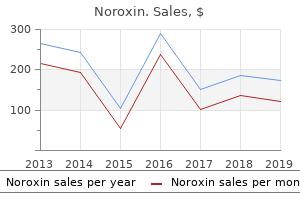
Noroxin
Marilyn Jones, M.D. - Rady Children’s Hospital
- San Diego, California
Buy noroxin 400 mg free shippingThe incidence of autoantibodies, however, will increase steadily with age, reaching a peak at around 60 to 70 years bioban 425 antimicrobial cheap noroxin 400mg online. Exogenous Factors Ultraviolet radiation, medicine, viruses, and chronic infectious disease could all play a role within the growth of autoimmune disorders infection control purchase 400 mg noroxin with amex. These components may alter antigens, which the body then perceives as nonself antigens bacteria 4 urinalysis discount noroxin 400 mg on-line. The variety of indicators and signs seen in patients with autoimmune problems displays the various types of the immune response virus 66 discount noroxin 400mg on line. It can additionally be important to notice that autoantibodies may be formed in patients secondary to tissue injury or when no proof of clinical disease exists. Unlike autoimmune issues, autoantibodies can happen as immune correlates of situations corresponding to blood transfusion reactions. In addition, autoantibodies can be demonstrated in hemolytic illness of the new child and graft rejection and can result from issues corresponding to serum illness, anaphylaxis, and hay fever when the immune response is clearly the reason for the illness. The mechanisms governing the deposition in one organ or another are unknown; nonetheless, a quantity of mechanisms may be operative in a single illness. Wherever antigen-antibody complexes accumulate, complement could be activated, with the subsequent release of mediators of inflammation. These mediators increase vascular permeability, attract phagocytic cells to the reaction site, and trigger native tissue harm. Alternatively, cytotoxic T cells can directly assault body cells bearing the target antigen, which releases mediators that amplify the inflammatory response. Autoantibody and complement fragments coat cells bearing the goal antigen, which leads to destruction by phagocytes or antibody-seeking K-type lymphocytes. An particular person may develop an autoimmune response to a big selection of immunogenic stimuli (Table 28-3). Antigens are sequestered within the organ and, because of the dearth of contact with the mononuclear phagocyte system, they fail to ascertain immunologic tolerance. Any circumstances producing a release of antigen would then provide a possibility for autoantibody formation. This situation occurs when sperm cells or lens and heart tissues are launched directly into the circulation, and autoantibodies are formed. In other ailments, only the production of autoantibodies is famous with tissue harm. These autoantibodies attack cell floor antigens or membrane receptors or mix with antigen to kind immune complexes which might be deposited in tissue, subsequently inflicting complement activation and irritation. Tolerance is the shortage of immune response to self antigens and is initiated throughout fetal development (central tolerance) by the elimination of cells with the potential to react strongly with self antigens. Peripheral tolerance is a course of involving mature lymphocytes and occurs in the circulation. Self antigens are presented by dendritic cells to self-reactive T cells that are liable for positive and negative number of particular lymphocytes. The final objective is to remove T lymphocytes that respond strongly to self antigens. Many diagnostic laboratory exams (Box 28-2) are primarily based on detecting these autoimmune responses. Common autoantibodies include thyroid, gastric, adrenocortical, striated muscle, acetylcholine receptor, easy muscle, salivary gland, mitochondrial, reticulin, myelin, islet cell, and skin. Vasculitis Deposition of circulating immune complexes is considered immediately or indirectly liable for many forms of vasculitis. The inflammatory lesions of blood vessels produce variable harm or necrosis of the blood vessel wall. This might end in narrowing, occlusion, or thrombosis of the lumen or aneurysm formation or rupture. Vasculitis occurs as a main illness course of or as a secondary manifestation of one other disease. Vasculitis is characterised by inflammation inside blood vessels, which often ends in a compromise of the vessel lumen with ischemia. Ischemia causes the main manifestations of the vasculitic syndromes and determines the prognosis. Therefore, the vasculitic syndromes are a heterogeneous group of ailments (Box 28-3). Antiendothelial antibodies are autoantibodies directed towards antigens in the cytoplasmic membrane of endothelial cells. Carditis the heart shares a susceptibility to immune-mediated injury with different organs. The consequent reaction of cardiac myocytes to immune damage can range from reversible modulation of their electrical and mechanical capabilities to cell demise. Carditis may be brought on by quite a lot of conditions, together with acute rheumatic fever, Lyme disease, and cardiac transplant rejection. Myocardial contractility may be impaired by cell-mediated injury or the native launch of cytokines. Primary idiopathic myocarditis is an autoimmune disease characterized by infiltration of the center by macrophages and lymphocytes. Studies involving the mechanisms whereby immune cells and elements localize in the myocardium, modulate myocyte perform, and remodel myocardial architecture are beneath way. A analysis of acute rheumatic fever requires differentiation from different immunologic and infectious illnesses. Patients with rheumatic coronary heart disease exhibit antimyocardial antibodies that bind in vitro to foci in the myocardium and heart valves. These antibodies may be responsible for the deposition of immunoglobulin and complement elements present in the identical area of rheumatic coronary heart disease tissues at post-mortem. Because antimyocardial antibodies are sometimes present in sufferers with a latest myocardial infarction or streptococcal an infection without cardiac sequelae, detection of those antibodies has not been a particularly helpful differential diagnostic check for cardiac damage. Collagen Vascular Disorders Progressive Systemic Sclerosis (Scleroderma) Scleroderma is a collagen vascular disease of unknown trigger that assumes numerous varieties. The development of scleroderma has been related to a quantity of occupations and with drugs similar to bleomycin sulfate, tryptophan, and carbidopa. Occupational exposure to vinyl chloride, vibratory stimuli, and silicosis have been related to the following improvement of scleroderma. Scleroderma happens in all races and is thrice extra frequent in women than men. Scleroderma is characterized by fibrosis within the skin and inside organs and by arterial occlusions with a definite proliferative pattern. The disease is slowly progressive and chronically disabling, but can be rapidly progressive and fatal. Antinuclear antibodies are fashioned in 40% to 90% of sufferers to the following: (1) extractable nuclear antigens; (2) the nucleolus; (3) the centromere; and (4) Scl-70. Activated T cells can lead to both the vascular modifications and increased collagen production in scleroderma. It is now thought that both the vascular dysfunction and fibrosis outcome from this cellular immune activation.
