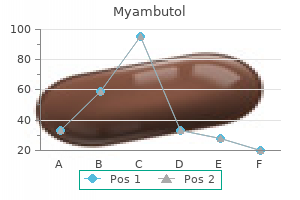
Myambutol
Joseph T. Cooke, M.D., FACCP - Associate Professor of Clinical Medicine
- Associate Director, Medical Critical Care
- The New York Hospital-Cornell Medical Center
- New York, NY
Order myambutol 800 mg with mastercardIts principal impact is to promote calcium absorption within the intestine to find a way to infection 2 cure race buy cheap myambutol 400mg line ensure an adequate supply of calcium virus zona 400mg myambutol mastercard. This effect could be overcome by increasing calcium intake so that passive (para-cellular versus virus 100 generic myambutol 600mg with amex trans-cellular) absorption can compensate infection lab values myambutol 400 mg amex. Summary Mineral metabolism in the fetus may be very completely different from that in post-natal life. Following start, profound adjustments occur which initially lead to transient hypocalcaemia however which, by the end of the first week, have largely settled all the means down to a postnatal sample which stays largely unchanged, at least in high quality, if not amount, in the course of the the rest of life. Because of this, defects within the varied mechanisms may not necessarily have any important results prenatally but turn into more obvious post-natally. The interrelationship of parathyroid function and calcium, magnesium, and phosphorus metabolism in regular, sick, and hypocalcemic newborns. Bone growth and mineral homeostasis in the fetus and neonate: Roles of the calciotropic and phosphotropic hormones. Circulating ranges of soluble alpha-Klotho are markedly elevated in human umbilical cord blood. Parathyroid hormone-related protein as a prohormone: Posttranslational processing and receptor interactions. Fibroblast progress issue 23 concentrations in wholesome time period infants through the early postpartum period. Glossary Calcipaenia Calcium deprivation within the body as a end result of vitamin D and/or dietary calcium deficiency. Epiphysis End of an extended bone formed from secondary middle of ossification which is initially separate from the body of the long bone and later unites with it through ossification. Metaphysis Growing part of the lengthy bone which lies between the growth plate and the diaphysis. Mineralization Integration of hydroxyapatite crystals into pre-formed osteoid, creates the bone matrix. Ossification Transformation of a cartilage body into bone tissue during bone growth. Introduction Rickets and osteomalacia happen as a consequence of faulty mineralization of the skeleton. Such reduced mineralization leads to soft bones, which deform and break extra easily, and stunting of growth. The non-nutritional types of rickets can be related to raised intracranial stress from craniosynostosis, and extreme hypophosphatasia is related to respiratory insufficiency from pulmonary hypoplasia secondary to insufficient chest growth. Dental manifestations are a frequent association as a end result of impaired mineralization of enamel. Defective mineralization occurs as a end result of (1) lack of mineral provide to mineralization sites (calcium or phosphate), (2) lack of the mineral provider calcitriol (hormone synthesized from vitamin D) which controls their intestinal absorption, and (3) less commonly because of lack of the tissue non-specific alkaline phosphatase enzyme which facilitates mineralization. The main cause of rickets worldwide is dietary calcium deficiency and/or vitamin D deficiency (Munns et al. The current refugee disaster and immigration of darkish skinned individuals from low earnings international locations into high latitude regions has led to the resurgence of nutritional rickets in excessive earnings countries (H�gler and Munns, 2016). A primary understanding of the physiology of bone development, structure and mineralization is crucial to differentiate and manage varied forms of rickets and osteomalacia, and their basic difference to osteoporosis. Terminology Buster: Bone Formation, Mineralization, Ossification, Calcification the bone tissue or matrix is composed of 50%�70% mineral (predominantly calcium and phosphate), 20%�40% natural material (predominantly type 1 collagen), 5%�10% water, and o3% lipids (Clarke, 2008). The three major types of bone cells are (1) osteoblasts which type new bone, (2) osteoclasts which resorb old bone and calcified growth plate cartilage, and (3) osteocytes which constitute 90% of the cells within the matrix and are liable for biomechanical sensing and hormone manufacturing (Bellido et al. The term "bone formation" describes the method of synthesis of extracellular natural osteoid followed by its mineralization, with later integration of osteoblasts which remodel into osteocytes. In contrast, the term "ossification" relates to the two main modes of bone growth: intramembranous ossification is seen in flat bones such because the skull and endochondral ossification in lengthy bones such as the femur (Gilbert, 2000). Pathological mineralization or "calcification" in its true that means is deposition of calcium-phosphate 334 Encyclopedia of Endocrine Diseases, Second Edition, Volume 5 doi:10. Some of the conditions associated with pathological calcification embody: Generalized arterial calcification of infancy, pseudoxanthoma elasticum, dermatomyositis and subcutaneous fats necrosis (Nitschke and Rutsch, 2017). Endochondral ossification and mineralization benefit extra detailed dialogue to be succesful of respect the pathogenesis and clinical features of rickets in kids. Endochondral Ossification Longitudinal growth occurs through endochondral ossification in lengthy bones. Condensation of mesenchymal cells to kind cartilage precedes their differentiation into chondrocytes (Mackie et al. The cartilage structure is invaded by cells to form the first ossification heart at the middle (midshaft) followed by secondary ossification centers at the ends (epiphyses). The main and secondary ossification centers are separated by the growth plate which is liable for longitudinal progress and drives expansion of the primary ossification center (Mackie et al. The articular epiphyseal development cartilage is answerable for growth and shaping of the epiphyses and drives growth on the secondary ossification middle. The primary and secondary ossification centers encroach onto each other steadily replacing the cartilage with bone tissue besides on the articular floor. The chondrocytes within the growth plate are arranged in morphologically distinct zones. Cells in the resting zone then enter the proliferative zone the place they endure division and produce giant quantities of extracellular matrix protein (Rauch, 2005). Intracellular calcium focus continues to increase within the hypertrophic chondrocytes and sooner or later they start to mineralize the longitudinal septa within the surrounding matrix to type the zone of provisional calcification (Rauch, 2005). The ultimate apoptosis of hypertrophic chondrocytes triggers mineralization of the matrix and vascular invasion (facilitating osteoblast invasion) on the metaphyseal/growth plate junction (primary spongiosa). Lack of phosphate supply at the progress plate (Tiosano and Hochberg, 2009) prevents apoptosis of hypertrophic chondrocytes and thus inhibits each mineralization and development. Eighty percent of the longitudinal septa of the expansion cartilage are quickly resorbed in the metaphyseal zone instantly behind the invading blood vessels and the remaining longitudinal septa serve as scaffolds, on which osteoblasts deposit additional bone matrix (secondary spongiosa) (Rauch, 2005). The proliferation and differentiation of chondrocytes is regulated by a variety of systemic factors (such as progress hormone, thyroid hormone, estrogen and cortisol) and a large quantity of nonetheless poorly understood locally secreted factors (such as Indian hedgehog, parathyroid hormone-related peptide, fibroblast development factors) which act on receptors to impact intracellular signaling and activation of chondrocyte-selective transcription factors (Mackie et al. The mineralization process therefore requires adequate provide of substrates, calcium and phosphate, which are provided by calcitriol (1,25 dihydroxy vitamin D) through intestinal absorption. The mineralization standing of the bone matrix can be assessed by quantitative backscattered electron imaging and normative information on mineralization density distribution in iliac bone biopsies can be found (Fratzl-Zelman et al. Modeling allows for bone progress in width by deposition of recent bone on the periosteal floor by osteoblasts and resorption of old bone on the endosteal floor by osteoclasts (Rauch, 2007). Modeling permits for change in form of bones in response to physiologic influences and mechanical forces (Frost, 1990). Remodeling is the method by which old bone is changed by new bone, important for sustaining bone energy and elimination of microcracks (Clarke, 2008).
