression should be prevented and thus etomidate is usually chosen as the induction agent of selection. The use of ketamine to induce common anesthesia for creation of a pericardial window has been described. A subcostal view in early diastole reveals a big circumferential pericardial effusion compressing the guts, with the best ventricle completely collapsed (arrowheads). Constrictive pericarditis is alleged to be present when the diastolic filling of the guts is restricted by a thickened and adherent pericardium. Several causes of constrictive pericarditis have been identified, together with infectious processes. In addition, radiation to the chest area and cardiac surgical procedure itself have emerged as extra causes of constrictive pericarditis over the past few a long time. A excessive driving stress throughout the valves causes a fast filling of the ventricles in diastole and results in sudden improve in the ventricular pressures.
Diosma (Buchu). Lady era. - Dosing considerations for Buchu.
- Are there safety concerns?
- Are there any interactions with medications?
- How does Buchu work?
- What is Buchu?
- Urinary tract infections, kidney infections, and sexually transmitted diseases.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96216
Buy generic lady era 100 mg on lineBecause standard laboratory tests monitor solely coagulation menstrual migraine headaches lady era 100mg on-line, this balance could additionally be troublesome to assess within the absence of viscoelastic tests menstruation 4 days early buy cheap lady era 100mg, which consider complete blood clotting menstrual show order lady era 100mg mastercard. For occasion breast cancer oakley sunglasses generic lady era 100 mg without a prescription, hepatic artery thrombosis is extra common in pediatric recipients due to the small caliber of the vessel, and bile leaks are extra common after liver transplantation using grafts from cardiac demise donors. Immunosuppressive medicines, used to stop rejection, are largely liable for this threat. Surgical web site infections, intraabdominal abscesses, and infected hematomas are widespread. In liver transplant recipients, bacterial translocation or bile leaks can lead to peritonitis, cholangitis, and perihepatic abscesses. Prolonged endotracheal intubation and indwelling central venous and urinary catheters are a typical supply of an infection. In the meantime, strict aseptic approach is required when accessing indwelling catheters and tubes. Comorbidities, such as diabetes and renal dysfunction, can improve the danger of an infection. The targets of immunosuppression are to stop graft loss and to avoid the adverse penalties of antirejection regimens. Hypertension is due to vasoconstriction and sodium retention, and usually seems within the first weeks of remedy. Neurologic toxicity includes tremors, complications, seizures, and even focal neurologic abnormalities. Mycophenolate mofetil remedy is a beneficial adjunct by permitting a discount within the doses of calcineurin inhibitors. In addition to tacrolimus, probably the most broadly used drug, there are tons of other drugs out there. Of observe, recipients of liver grafts require much less immunosuppression than do recipients of other organs, and liver grafts confer protection on different organs transplanted from the same donor. The threshold for performing a biopsy must be low, albeit with an consciousness that other conditions can mimic the histologic adjustments seen with rejection. For instance, diffuse lymphocytic infiltration of the kidney may be seen with rejection or lymphoproliferative disorder, and recurrent hepatitis C in the liver can resemble rejection. Malignancy Immunosuppressant medication improve the susceptibility of transplant recipients to malignancy. Clinical presentation varies from a mononucleosis-like syndrome to malignant lymphoma. The mean latency period for all cancers is three to 5 years after transplant, though specific malignancies exhibited unique time intervals. Cancer websites vary relying on the organ transplanted; for instance, renal transplant recipients have a 100-fold greater than expected danger of growing carcinoma in the native kidney. Challenges for the longer term include a solution to the organ scarcity, strategies to minimize the probability of illness recurrence, and pharmacologic advances aimed at limiting the unwanted side effects of immunosuppression. Long-Term Survival Long-term survival is affected by widespread illnesses corresponding to hypertension, hyperlipidemia, and diabetes mellitus. From its starting as an experimental procedure, it has become the best hope for survival in the case of liver transplantation, and the greatest option for an unbiased life with out morbidity in the case of renal and pancreatic 60 � Anesthesia for Abdominal Organ Transplantation forty six. Natl Vital Stat Rep Cent Dis Control Prev Natl Cent Health Stat Natl Vital Stat Syst. Paediatric intestinal and multivisceral transplantation: indications, choice, and perioperative administration. Predicting outcome after liver transplantation: utility of the model for end-stage liver illness and a newly derived discrimination function1. State of deceased donor transplantation in India: a mannequin for creating countries around the world. The international diffusion of organ transplantation: tendencies, drivers and policy implications. The need for kidney transplantation in low- and middle-income countries in 2012: an epidemiological perspective. Strategies to increase the donor pool and access to kidney transplantation: a global perspective. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality normally population cohorts: a collaborative meta-analysis. Diastolic coronary heart failure in dialysis sufferers: mechanisms, diagnostic method, and remedy: cardiomyopathy in dialysis sufferers. Reverse transforming and prognosis following kidney transplantation in contemporary sufferers with cardiac dysfunction. Severe left ventricular systolic dysfunction might reverse with renal transplantation: uremic cardiomyopathy and cardiorenal syndrome. Atrial fibrillation and persistent kidney disease: struggling by way of thick and skinny: table 1. An professional opinion on the current remedy of anemia in sufferers with kidney illness. Coagulation profile in patients with chronic kidney illness before and after kidney transplantation: a retrospective cohort study. Dyspepsia and gastric emptying in end-stage renal illness sufferers on hemodialysis. Cardiac illness analysis and management amongst kidney and liver transplantation candidates. Clinical characteristics of dialysis patients with acute myocardial infarction in the us: a collaborative project of the United States renal data system and the national registry of myocardial infarction. A call to motion: variability in pointers for cardiac evaluation before renal transplantation. Cardiac testing for coronary artery illness in potential kidney transplant recipients: a scientific evaluate of take a look at accuracy research. Myocardial ischemia evaluation in chronic kidney disease: challenges and pitfalls. Technetium myocardial perfusion scanning in prerenal transplant analysis in the United Kingdom. Stress echocardiography for risk stratification in patients with end-stage renal illness present process renal transplantation. Prognostic value of myocardial perfusion research in patients with end-stage renal disease assessed for kidney or kidney-pancreas transplantation: a meta-analysis. Effect of perioperative insulin infusion on surgical morbidity and mortality: systematic evaluate and meta-analysis of randomized trials. Succinylcholine-induced hyperkalemia in sufferers with renal failure: an old question revisited. Moving beyond Kucera and Francis: a crucial evaluation of current word frequency norms and the introduction of a new and improved word frequency measure for American english.

Lady era 100mgIn Europe women's health free trial raspberry ketone buy cheap lady era 100 mg on-line, there are a variety of regional or nationwide organ allocation bodies that distribute organs within their respective nation or region based mostly on totally different allocation standards womens health 2012 buy 100mg lady era. Regional disparities in candidate entry to transplantation have been addressed with the Regional Share 35/National Share 15 coverage menstrual vacuum purchase lady era 100mg fast delivery. Careful adherence to sterile approach is required to prevent infectious complications in this immunosuppressed population menopause without symptoms lady era 100mg with amex. A stress dose of corticosteroids is required for sufferers receiving chronic supplementation. Renal perform must be assessed and managed fastidiously to keep away from an exacerbation of immunosuppressant-associated renal impairment. Hypertension is a standard discovering in sufferers whose situation is managed with calcineurin inhibitors corresponding to cyclosporine. Drugs recognized to decrease hepatic blood flow, corresponding to propranolol, ought to be avoided. In others, transplant is indicated because of a high danger of demise related to the underlying condition, as in congenital mucosal issues, desmoid tumor, and ultrashort bowel syndrome. In some patients, transplant is considered within the context of frequent debilitating hospitalizations, typically for dehydration from stomal losses. Over the past 2 decades, additional refinements in immunosuppression, donor-recipient matching, surgical technique, and perioperative care have steadily improved outcomes. These procedures now have an established function within the therapy of intestinal failure from a variety of causes. The Intestinal Transplant Registry collected worldwide information from 82 programs transplanting 2699 patients between 1985 and 2013 and reported