Purchase noroxin 400mg fast deliveryThe alarming statistics of developing renal failure after stable organ transplantation grew to become well known with landmark papers by Ojo et al43 and Gonwa et al44 over a decade ago virus 5 days of fever generic 400 mg noroxin with amex. Posttransplant continual kidney illness is mostly because of antibiotic resistance can boost bacterial fitness cheap 400mg noroxin free shipping ongoing calcineurin inhibitor nephrotoxicity and the progression of underlying medical illnesses antibiotic resistance youtube 400 mg noroxin mastercard. Unlike the candidate on long-term dialysis antibiotic resistance legionella pneumophila generic noroxin 400mg otc, these candidates generally have lengthy posttransplant programs. Thus transplant centers should face the next questions: (1) When is the recipient medically suitable for an additional transplant and immunosuppressive load? Ruiz et al49 proposed a minimal 60-day postÂliver transplant ready interval because chances of renal restoration were low. Impact of immunosuppression in liver transplantation across a optimistic crossmatch. Immunosuppressive effects of soluble cell membrane fractions, donor blood and serum on renal allograft survival. Combined transplantation of liver and kidney from the same donor protects the kidney from rejection and improves kidney graft survival. Analysis of the United Network for Organ Sharing database evaluating renal allografts and affected person survival in combined liver-kidney transplantation with the contralateral allografts in kidney alone or kidney-pancreas transplantation. There are clear indications for the process and others that still require investigation and implementation. Pulsatile perfusion reduces the risk of delayed graft function in deceased donor kidney transplants, regardless of donor kind and chilly ischemic time. Kidney transplantation after previous liver transplantation: analysis of the organ procurement transplant community database. Kidney transplantation for end-stage renal failure in Liver transplant recipients with hepatitis C viral infection. Indications for combined liver and kidney transplantation: Propositions after a 23-year experience. Liver and kidney transplantation for polycystic liver and kidney-renal operate and consequence. Cadaveric orthotopic auxiliary split liver transplantation and kidney transplantation: An alternative for kind 1 primary hyperoxaluria. Sequential liver and kidney transplantation from a single living donor in two younger adults with major hyperoxaluria sort 1. Long-term survival and renal operate following liver transplantation in sufferers with and without hepatorenal syndrome  experience in 300 patients. Estimation of glomerular filtration charges earlier than and after orthotopic liver transplantation: analysis of present equations. Glomerular filtration fee equations for liver-kidney transplantation in cirrhotic patients: validation of current suggestions. Currently greater than 50% of grafts survive 10 years or more,1 however within the absence of synthetic hepatic help, similar to dialysis for kidney failure, retransplantation remains the only option for patients with allograft failure. Indeed, advances in organ preservation, surgical strategies, immunosuppression, and antiviral remedy have doubtless all contributed to the observed decreased frequency of retransplantation. Placing a second and even third liver graft right into a patient can pose important surgical, monetary, and moral challenges. From a technical perspective the graft hepatectomy can be fraught with peril because of the development of dense adhesions. A second liver implantation can be anatomically complex and requires intensive preoperative planning for the identification of appropriate vascular inflow, which may involve the use of vascular grafts. As rising well being care expenditures invite rising scrutiny of value effectiveness, studies observe that hospital expenses are significantly higher, and the length of keep longer, for patients present process retransplantation. Of eleven,796 registrants for liver transplant on the ready record in 2011, 6056 underwent deceased donor liver transplantation, 247 underwent dwelling donor liver transplantation, and 2939 died or became too sick to transplant earlier than a liver grew to become obtainable. However, to keep away from futile transplants within the setting of limited resources, a higher emphasis is now placed on benefit derived from transplantation, with the extra give consideration to posttransplant outcomes. In this context it has become crucial to develop prognostic fashions that can aid in the number of viable retransplant candidates and in the medical management of these candidates. The relative contribution of each to retransplantation varies by institution and may be associated to how aggressive every institution is in accepting "marginal," livers in addition to how unwell the recipients are at time of transplant. Significant donor factors embody degree of steatosis within the donor allograft, elevated chilly ischemic time (>12 hours), reduced-size allograft, and older donor age (>50 years old). The mixture of those components has the potential for additive effects that may yield significantly dismal outcomes,10,11 as was discovered when marginal livers were initially utilized in critically unwell patients. In spite of poor posttransplant outcomes, these patients nonetheless have a better probability of survival accepting a marginal liver than waiting for a standard criteria donor liver. B, Unadjusted residing donor liver graft survival for main transplants (blue bars) and retransplants (red bars) at 3 months, 1 yr, 5 years and 10 years after transplant (Tx). Advances in endoscopic and percutaneous biliary intervention for administration of ischemic cholangiopathy can now postpone or altogether avoid the necessity for retransplantation. However, there stays the subset of patients who develop secondary biliary cirrhosis or who experience repeated episodes of life-threatening biliary sepsis regardless of endoscopic or percutaneous intervention and thus progress to requiring retransplantation. Precise timing between the donor and recipient groups is crucial not solely to minimizing cold ischemia time but additionally to allowing enough time for what can typically be an in depth hepatectomy section. A thorough review of the previous operative course, together with examination of high-quality cross-sectional imaging, with consideration to the websites and sort of vascular and biliary reconstruction, will help in proceeding with the dissection. In all instances the abdomen is opened by way of the previous bilateral subcostal incision, and a mechanical retractor is placed with blades underneath each costal margins to pull the ribs laterally and cephalad, opening the aperture. In the setting of late retransplantation, nonetheless, dense adhesions and portal hypertension combine to create a surgical field that may tax even essentially the most skilled surgeon. Blunt dissection ought to be prevented, and considered use of electrocautery with sharp dissection alongside tissue planes can minimize blood loss and injury to very important constructions. First, the adhesions of the liver to the anterior abdominal wall and diaphragm are divided, and the suprahepatic vena cava is recognized. Full caval exposure/dissection ought to be undertaken in the presence of an allograft ready for implantation, or alternatively with venovenous bypass out there for initiation, should one require expeditious hepatectomy within the setting of bleeding. Dissection of the porta hepatis have to be carried out meticulously as a end result of 64 RetRansplantation 805 the disappearance of normal tissue planes makes it very troublesome to identify vascular buildings. Injury to the hepatic artery or portal vein surrounded by scar can outcome in large bleeding or compromise of the vascular reconstruction to the new implant. In tough circumstances, starting the dissection excessive within the hilum might facilitate proximal management and subsequent vascular reconstruction. If too much scarring or collateral vessel formation has occurred, it could be essential to place the patient on venovenous bypass before finishing the hepatectomy. Venovenous bypass is initiated with the systemic circulation, by cannulating the saphenous or femoral vein for blood extraction and the axillary or inner jugular veins for blood return. The portal vein can then be cannulated and its circulate added to the identical circuit by way of a Y-connector. Before continuing with completion of the hepatectomy, acceptable planning of portal and arterial inflow, with consideration of vascular grafts, must be thought of to minimize the nice and cozy ischemic time.