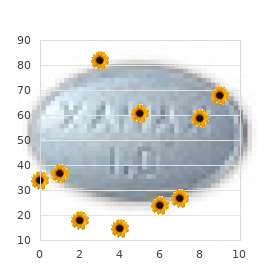
Myambutol: 800 mg, 600 mg, 400 mg
Purchase 600mg myambutol free shippingIn distinction virus 72 hours buy generic myambutol 800mg on line, adult research confirmed reversible cognitive decline and loss of mind function with normalization of cortisol levels (Merke et al antibiotics for sinus infections in adults myambutol 800 mg on-line. In our collection antibiotics that start with c discount myambutol 600 mg without prescription, 5/21 patients (24%) had long-term psychiatric comorbidities which included cognitive dysfunction antibiotics quick reference generic 400mg myambutol mastercard, melancholy and temper disturbance (Yordanova et al. A cautious detailed historical past and a formal investigation protocol requiring hospitalization is necessary to make a safe prognosis. A specialized multidisciplinary method to define the optimal therapeutic strategy is essential. Posttreatment management might pose difficulties in optimizing growth, physique composition and puberty. Additionally, additional studies are warranted to establish novel genetic defects related to pituitary corticotroph cell tumourigenesis and to assess the efficacy of new medical therapies and surgical approaches. An evaluation of petrosal sinus sampling for localization of pituitary microadenomas in youngsters with Cushing illness. European journal of endocrinology/European Federation of Endocrine Societies 166, 1101�1105. Endoscopic versus microscopic trans-sphenoidal pituitary surgical procedure: A systematic evaluation and meta-analysis. Quality of life in youngsters and adolescents 1-year after remedy of Cushing syndrome: A prospective examine. Effects of child- and adolescent-onset endogenous Cushing syndrome on bone mass, physique composition, and progress: A 7-year prospective study into younger adulthood. Quality of postoperative course in kids: Endoscopic endonasal surgical procedure versus sublabial microsurgery. Children expertise cognitive decline regardless of reversal of mind atrophy one year after resolution of Cushing syndrome. Neuroendocrine disorders in children (Chapter 17)-Cushing disease: Diagnosis and management (ebook). Pituitary macroadenoma in a 5-year-old: An early expression of multiple endocrine neoplasia sort 1. Granulosa cells Cells that provide vitamins to the creating oocyte in the ovary and have a perform analogous to that of the Sertoli cells in the testis. Leydig cells Testosterone-producing cells positioned adjacent to the seminiferous tubules within the testis. Sertoli cells Somatic supporting cells within the seminiferous tubules of the testes to which spermatids connect until they type spermatozoa. Testis cords Specialized tubular buildings that enclose and protect germ cells from external alerts, help their growth into mature spermatogonia, and eventually channel them into the male reproductive tract. Theca cells Endocrine cells associated with ovarian follicles that produce the androgen substrate required for ovarian estrogen biosynthesis. Sex Determination the gonads are reproductive organs that operate to produce gametes and intercourse hormones. As a results of this distinctive function, gene mutations that disrupt gonad improvement not solely result in defects in gonadal formation or perform, but also can result in sex reversal. The bipotential gonad develops through thickening and proliferation of the coelomic epithelium alongside the mesonephros, giving rise to the somatic cells of the gonad (Karl and Capel, 1998). A thickening of the coelomic epithelium of the mesonephros (gray) around E10 permits growth of the bipotential gonad (yellow). Primordial germ cells (green) migrate from the hindgut into the genital ridge and populate the gonads between E9. The steroidogenic Leydig cells (blue) in the testicular interstitium start to differentiate round E12. In contrast, during ovarian development, regulated by Rspo1 and Wnt4, no apparent morphological adjustments are observed until the entry of germ cells into meiosis between E13. In mice, the expression of Sry and Sox9 enables the proliferation of coelomic epithelial cells (Schmahl et al. In parallel, male-specific vasculature develops from vascular endothelial cells that migrate from the mesonephros into the gonad (Brennan et al. The steroidogenic fetal Leydig cells then differentiate within the interstitial spaces between testis cords from E12. Other occasions, such as differentiation of the somatic granulosa cells and growth of the primordial follicles, happen just previous to start (Ross and Capel, 2005). In addition, Forkhead field L2 gene (Foxl2) is a transcriptional regulator required for granulosa cell function. For instance, overexpression of b-catenin (Ctnnb1), a Wnt signaling part, inhibits the male pathway (Maatouk et al. It has also been shown that Foxl2 actively prevents transdifferentiation of the ovary into a testis (Uhlenhaut et al. These antagonistic interactions between the male and female pathways are exemplified by intercourse reversal phenotypes ensuing from the achieve or loss of perform of the above-mentioned genes. Sex Differentiation Sex differentiation refers to the progressive acquisition of male or feminine traits within the genital tract and external genitalia. Once sex is determined, subsequent gene expression within the Leydig cells provides rise to testosterone manufacturing, which leads to the male sexual phenotype. Before intercourse differentiation has occurred, both male and female reproductive ducts are current in the creating embryo. Through the motion of testosterone, the male-specific Wolffian duct develops into the epididymis, vas deferens, and seminal vesicles. Similarly in the female, subsequent estrogen synthesis from the theca cells leads to the feminine sexual phenotype. Disorders of Sex Development Sex willpower and differentiation are tightly regulated by genetic pathways involving several transcription components and signaling molecules. Perturbations during sex dedication can lead to defects in early gonad formation, whereas disruptions of sex differentiation might affect improvement of the inner and/or exterior genitalia and different secondary sexual characteristics. Patients and their households are often traumatized by the uncertainty of gender, and the accompanying psychosexual consequences and attainable surgical interventions. Current approaches to prognosis involve anatomical, imaging, and endocrine analysis. Together with gain-of-function and loss-of-function research in mouse fashions, the roles of these genes within the control of gonadal development and endocrine function have been outlined. It capabilities as a signaling molecule required for the regression of the M�llerian ducts in male embryos which might in any other case differentiate into the uterus and fallopian tubes. Other related circumstances embrace X-linked lissencephaly with ambiguous genitalia, epilepsy, Proud syndrome (agenesis of the corpus callosum with abnormal genitalia and intellectual disability), and Partington X-linked mental retardation syndrome (Kitamura et al. In mice, Dhh regulates differentiation of Leydig cells and peritubular myoid cells to allow normal development of the testis cords (Clark et al. Dhh knockout mice develop testes with abnormal peritubular tissue and severely restricted spermatogenesis. Dmrt1 prevents the transdifferentiation of male-specific Sertoli cells into female-specific granulosa cells by antagonizing the feminine sex figuring out factor Foxl2 in the postnatal testis (Matson et al. Phenotypes embrace full gonadal dysgenesis, presence of M�llerian structures, feminine or ambiguous exterior genitalia, and cryptorchidism.
