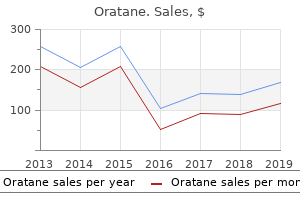
Oratane
Roger E. Stevenson, M.D. - Greenwood Genetic Center
- Greenwood, South Carolina
Discount 5 mg oratane otcUp till the age of forty years this zone makes up approximately 20% of the prostate gland skin care with peptides buy 30 mg oratane free shipping. As a man ages acne 4 days before period purchase 10mg oratane mastercard, the transition zone begins to enlarge acne jeans shop purchase oratane 30mg with amex, till it turns into the biggest area of the prostate acne 2008 generic oratane 5mg without prescription. As the transition zone enlarges, it then pushes the peripheral zone of the prostate towards the rectum. This zone is farthest from the rectum and contains approximately 1/3 of the ducts that secrete fluid that helps create semen. The gland has a variety of surfaces: a base, an apex, an anterior, a posterior and two lateral surfaces. It counteracts the clotting enzyme within the seminal vesicle fluid, which principally glues the semen to the cervix, situated subsequent to the uterine entrance contained in the vagina. The surfaces of the prostate gland the base the bottom on palpation is directed upwards and inferior to the floor of the bladder. The urethra penetrates it closer to its anterior border than its posterior border. This course of commences at puberty, persevering with for as long as the person lives, versus oogenesis (the manufacturing of the primordial ova), which occurs solely throughout foetal life. Each main spermatocyte divides into two secondary spermatocytes; and each secondary spermatocyte into two spermatids or younger spermatozoa. The major spermatocyte provides rise to two cells, the secondary spermatocytes; and the two secondary spermatocytes, by their subdivision, produce 4 spermatozoa. Diploid (46 chromosome) germ cells generally identified as spermatogonia line the basement membrane of each seminiferous tubule. The spermatogonia move away from the basement membrane as meiosis happens, as they mature they become main spermatocytes. Meiosis happens again and this produces two haploid (23 chromosome) cells known as secondary spermatocytes. Four spermatids are the end result of the two secondary spermatocytes undergoing meiosis. For spermatids to develop into sperm this is depending on the Sertoli cells which may be present in the seminiferous tubules. Attaching themselves to the Sertoli cells the spermatids receive the nourishment wanted and the hormonal signals required to turn into sperm. It has been estimated to take roughly 70 to eighty days for spermatogenesis to occur from meiotic division of spermatogonium to the maturation of a mature spermatid. The mature sperm journey from the seminiferous tubules to the epididymis, their capacity for fertilisation continues to happen. Usually, every millilitre of semen contains hundreds of thousands of spermatozoa, but the majority of the volume is made up of secretions of the glands within the male reproductive organs. The head incorporates the nucleus containing densely coiled chromatin fibres, surrounded anteriorly by an acrosome, which incorporates enzymes that are used for penetrating the feminine egg. Both courses of female and male hormones are current in each men and women alike, nevertheless they differ vastly of their amounts. Testosterone production will increase exponentially (approximately 18-fold) throughout puberty. It is common after puberty for the interstitial cells to produce testosterone continually. Once a person reaches 40 years of age testosterone manufacturing declines, on average men expertise a 1% per yr drop in testosterone production as quickly as they reach this age. Primary intercourse characteristics embody size of penis and testes size in adult men testosterone is answerable for creating the male genitals, spermatogenesis, and regulating the libido. Erectile function is influenced by testosterone as this increases the activity of nitric oxide synthase which regulates the motion of clean muscles in the penis. Increased nitric oxide synthase activity increases leisure of easy muscle tissue within the penis bettering the ability to obtain and keep an erection. Secondary sex characteristics embrace the growth of hair (pubic, physique and facial hair), a deep voice and heavier bones. Greater portions of testosterone cause males to have a greater proportion of lean body mass and decrease proportion of fat in comparison with ladies. Testosterone is liable for stimulating the ultimate steps of spermatogenesis in the seminiferous tubules. Throughout being pregnant and childbirth the uterus has to stretch and the muscular layer permits this to occur. The muscle will contact throughout labour and submit natally this muscular layer contracts forcefully to force out the placenta. During menstruation the layers of the endometrium are shed, sloughing away from the inside layer, this is the menstrual interval occurring on account of hormonal changes taking place. The endometrium thickens in the course of the menstrual interval becoming rich with blood vessels and glandular tissue till the following period happens and the cycle begins once more. The myometrium the endometrium Anatomy and Physiology for Nurses at a Glance, First Edition. This system is each a reproductive system in addition to containing the feminine sex organs. The ovaries provide a space for storage of the female germ cells and likewise produce the feminine hormones oestrogen and progesterone. The ovary accommodates numerous small buildings, these are known as ovarian follicles. The developing follicles are enclosed in layers of follicle cells, mature follicles are known as graafian follicles. Oestrogens are important for the development and maintenance of secondary sex characteristics working with a selection of different hormones, stimulating