Noroxin: 400 mg
Discount noroxin 400mg visaLaboratory examination reveals leukocytosis infection process order noroxin 400mg visa, rising serum bilirubin and alkaline phosphatase levels treatment for sinus infection in child best noroxin 400mg, and increased bilirubin in belly drainage higher than serum ranges within the presence of a leak antibiotics used to treat pneumonia 400mg noroxin. Ultrasonographic examination reveals a biliary collection within the case of a leak and biliary dilation proximal to the location of any obstruction antibiotic resistance crisis generic noroxin 400mg free shipping. Cholangiography or hepatobiliary scintigraphy demonstrates leakage of contrast or radionuclide into the subhepatic house. Delayed views may be essential to differentiate intraluminal accumulation from an intraperitoneal leak. Hyperacute rejection, though seen with different organ transplants, hardly ever occurs after liver transplantation. Significant intra-abdominal bleeding requiring surgical intervention is extra widespread after transplantation with reduced-size grafts. The hematocrit is kept higher than 20% to present enough oxygen-carrying capacity and fewer than 30% to probably lower the danger for hepatic artery thrombosis. Output from the abdominal drains is quantified every hour initially, and a hematocrit is spun on the drainage if it appears sanguineous. Routine anticoagulation was previously discussed with respect to hepatic artery thrombosis. Forty-four % of postoperative infections occurred within the first 2 weeks; 78% were bacterial, 19% had been fungal, and 3% were viral in origin. The most prevalent bacterial pathogens in the postoperative period in pediatric sufferers are listed in Table 70-5. The overwhelming majority of fungal infections are from Candida albicans, with the abdomen and urinary tract being the commonest primary source. Fever in the early postoperative course is extremely suggestive of infection, and when leukocytosis is also present, empirical antibiotic protection must be initiated after appropriate materials for culture is obtained, including sputum, blood, urine, and peritoneal fluid. Fungal infections are also a big problem in the early postoperative period, with C. Risk factors for fungal an infection include antibiotic remedy, vascular complications, high transfused blood volumes, intra-abdominal issues, reintubation, steroid use, and retransplantation. When a vascular or other type of intra-abdominal complication occurs postoperatively, prophylactic antifungal coverage is typically started as a end result of a significant proportion of this inhabitants could have an invasive fungal an infection. The patient at highest danger is a seronegative recipient who receives a graft from a seropositive donor. The lowest incidence of an infection happens when both the recipient and donor are seronegative; seropositive recipients are at intermediate threat. For all different sufferers, a regimen of acyclovir, ganciclovir, or each is advocated. This is ideally carried out shortly after deciding to list the child for transplantation and once more in the immediate preoperative interval. Postoperatively, having acquainted toys at the bedside as nicely as a parent with the child is useful in providing consolation. A multidisciplinary approach is required, along with efficient communication among all caregivers. With attentive, anticipatory care, many potential problems may be averted and new issues detected early and handled appropriately. Long-term outcomes of pediatric liver transplantation in a mixed pediatric and grownup transplant program. Intensive care management after pediatric liver transplantation: A single-center experience. Computed tomography in the assessment of raised intracranial stress in non-traumatic coma. Intracranial hypertension in acute liver failure: Pathophysiological basis of rational administration. Mannitol causes compensatory cerebral vasoconstriction and vasodilation in response to blood viscosity changes. The impact of hypertonic sodium chloride on intracranial strain in patients with acute liver failure. Hypothermia for the management of intracranial hypertension in acute liver failure. Moderate hypothermia with intracranial stress monitoring as a therapeutic paradigm for the management of acute liver failure: a scientific evaluation. Orthotopic liver transplant sufferers require less postoperative morphine than do sufferers present process hepatic resection. Prolonged use of dexmedetomidine in an toddler with respiratory failure following residing donor liver transplantation. Immediate tracheal extubation of pediatric liver transplant recipients within the working room. Effect of hypophosphatemia on diaphragmatic contractility in sufferers with acute respiratory failure. A potential research of indexes predicting the result of trials of weaning from mechanical ventilation. Crying very important capability and maximal inspiratory stress as scientific indicators of readiness for weaning of infants less than a 12 months of age. Effect of mechanical ventilator weaning protocols on respiratory outcomes in infants and children. Mechanisms of hypertension throughout and after orthotopic liver transplantation in kids. Severe hypertension after liver transplantation in alpha 1 antitrypsin deficiency. Diuretic efficiency of furosemide throughout continuous administration versus bolus injection in healthy volunteers. Comparison of continuous versus intermittent furosemide administration in postoperative pediatric cardiac sufferers. Efficacy of steady arteriovenous hemofiltration with dialysis in sufferers with renal failure. Liver transplantation: energy expenditure, nitrogen loss, and substrate oxidation price within the first two postoperative days. Intensive-care unit experience in the Mayo liver transplantation program: the first one hundred instances. Early graft loss after liver transplantation: Etiology, chronology, and prognosis. Long-term outcomes of pediatric liver transplantation: An analysis of 569 transplants. Fungal illness in liver transplant recipients: A multivariate evaluation of risk factors. The influence of perioperative transfusion of blood merchandise on survival after pediatric liver transplantation. Prophylactic fluconazole in liver transplant recipients-a randomized, double-blind, placebo controlled trial.