Cheap 800mg myambutol otcHowever bacteria in florida waters order myambutol 800mg without a prescription, primarily based on present data antibiotic resistance of helicobacter pylori in u.s. veterans purchase 600 mg myambutol overnight delivery, expert surgery at an early age virus movie cheap myambutol 400 mg visa, somewhat than hormonal therapy can antibiotic resistance kill you cheap myambutol 600mg online, appears to be advisable. The epidemiologic proof linking prenatal and postnatal publicity to endocrine disrupting chemicals with male reproductive problems: A systematic evaluation and meta-analysis. Germ cell apoptosis after therapy of cryptorchidism with human chorionic gonadotropin is associated with impaired reproductive function in the grownup. Growth of spontaneously descended and surgically handled testes throughout early childhood. Occurrence of testicular most cancers in sufferers operated on for cryptorchidism and inguinal hernia. Testicular dysgenesis syndrome: An more and more widespread developmental disorder with environmental features. Management of undescended testes: European Association of Urology/ European Society for Pediatric Urology Guidelines. The reaction consists of three hydroxylations of the 19 methyl group of the androgen molecule with the simultaneous elimination of the methyl group that results in the formation of a benzene ring. Congenital adrenal hyperplasia Group of steroidogenic issues that impair cortisol biosynthesis. Disorders of sexual development Congenital conditions in which chromosomal, gonadal, or anatomical intercourse is atypical. Hypospadias Disorder of the anterior urethral and penile improvement by which the urethral opening is ectopically positioned on the ventral aspect of the penis. Osteopenia A skeletal situation characterized by a decreased bone mineral density in comparison with the reference normal (between � 1 and � 2. Osteoporosis A skeletal situation characterised by a decreased bone mineral density compared with the reference standard (under � 2. Polycystic ovary syndrome Disorder characterized by hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology. This has contributed considerably to the understanding of cP450arom exercise in several tissues, influencing sexual differentiation, patterns of gonadotropin secretion by the hypothalamic�pituitary axis, reproductive capacity, lipid metabolism, insulin sensitivity, and skeletal maturation and development. Studies of aromatase deficiency in people have been complemented with studies in mouse knockout fashions that demonstrated the role of estrogens in a quantity of tissues. In this text, molecular research, the scientific phenotypic variations throughout life in both sexes, gonadal operate, fertility, and gender identification are addressed. Characteristics of cP450arom cP450arom is the enzyme that catalyzes the synthesis of estrogens from androgens. Therefore, the exercise of this enzyme advanced impacts each androgen metabolism and estrogen synthesis. The biological importance of the aromatase complex is said not only to its function in the synthesis of estrogens, but additionally to its potential influence on the stability of the androgen�estrogen ratio in numerous tissues. In the Eighties, the human aromatase protein was purified from placental microsome and the aromatase activity was demonstrated by conversion of androstenedione to estrone (Pasanen and Pelkonen, 1981; Mendelson et al. The aromatase Encyclopedia of Endocrine Diseases, Second Edition, Volume 5 doi:10. Several promoters are discovered within a 90-kb area upstream of the coding region related to a quantity of first exons that are concerned in tissue-specific expression. The three-dimensional crystal construction of human aromatase was recognized with purified aromatase protein extracted from placental microsome (Ghosh et al. The human aromatase consists of a heme group and a polypeptide chain of 503 aminoacid residues and exhibits excessive substrate specificity in catalyzing the synthesis of estrogens from androgen precursors. The most highly conserved area consists basically of a four-helix bundle, two sheets, and the heme-binding region (Graham-Lorence et al. Thus, a strict management over tissue-specific expression is necessary for correct regulation of estrogen synthesis during fetal development, as nicely as during postnatal life. The human placenta (syncytiotrophoblast layer) is able to aromatizing massive quantities of androgen precursors produced by the fetal and maternal adrenal glands into estrogens. The fee of estrogen production and the level of circulating estrogens improve markedly throughout being pregnant. Following fertilization, concentrations of 17b-estradiol increase steadily to a spread of 6�30 ng/mL at time period (Tal et al. This enzyme protects the fetus from virilization even in the presence of large quantities of aromatizable androgens. One of the scientific signs of aromatase deficiency could manifest throughout being pregnant, as a pregnant mother of an aromatase-deficient fetus turns into virilized (see later). Human Aromatase Deficiency 529 Reported Human Mutations Since aromatase deficiency was first described by Shozu et al. Tables 1 and a pair of describe the molecular defects, in-vitro aromatase activity of mutants, and clinical phenotype in female and male aromatase-deficient subjects, respectively. Variations in phenotype are in contrast with in-vitro practical derangements of mutants. Data reported recommend some genotype�phenotype correlation as decrease cP450arom activity was associated with a more extreme phenotype. Pregnancy, the Fetus, and Newborns the energetic human placental aromatization of androgens protects the fetus against the virilizing motion of fetal androgens. In congenital aromatase deficiency, the overload of androgens may cause indicators of maternal virilization (acne, deep voice, clitoris enlargement) throughout pregnancy, and this would possibly alert obstetricians to the risk of this prognosis. In the female fetus, placental aromatization of androgens is particularly essential to avoid an effect of androgens on the differentiation of the external genitalia. In most feminine instances of aromatase deficiency described within the literature, ambiguous genitalia, with various degrees of masculinization of the external genitalia, have been reported. As expected, in all these instances, gonads had been nonpalpable and differentiation of the female internal genitalia was not affected. Milder genital manifestations, such as clitoral hypertrophy or partial fusion of the labia, have been described in 4 females (Lin et al. This phenotype would possibly characterize a placenta-specific, prenatally restricted element of aromatase deficiency occurring in utero solely. An endocrinological profile has been described in some feminine circumstances with aromatase deficiency through the first month of postnatal life. Low estrogen levels along with excessive androgen ranges were discovered in the twine serum and serum androgen levels returned rapidly to normal after delivery in some instances (Shozu et al. Normal serum testosterone ranges were reported in an affected woman of three days (Conte et al. Very excessive serum-free testosterone and androstenedione ranges at 2 weeks of postnatal life followed by a lower to the normal range through the first month of life was reported in only one affected new child boy (Delado�y et al. At 4 weeks after start, the estradiol levels were low; the androstenedione level was lowering toward the normal level for age and sex, whereas the free testosterone stage had already dropped to within the normal vary. Then, a protein with further extremely hydrophobic 29 amino acids shall be generated p. Arg435Cys: Arg435 is very conserved throughout the heme-binding area among cP450s p.