the feminine reproductive organ to put together for the growth of a foetus, playing a key position within the usual construction of the pores and skin and blood vessels. They help reduce the speed of bone resorption, improve increased high-density lipoproteins, decrease cholesterol levels and increase blood clotting. The uterus A hollow muscular organ within the pelvic cavity posterior and superior to the urinary bladder, anterior to the rectum, roughly 7. The fundus is a thick muscular region above the fallopian tubes; the body is joined to the cervix by the isthmus. The uterus additionally has three layers; the uterine wall has three distinct layers (see Table 38. The fallopian tubes the ovarian cortex this lies deep and near the tunica albuginea containing the ovarian follicles surrounded by dense irregular connective tissue. These follicles include oocytes in different phases of growth and a variety of cells that feed the creating oocyte, because the follicle grows it secretes oestrogen. Graafian follicles the graafian follicles manufacture oestrogen, stimulating the expansion of endometrium. The massive ruptured follicle turns into a brand new construction the corpus luteum, the remnants of a mature follicle. The paired fallopian tubes are delicate, thin cylindrical buildings approximately 814 cm lengthy, affixed to the uterus on one finish supported by the broad ligaments. The lateral ends of the fallopian tubes are open and manufactured from projections known as fimbriae draped over the ovary. Fertilisation of the ovum usually happens within the outer portion of the fallopian tubes.
Purchase 10mg oratane amexThe outer ovary is enveloped in a fibrous capsule known as the tunica albuginea skin care urdu tips purchase oratane 5 mg online, this is composed of cuboidal epithelium skin care event ideas oratane 30 mg amex. It is situated posterior to the urinary bladder and urethra acne laser removal order oratane 30 mg with visa, anterior to the rectum acne en la espalda trusted oratane 5 mg. Vaginal partitions are manufactured from membranous folds of rugae, composed of mucous-secreting stratified squamous epithelial cells. Oestrogen causes the expansion of vaginal mucosal cells, thickening and growing them, increasing glycogen content leading to a slight acidifying of the vaginal fluid. The vagina the ovarian medulla accommodates blood vessels, nerves and lymphatic tissues surrounded by unfastened connective tissue. This pertains to the event of comparatively undifferentiated germ cells oogonia which are mounted to between 2 to 4 million diploid (2n) stem cells during foetal growth. All ova are in the end the cervix the cervix forms a pathway between the uterus and the vagina. The uterine opening of the cervix is the inner os and the vaginal opening the external os. The house between these openings, the endocervical canal, acts as a conduit for the discharge of menstrual fluid, the opening for sperm and supply of the infant throughout start. The external genitalia have three key functions: 1 Enabling sperm to enter the body. There are variations in dimension with some ladies and the clitoral glans could additionally be very small in other girls they may have a large clitoris and the hood may not utterly cover it. The mons acts in such a means as to protect the pubic bone (the symphysis pubis is the name given to where two bones meet on the entrance of the pelvis) from the impact of sexual activity. During puberty the mons is covered with coarse pubic hair, after puberty this decreases. The urethra the exterior urethral orifice is located 2 to three cm posterior to the clitoris and instantly anterior to the vaginal orifice. It is usual for these labia to be covered with pubic hair, they contain numerous sweat and oil glands, the scent (pheromones), from these glands may have a role to play in sexual arousal. This is important, because the opening within the hymen permits the menstrual blood to come through when the girl starts having periods. The inner lips of the vulva are known as the labia minora, composed of skinny stretches of tissue within the labia majora, folding and protecting the vagina, urethra and the clitoris. They are thin, delicate folds of fats free hairless pores and skin located between the labia majora. The labia minora comprise a core of spongy tissue and within this there are many small blood vessels but no fat. The look of the labia minora varies from girl to lady, from tiny lips which would possibly be hidden between the labia majora to bigger lips that can protrude. Internally the floor consists of skinny skin and has a pink color associated with mucous membranes. Blood provide Arterial supply of the female external genitalia the rich arterial provide to the vulva comes from two external pudendal arteries in addition to one inner pudendal artery situated on either aspect. The internal pudendal artery supplies the pores and skin, sex organs and the perineal muscular tissues. The labial arteries are branches of the internal pudendal artery, and this is similar for the dorsal and deep arteries of the clitoris. Venous drainage of the female external genitalia the labial veins are offshoots of the internal pudendal veins and venae comitantes of the internal pudendal artery. The clitoris can lengthen and the hood retracts to make the clitoral glans more accessible throughout sexual excitement, the clitoris Lymph drainage Within the vulva there are a number of very wealthy networks of lymphatic channels. The majority of lymph vessels move to the superficial inguinal lymph nodes and deep inguinal nodes. Nerve provide the nerves that offer the vulva are branches of: 1 the ilioinguinal nerve. The subclavian, intercostal and inner thoracic veins also assist in returning blood to the heart. The milk is carried to the