Order noroxin 400 mg otcPathogenesis of main sclerosing cholangitis and advances in diagnosis and management antibiotic resistance by area 400 mg noroxin for sale. Liver transplantation in alcoholic liver illness current standing and controversies antibiotics for dogs at petco order noroxin 400 mg with amex. Pediatric non alcoholic fatty liver disease: old and new ideas on development antibiotics for uti dog buy noroxin 400 mg without prescription, progression treatment for gardnerella uti buy noroxin 400mg without a prescription, metabolic insight and potential treatment targets. Clinical evaluation of nonalcoholic steatohepatitis in liver surgical procedure and transplantation. Development of nonalcoholic fatty liver disease after orthotopic liver transplantation for cryptogenic cirrhosis. Non-alcoholic fatty liver disease in liver transplant recipients: one other story of "seed and soil". Recurrent illness following liver transplantation for nonalcoholic steatohepatitis cirrhosis. Treatment of chronic hepatitis E in liver transplant recipients with pegylated interferon alpha-2b. Influence of immunosuppressive therapy on the natural historical past of genotype three hepatitis-E virus an infection after organ transplantation. Prevalence of hepatitis E virus an infection in pediatric stable organ transplant recipientsÂa singlecenter expertise. S100 protein constructive dendritic cells in main biliary cirrhosis and other continual inflammatory liver ailments. Development of autoimmune hepatitis following liver transplantation for primary biliary cirrhosis. Hepatitis C-associated granulomas after liver transplantation: morphologic spectrum and scientific implications. Antibodies in opposition to cytokeratin 8/18 in a affected person with de novo autoimmune hepatitis after livingdonor liver transplantation. Identification by proteomic tool of atypical anti-liver/kidney microsome autoantibodies targets in de novo autoimmune hepatitis after liver transplantation. Relapsing features of bile salt export pump deficiency after liver transplantation in two patients with progressive familial intrahepatic cholestasis sort 2. Recurrent autoimmune hepatitis after liver transplantation: Diagnostic criteria, threat factors, and end result. Monitoring of human liver and kidney allograft tolerance: a tissue/histopathology perspective. Liver Transplant Tolerance and Its Application to the Clinic: Can We Exploit the High Dose Effect? Tolerance and chimerism and allogeneic bone marrow/stem cell transplantation in liver transplantation. Complete Immunosuppression Withdrawal for Pediatric Liver Transplant Recipients: A Prospective, Multi-Center, Single Arm Pilot Trial. Liver transplant recipients weaned off immunosuppression lack circulating donorspecific antibodies. Intra-graft expression of genes involved in iron homeostasis predicts the development of operational tolerance in human liver transplantation. Requirement of protocol biopsy earlier than and after full cessation of immunosuppression after liver transplantation. Significance of nodular regenerative hyperplasia occurring de novo following liver transplantation. Drug publicity and perceived adverse drug events reported by liver-transplant patients. Ground-glass, polyglucosan-like hepatocellular inclusions: A "new" diagnostic entity. Distribution of the main histocompatibility complex antigens on completely different mobile components of human liver. Increased expression of sophistication I main histocompatibility advanced antigens on hepatocytes in rejecting human liver allografts. Expression of main histocompatibility complicated antigens and alternative of donor cells by recipient ones in human liver grafts. Human hepatic stellate cells show options of antigen-presenting cells and stimulate lymphocyte proliferation. Liver transplantation for youngsters with Wilson illness: comparability of outcomes between youngsters and adults. Effect of liver transplantation on the survival of patients with strange onset familial amyloid polyneuropathy in Japan. Outcomes of liver transplantation for glycogen storage disease: a matched-control research and a review of literature. Fortunately, liver allografts are infrequently lost to rejection or opportunistic infection. Recurrent illness, however, stays a significant issue and is a frequent cause of graft dysfunction and loss. The presence and severity of macrovesicular steatosis, the severity of necroinflammatory exercise at presentation, the extent of hepatocellular apoptosis, the presence of ballooning degeneration and cholestasis, and the extent of hepatic stellate cell activation have been reported to be associated with extra extreme illness recurrence. Histology of Recurrent Hepatitis C the histological features of hepatitis C in a transplant liver are very comparable to those in a local liver with a quantity of exceptions. Early in the middle of recurrence the initial histological image resembles that of acute hepatitis with a predominance of lobular exercise. Steatosis has also been reported as one of the earliest histological feature of recurrent hepatitis C, but this finding is neither particular nor sensitive. Alternatively, there may be an intensive sinusoidal lymphocytic infiltrate with only uncommon apoptotic hepatocytes. Bile duct infiltration by lymphocytes is frequently seen however is mostly mild and with out important epithelial injury. Ductular reaction at the interface usually results from interface exercise and may complicate the assessment of biliary obstruction in these sufferers (see later). A, Nodular portal infiltrate with interface activity typical of continual hepatitis C, native liver (hematoxylin-eosin, Ч100). B, Interface activity with disruption of the limiting plate, allograft liver (hematoxylin-eosin, Ч400). C, Lymphocytic infiltration of the bile duct, native liver (hematoxylin-eosin, Ч400). Diffuse, not nodular Variable infiltration by lymphocytes from mild to marked, with epithelial damage from delicate to severe Swollen or pyknotic endothelium, detached from basement membrane by subendothelial inflammatory cells (endotheliitis) Often seen in reasonable to extreme acute rejection and in late acute rejection Inflammation and mobile injury in extreme acute rejection and in late acute rejection ± Endotheliitis and perivenular irritation and necrosis (central perivenulitis) in extreme acute rejection or late acute rejection Hepatitis C Predominantly lymphocytic, often nodular ± Mild infiltration by lymphocytes with gentle epithelial harm Lymphocytes might encroach upon endothelium from the stroma or adhere to the luminal aspect of the cell Minimal in early recurrence, variable from delicate to marked with chronicity Predominant in early recurrence, variable later ± Focal and delicate perivenulitis (present in lower than half of the lobules) Primary Biliary Cirrhosis Lymphoplasmacytic, sparse or dense, may be nodular, could additionally be centered on bile duct. Edema and neutrophils in some instances Variable infiltration and injury from mild to florid duct lesion Lymphocytes could encroach upon endothelium from the stroma or adhere to the luminal aspect of the cell Primary Sclerosing Cholangitis Predominantly lymphocytic or lymphoplasmacytic. Edema and neutrophils in some circumstances Variable from regular to lymphocytic infiltrate to periductal edema and fibrosis Lymphocytes could encroach endothelium from the stroma or adhere to the luminal aspect of the cell Ductal metaplasia and interface activity is often present ± Activity, variable Bile ducts Portal veins Interface activity Ductal metaplasia and interface activity is often present ± Activity, variable Lobules Central vein Generally uninvolved; nonetheless, focal/mild perivenular activity may be seen in circumstances with a outstanding component of hepatitis Generally uninvolved; nonetheless, focal/mild perivenular exercise may be seen in instances with a outstanding element of hepatitis and endotheliitis.