Generic myambutol 800 mg free shippingFirstly antibiotic resistance and meat order myambutol 800mg with amex, they may present as a end result of antibiotic joint replacement dental 800mg myambutol visa indicators and signs of hyperthyroidism similar to anxiousness virus movies list myambutol 800mg visa, tremor antimicrobial pillows buy myambutol 800mg without prescription, palpitations, weight reduction, heat intolerance, or increased frequency of bowel movements (summarized in Table 1). It is necessary to note that these traditional signs of hyperthyroidism may be absent within the aged (Thomas et al. Secondly, subclinical or biochemical hyperthyroidism may be detected because of Table 1 History Anxiety Fatigue Increased perspiration Heat intolerance Tremor Hyperactivity Palpitations Appetite change (usually increased) Weight loss Menstrual disturbances Note: Classic features of hyperthyroidism are sometimes absent in the elderly. Alternatively, sufferers could present because of detection of a thyroid nodule or goiter by neck palpation, ultrasonography, or as a outcome of signs suggestive of obstruction, similar to dysphagia, dyspnea, or cough. Therefore, the medical pathway for the diagnostic workup of sufferers with poisonous multinodular goiter will depend upon the presenting grievance. In all cases, clinicians should begin their assessment with a detailed history and physical examination centered on delineating indicators and signs of hyperthyroidism, obstruction, and risk elements for thyroid cancer. Physical examination of the thyroid might reveal diffuse, painless enlargement of the gland with multiple palpable nodules. Examination should also include palpation of the decrease edge of the thyroid gland and percussion over the manubrium listening for dullness, to assess for retrosternal extension of the goiter. Neck ultrasonography must be obtained to verify the location, measurement, and variety of thyroid nodules, the dimensions of the gland, and presence of lymphadenopathy. Ultrasound of the thyroid is also a vital step in threat stratification of thyroid nodules and determination of the need for nice needle aspiration biopsy. If subclinical or overt hyperthyroidism exists within the context of solitary or multiple thyroid nodules, the subsequent step is thyroid scintigraphy to decide the useful standing of the gland and related nodules. Scintigraphy also provides details about possible substernal extension of the goiter (Bahn and Castro, 2011; Becker et al. As previously mentioned, poisonous multinodular goiter is a heterogeneous situation and nodules can exhibit variable scintigraphic patterns together with normal or decreased uptake, circumscribed areas of increased uptake with suppression of surrounding thyroid tissue, or areas of elevated uptake without suppression of the encircling parenchyma. In patients without full scintigraphic suppression of the encompassing parenchyma, thyroid hormones may be administered prior to suppression scintigraphy to have the ability to differentiate autonomous from normal thyroid tissue. In iodine-deficient areas, the distinction between autoimmune and non-autoimmune types of hyperthyroidism. Treatment Management of sufferers with poisonous multinodular goiter ought to keep in mind a quantity of clinical and demographic components, in addition to affected person values and preferences. The goal of remedy is fast and lasting elimination of the hyperthyroid state and alleviation of obstructive signs. Therefore, the principle indications for remedy embrace a big goiter causing compressive symptoms or thyrotoxicosis. Subclinical hyperthyroidism has been related to larger risk of atrial fibrillation, osteoporosis, and a rise in 10-year cardiovascular mortality (Krohn et al. Medical Therapy In sufferers with severe thyrotoxicosis or those at vital danger of complications due to worsening of hyperthyroidism, pretreatment with thionamides and/or beta blockers ought to be thought of. Low dose thionamides corresponding to carbimazole or methimazole should be used as first line. Beta blockers can be used as adjunctive therapy to management adrenergic signs corresponding to nervousness, tremor, and palpitations. Prior to initiation of remedy, patients must be recommended about widespread unwanted side effects of thionamides together with pores and skin rashes (1%�5%), arthritis and uncommon however severe problems corresponding to hepatotoxicity and agranulocytosis (o0. However, long term antithyroidal drug use can be thought-about when definitive remedy is contraindicated, similar to within the elderly or those with limited life expectancy. Definitive Management Definitive therapy of poisonous multinodular goiter includes surgical resection of the thyroid gland or radioactive iodine. The risks, benefits, and alternate options of every treatment should be discussed with the affected person prior to selecting a therapy. Surgery Surgery is the preferred treatment option if quick eradication of hyperthyroidism is desired, if thyroid malignancy is suspected or confirmed, if obstructive symptoms are present due to massive goiter with mass impact, or if coexisting hyperparathyroidism exists that requires simultaneous treatment. Relative contraindications to surgical procedure for toxic multinodular goiter embody important comorbidities, limited life expectancy, and being pregnant. If surgery is chosen as the therapy for a affected person with poisonous multinodular goiter, pre-treatment with a thionamide � / � beta blockade is recommended to obtain euthyroidism, thus minimizing the chance of intraoperative and postoperative complications from hyperthyroidism. The preferred surgical process for remedy of poisonous multinodular goiter is a near-total or total thyroidectomy. Thionamides must be stopped after surgery, whereas �-adrenergic blockade ought to be slowly tapered following the operation. The Toxic Multinodular Goiter 735 Table 2 Factors influencing the choice of therapy modality for poisonous multinodular goiter Factors that favor surgical treatment Large goiter or compressive symptoms Desire for fast termination of hyperthyroidism Suspicion of thyroid malignancy Low radioiodine uptake Coexisting hyperparathyroidism requiring treatment Factors that favor radioiodine treatment Small to medium sized goiter Previously operated or irradiated neck Increased surgical threat of affected person risk of therapy failure or want for repeat therapy is o1% following near-total or whole thyroidectomy, nevertheless the risk of everlasting hypothyroidism requiring thyroid hormone alternative is 100%. Potential surgical issues embrace risk of everlasting hypoparathyroidism (o1. Although these problems are rare within the setting of experienced, excessive volume surgeons, they should be mentioned with sufferers prior to embarking with this therapy choice. Thionamides may also be used to obtain euthyroidism in patients at high danger of decompensation from worsening hyperthyroidism. If goiter volume discount is a aim of remedy, this property may be leveraged to achieve a greater discount in goiter dimension at the expense of everlasting hypothyroidism. Biochemical monitoring ought to happen each 4�6 weeks for the primary 6 months, and annually thereafter (Ross et al. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi medical guidelines for scientific apply for the prognosis and administration of thyroid nodules-2016 replace. Transient thyrotoxicosis related to acute hemorrhagic infarction of autonomously functioning thyroid nodules. Incidence of hypothyroidism occurring long after iodine-131 remedy for hyperthyroidism. Etiopathology, scientific features, and remedy of diffuse and multinodular nontoxic goiters. Clinical and biochemical modifications following 131I remedy for hyperthyroidism in patients not pretreated with antithyroid drugs. Linkage of familial euthyroid goiter to the multinodular goiter-1 locus and exclusion of the candidate genes thyroglobulin, thyroperoxidase, and Na � /I� symporter. Effects of antithyroid medicine on radioiodine therapy: Systematic evaluation and meta-analysis of randomized managed trials. Polyclonal and monoclonal thyroid nodules coexist inside human multinodular goiters. High incidence of multinodular toxic goiter in the aged population in a low iodine intake area vs. Prophylactic software of thyrostatic drugs during extreme iodine publicity in euthyroid sufferers with thyroid autonomy: A randomized study. Natural heterogeneity of thyroid cells: the basis for understanding thyroid operate and nodular goiter growth. The use of fine-needle aspiration biopsy underneath ultrasound steering to assess the risk of malignancy in patients with a multinodular goiter. Thyroiditis, Infectious and Subacute Grigoris Effraimidis, Copenhagen University Hospital, Copenhagen, Denmark Ulla Feldt-Rasmussen, Copenhagen University Hospital, Copenhagen, Denmark r 2017 Elsevier Inc. Glossary Genetic susceptibility Heritable trait primarily based on histocompatibility genes. Fine needle aspiration biopsy Aspiration of the contents of a thyroid nodule for diagnostic evaluation.