pooled affected person survival of 76%, 56%, and 43% at 1, 5, and 10 years, respectively. Small numbers favor administration in regional or national models during which expertise is concentrated. Definitions of intestinal transplant procedures are debated but the most extensively used are as follows: Small gut transplant: gut with out the liver or stomach; liver-intestine transplant: small gut and liver however no stomach; modified multivisceral transplant: abdomen and intestine with out liver; multivisceral transplant: gut plus liver and stomach. The pancreas is often included in a composite graft, often for technical simplicity but typically also to treat pancreatic insufficiency. Indications for intestinal transplant in kids include quick bowel syndrome from gastroschisis, necrotizing enterocolitis and volvulus, and microvillous inclusion illness. Adults are offered transplantation for thrombotic and traumatic intestinal infarction, desmoid tumor, Crohnrelated quick bowel syndrome and intestine motility issues. In most of these circumstances transplantation has been supplied due to life-threatening problems of parenteral diet, including progressive cholestasis and liver Surgical Procedures Organs transplanted depend upon the indication, recipient liver operate, and surgical situations following earlier procedures. Isolated small bowel or small bowel-stomachduodenum transplant is usual in short bowel syndrome, motility disorders, and desmoid tumor. Inclusion of pancreas avoids the risk of hilar damage associated with its removing on the back-table and reduces the danger of kinking of adjacent vessels (superior mesenteric vessels, portal vein, middle colonic artery) in the implanted graft. It additionally avoids the need for Roux loop biliary drainage and is beneficial if the recipient is diabetic. Pretransplant renal dysfunction from obstructive uropathy, renal vein thrombosis, or recurrent extreme dehydration might require implantation of a kidney graft as a half of the identical procedure. Once the graft advanced is reperfused, a proximal intestinal, gastric, or gastroesophageal anastomosis, is carried out for higher intestine continuity. This could also be adopted by end-to-side anastomosis of recipient colon to donor ileum to full lower intestine continuity. The distal finish of the transplanted small intestine is then introduced out as a brief stoma. This could additionally be difficult, sometimes requiring delayed primary closure, use of reinforcing mesh, a muscle flap, or even grafting of the donor belly wall. Logistics and technique for procurement of intestinal, pancreatic and hepatic graft from the identical donor. Preoperative assessment mirrors that for liver transplant (described earlier) with further caveats as follows. Central venous entry is usually compromised by previous catheter-related infection or thrombosis. Partial or full obstruction of the innominate veins or superior vena cava is usually encountered, even presenting as facial swelling with fluid overload or with exercise, which can contraindicate any graft incorporating a liver. All central vessels should be assessed for patency by ultrasound and, if any doubt, by magnetic resonance angiography. Access should be planned earlier than wait itemizing, including provision for involvement of an interventional radiologist if needed. Most multivisceral candidates are prothrombotic on viscoelastic testing, even within the presence of liver dysfunction, and confirmation of this will affect intraoperative management. Chronic stomach pain related to opiate use can be current in many intestinal transplant candidates, and specialist pain service evaluation and advice are essential, since postoperative and longer-term follow-up are sometimes wanted. Given the greater physiological and metabolic demands of a multivisceral procedure in comparison with liver transplant alone, each of these conditions might contraindicate multivisceral transplant. Important comorbidities embrace sarcopenia, ischemic heart illness, and diabetes, especially in candidates over 60 years old, and can also point out prohibitive threat. Intraoperative Management To date, literature on the perioperative anesthetic management of intestinal and multivisceral transplant recipients is essentially anecdotal. Anesthetic method, vascular access, and monitoring modalities are mainly as described within the setting of liver transplantation, though the pathophysiological adjustments of end-stage liver disease are only current in liver-intestine and multivisceral candidates. A description of the differences between liver-intestine and liver-only transplantation follows. Dissection and removing of recipient viscera can therefore be extended and related to severe surgical bleeding. An agreed upon large transfusion protocol with the hospital blood bank is important. Difficult dissection also will increase the risk of lengthy ischemia times