nipple by the ducts and from the nipple to the infant throughout breast-feeding. Axillary lymph nodes are positioned above the clavicle, behind the sternum in addition to in other components of the physique. Lymph circulates throughout physique tissues picking up fat, micro organism and different unwanted materials and filtering them out via the lymphatic system. Breast lymph nodes embody, supraclavicular nodes above the clavical; infraclavicular (or subclavicular) nodes beneath the clavicle; axillary nodes within the axilla and inside mammary nodes inside the chest across the sternum. Each breast incorporates a number of lobules (sections) that branch out from the nipple, the lobules are the glands that produce milk. During breast-feeding, the ducts carry milk from the alveoli towards the breast areola (the darkish area of pores and skin in the centre of the breast). From the areola, the ducts join together into larger ducts that terminate at the nipple. The areola (pink or brown in colour) is the circular area across the nipple, this incorporates small sweat glands which secrete moisture, this acts as a lubricant throughout breast-feeding. The nipple is the area found on the centre of the areola the place the milk emerges Breast development Fat, ligaments and connective tissue the spaces around the lobules and ducts are crammed with fat, ligaments and connective tissue. The amount of fat in the breast determines their dimension; the fats gives form to the breast. They run from the pores and skin via the breast attaching themselves to muscle tissue on the chest. Changes happen during puberty, in the course of the menstrual cycle, during pregnancy and after menopause. Most of the glandular and ductal tissue in older women is changed with fatty tissue and breasts become much less dense. Hormones and the breast Nerve supply There are a number of main nerves in the breast space, these embody nerves within the chest and arm. Arteries and capillaries Arterial blood provide to the breast comes from the thoracic branches of the axillary arteries and the inner mammary and intercostal arteries. Progesterone prepares the uterus for pregnancy and the breasts for producing milk for breast-feeding (lactation). In the first a half of the menstrual cycle, oestrogen stimulates the growth of the milk ducts. The adrenal glands however, proceed to produce oestrogen and a lady retains her sexual traits. The key members in the female reproductive cycle are the pituitary gland, the ovaries and the uterus and the activities of each are very closely coordinated. The reproductive cycle encompasses a series of occasions that happen regularly each 26 to 30 days throughout the child-bearing period. The reproductive cycle the ovulatory part 97 Ovulation is the important thing event of the menstrual cycle. The levels of progesterone starts to rise towards follicle release, this prepares the endometrial lining of the uterus for implantation.
Diseases - Lymphangioleiomyomatosis
- Microcephalic osteodysplastic primordial dwarfism
- Girate atrophy of choroid and retina
- Mental retardation skeletal dysplasia abducens palsy
- Anthrax
- Congestive heart failure
- Bonnevie Ullrich Turner syndrome
- Small cell lung cancer
- Pagon Bird Detter syndrome
Order oratane 20 mg with amexHistory Taking from Psychotic Patient this affected person often suffers from hallucination skin care yang bagus untuk jerawat purchase oratane 20mg otc, delusion acne 2016 purchase 20 mg oratane fast delivery, flight of ideas acne 4 year old cheap 5mg oratane free shipping, feeling of persecution skin care during pregnancy purchase oratane 10 mg without prescription. So the interviewer has to calm, quiet, perceive the patient as a lot as possible. History Taking from the Demented and Delirious Patient Demented patient has misplaced his intellectual reminiscence, turns into confused from their environment z Delirious patient has altered level of consciousness-as a result of which he behaves incorrectly together with his environment Both kinds of sufferers undergo from concern. Hence, during questionnaire to those sufferers, the interviewer should be calm, quiet and watch out for that type of questions, which can be harmful to the patients z Patient with organic mental syndrome is lucid, often becomes disorientated, has defect in attention, reminiscence and thought. After few minutes, the interviewer asks similar questions and he should z Art of Interviewing to a Patient 19 verify whether the patient gives similar reply or not. As the affected person turns into stabilized, the interviewer can take detailed history and will do accordingly. History Taking from Patient Suffering from Cancer Patient with cancer has 5 major concerns: 1. Fear of mutilation-women with mastectomy could suffer from a worry of rejection by the community as no longer being a whole lady. Patient always thinks of his inevitable mortality very quickly, as a end result of the pathologic course of at all times progresses very quick. Physician is at all times afraid of the patient, as a outcome of he may ask the progress of the disease. In this case, interviewer must be particular in asking history, as a end result of, it might make the patient irritated, explosive. Because he has to examine the entire physique in spite of no abnormality in any system other than the involved system for which he has been admitted in this hospital Draping of the patient could be very important for keeping the privateness of the patient. This helps within the following methods: this helps to pay attention the examination space this draws confidence of the patient this attracts respect from the patient. Tangential gentle is required for seeing: � Jugular venous pulsation � Thyroid gland � Apical impulse. Because, it could shadow on the surface-so that