Buy 400 mg noroxin with visaSteroids Gastritis Although steroids have been associated with gastritis and ulceration antibiotic rocephin buy noroxin 400 mg free shipping, the association is weak treatment for dogs fever cheap 400 mg noroxin with visa, with peptic ulcer disease probably only related to high-dose steroid use antibiotic jokes order 400mg noroxin otc. Calcineurin Inhibitor Neurotoxicity Both tacrolimus and cyclosporine are related to a big selection of neurotoxic signs antibiotic resistant klebsiella pneumoniae cheap noroxin 400 mg on line, including headache, tremor, confusion, altered consciousness, dysarthrias, seizures, and coma Table 69-8). These complications are particularly relevant in the Serious 69 PostoPerative intensive Care ManageMent in adults 889 status and guarantee no neurotoxicity. The remedy of seizures in transplant recipients is much like that of any patient having seizures. If the seizure has not resolved spontaneously and has lasted greater than 5 minutes, then it must be thought-about evolving standing epilepticus and it requires emergent remedy. Levetiracetam is the antiepileptic of choice in transplant recipients given its broad efficacy throughout a variety of seizure varieties, its favorable side impact profile, its lack of hepatic metabolism, and minimal drug-drug interactions. Once the seizure is managed, the underlying reason for the seizure ought to be established, significantly in patients with acute repetitive seizures or status epilepticus. If all research results are normal and the affected person is secure, a period of statement could be thought of. It is assumed that the coagulopathy and thrombocytopenia that persist into the initial posttransplant period are protecting in opposition to ischemic/embolic strokes. Some reports169 describe an affiliation of huge blood loss and hypotension in the course of the transplant to a later cerebral hemorrhage and hypothesize that an ischemic harm during transplant leads to later bleeding with the posttransplant coagulopathy. Intracranial bleeding presents as aphasia, hemiparesis, seizure, and unconsciousness, and any sudden loss of consciousness should make the clinician suspect bleeding. In varied reports168,169 craniotomy after intracranial bleeding was uniformly futile, so one of the best answer is a preventative technique. Hepatic encephalopathy is a frequent complication of cirrhosis, but it often improves after liver transplantation. Uremic encephalopathy is related to renal failure, and signs can range from mild confusion to deep coma. Pulmonary artery occlusion pressure and central venous pressure fail to predict ventricular filling volume, cardiac performance, or the response to volume infusion in regular subjects. Measurement of cardiac output by pulse dye densitometry using indocyanine green: A comparison with thermodilution methodology. Perioperative use of transesophageal echocardiography by anesthesiologists: Impact in noncardiac surgery and in the intensive care unit. Perioperative fluid and volume management: physiological basis, tools and methods. Association of hydroxyethyl starch administration with mortality and acute kidney harm in critically ill sufferers requiring quantity resuscitation: a systematic evaluate and meta-analysis. Goal-directed haemodynamic remedy and gastrointestinal issues in major surgical procedure: a meta-analysis of randomized controlled trials. Early goal-directed remedy after major surgery reduces issues and duration of hospital stay. Elevation of systemic oxygen supply in the remedy of critically unwell sufferers. The impact of postreperfusion syndrome on short-term patient and liver allograft consequence in patients present process orthotopic liver transplantation. It is one of the most critical neurological problems occurring in liver transplantation, but the incidence is now lower than 1%. In sufferers transplanted with a Na+ level of less than 125 mmol/L, a standard saline (0. Risk elements for primary dysfunction after liver transplantation  a multivariate evaluation. Sinusoidal lining cell damage: the important damage in chilly preservation of liver allografts in the rat. Reduction of primary nonfunction with prostaglandin E1 after scientific liver transplantation. Successful reversal of main graft non-function in a liver transplant patient handled with prostaglandin E1. A double-blind, randomized, placebocontrolled trial of prostaglandin E1 in liver transplantation. Prostaglandin E1 administration following orthotopic liver transplantation: ad randomized prospective multicenter trial. The efficacy of N-acetylcysteine as a hepatoprotective agent in liver transplantation. Past and future approaches to ischemia-reperfusion lesion related to liver transplantation. Mechanisms of ischemic harm are totally different within the steatotic and regular rat liver. Mouse livers with macrosteatosis are extra prone to normothermic ischemic harm than these with microsteatosis. The impact of donor age on liver transplantation: affect of donor age on early liver perform and on subsequent affected person and graft survival. Use of prolonged standards liver decreases wait time for liver transplant with out adversely impacting posttransplant survival. Correlation between donor age and the sample of liver graft recovery after transplantation. The effect of methylene blue throughout orthotopic liver transplantation on publish reperfusion syndrome and postoperative graft perform. The effect of methylene blue on the hemodynamic during ischemia reperfusion injury in orthotopic liver transplantation. Risk elements for and clinical course of nonanastomotic biliary strictures after liver transplantation. The Task Force for Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology and the European Respiratory Society, endorsed by the International Society of Heart and Lung Transplantation. Hematologic aspects of liver transplantation for Budd-Chiari syndrome with particular reference to myeloproliferative problems. Incidence of tricuspid regurgitation and vena caval backflow in mechanically ventilated patients. Fast monitor anaesthesis for liver transplantation reduces postoperative ventilation but not intensive care unit keep. Very early tracheal extubation with out predetermined standards in a liver transplant recipient. Acute respiratory distress syndrome after liver transplantation: etiology, prevention and administration. Ventilation with lower tidal quantity as compared with traditional tidal volumes for acute lung harm and the acute respiratory misery syndrome. Effects of positive end-expiratory stress air flow on splanchnic oxygenation in humans. Impaired responsiveness to endogenous vasoconstrictors and endothelium derived vasoactive components in cirrhosis. Recommendations for the prognosis and management of corticosteroid insufficiency in critically ill grownup sufferers: consensus statements from an international task drive by the American College of Critical Care Medicine. Hyponatremia and mortality among sufferers waiting for liver transplant waiting list.
Turnera diffusa var. aphrodisiaca (Damiana). Noroxin. - Are there safety concerns?
- How does Damiana work?
- What is Damiana?
- Are there any interactions with medications?
- Headaches, bedwetting, depression, nervous stomach, constipation, sexual problems, boosting mental and physical stamina, and other conditions.