Diseases - Nivelon Nivelon Mabille syndrome
- Thrombocytopenic purpura, autoimmune
- Ulna and fibula absence with severe limb deficit
- Koone Rizzo Elias syndrome
- Moeschler Clarren syndrome
- Spastic paraplegia type 3, dominant
- Megacystis microcolon intestinal hypoperistalsis syndrome
Order 400mg myambutol visaThyroid perform and mental development of infants nursed by mothers taking methimazole ardis virus purchase 600 mg myambutol free shipping. Effect of long-term continuous methimazole therapy of hyperthyroidism: Comparison with radioiodine virus research quality myambutol 800mg. Antineutrophil cytoplasmic antibody-positive small-vessel vasculitis associated with antithyroid drug remedy: How vital is the clinical drawback Sources of circulating 3 antimicrobial washcloth purchase 400mg myambutol mastercard,5 antibiotic quality premium buy 400mg myambutol fast delivery,30 -triiodothyronine in hyperthyroidism estimated after blocking of kind 1 and kind 2 iodothyronine deiodinases. Radioactive Iodine Barbara Jarzab and Jolanta Krajewska, Maria Sklodowska-Curie Memorial Institute - Cancer Center, Gliwice, Poland r 2018 Elsevier Inc. Glossary Differentiated thyroid cancer the most common endocrine malignant neoplasm arising from the follicular thyroid cell, which reveals thyroid differentiation features. Introduction Iodine plays an important role for normal functioning of the thyroid gland, its homeostasis, and thyroxine (T4) and triiodothyronine (T3) production. Normal thyroid takes as much as 20%�30% of orally administered iodine, whereas in patients with hyperthyroidism this price could increase even up to 80%. Radiation Physics Only two amongst greater than 20 identified iodine radioactive isotopes are utilized in a day by day clinical follow: I-123 for diagnostics and I131 for each diagnostics and treatment. Therefore I-131 administration, notably its lower activity in kids is disputable. Franklyn, Iodine, Radioactive, In Encyclopedia of Endocrine Diseases, edited by Luciano Martini, Elsevier, New York, 2004, Pages 100�102. Thyroid scanning permits visualization of the thyroid gland and functioning thyroid tissue elsewhere within the body, identifying the rationale of hyperthyroidism, and evaluating thyroid enlargement and performance of thyroid nodules. Radioactive Iodine in the Treatment of Thyroid Disease Benign Thyroid Disease (Allahabadia and Franklyn, 2004; Stokkel et al. Radioiodine doses used within the treatment of toxic or unhazardous nodular goiter have been already empirically established. The recommended absorbed radiation dose used in the therapy of toxic and nontoxic nodular goiter ranges between 100 and one hundred fifty Gy, requiring about three. In sufferers with autonomous nodules the really helpful absorbed radiation dose is 300�400 Gy. While larger absorbed doses, ranged between 200 and 300 Gy, are required for complete ablation of thyroid tissue. Some patients, significantly those with uncontrolled hyperthyroidism and large goiter, could develop thyroid storm. Autoimmune thyroiditis may be not often observed in sufferers with autonomous nodule or poisonous goiter (Stokkel et al. Another important concern is the danger of radiation-induced neoplasms, among them leukemia, breast, urinary bladder, and colon most cancers (Brown et al. A relative threat of the development of radiation-induced leukemia is approximately 2. Some specialists also recommend 3-month ready period for males to keep away from any potential transient chromosomal abnormalities. The use of dopaminergic brokers may be helpful to lower breast publicity in recently nursing women, nevertheless the danger of significant side-effects associated to their administration to suppress lactation ought to be considered. It is worthy to be thought of that antithyroid medication protect thyroid towards ionizing radiation. In uncommon cases, when antithyroid medication or surgery are contraindicated I-131 could also be given underneath the duvet of steroids and b-blockers. The danger of second major malignancies as much as three many years after the treatment of differentiated thyroid cancer. Radioiodine remedy of hyperthyroidism (toxic goiter, hyperfunctioning nodule) and non-toxic goiter: Procedures and guidelines. Thyrotoxicosis Factitia Fausto Bogazzi and Enio Martino, University of Pisa, Pisa, Italy r 2018 Elsevier Inc. The time period "thyrotoxicosis factitia" describes thyrotoxicosis due to the voluntary and surreptitious ingestion of extra thyroid hormone(s). The ingested thyroid hormone is most frequently represented by thyroxine (T4), however triiodothyronine (T3) or a combination of those two hormones (T4 and T3) may be the product answerable for the occurrence of this syndrome. Thyrotoxicosis factitia ought to be distinguished from iatrogenic thyrotoxicosis, which is said to extreme doses of thyroid hormones erroneously given by the doctor or inadvertently taken by the patient (Table 1). Thyrotoxicosis factitia is normally noticed in psychiatrically disturbed sufferers. By voluntarily inducing thyrotoxicosis, they often seek consideration of their partners to their "sickness. The main psychopathological disturbances range from anorexia to depression, anxiety panic dysfunction, or phobic disorders. Acute schizophrenia like psychosis has been reported as major clinical manifestation of thyrotoxicosis factitia in few circumstances. Patients with thyrotoxicosis factitia usually deny the deliberate assumption of extra thyroid hormones. The age of these sufferers seems to have been growing throughout latest many years (Bogazzi et al. Patients might complain of tachycardia, tremors, loss of weight, increased perspiration, warmth intolerance, excessive nervousness and nervousness, increased bowel activity and/or insomnia. Thyroid ache and tenderness, commonly observed in subacute thyroiditis, are absent (Table 1). Poisoning with thyroid hormone could additionally be significantly severe, in chosen patients: the burst of enhanced, excessive sympathetic activity arising from thyrotoxicosis factitia has been proposed as a cause of Takotsubo cardiomyopathy (Tsao et al. Diagnosis Diagnosis of thyrotoxicosis factitia requires a high grade of suspicion (Rose et al. Serum thyroglobulin concentration is usually markedly lowered or undetectable in thyrotoxicosis factitia (Mariotti et al. This article is an update of Enio Martino, Fausto Bogazzi, Luigi Bartalena, Thyrotoxicosis Factitia, In Encyclopedia of Endocrine Diseases, edited by Luciano Martini, Elsevier, New York, 2004, Pages 551-553. Measurement of thyroid hormones in stool could additionally be helpful for identifying the abnormally high fecal excretion of ingested thyroid hormones, particularly, in these patients (Bouillon et al. Color move Doppler sonography of the thyroid reveals an absent elevated vascularity and normal-low peak systolic velocity regardless of the thyrotoxic state (Bogazzi et al. Under strict medical controls, a rapid enchancment within the clinical and laboratory features of thyrotoxicosis is regularly noticed after hospital launch until reasons for surreptitious thyroid hormone consumption are recognized. Treatment Treatment of thyrotoxicosis factitia obviously requires withdrawal of thyroid hormones. It could additionally be helpful to affiliate a short-term remedy with beta- adrenergic blocking medication to control tachycardia and tremors promptly. However, for a full recovery of the affected person, psychiatric aid or counseling is mandatory in all cases (Da Silva et al. Thyrotoxicosis factitia induces Takotsubo cardiomyopathy in end-stage renal illness: A pathogenetic hypothesis. Hemoperfusion Experimental strategy of filtration of blood by way of extracorporeal special filters or adsorbents to take away extra thyroid hormone. Sick euthyroid syndrome A state of altered thyroid function tests in response to systemic illness without major thyroid pathology.