and hurt to the graft. The need to decrease ischemic time requires close coordination between donor and recipient teams, and the recipient anesthetic is began as quickly as the organs are judged to be usable, sometimes even before donor explant. A warmth exchanger is integrated within the bypass circuit to maintain normothermia throughout a protracted interval of partial extracorporeal circulation. Since acidosis and hyperkalemia are also common issues in these massively transfused sufferers, some centers make use of preemptive intraoperative hemofiltration, requiring placement of a dual-lumen dialysis catheter in one other central vein, ideally separate from any multi-lumen catheter used for vasoactive medication. If right inside jugular vein cannulation is known to be not potential, different websites ought to be planned on the time of evaluation. These might involve interventional radiology or surgical access at different supradiaphragmatic websites. The danger of spontaneous thromboembolism, probably life-threatening, also appears be greater than in liver-alone implantation, given the hypercoagulability often seen on baseline thromboelastogram and unpredictable changes in coagulation during fast administration of huge volumes of blood merchandise. This will help maintain a supportive relationship between blood bank and the transplant team despite distinctive calls for on this service, and in addition facilitates timely use of prothrombin and fibrinogen concentrates when requested. Reperfusion of an intestine-only graft is usually uneventful, however inclusion of liver in a composite graft usually produces hyperkalemia and at least transient hypotension, since reperfusion involves a large mass of tissue and occurs via hepatic arterial and portal venous routes in shut succession. Although the latter could also be useful in the prevention of hyperkalemia and extreme acidosis, its benefits are unproven.

Order 100mg lady era otcEven with surgical procedure menstrual extraction procedure discount lady era 100mg with mastercard, perfect weight is hardly ever achieved pregnancy reveal buy generic lady era 100mg, and after a selection of years at a plateau menstruation for more than a week proven lady era 100 mg, weight achieve usually recurs menopause the musical songs lady era 100mg without a prescription. In some patients, especially within the presence of severe comorbidities, simple prevention of further weight achieve may be the most affordable goal. Beyond the useful effects of therapeutic way of life change, particular intervention could also be required to deal with the dyslipidemia and hypertension related to obesity and metabolic syndrome. Statins cut back cardiovascular disease threat in sufferers with type 2 diabetes and metabolic syndrome. Omega-3 fatty acids lower triglyceride ranges and enhance insulin resistance in patients with metabolic syndrome. They are often used in combination remedy with other courses of the hypolipidemic drugs. A appreciable factor of the risk reduction resulting from antihypertensive therapy is lowering arterial blood stress. The therapy of insulin resistance and hyperglycemia in metabolic syndrome, type 2 diabetes, and obesity is often achieved with oral hypoglycemic medication. These include -glucosidase inhibitors, sulfonylureas, meglitinides, D-phenylalanine derivatives, biguanides, and thiazolidinediones. There is a critical potential for postoperative lactic acidosis that may develop in patients utilizing this drug. This chance has led some physicians to routinely cancel or delay surgical procedures if metformin has been ingested inside 48 hours of the scheduled surgery. Other physicians, nevertheless, have their sufferers continue taking metformin, both before and after surgery, without interruption if possible. Recent evidence signifies that sufferers taking metformin have a 58 � Anesthesia for Bariatric Surgery 1917 reduced risk for problems. Orlistat, a lipase inhibitor, reversibly binds to lipase and prevents both absorption and digestion of sure dietary fats. Because orlistat also interferes with the absorption of fat-soluble nutritional vitamins, sufferers utilizing this drug have to complement fat-soluble vitamins A, D, E, and K. It has important gastrointestinal unwanted facet effects including diarrhea, steatorrhea, flatulence, fecal incontinence, and oily rectal discharge. The key options of typical behavioral packages embrace self-monitoring, objective setting, nutrition and train schooling, stimulus control, drawback fixing, cognitive restructuring, and relapse prevention. Patients typically profit from referral to multidisciplinary weight reduction applications that incorporate diet, bodily exercise, and behavioral interventions to achieve their weight loss objectives as a end result of these mixed interventions provide one of the best weight loss and weight upkeep results with out pharmacologic or surgical