contour, elevation, melancholy, pulsations could additionally be seen. Primary place of the affected person and the examiner: z Patient should be examined from his right facet. This position is important for having following advantages: is reliable to see jugular venous pulse from proper It Placement of hand for palpation of apical impulse is comfortable Palpation of belly organs, corresponding to liver, spleen, and kidney is much less complicated and cozy the examiner can transfer for examination of the extremities to the foot end or left hand side. In case of cellular affected person: Sitting position: � General survey � Examination of head � Examination of neck � Thyroid gland � Cervical lymph node � Anterior and posterior part of chest � Breast � Few elements of nervous system examination-mental standing, orientation, cranial nerves, cerebellar function, higher extremities � Palpation of aortic and pulmonary space. Lying supine with head finish of the physique raised to forty five diploma position-Jugular venous wave, carotid artery, tricuspid space Supine place with 30� elevation of the top finish and rotation barely in the course of left-mitral area for murmur and different abnormal sound sitting place with leaning forward-tricuspid and aortic In space. Lying in supine place in flat bed: � Face � Anterior neck � Anterior thorax � Breast � Abdomen � Axillae � Pubic space � Genital space � Upper and lower extremities � Plantar response. Supine with flexed, kidnapped and externally rotated hip and knee flexed place: � Pelvic examination � Rectal examination. Art of Interviewing to a Patient 23 the next strategies of examination are often done: z Inspection: It means shut remark of: Skin Facial expression Body habitus Eye movements Any thoracic asymmetry, deformity, fullness, abnormal motion Abdomen-size, shape, lesion, venous prominence Cardiovascular system-jugular venous pulsation, irregular precordial pulsation, aortic and pulmonary space Height Weight Body mass index. To Analysis of Data Data collected from history-subjective knowledge Data collected from bodily examination-objective knowledge Now compilation of subjective and objective information can be done in the following ways. If a affected person complains of headache, then it might signify: Infection Vascular Trauma Metabolic Neoplastic Nutritional. If associated loss of consciousness it might recommend: Vascular Traumatic Associated cerebral involvement in case of meningitis. If the affected person, his or her celebration are educated or understand the issue, then she or he will proceed. Age of the patient: � If the patient is younger, the patient in all probability is suffering from one illness. Timing of sickness: � If the patient suffers from pharyngitis 1 month in the past, latest history of fever, cough, chest pain will not be related to earlier pharyngitis. In this case, it might be due to: Involvement of brain because of increase blood ammonia degree Decreased micturition due to hepatorenal syndrome unless proved in any other case. After assortment of data-both subjective and objective, the interviewer should compose the data with proper interpretation. By asking a number of relevant questions, he ought to exclude some of the differential diagnoses earlier than doing investigations. Deviation of temperature by more than 4�C above or beneath the normal is warning mobile dysfunctions. Site of Measuring Temperature Rectum, mouth, ear, axilla and groin Rectal temperature is about zero. It is far larger in mouth breather or tachypneic affected person, because oral temperature is low on this affected person Axillary temperature is about 1. Diurnal Variation of Body Temperature For daytime employees: Minimum temperature at three:00 to 4:00 am rises slowly to maximum between eight:00 to 10:00 pm For night-time staff: this pattern is reversed. Causes of Decrease or Increase in Oral Temperature Tachypneic patient (tachypnea lower oral temperature by 0. Axillary Temperature It should be averted because it is rather inaccurate In hemiparesis patient, affected website all the time exhibits decrease temperature. Time of Recording of Oral Temperature Three minutes for old thermometer mannequin One minute for new thermometer mannequin. Temperature Physiology Hypothalamus maintains a set-point for temperature Autonomic nervous system regulates the blood flow from the inner organs to skin and the sweat glands. Conductive heat loss may be done by: Dilatation of capillaries Increasing blood move in course of cutaneous capillaries. At that point the patient requires shade, cooler environment and to be less energetic. When the physique temperature is low, the affected person tries to increase the core temperature by: Shivering-generates warmth in muscular tissues Behavioral adaptations-like placing on clothes or entering heat setting. Pathophysiology of Elevated Temperature Release of endogenous pyrogen (Interleukin-I) triggered by tissue necrosis, infection, irritation and tumors improve the temperature set-point. When set-point is reached, skin turns into warm, moist and flushed; in some circumstances skin temperature is normal or subnormal, however core temperature is markedly elevated. Temperature elevation is usually accompanied by tachycardia, he turns into comfy in warm environment. Physical Examinations 29 New set-point and the fever curve dynamics rely upon explicit pathophysiologic process that varies in accordance with the disease course of. As the disease resolves gradually, the set-point of temperature resolves briefly or completely, marked by sweat and flushing of the physique. Night sweat happens in: Chronic infectious illness Chronic inflammatory illness Malignancies. Tertian fever: Here fever paroxysms are separated by a day having normal temperature Example: Plasmodium vivax.