- Dosing considerations for Damiana.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96689
Buy 400 mg noroxin mastercardOn the graft facet a wide venous orifice with an extended cuff is shaped by gathering the left virus x movie 400mg noroxin overnight delivery, center zombie infection android discount noroxin 400mg visa, and quick hepatic veins using a conduit vein graft and patch vein grafts antibiotic abuse cheap 400mg noroxin overnight delivery. In such cases an autologous or cryopreserved homologous vein interposition graft can be utilized antibiotic 3 day course generic noroxin 400mg with mastercard. It is rare that the anastomosed portal vein seems redundant, having the danger for kinking after the liver graft regeneration as a result of the length of the recipient right portal vein is short. Alignment is crucial, and the anterior wall of the graft and recipient portal vein are marked with 6-0 polypropylene (Prolene). The anastomoses are performed in a running fashion with 6-0 polypropylene sutures with integrated progress issue. Infrequently the right liver graft has right anterior and posterior branches, which are individually situated. A single portal orifice could be created in many cases by performing venoplasty of the anterior and posterior branches within the bench operation. When the anterior and posterior branches are too distantly positioned to permit for venoplasty, a vein graft can be used as an interposition. An autologous graft12 (such as proper anterior and posterior branches of the recipient) or cryopreserved vein. The first sew is began with an adjustment of the anterior partitions of the graft and recipient left portal branches. In such cases the venoplasty technique14 is helpful for securing an sufficient influx. In the left liver plus caudate lobe graft, an isolated caudate portal vein originating from the left facet wall of the portal branches of the caudate lobe is sometimes noticed. Cases With Preoperative Portal Vein Thrombosis Preoperative portal vein thrombosis is an important issue. In cases with in depth splenorenal shunts,21 anastomosis of the divided left renal vein with a portal vein using a vein graft as a conduit can be carried out as an exception. Left Liver Left liver circumstances nearly all the time require a single portal reconstruction between the graft and recipient left portal department or portal vein trunk. In detail, the recipient and graft arteries are clamped with single microclamps to quickly halt blood flow. The first suture is positioned utilizing monofilament sutures at the level in the artery most troublesome to visualize. Each stitch is positioned from the inside aspect of the arterial wall to the outer side because there may be a minute separation of the intima from the media within the recipient or graft artery. Subsequent sutures are superior anteriorly on either aspect adjacent to the earlier suture. Among them, the optimal artery is selected primarily based on the situation, size, and rigidity when anastomosed. The circumference discrepancy between the graft arterial stump and the recipient artery should be less than 50%, which may be adjusted through the anastomosis. The hepatic arterial branch close to the trunk of the proper hepatic artery is often thicker than the arterial stump of the graft and inappropriate for anastomosis. Dissection of the common hepatic artery or ligation of the gastroduodenal artery to mobilize the hepatic arterial department for anastomosis must be avoided. When the right hepatic artery is thrombosed because of, for example, repeated transhepatic arterial chemoembolization for therapy of hepatocellular carcinoma, the splenic artery, left gastric artery, gastroduodenal artery, or proper gastroepiploic artery can be used as an inflow. The majority of arterial reconstructions in the proper liver could be single reconstructions between the graft proper hepatic artery and recipient proper hepatic arterial branch. Also, in such cases socalled nonanatomical anastomosis utilizing arteries aside from the branches of correct hepatic arteries ought to be prevented to keep away from poor patency over the lengthy term. The anastomosis is mostly carried out in an interrupted trend with 9-0 nylon sutures (diameter 0. A partial liver graft often has multiple and small ducts (usually 2 to 5 mm in diameter). As a end result the incidence of biliary complications, together with leaks and strictures, is greater in partial liver grafts. Biliary reconstruction in partial liver grafts was beforehand performed with a Roux-en-Y hepaticojejunostomy with or without stenting because the main indication for living donor liver transplantation was pediatric sufferers with biliary atresia. Leakage is more doubtless associated to the portal vein or hepatic arterial thrombosis in Roux-en-Y hepaticojejunostomy. Pearls and Pitfalls · Outflow reconstruction is amongst the most necessary technical features in partial graft implantation. The ultimate graft positioning can play an important position as a end result of the outflow could be easily blocked by torsion of the liver graft. In such circumstances the anastomosis can be carried out even when there are multiple ducts positioned far from one another within the graft. Management of Grafts With Multiple Ducts Multiple ducts situated shut collectively and sharing a standard wall must be joined collectively so that a single anastomosis could be carried out. In these circumstances the shared septum of the adjacent ducts may be divided vertically after which mixed with fine absorbable sutures to create a single massive orifice for the anastomosis. Biliary tree anastomosis should be fashioned tension-free, and leakage and strictures ought to be checked by cholangiography via the external stent tube upon completion. An synthetic vascular graft is a useful interpositional material for drainage of the proper anterior section in dwelling donor liver transplantation. Vein reconstruction in modified proper liver graft for living donor liver transplantation. Technique and outcome of autologous portal Y-graft interposition for anomalous proper portal veins in residing donor liver transplantation. It is an indispensable choice, nevertheless, for end-stage liver disease sufferers in the Eastern world, where the source of deceased donors is inadequate. The left liver graft is optimized for both flow and outflow, although the potential for a separated arterial provide remains problematic. The left liver graft, however, is usually too small to satisfy the metabolic calls for of sufferers with superior liver cirrhosis and low Model for End-Stage Liver Disease rating. Hepatic artery reconstruction with double-needle microsuture in living-donor liver transplantation. Simple check on the again table for justifying single hepatic-arterial reconstruction in residing associated liver transplantation. Biliary reconstruction, its issues and management of biliary problems after grownup liver transplantation: a systematic review of the incidence, risk elements and outcome. Improved strategy of portal vein reconstruction in pediatric liver transplant recipients with portal vein hypoplasia. Innovative methods for and results of portal vein reconstruction in living-related liver transplantation. Portal vein thrombosis in adults present process liver transplantation: threat factors, screening, administration, and consequence.