intervention. According to the evaluation, claims for weight loss have been made for multiple merchandise corresponding to chitosan, chromium picolinate, conjugated linoleic acid, ephedra alkaloids (ma huang),fifty two and Garcinia cambogia. The solely studies involving herbals that have constantly demonstrated weight reduction contain mixtures of ephedrine and caffeine. For this reason, ma huang, a pure supply of the ephedra alkaloid, is added to most, if not all, dietary dietary supplements marketed for weight loss. The success of ephedrine as a weight loss agent in combination with caffeine and or aspirin is well established. Unfortunately, a number of instances of cardiac and neurological issues, together with hypertension, stroke, seizure, and even dying have been reported,fifty five presumably associated to the inconsistent doses in the preparations and the dearth of medical supervision in folks consuming these products for weight reduction. Consequently, the National Institutes of Health has banned these products from any really helpful weight loss regimen. In current practice, there are solely two classes of weight reduction drugs: appetite suppressants and lipase inhibitors. Three medicine are at present obtainable for the specific indication of weight reduction: phentermine, lorcaserin,50 and orlistat. Phentermine decreases appetite and food intake and will increase resting metabolic price to promote weight loss. These gastric stimulators have been tried for the explanation that early 2000s and have been found to cause modest weight reduction with few unwanted effects. Most studies demonstrated weight loss in the course of the first 12 months; however just a few studies had a followup interval of longer than 1 year. No serious side effects have been noted in the first sixty five patients reported on in this study56 or within the 20 patients followed in one other. Unfortunately, pediatric weight problems is the most common childhood nutritional dysfunction within the United States. This is one of the tragedies of the present weight problems epidemic: the numerous and rising prevalence of obesity within the younger. It has attained a stage of controversy that has concerned the location of vending machines in schools and the availability of sweetened snacks and delicate drinks in public locations as public policy is developed to assist control the epidemic of pediatric obesity. The National Health and Nutrition Examination Survey 2011�14 knowledge show that the prevalence of obesity in children for age 2 to 5, 6 to eleven, and 12 to 19 years are 9. While the prevalence of weight problems among children of ages 6 to 11 and 12 to 19 has steadily elevated since 1988, there has been a slight recent decline in obesity amongst ages 2 to 5 years. A number of growing countries have childhood prevalence rates greater than that of the United States,sixty one indicating that adolescent weight problems is turning into pervasive. Treatment of pediatric obesity is predicated on the balance of caloric consumption and expenditure. The three pillars of success in this treatment are: higher eating habits, elevated physical activity, and decreased sedentary activity. Lifestyle interventions remain the treatment of selection in pediatric weight problems, however concomitant pharmacotherapy could also be helpful in some sufferers. Orlistat, which is covered elsewhere on this chapter, should be thought-about as second-line therapy for pediatric obesity. More adolescents are presenting for weight reduction surgery, after failing to cut back weight and/or comorbidities in medically supervised and pharmacologically assisted weight loss applications. Even though many grownup bariatric surgery programs are well certified to present protected and effective perioperative take care of these sufferers, they may not be as well geared up to handle the distinctive metabolic and psychological wants of teenagers. Because of the shorter period of obesity and fewer age-related comorbidities, adolescent sufferers have shorter size of keep and decrease immediate postoperative mortality when in comparability with adults. Is parental consent to a semi-elective, relatively high-risk process applicable Does the kid really perceive the concept of excessive threat of death in the month after surgery These and other such questions of ethics in medication must be addressed, but are beyond the scope of this chapter. The fast enhance within the prevalence of both morbid obesity and superobesity, along with the increased danger of early demise throughout the overweight inhabitants, has considerably elevated the number of bariatric surgical procedures performed annually. The term bariatric surgery refers to surgical alteration of the small gut or abdomen with a view toward producing weight reduction. It is estimated that over 216,000 bariatric surgeries are being performed yearly in the United States.