Discount oratane 5 mg onlineCauses: Immune: Contact dermatitis Endocrine: Atrophic vulvovaginitis Infections: Candidiasis, fungal infections, abscess of mucosal glands acne 4 months postpartum discount oratane 40 mg fast delivery. Atrophic vulvo vaginitis: Vulva is thinned, inelastic, simply irritated and inflamed skin care japanese product oratane 20 mg on-line. Causes: Inflammatory: Granulomatous illness Infections: Condyloma lata, condyloma acuminata, histoplasmosis acne quizzes buy cheap oratane 30mg on line. Diffuse swelling of vulva: Causes Lymphatic obstruction Systemic venous strain is high in case of right ventricular failure or constrictive pericarditis and edema reached above thigh and inguinal ligament acne q-4 scale buy cheap oratane 30 mg. Swelling of labia majora: Hematoma: Large, painful, bluish swelling-occur, inside few hours of trauma. Cellulitis Labial hernia: Invagination of peritoneal pouch descends from abdomen into labia majus. Absence of larger vestibular gland: Bartholin gland cyst is fairly common and asymptomatic. When vaginal discharge is cloudy containing white blood cells and excessive mucus-it is pathological. Causes: Inflammatory: Dermatitis Endocrine: Atrophic vaginitis Infections: Bacterial, Fungal, Candida Trichomonal: Mycoplasma, Gardnerella Vulval and cervical most cancers. Genitalia 1435 Vaginitis: Bacterial vaginitis: Most common in women of child bearing age. Cytolytic vaginitis: Lactobacillus overgrowth decreases pH of vaginal fluid-leading to breakdown of epithelial cells and irritation. Vaginal Mass It may be: z Primary z Secondary to mass in cervix, uterus, rectum, bladder. Rectovaginal Pouch Mass: It is most dependant pouch in between rectum and vaginal wall. Masses are: z Ovary z Carcinoma colon z Bowel loops z Endometrium z Ovarian carcinoma z Accumulation of pus, fluid, blood from stomach. Opening could be recognized as a patch of induration on the posterior wall of vagina seen through vaginal speculum. Pathophysiology-columnar epithelium of endocervix becomes vulnerable to infection with Candida, gonorrhea, Chlamydia, herpes or Mycoplasma. Cervical eversion: Outward extension of nonulcerated red mucosa via cervical os-due to migration of endocervical tissue onto visible portion of cervix. Cervical hypertrophy: Lips of cervix of parus girl become elongated and hypertrophic. But funds is in its normal place, cervix retains its regular colour in hypertrophy. Cervical polyp: Pedunculated, pink delicate benign tumor protrudes through cervical Os. Stuart McKechnie Timothy Walsh Metabolic response to injury, fluid and electrolyte balance and shock Chapter contents the metabolic response to injury three Fluid and electrolyte stability 9 Shock 18 1 the metabolic response to harm To improve the possibilities of surviving injury, all animals have a complex set of mechanisms that act domestically and systemically to restore the physique to its preinjury situation. While these mechanisms are vital for survival in the wild, in the context of surgical injury they can be harmful. By minimizing and manipulating the metabolic response to damage, surgical mortality, morbidity and restoration instances may be tremendously improved. An understanding of the metabolic response to injury is therefore fundamental to trendy surgical follow. Reduction of the metabolic (or stress) response to surgical procedure has improved scientific outcomes in surgical patients. The acute inflammatory response Inflammatory cells and cytokines are the principal mediators of the acute inflammatory response. Physical harm to tissues ends in local activation of cells corresponding to macrophages that release a big selection of cytokines (Table 1. Other proinflammatory (prostaglandins, kinins, complement, proteases and free radicals) and antiinflammatory substances similar to antioxidants. The medical situation of the affected person is dependent upon the extent to which the inflammation remains localised in addition to the stability between these pro- and antiinflammatory processes. In the ebb phase through the first few hours after damage, sufferers have been chilly and hypotensive (shocked). When intravenous fluids and blood transfusion turned obtainable, this shock was typically found to be reversible and in different cases irreversible. If the person survived the ebb phase, sufferers entered the flow phase, which was divided into two parts. The preliminary catabolic flow part lasted a few week and was characterised by a excessive metabolic fee, breakdown of proteins and fat, a web loss of body nitrogen (negative nitrogen balance) and weight loss. Over 2�4 weeks, there then followed the anabolic move part during which protein and fats stores were restored and weight achieve occurred (positive nitrogen balance). Modern understanding of the metabolic response to damage is still based on these basic rules. The endothelium and blood vessels the expression of adhesion molecules upon the endothelium leads to leucocyte adhesion and transmigration. Colloid particles (principally albumin) leak into injured tissues, leading to oedema. The