Generic myambutol 600 mg lineIn 1985 he joined the staff of the Ghent University Hospital; he headed the division of Endocrinology from 2003 to 2014 and the Laboratory for Hormonology from 1995 to 2014 antibiotic 127 discount 800 mg myambutol visa. In 1986 he moved to the University of Catania to the Chair of Andrology and Endocrinology antibiotic kennel cough buy discount myambutol 400mg online, in 1992 to the University of Ancona infection urinaire discount myambutol 800 mg with amex, and in 2000 to the University of Padua to the Chair of Endocrinology and Chief of the Endocrinology Unit of the Department of Medicine virus 56 myambutol 600mg low cost. He has received national and international honors, together with a Doctor Honoris Causa at the Semmelweis University, Budapest, Hungary. He has authored roughly 500 peer�reviewed articles and edited a number of books and proceedings. Her basic research research concentrate on the regulation of spermatogenesis and mitochondrial derived peptides in spermatogenesis. Wang served on the Executive Council, several committees and was the President of the American Society of Andrology (2006�07). Wang has been invited speaker and distinguished lecturer at many national and worldwide endocrinology, reproductive endocrinology, and andrology conferences. Amar Hopital Europ�en Georges Pompidou, Paris, France; and Paris Descartes University, Paris, France Gisah Amaral de Carvalho Federal University of Parana, Curitiba, Brazil Ravinder Anand-Ivell University of Nottingham, Nottingham, United Kingdom Dana K. Avellar Federal University of S�o Paulo, Paulista School of Medicine, S�o Paulo, Brazil M. Barri University Hospital Quiron Dexeus, Barcelona, Spain Luigi Bartalena University of Insubria, Varese, Italy Anu Bashamboo Institut Pasteur, Paris, France Spyridon P. Chrousos National and Kapodistrian University of Athens Medical School, Athens, Greece; and Biomedical Research Foundation of the Academy of Athens, Athens, Greece Janet S. Laurent University Hospitals Leuven, Leuven, Belgium Fabio Lauria National Research Council of Italy, Avellino, Italy John H. Scherpe University of Cambridge, Cambridge, United Kingdom xl List of Contributors Stefan Schlatt Institute of Reproductive and Regenerative Biology, Mu nster, Germany Peter N. Semple University of Cambridge Metabolic Research Laboratories, Cambridge, United Kingdom Luisa M. Thornalley University of Warwick, Coventry, United Kingdom xlii List of Contributors Francisco J. Tsolakis Karolinska Institute, Stockholm, Sweden; and Karolinska University Hospital, Stockholm, Sweden Marina Tsoli National and Kapodistrian University of Athens, Athens, Greece Giovanni Tuccari University of Messina, Messina, Italy Michael L. The new Edition is a must-have one-stop reference masking every facet of the physiological background, pathogenesis, medical diagnostics, and therapeutic aspects of the big selection of endocrine and associated metabolic ailments. It additionally provides helpful information for the lay public about normal and abnormal functions of hormones. The Encyclopedia is meant to serve as a helpful and comprehensive supply of data spanning the many and diversified features of the endocrine and metabolic system. Each article begins with a glossary record defining key terms which might be unfamiliar to the reader and are necessary for understanding the article. The primary textual content is followed by referenced citations to present the reader with entry to additional info on the topic, and cross-references lead the reader to related entries within the encyclopedia. The fifth volume is a stand-alone compilation of all articles on pediatric endocrinology. Nevertheless, to deliver a major reference work with such a broad scope from initial conception to ultimate publication involved quite lots of planning and organization, together with the efforts of innumerable individuals. Hence, the Second Edition contains to a large extent completely new info, or no less than the fluency of all texts has been scrutinized. We also note that as may be anticipated for a large multi-author compilation the individual articles do differ in detail and approach. Most of the enhancing work of the Encyclopedia has been carried out by a highly competent board of 16 Section Editors, each of them internationally renowned consultants of their respective area inside scientific endocrinology. This has made the task of the Editor in Chief easy, primarily entailing the supervision of smooth progress of the project. Clayton (United Kingdom, pituitary gland), Jean-Louis Chiasson (Canada, diabetes), Sophie Christin-Maitre (France, feminine reproduction), Wouter W. The Elsevier editorial workers, Will Smaldon, Laura Escalante Santos, and Kate Miklaszewska-Gorczyca, have been of monumental help to the editors at every step throughout this lengthy project. I admire the professionalism of everybody and am deeply indebted to all for their dedication and onerous work to make the Encyclopedia the leading reference book of scientific endocrinology. The authors of the person chapters, more than 450 in whole, were specifically selected by the Section Editors to symbolize the most effective obtainable information on the subject out there. Hence the decision to commit a standalone volume to the topic in this second version of the Encyclopedia. In the first edition, topics corresponding to congenital hypothyroidism, delayed puberty, and Turner syndrome had been scattered all through the encyclopedia based mostly on utilizing an alphabetical system. Growth, puberty, and disorders of sex development are utterly throughout the purview of the pediatric endocrinologist and are lined intimately in this volume. Thereafter, chapters are extra organ-specific (thyroid, adrenal, pituitary) and paired as regards to additional related info in the cognate grownup chapter. A few topics are lacking, similar to rarer adrenal enzyme deficiencies however specifically, matters rela ted to pediatric diabetes. Some features are lined within the adult diabetes part, but this omission shall be rectified in the end by posting some chapters on line using the Reference Module system. I acknowledge the support of the Editor in Chief, Ilpo Huhtaniemi, for allowing me the freedom to compile this volume, the authors for their glorious contributions, my fellow Section Editors for his or her prepared collaboration, and the aforementioned Elsevier employees for their steering and persistence. Introduction A favorable in utero surroundings facilitating sufficient fetal growth is crucial, not just for fetal and neonatal wellbeing, but additionally as a determinant of long term health. In the absence of different dependable measures, evaluation of fetal growth has been the mainstay of fetal monitoring for over one hundred years. Over the last forty years, ultrasound evaluation has been established because the gold normal technique for monitoring fetal development. Initially, assessment of fetal development consisted of fetal biometry and calculation of an estimated fetal weight (via any one of a selection of accepted formulae), with a comparability of those parameters to revealed longitudinal nomograms. The dilemma, that partly stays to today, is distinction of the pathologically growth restricted fetus, failing to meet its genetic development potential, from the physiologically small fetus. Fetal Doppler has turn into ubiquitous as a monitoring device in fetal progress restriction, with abnormalities in circulate velocity waveforms from a quantity of fetal vessels being employed as triggers for delivery within the context of the untimely and development restricted fetus. However, even small fetuses with regular Doppler indices are at increased threat of requiring operative delivery during labour, when compared to appropriately grown fetuses (Danielian et al. Furthermore, inside a cohort of appropriately grown fetuses, imply birthweights and birthweight centiles are considerably lower in infants that develop signs of compromise in labour (Prior et al. Control of Fetal Growth Fetal growth is influenced by genetic, environmental and hormonal influences. It is beyond the scope of this text to describe all of those influences intimately, and as an alternative will briefly discuss endocrine controls. Metabolically insulin is an anabolic hormone, and its influence on fetal development is clearly evidenced by the elevated fetal development observed in fetuses of diabetic mothers. Deficiency of insulin, as would be anticipated, results in fetal growth restriction (Fowden et al.