Discount lady era 100 mg overnight deliveryThis latter occasion can only occur when coughing happens after the endotracheal tube has been eliminated pregnancy exercise discount 100mg lady era visa. Two retrospective studies have revealed that increased postoperative arterial blood stress was related to intracerebral bleeding after craniotomy womens health 092012 purchase 100 mg lady era otc. Also women's health boutique escondido ca lady era 100 mg on-line, the connection between hypertensive transients at emergence and edema formation is unconfirmed women's health center of chicago buy cheap lady era 100 mg. A widespread technique for the management of systemic hypertension over the past stages of a craniotomy is the expectant and/or reactive administration of lidocaine and vasoactive agents, most commonly labetalol and esmolol. Administration of dexmedetomidine through the process or just previous to its conclusion additionally reduces the hypertensive response to emergence173 and hypertension in the postanesthesia care unit. The authors encourage trainees to embody in their anesthetic technique as much narcotic as is consistent with spontaneous air flow at the conclusion of the process, as opioids are antitussive and depress airway reflexes. Patients can also emerge extra quickly and easily when the last inhaled anesthetic to be withdrawn is nitrous oxide. This could be supplemented, if necessary, with propofol by both bolus increments or infusion at charges within the range of 12. An additional principle related to the emergence from neurosurgical procedures is that emergence ought to be timed to coincide not with the final suture however quite with the conclusion of the applying of the head dressing. Many a great anesthetic for neurosurgery has been spoiled by severe coughing and straining that occurs in association with endotracheal tube motion during the utility of the pinnacle dressing. Another nuance of our apply has been to withhold administration of neuromuscular antagonists so long as possible in the later levels of the process. The administration of lidocaine is one other apparently effective approach for decreasing airway responsiveness and the probability of coughing/straining as the depth of anesthesia is reduced in anticipation of emergence. Because of the premium positioned on minimizing coughing and straining and hypertension, there could also be a temptation to extubate from the trachea earlier than full restoration of consciousness. Specific Procedures Many of the concerns relevant to particular person neurosurgical procedures are generic ones which have already been presented within the previous section on Recurrent Issues in Neuroanesthesia. The descriptions that observe will spotlight only procedure-specific issues (Box fifty seven. Location and size of the tumor give the anesthesiologist an indication of the surgical position, the potential for blood loss, and will generally reveal a threat of air embolism. Irritation of the hypothalamus can elicit sympathetic responses together with hypertension. Damage to the hypothalamus can result in a spectrum of physiologic disturbances, notably water balance. Diabetes insipidus is the most probably, although the cerebral salt-wasting syndrome can infrequently occur. The numerous disturbances of water steadiness usually have a delayed onset, beginning 12 to forty eight hours postoperatively, somewhat than within the operating room. Retraction and irritation of the inferior surfaces of the frontal lobes can lead to a patient who reveals both delayed emergence or some extent of disinhibition, or each. The phenomenon is more likely to be evident when there has been bilateral frontal lobe retraction. The anesthetic implication is that the clinician should be extra inclined to confirm return of consciousness earlier than extubating the affected person somewhat than to extubate expectantly. A further implication taken by these authors (though not confirmed by any systematic study) is that a less liberal use of intravenous anesthetic medication. This relies on the rationale that low residual concentrations of those anesthetics which are suitable with reasonable recovery of consciousness in most sufferers may be much less properly tolerated in this inhabitants. Subfrontal approaches are mostly utilized in patients with olfactory groove meningiomas and sufferers with suprasellar tumors together with craniopharyngiomas