exposure of tissue issue promotes coagulation, which, along with platelet activation, decreases haemorrhage however at the danger of causing thrombosis and tissue ischaemia. Factors mediating the metabolic response to injury the metabolic response is a fancy interplay between many body techniques. Activation of the sympathetic nervous system results in the release of noradrenaline from sympathetic nerve fibre endings and adrenaline from the adrenal medulla, leading to tachycardia, increased cardiac output, and modifications in carbohydrate, fats and protein metabolism (see later). Interventions that reduce sympathetic stimulation, such as epidural or spinal anaesthesia, might attenuate these changes. This occurs both because of direct gland stimulation or due to adjustments in feedback mechanisms. Afferent nerve impulses and sympathetic activation Tissue injury and irritation lead to impulses in afferent ache fibres that attain the thalamus by way of the dorsal horn of the spinal twine Bacterial invasion Macrophage activation � Phagocytosis � Cytokine launch � Prostanoid launch � Protease launch Neutrophil accumulation � Phagocytosis � Cytokine launch � Protease launch Stimulation of afferent nerve impulses Haemorrhage into injured tissue Plasma cascades activated � Coagulation/platelets � Complement Neutrophil�endothelial cell adherence and neutrophil migration Endothelial activation � Vasodilatation � Increased capillary permeability Fluid and protein leak � Tissue oedema. This sometimes lasts 24�48 hours, with the extent (many litres) and duration (weeks and even months) of this loss dependent on the kind and severity of tissue injury. The neuroendocrine responses to hypovolaemia try to revive normovolaemia and maintain perfusion to vital organs. Aldosterone secretion from the adrenal cortex is elevated by: Activation of the renin�angiotensin system. Renin is released from afferent arteriolar cells within the kidney in response to decreased blood strain, tubuloglomerular feedback (signalling by way of the macula densa of the distal renal tubules in response to changes in electrolyte concentration) and activation of the renal sympathetic nerves. Typically, urinary sodium excretion decreases to 10�20 mmol/24 hours (normal 50�80 mmol/24 hours) and potassium excretion will increase to >100 mmol/24 hours (normal 50�80 mmol/24 hours). Despite this, hypokalaemia is comparatively uncommon because of a internet efflux of potassium from cells. Blood flow�conserving measures Hypovolaemia reduces cardiac preload, which results in a fall in cardiac output and a lower in blood circulate to the tissues and organs.
Oratane: 40 mg, 30 mg, 20 mg, 10 mg, 5 mg
Buy oratane 30 mgThe course of standing asthmaticus based mostly on auscultation: z In delicate bronchial asthma: Site of obstruction within the central airways Bronchial wall fluttering produces random monomorphic wheezes transmitted upwards (to the mouth) and downward (to the chest wall) acne doctor generic oratane 30mg with mastercard. Subsequently: z Airway fluttering moves to peripheral airways z Airflow is so sluggish acne description trusted oratane 10mg, that it fails to generate vibrations skin care with peptides discount 5mg oratane with mastercard. Relationship with pulsus paradoxus Pulsus paradoxus has a direct relation with hypercapnia in youngsters with standing asthmaticus acne juice cleanse generic 20 mg oratane mastercard, so acts as oblique monitor of hypercapnia. Stridor: z High pitched z Inspiratory z It signifies higher airway obstruction z Louder over the neck. This layer is lubricated by skinny film of fluid, so that during normal respiration the pleural surfaces glide on each other silently z During pleural irritation, pleural surface are lined by fibrin and inflammatory/neoplastic cells, in consequence the roughened pleural surfaces rub in opposition to each other during respiration producing grating sound-pleural rub z As the fluid accumulates within the pleural house, pleural surfaces are separated, pleural rub disappear So pleural rub in pathgnomonic of pleural inflammation. Most common causes of pleural rub: z Inflammation: Infective-pneumococcal, staphylococcal, gram �ve micro organism Noninfective-collagen vascular disease. Type of transmitted voice sounds are: z Bronchophony: this is heard over the chest areas distant from both bronchi or larynx-but as clear heard as over central bronchi or larynx z Pectoriloquy: the sound heard is clear and intelligible phrases over the chest in the type of both: Whispering (whispering pectoriloquy) Speaking (spoken pectoriloquy). Significance of this maneuver: It suspects abnormal sound transmission alongside the tracheobronchial tree throughout the lungs when suspecting consolidation. The alveolar air acts as low-pass filter, eliminating excessive frequency sounds (>3000 Hz) and most of low frequency sounds (100�300 Hz) attain the chest wall. This filter additionally eliminates high frequency parts of vowels so known as formants. Because recognition of vowels is important for comprehension of phrases, elimination of formants by