Myambutol 800 mg overnight deliveryGonadal maldevelopment as danger issue for germ cell most cancers: Towards a medical choice mannequin antimicrobial zeolite and its application myambutol 800mg on-line. The long-term followup of 33 circumstances of true hermaphroditism: A 40-year expertise with conservative gonadal surgery virus 68 affecting children discount myambutol 600 mg otc. Gender assignment the decision-making process involved in declaring a new child a "boy" or "lady bacteria jacuzzi buy myambutol 800mg line. Gender id the essential sense of being a woman or boy antibiotic resistance cdc purchase myambutol 800 mg visa, lady or man, or a different class of gender, corresponding to a hermaphrodite or a trans(gender). Gender reassignment the decision-making process involved in revising the unique task decision later, which can occur at any age of the individual. Gender-role conduct All behaviors by which the genders differ in a given time and place. Some examples are rough- and-tumble play of childhood, courtship and sexual behavior in adolescence, and aggression and parenting behavior in adulthood. Gender-role id the diploma to which a girl or boy, or a lady or man, perceives herself or himself as being feminine or masculine. Sexual orientation the degree to which an individual erotically responds to male or feminine intercourse partners, as reflected in romantic/erotic points of interest, fantasies, dreams, and likewise in overt sexual conduct, often rated on the 7-point Kinsey scale ranging from 0 (exclusively heterosexual) to 6 (exclusively homosexual). Gender Assignment Policies Introduction In most newborns, gender task is unproblematic and instantaneous. The new child is assigned to the gender that corresponds to the appearance of the genitalia, and the vast majority of people will develop a steady gender identity commensurate with the original task. The medical categorization of somatic sex must be distinguished from the growing use of identity labels or legal phrases for gender categories aside from the normal male or female. In patients with intersexuality, the decision relating to gender project is complex, may require a variety of medical checks to establish the purpose for the problem, and involves prognostic concerns and value judgments. Meyer-Bahlburg, Gender Assignment and Psychosocial Management, In Encyclopedia of Endocrine Diseases, edited by Luciano Martini, Elsevier, New York, 2004, Pages 125-134. The assumption under this coverage was that the true sex is revealed by a definitive, single organic criterion. In cases of genital ambiguity, Aristotle had already really helpful basing the choice on the "predominant intercourse. The Optimal-Gender Policy On the basis of a critical examination of the true-sex coverage and studies of the general psychosocial end result and high quality of lifetime of intersex patients, John Money and the Hampsons at Johns Hopkins Hospital in Baltimore, Maryland, formulated an optimalgender policy in the course of the Nineteen Fifties (Meyer-Bahlburg, 1998). Therefore, the new child with intersexuality should be assigned to that gender that allows the optimal psychosexual and psychosocial functioning when all out there medical remedy choices are taken into consideration. So, in distinction to the query of the true-sex policy-"Is this a boy or a girl" Another consequence was the recommendation of early feminizing or masculinizing surgery of the external genitalia so that their appearance would be as much like the gender norm as potential and would due to this fact not intrude with gender-typical rearing conditions and body-image improvement. These pointers have been intended to stop the dad and mom from growing chronic doubts concerning the gender of their baby and to shield the kid from stigmatization by other folks, however have regularly led to parental attempts of stopping the disclosure of particulars of the medical historical past to the intersex youngsters themselves, generally even after they attained maturity. The True-Brain-Sex Policy Increasingly because the mid-1990s, the optimal-gender policy has come underneath criticism. One reason is that also underneath this policy some people turn out dissatisfied with their assigned gender and may search gender reassignment, which is made tougher if the exterior genitalia have been operated on to be more suitable with the originally assigned gender. A second argument is that, even without later gender change, genital surgery carries a risk of harm to sexual functioning in adolescence and maturity (see below). Third, the optimal-gender policy is blamed (although unjustly attributed to its authors; see above) for keeping the medical information secret, particularly from the affected person him- or herself, which contributes to the upkeep of the social stigma of intersexuality and thereby to a adverse self-image and disgrace of the intersexed particular person. Many intersex activists, therefore, argue for early complete disclosure of their medical history to intersex patients. Because of those data, some organic determinists counsel that the decisive issue for gender identification formation is the prenatal androgenization of the mind and that psychosocial elements have solely a secondary position. If such a "true-brain-sex coverage" is legitimate, gender task selections ought to be based on the degree of androgenization/masculinization of the mind, and minimization of obstacles to socialization is unimportant. Policy Effects on Gender Assignment the three major insurance policies outlined above may lead to quite diversified choices on gender assignment. According to the true-sex policy, case (1) must be raised feminine due to the clearly female histology of the gonads. Under the optimalgender coverage, case (1) can be assigned to the female gender, as a outcome of the external genitalia may be feminized in order to allow coitus and to thereby retain the choice of conception and being pregnant, as a end result of the interior feminine reproductive organs are intact. Some activists advocate assigning the intersex baby to the gender that appears to offer the more promising outcome, however to accomplish that provisionally and to consider from the outset the potential of later gender change and due to this fact to not operate on the genitals before the age of consent, except medically essential. The Status of the Evidence In response to the increasing controversies, an international consensus conference was held in Chicago in 2005, which reviewed the prevailing data and began a cautious modification of the predominant policy (Hughes et al. A definitive consensus a couple of new administration coverage has but to emerge (Lee et al. The main problem is inadequate data regarding the long-term psychological consequence. Patient-initiated later gender change, for instance, can be noticed in intersex people in each instructions, from male to feminine and from feminine to male (and, in some instances, from the assigned gender to "intersex" or another time period outdoors the standard binary sex/gender system). Given the psychological, social, and medical issues which may be associated with later gender change, clinicians usually favor a coverage that minimizes its occurrence. Thus, long-term followup knowledge are needed that can allow clinicians to state the relative frequency of gender change of patients with a given syndrome and degree of severity who had been managed beneath a defined coverage and in a particular cultural context. Because gender change can happen as late as in midlife, follow-up research must reach no less than into that age range. As an extreme example, think about the query of gender reassignment in chromosomal males with traumatic loss of the penis in infancy (Meyer-Bahlburg, 2005). One such case, by which reassignment to female at 17�21 months of age was followed by patient-initiated re-reassignment to male in adolescence, has drawn enormous consideration among care suppliers in addition to in the media, as quickly as his unfortunate story was investigated and printed, when he was in his mid-30s. However, just one other case with a historical past of traumatic loss of the penis in infancy and reassignment to female has been adopted into adulthood and printed and this individual continues to stay as a girl without gender dysphoria. The true-brain-sex policy seems very believable at first glance, but turns into extra problematic on nearer scrutiny (MeyerBahlburg, 2013). The assumption that the consequences of prenatal hormones on the mind are the decisive biological factor within the development of gender and subsequently the most effective criterion for gender task is primarily derived from analysis on the sexual differentiation of mind and behavior in nonhuman mammals, particularly rodents, which has yielded a quantity of neuroendocrine models of the sexual differentiation of brain and behavior. In common, the ensuing knowledge permit the preliminary conclusion that efficient prenatal androgens are indeed associated with the masculinization of gender-role habits. Outcome data are additionally unsatisfactory with regard to the question of impairment of sexual functioning after gender-confirming genital surgery. Most surgical consequence reports are limited to anatomical knowledge and appearance ratings. As a bunch, they show impaired sexual and genital functioning, presumably each despite corrective genital surgery and due to it (for references, see MeyerBahlburg, 2014). But surgical methods have undergone many adjustments since then and discount of the clitorophallus quite than excision has become the norm. However, how can one determine in a new child whether and to what extent the brain was prenatally masculinized and/or defeminized