Noroxin 400 mg on linePolysaccharides are known as activator surfaces and favor the uptake of factor B on the chain of C3b, with the corresponding displacement of factor H homemade antibiotics for sinus infection purchase 400 mg noroxin visa. In this situation, binding of factor H is inhibited, and consequently issue B will substitute H at the widespread binding site infection fighting foods discount noroxin 400 mg on-line. When factor H is excluded, C3b is considered fashioned repeatedly in small amounts antimicrobial zinc gel buy noroxin 400mg line. Another controlling point within the amplification loop is decided by the steadiness of the C3b,Bb convertase antibiotics meaning buy cheap noroxin 400 mg. Ordinarily, C3b,Bb decays because of the lack of Bb, with a half-life of roughly 5 minutes. However, if properdin (P) binds to C3b,Bb, forming C3b,BbP, the half-life is extended to half-hour. The association of quite a few C3b units, factor Bb, and properdin on the surface of an aggregate of protein or the floor of a microorganism has potent exercise as a C5 convertase. With the cleavage of C5, the rest of the complement cascade continues as in the traditional pathway. Mannose-binding lectin, a sample recognition molecule of the innate immune system, binds to arrays of terminal mannose groups on quite so much of micro organism. A deficiency of mannose-binding lectin is caused by certainly one of three level mutations in its gene, every of which reduces ranges of the lectin. The second class encompasses different results of complement in immunity and inflammation that are mediated by the proteolytic fragments generated during complement activation. These fragments may stay bound to the identical cell surfaces at which complement has been activated or may be launched into the blood or extracellular fluid. In either state of affairs, active fragments mediate their effects by binding to specific receptors expressed on varied types of cells, including phagocytic leukocytes and the endothelium (Table 5-3). In distinction, the absence of an integral element of the traditional, different, or terminal lytic pathways can result in decreased complement activation and a scarcity of complementmediated organic capabilities. Alterations in Complement Levels the complement system may cause vital tissue harm in response to abnormal stimuli. Biological results of complement activation can occur as a response to persistent infection or an autoantibody response to self antigens. Complement activation is also associated with intravascular thrombosis, which results in ischemic injury to tissues. Elevated Complement Levels the complement level may be elevated in many inflammatory situations. Decreased Complement Levels Low levels of complement suggest one of many following organic effects: ďż˝ Complement has been excessively activated recently. Specific part deficiencies are related to quite so much of problems (Table 5-4). Deficiencies in any of the protein elements of complement are normally brought on by a genetic defect that leads to abnormal patterns of complement activation. If regulatory parts are absent, excess activation may occur on the wrong time or at the incorrect website. The potential penalties of elevated activation are extra inflammation and cell lysis and consumption of complement parts. Hypocomplementemia may result from the complexing of IgG or IgM antibodies able to activating complement. Depressed values of complement are related to illnesses that give rise to circulating immune complexes. C1q Binding this procedure measures the binding of immune complexes containing IgG1, IgG2, or IgG3 and IgM to the complement component C1q. High values of C1q binding are related to the presence of circulating immune complexes of the kind that interacts with the basic pathway of complement activation. Of symptomatic patients, 50% exhibit a lupus-like dysfunction with photosensitivity and rash. C3 Also an acute-phase protein, elevated C3 levels can indicate an acute inflammatory illness. Extremely decreased ranges are seen in sufferers with poststreptococcal glomerulonephritis and in those with inherited (C3) complement deficiency. The following three forms of complement deficiency can cause elevated susceptibility to pyogenic infections: 1. Deficient perform of the mannose-binding lectin pathway Increased susceptibility to pyogenic bacteria. Low ranges of mannose-binding lectin in young children with recurrent infections recommend that the mannosebinding lectin pathway is important in the course of the interval between the loss of passively acquired maternal antibody and the acquisition of a mature immunologic repertoire of antigen publicity. These proteins may be demonstrated in tissue by acceptable immunopathologic stains. The most frequent analysis of complement is by serum or plasma assay (Table 5-5). Assessment of Complement the procedures discussed subsequent can be utilized in diagnostic immunology. Activation of the classic pathway (and sometimes with accompanying various pathway activation) is associated with problems such as immune complex illnesses, various forms of vasculitis, and acute glomerulonephritis. Elevated C4 ranges can point out an acute inflammatory reaction or a malignant condition. Patients with extraordinarily low C4 levels in the presence of normal levels of the C3 part could also be demonstrating the effects of a genetic deficiency of C1 inhibitor or C4. Reduction of C3 and C4 elements implies that activation of the traditional pathway has been initiated. C5 A genetic deficiency of the C5 element is related to elevated susceptibility to bacterial an infection and is expressed as an autoimmune dysfunction. C6 A decreased amount of C6 predisposes a person to important neisserial (bacterial) infections. Select Complement Deficiencies Properdin Deficiency Properdin acts to stabilize the choice pathway C3 convertase (C3bBb). Two types exist, type 1 (low antigen degree and low useful protein) and type 2 (normal antigen stage with low function). Familial Mediterranean Fever this defect in protease in peritoneal and synovial fluid is transmitted as an autosomal recessive trait on chromosome sixteen. Patients with this defect experience recurrent episodes of fever and irritation within the joints and pleural and peritoneal fluids. Cytokines are synthesized and secreted by the cells associated with innate and adaptive immunity in response to microbial and other antigen exposures (Tables 5-6 and 5-7). The generic term cytokines has turn into the popular name for this class of mediators. Lymphokines is one other term used to explain cytokines produced by activated lymphocytes.