the normal lung, hence voice sounds heard on the chest wall is low pitched, unintelligible, mumbles. But in case of consolidation-solid lung (fluid or solid) can transmit greater frequencies, so transmitted vowels become louder, clear and intelligible. Mechanism of E to A change: Consolidation extending from chest wall to tracheobronchial tree produce E to A change. The commonest causes of consolidation: z Filling of alveoli with: Pus Fluid Blood. The exception is-patient with collapsed bronchi or obstructed bronchi nonetheless manages to transmit excessive frequency sound via lung parenchyma instantly. Transformation of E to A in vocal resonance in consolidated lung: z E is a mixture of excessive and low frequencies-high frequencies are 2000 to 3500 Hz and low frequencies are one hundred to 400 Hz vary A is a mixture of high and low frequencies-low frequencies are higher than the low frequencies of E (600 Hz). Disease Vesicular Late-inspiratory crackles at bases (resolved with deep breath) Late inspiratory crackles Late inspiratory crackles Mid inspiratory crackles Early inspiratory crackles Rub above effusion Absence Trachea Fremitus Percussion note Breath sound Adventitious sound Vocal resonance � Normal Midline Normal Resonant � Consolidation (pneumonia hemorrhage) Bronchovesicular Vesicular Vesicular Absent over effusion bronchial above effusion Midline Increased Woody uninteresting Bronchial (tubular) Increased � Pulmonary fibrosis Midline Increased Dull Absent Absent Absent Egophony above effusion absent above effusion Contd. Shape: Resembles a truncated cone, one and half occasions of the closed fist of a man Size: 12 cm � 9 cm Weight: male: 320 � seventy five g In feminine: 275 � 70 g. Extends superiorly as much as bifurcation of pulmonary trunk and inferiorly up to coronary groove It receives pulmonary veins on the best and left aspect of left atrium It receives superior and inferior vena cavae on superior and inferior ends of right atrium. Diaphragmatic (inferior) surface: Mainly by left ventricle and part of the proper ventricle. Having a chink of right atrium on its proper and left ventricle on its left Right atrium is separated from right ventricle by right atrioventricular sulcus, additionally called coronary sulcus, containing right coronary artery and an excellent vein of the center that drains into proper atrium by coronary sinus Right ventricle is separated from left ventricle by interventricular sulcus containing left anterior descending artery. Its apex extends upwards and to the left of ascending aorta, growing the capability of the ventricle Superior vena cava opens at its higher part having no valve at its orifice Inferior vena cava opens at its decrease end having a rudimentary valve at its orifice (Eustachian valve) Coronary sinus lies on the posterior a part of the coronary groove and receives blood from cardiac veins. This known as patent foramen ovale Triangle of Koch: It is bounded anteriorly by base of septal cusp of tricuspid valve, behind by coronary sinus and above by tendon of todaro-a fibrous ridge extending from a fibrous physique to the left horn of inferior vena cava. Shape is conical Apex of infundibulum has pulmonary orifice having three semilunar cusp Free edge of each cusp has thickening at its middle called Nodule Arantii. It has no rim or limbus Its appendage initiatives anteriorly and overlaps infundibulum of left ventricle. Inflow component Anteromedial leaflet of mitral valve extends from posteromedial wall of the septum to the anteromedial wall of the left ventricle. It separates the left ventricular cavity into influx tract and outflow tract Mitral orifice is elliptical, guards the left atrioventricular orifice Inflow tract is funnel shaped; accommodates mitral equipment, which direct the circulate of blood anteriorly, inferiorly and to the left. Outflow part It is conical formed, clean walled, nonmuscular superoanterior outflow a part of aortic vestibule leading to aortic orifice and aortic valve It is bounded by: Inferior floor of anteromedial mitral cusp Left ventricular free wall Ventricular septum. Aortic orifice is surrounded by a fibrous ring to which proper, left and posterior cusps are hooked up It directs the blood circulate anteriorly and superiorly making an angle of 90� with the influx tract in path of ascending aorta Aortic orifice is guarded by three semilunar cusp. It separates infundibulum from the skin of the guts With rising age, septum turns into sigmoid and interventricular part of the membranous half increases. Apical Part of Ventricle Extensive fine trabeculation greater than the proper ventricle is present right here. It has no tensor equipment like, chordae tendineae, papillary muscle Three cusps-two of them are named in accordance with the origin of the coronary arteries-right coronary cusp, left coronary cusp. Third one is noncoronary cusp Free edge of each cusp is thickened to type a nodule Anterior mitral leaflet has a fibrous continuity with aortic cusp- the place aortic and mitral rings are fused together Annulus-2. Chordae tendineae are hooked up to free