Order 400mg myambutol with mastercardUnder androgen stimulation in the male fetus infection of the cervix buy 800 mg myambutol overnight delivery, the urethral folds antibiotics for moderate acne cheap myambutol 400 mg with amex, genital tubercle and genital swellings give rise to corpus spongiosum and primitive urethra antibiotic resistance video cheap myambutol 800 mg without a prescription, phallus antibiotics in milk cheap myambutol 600 mg otc, and scrotal swellings respectively. After testis willpower, hormones produced by the male gonad induce the differentiation of internal and external genitalia acting on their particular cognate receptors. The inguinoscrotal part, occurring between 27 and 35 weeks, is essentially mediated by androgen motion. Most evidence indicates that ovarian differentiation occurs independently in a number of lineages including supporting cells and germ cells. In the absence of both testosterone secretion or 5a-reductase exercise, bipotential external genital buildings develop along female strains. Specifically, in the absence of androgens the labioscrotal and urethral folds form the labia majora and minora, respectively. The genital tubercle develops into a clitoris and the urogenital sinus offers rise to the urethral opening and anterior portion of the vagina. Positive aspects about having a term providing for scientific accuracy inside a organic and medical context include: (1) bona fide genetic problems Encyclopedia of Endocrine Diseases, Second Edition, Volume 5 doi:10. At the identical time, this terminology avoids confusion by distinguishing these genetic situations from particular person variation in gender identification and sexual orientation (Barthold, 2011; Hughes et al. This broad category, created in the course of the 2005 Intersex Consensus convention, was proposed to replace beforehand used terms including the term intersex, ambiguous genitalia, and the hermaphroditism classes (Houk et al. While these latter classes have been based upon anatomic definitions, they carried connotations regarding gender and sexual conduct. Because the trigger is androgen excess, the inner genitalia are expected to be feminine. This category includes both isolated unilateral and bilateral cryptorchidism and hypospadias, that are associated with other reproductive system developmental problems. Nonhormone issues corresponding to peno-scrotal transposition have been included underneath this classification. This includes two main classes of gonadal maldevelopment: Turner syndrome and Klinefelter syndrome and their variants. Once a particular analysis is confirmed, the patient may be described by the particular analysis. In spite of the makes an attempt to be conscious and respectful, this newer classification has been criticized for stigmatizing and unnecessarily "medicalizing" these with intersex traits. Nonetheless, this classification scheme supplies the framework to information the initial diagnostic analysis of particular person sufferers. With growing knowledge accrues of the molecular foundation of disorders of intercourse differentiation/development, larger clarity will happen (Lee et al. In the past, comparable discomfort led to the overly simplistic and dogmatic administration strategy, particularly gender assignment, whereby sexually ambiguous infants have been assigned a gender based mostly on a prescriptive algorithm. These rules concerned potential for fertility and conventional sexual activity given attainable surgical genital repair. The start prevalence of genital anomalies could additionally be as high as one in 300 births however the birth prevalence of complicated anomalies of true genital ambiguity on skilled examination could additionally be as little as one in 5000 births (Ahmed et al. When evaluating these infants, the scientific features of the exterior genitalia that require examination embrace the symmetry of the external genitalia, presence of gonads in the labioscrotal folds, the fusion of the labioscrotal folds, the dimensions of the phallus and the site of the urinary meatus on the phallus, though the real site of the urinary meatus could, generally, solely turn out to be clear on surgical exploration. This will avoid unnecessary detailed investigations into boys with isolated glanular or mid-shaft hypospadias and boys with an unilateral inguinal testis. However, investigations are usually indicated with the co-existence of a systemic metabolic disorder, related malformations or dysmorphic options, a household historical past of consanguinity, stillbirths, multiple miscarriages, fertility issues, genital abnormalities, hernias, delayed puberty, genital surgical procedure, unexplained deaths, and the necessity for steroid replacement. The external genital look may be similar for a masculinized female newborn and an undervirilized male newborn, though the former is symmetrical and the latter could additionally be asymmetrical. An acceptable hospital setting is very important for the delicate management of advanced situations with full entry to the mandatory medical, nursing and psychological care. Whilst the reason of the analysis to the patient and the family is crucial, this must be carried out sensitively and carefully and expert psychological enter is essential. Mayer�Rokitansky�Kuster�Hauser syndrome Failure of attempted sexual activity 1. And, if attainable, a particular etiology may be identified, so that, together with the mother and father, an applicable gender task can be made. Parents have to be offered info regarding reproductive system differentiation so they can understand how ambiguity could happen (Indyk, 2017). One can share the idea that particular genes direct reproductive system development. Changes in these genes alter the perform of the genes and the proteins encoded by these genes. Together with the group of experts, the dad and mom will take part within the decision-making relating to gender assignment. Full disclosure and training ought to present the dad and mom with a perspective that their child, with cautious ongoing care, could be anticipated to have a great quality of life. It have to be considered that androgen exposure to the developing fetal mind impacts features of sexual identification, most clearly gender function habits as manifest by childhood play preferences, but less clearly effects upon each gender id and sexual orientation. Hence, while extent of fetal androgen exposure must be thought of, this still represents an unknown issue within the development of a gender identification with the future chance of a gender id that differs from the intercourse of rearing (Lee et al. The subjects of biological sex, sex of rearing, and gender identification must be discussed with the mother and father (Wilson et al. The rationale for that is that the ovaries and uterus have the potential for regular operate so with applicable medical remedy and surgical development, fertility and sexual perform could be expected. An exception to this task ought to however be considered when exterior genital development is totally male, besides of an empty scrotum. Such individuals raised as males have gender identity and sexual orientation typical for most males, require much less surgical procedure and function socially and sexual as males, albeit with infertility (Mieszczak et al. Assignment as female is at present considered a drastic step, based upon consequence information including gender improvement contrary to assignment and self-reassignment of gender. In these situations, intercourse of rearing needs to be rigorously thought of with the mother and father. Those with partial androgen insensitivity have to be fastidiously assessed; those with proof of androgen responsiveness are usually assigned male, whereas these with no evidence of responsiveness postnatal, feminine. A defect in 5a-reductase is an indication for male sex for rearing as a end result of pubertal virilization will result in penile growth (although it goes to be subnormal), normal pubic hair development, and the acquisition of male sexual identity. In distinction, very rarely with inborn errors of testosterone biosynthesis, if male reconstructive surgery appears to be extremely unlikely, female project could also be a consideration, if outcomes suggest that fetal testosterone secretion was markedly subnormal. When a vagina and uterus are current, feminine assignment could also be thought-about relying upon evidence of testicular testosterone secretion and extent of masculinization and chance of successful vaginoplasty. In cases of complete androgen insensitivity, feminine task is appropriate; with partial androgen insensitivity, male assignment is currently done except in these cases failing to demonstrate responsiveness to exogenous testosterone stimulation. Confirmation of a described mutation within the androgen receptor gene could additionally be helpful for management depending upon variability described for the specific mutation.
References - Dhawan V, Dhoat S, Williams AJ, et al. The range and nature of sleep dysfunction in untreated Parkinsonis disease (PD): a comparative controlled clinical study using the Parkinsonis disease sleep scale and selective polysomnography. J Neurological Sci 2006;248 (1-2):158-62.
- Warnell, P. (1991). The pain experience of a multiple sclerosis population: A descriptive study. Axone, 13(1), 26n28.
- Aletras AH, Tilak GS, Natanzon A, et al: Retrospective determination of the area at risk for reperfused acute myocardial infarction with T2-weighted cardiac magnetic resonance imaging: Histopathological and displacement encoding with stimulated echoes (DENSE) functional validations, Circulation 113:1865-1870, 2006.
- Wikstrom B, Backman U, Danielson BG: Ambulatory diagnostic evaluation of 38 recurrent renal stone formers: a proposal for clinical classification and investigation, Klin Wochenschr 61:85, 1983.
|