and pituitary tumors with suprasellar extension. Second, the administration of the ischemia caused by vasospasm involves fluid resuscitation and induced hypertension. Early occlusion of the aneurysm eliminates the risk of rebleeding related to this therapy. A 48-hour course is right (see the earlier dialogue of steroids), although 24 hours is sufficient for a scientific impact to be evident. A routine corresponding to 10 mg intravenously or orally adopted by 10 mg every 6 hours is typical. Preinduction placement could also be applicable in patients with extreme mass effect and little residual compensatory latitude. It is the interval of induction and pinning during which hypertension, with its attendant dangers in a affected person with impaired compliance and autoregulation, is most probably to happen. Arterial traces also facilitate careful administration of blood stress throughout emergence. Once the skull is open, observation of situations within the surgical area provides equal data. Management of Anesthesia the ideas governing the choice of anesthetic medication are introduced within the earlier section, Control of Intracranial Pressure and Brain Relaxation. Early aneurysm clipping reduces the period of hospitalization and reduces the incidence of the medical complications. Furthermore, a point of hydrocephalus is quite common after blood contaminates the subarachnoid area. All this places a substantial premium on techniques designed to reduce the volume of the intracranial contents (see Control of Intracranial Pressure and Brain Relaxation earlier on this chapter) to facilitate exposure and minimize retraction pressures. Cerebral salt-wasting syndrome is associated with a contracted intravascular quantity. The anesthesiologist should determine whether vasospasm has occurred and what, if any, therapies for it have been undertaken. Symptomatic vasospasm has historically been handled with "Triple H" therapy (hypervolemia, hypertension, and hemodilution). Current management has shifted towards fluid resuscitation to euvolemia (rather than hypervolemia),a hundred seventy five,188 hypertension, and generally balloon angioplasty or intraarterial vasodilators. The association of hypotension with poor consequence,one hundred ninety and the potential for hypotension to trigger or worsen cerebral ischemia in patients with some degree of vasospasm, is nicely acknowledged. The science behind hypervolemic-hypertensive therapy is gentle and the efficacy of neither Triple H therapy nor volume growth in isolation has been proved by prospective examine. Because nimodipine should be administered orally in North America, nicardipine has been evaluated as an intravenous different. The multicenter nicardipine trial202,203 revealed a reduced incidence of symptomatic vasospasm however no improvement in consequence. Several other agents/ drug classes have been thought-about for the prevention of vasospasm and delayed ischemic deficits. A research of the endothelin antagonist clazosentan revealed improved mortality without enchancment within the consequence of survivors. Meta-analysis revealed only nonsignificant trends towards lowered incidence of delayed cerebral ischemia and death.
References - Fisher ER, Palekar AS, Gregorio RM, Paulson JD. Mucoepidermoid and squamous cell carcinomas of breast with reference to squamous metaplasia and giant cell tumors. Am J Surg Pathol. 1983;7(1):15-27.
- Kleine, R.S., Cattolica, E.V., Rankin, K.N. Hemiacidrin renal irrigation: complications and successful management. J Urol 1982;128:241-242.
- Menon M, Kaul S, Bhandari A, et al: Potency following robotic radical prostatectomy: a questionnaire based analysis of outcomes after conventional nerve sparing and prostatic fascia sparing techniques, J Urol 174(6):2291n 2296, discussion 2296, 2005.
- Gehring, H., Nahm, W., Zimmermann, K. et al. Irrigating fluid absorption during percutaneous nephrolithotripsy. Acta Anaesthesiol Scand 1999;43:316-321.
- Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology. 1999;30:1434-1440.
- Kuerer HM, Wayne JD, Ross MI. Anaphylaxis during breast cancer lymphatic mapping. Surgery. 2001;129:119-120.
- Bays RA, Fonseca RJ, Turvey TA. Single arch stabilization devices for segmental orthognathic surgery. Oral Surg 1978; 46:467-476.
- Massey NJ, Sherry KM, Oldroyd S, et al: Pharmacokinetics of an infusion of propofol during cardiac surgery, Br J Anaesth 65(4):475-479, 1990.
|