400mg noroxin with visaIntravenous ganciclovir antimicrobial guidelines 2013 buy 400 mg noroxin overnight delivery, followed by oral valganciclovir (900 mg/day) antibiotic 933171 cheap 400 mg noroxin fast delivery, has been used on this setting virus fbi buy 400mg noroxin. Varicella-Zoster Virus Primary or de novo varicella could be a severe complication after liver transplantation and might trigger a extreme hemorrhagic rash and multiple organ failure antibiotics non penicillin noroxin 400mg amex. Intravenous acyclovir (10 mg/kg every eight hours if kidney function is normal) is incessantly recommended for the preliminary therapy of varicella or herpes zoster virus in transplant patients. After enchancment, therapy could additionally be changed to high-dose oral acyclovir or valacyclovir. If a seronegative affected person is inadvertently exposed to an individual with varicella or herpes zoster virus, prophylactic zoster immune globulin should be administered. The timing of the an infection may be quite variable, but the majority of sufferers are affected inside the first 6 months after transplantation. Fever, lymphadenopathy, pharyngitis, splenomegaly, and atypical lymphocytosis are widespread options of the disease. Atypical findings corresponding to a chronic mononucleosislike illness lasting several weeks, pneumonia, and encephalitis have also been observed. Reactivation of virus can occur after transplantation and has been related to hemorrhagic cystitis, progressive multifocal leukoencephalopathy, and interstitial nephritis. Although cidofovir has been used to deal with papovavirus infections, efficient treatment nonetheless needs to be established. Management methods embrace discount of immunosuppression, remedy with antiviral brokers (acyclovir, adefovir, cidofovir, foscarnet, ganciclovir, or penciclovir) and cytotoxic chemotherapy. Influenza Virus Types A and B, Parainfluenza Virus, and Respiratory Syncytial Virus Community-acquired respiratory viral disease in liver transplant recipients is often manifested as upper respiratory tract symptoms frequently related to fever, myalgia, arthralgia, and anorexia. The analysis of respiratory viral illness is facilitated by speedy detection of virus-laden higher respiratory cells. Progressive viral an infection can lead to fatal pneumonia or dying from superinfection with bacterial pathogens corresponding to S. Treatment of influenza A has included early administration of amantadine or rimantadine. If began within 30 to 36 hours after the onset of symptoms, they could shorten the duration of illness and decrease upper respiratory complications. Aerosolized ribavirin has been used to deal with parainfluenza virus and respiratory syncytial virus infections, but its efficacy is unsure. Immunization with influenza vaccine is really helpful for transplant recipients, however its efficacy could also be diminished by suboptimal antibody responses to the vaccine. After liver transplantation the spectrum of adenovirus an infection contains asymptomatic shedding (urine, respiratory secretions, or stool), Parvovirus In transplant recipients, parvovirus infection is an occasional reason for refractory extreme anemia, pancytopenia, and thrombotic microangiopathy. However, false-negative results of the enzyme-linked immunosorbent assay could occur, especially through the preliminary postinfectious interval. Hepatitis B and C Virus the posttransplant threat for viral hepatitis in a liver transplant recipient may be associated to acquisition of an infection from an contaminated organ, a blood donor, or recurrence of infection current earlier than transplantation. Thus the indications for retransplantation on this affected person population stay controversial. Although the choice of calcineurin blockers has not clearly been shown to have an impact on histological recurrence of hepatitis C, cumulative publicity to corticosteroids has been related to enhanced viremia, extra severe histological recurrence, and better mortality charges. Additionally, clinically vital pharmacokinetic drug interactions with tacrolimus and cyclosporine (increased area underneath the curve and elimination halflife) can occur with these brokers. Bronchoalveolar lavage with transbronchial biopsy is a extremely delicate methodology of identifying the organisms in the lung. Only a few circumstances have been reported and had been manifested by encephalitis, focal lesions within the mind, or pneumonia. Pyrimethamine plus sulfadiazine or pyrimethamine plus clindamycin is used for remedy. The antibiotics chosen for prophylaxis are directed in opposition to organisms generally found in the gastrointestinal flora (Enterobacteriaceae, enterococci, anaerobes) plus staphylococci. Intravenous cefoxitin, ceftizoxime, ampicillin-sulbactam, cefotaxime plus ampicillin, and piperacillin-tazobactam have all been used efficiently. In distinction, other liver transplant centers have used oral regimens of polymyxin, gentamicin, and nystatin or polymyxin, tobramycin, and nystatin, starting preoperatively and persevering with for a quantity of weeks postoperatively. Before the provision of newer antifungal medication, oral regimens with nystatin, clotrimazole, or amphotericin, or an intravenous regimen using low-dose amphotericin had been employed. However, the efficacy of those antifungal regimens for prophylaxis has never been clearly established. The efficacy of the azole antifungal brokers, fluconazole, itraconazole, voriconazole, and posaconazole, for prevention of invasive and superficial Candida an infection has been demonstrated in double-blind, placebo-controlled trials in either liver transplant recipients or oncology sufferers. Fluconazole is currently beneficial by the American Society of Transplantation Infectious Diseases Community of Practice for antifungal prophylaxis in liver transplant recipients at high-risk for invasive fungal infections. For patients colonized with Aspergillus or those who produce other specific risk elements for invasive aspergillosis, voriconazole or an echinocandin is selectively used for antifungal prophylaxis. In a recently completed randomized, double-blind trial, in high-risk liver transplant recipients the overall efficacy of anidulafungin and fluconazole for antifungal prophylaxis was similar. However, anidulafungin appeared extra helpful in sufferers with increased threat for aspergillosis or those who had received fluconazole before transplantation. To reduce morbidity and mortality from infection after liver transplantation, you will want to establish sufferers at greatest threat for critical infection as a consequence of those elements. Before transplantation, acutely ill sufferers with superior liver disease incessantly have been hospitalized for prolonged periods and are already colonized or contaminated with doubtlessly pathogenic organisms. Patients with intraoperative complications at the time of initial transplant surgical procedure or who require repeat transplantation due to graft failure have an elevated risk for infection. After transplantation, prolonged hospitalization within the intensive care unit and therapy of a number of episodes of rejection with corticosteroids, thymoglobulin, and different immunosuppressive brokers increase the risk for opportunistic infection. Except for some bacterial infections brought on by multiresistant organisms (Enterobacter, P. Over time, hepatitis B immune globulin has been replaced with a mix of oral hepatitis B antivirals. Hopefully, a well-tolerated and efficacious routine for prevention of recurrent hepatitis C can be established soon. Infection and rejection of main hepatic transplant in ninety three consecutive patients treated with triple immunosuppressive remedy. Incidence, distribution, and outcome of episodes of an infection in one hundred orthotopic liver transplantations. Impact of pretransplant infections on medical outcomes of liver transplant recipients. Donor-derived bacteremia in liver transplant recipients regardless of antibiotic prophylaxis. Mycobacterium tuberculosis infection in solid-organ transplant recipients: Impact and implications for administration. Tuberculosis in the transplant candidate: Importance of early prognosis and treatment. Tuberculosis in liver transplant recipients: A systematic evaluate and meta-analysis of particular person patient knowledge.
References - Anderson JL, Horne BD, Stevens SM, et al: Randomized trial of genotype-guided versus standard warfarin dosing in patients initiating oral anticoagulation. Circulation 2007;116:2563-2570.
- Singh S, Minor CL. Cystic duplication of the rectum. A case report. J Pediatr Surg 1980;15:205.
- Pai D, Sharma A, Kanungo R, et al. Role of abdominal drains in perforated duodenal ulcer patients: a prospective controlled Study. ANZ J Surg 1999;69(3):210-3.
- Pawlowski B, Boothroyd LG, Perrett DI, Kluska S. Is female attractiveness related to final reproductive success? Coll Antropol 2008; 32(2): 457-60.
- Grindlinger GA, Niehoff J, Hughes SL, et al: Acute paranasal sinusitis related to nasotracheal intubation of head-injured patients, Crit Care Med 15:214-217, 1987.
|