edges of ventricular surfaces of the cusps like parachute Since chordae are connected to the adjacent sides of the cusps- they stop: Separation of cusps Inversion of the cusps Prolapse of the cusps into right atrium Backflow of blood from proper ventricle into proper atrium during forceful ventricular contraction. Papillary muscle tissue are triangular in shape with their apices hooked up to the more than one cusp via the attachment with the chordae Papillary muscles contract before the start of right ventricular contraction. Blood current within the pulmonary sinus prevent the cusps from sticking the wall of the pulmonary trunk. Arterial Supply of the Heart Heart is equipped by the coronary arteries lie deep to the epicardium embedded in fat. Left Coronary Artery Origin: It arises from left anterior coronary sinus Courses: It passes in between left pulmonary trunk and left auricle and divides into two branches: 1. Left circumflex artery Small branch, after its origin it follows the coronary sulcus on the left border of the guts to the posterior floor of the heart It terminates within the posterior coronary sulcus before reaching the crus and anastomosing with branches of right coronary artery. Branches In right coronary artery dominant circulation: Left atrium (1�2 branches) Lateral free wall of left ventricle (1�2 obtuse marginal branches). Left anterior descending artery Origin and courses this artery runs along the anterior interventricular groove towards the apex It winds around the inferior border of heart and anastomose with posterior interventricular branch of right coronary artery. Branches 2 to 6 diagonal branches-supplies anterolateral wall of left ventricle three to 5 septal branches-supply the interventricular septum. Right coronary artery Proximal proper coronary artery-from its origin in right coronary sinus and origin of proper ventricular branch Mid proper coronary artery-between the origin of right ventricular department and posterior descending artery Distal right coronary artery-portion distal to origin of posterior descending artery. Anterior Cardiac Veins They drain the anterior right ventricular wall It immediately drains into proper atrium. Thebesian Veins (Venae Cordis Minimi) Drain the myocardium Directly drains into proper atrium. It consists of cardiac muscle cells and specialized conducting fibers for initiating impulses and conducting the impulses through the heart. So in operative procedure involving the above valves or membranous a part of ventricular septum-the bundle is liable to be injured. Bundle Branches Right bundle branch: It arises from distal portion of bundle of His within the form of wire like structure, travels alongside the septal and moderator bands in the direction of anterior tricuspid papillary muscles Left bundle department: It is broad fenestrated sheet-present in subendocardial space. It progresses like fan like construction It has two divisions: Thin anterosuperior and thick posteroinferior fascicles. Blood provide of bundle branches: Septal perforators of: Left anterior descending artery Posterior descending coronary artery. Terminal Purkinje Fibers these connect the decrease end of bundle of His to endocardial surface of each ventricles in the type of interweaving network 274 Clinical Methods and Interpretation in Medicine these fibers are connected within the papillary muscular tissues at the base of the ventricles.

Buy 40mg oratane fast deliveryThe lens supplies the remaining variable focusing power and serves to further refine the main target skin care face cheap 30mg oratane with amex, permitting the eye to focus on objects at different distances acne keloidalis discount oratane 40 mg with visa. Ciliary muscle is a part of the ciliary physique skin care 30 years old discount 5mg oratane with visa, divided into ciliary muscle skin care network barnet ltd buy generic oratane 5 mg on-line, ciliary processes and pars plana. The surface of the attention is repeatedly bathed in tears predominantly secreted by the lacrimal gland, conjunctival secretions are also added. Mostly it is a transparent skinny tissue designed to seize photons of sunshine and initiate processing of the image by the mind. There are two forms of receptors: rods and cones: the outer section incorporates light sensitive visible pigment molecules opsins in stacked disks (rods) or invaginations (cones). Rods are mainly liable for peripheral vision; imaginative and prescient under low light circumstances, and are extra prevalent within the mid-peripheral and peripheral retina. The retina the visible system pathways to the mind the sclera this is derived from interwoven collagen fibrils of varying widths inside ground substance maintained by fibroblasts. At the optic chiasma, axons from the medial half of every retina cross to the alternative side, forming pairs of axons from every eye the left and right optic tracts. The crossing of the axons results in every optic tract carrying data from both eyes, the left carries visual information from the lateral half of the retina of the left eye and the medial half of the retina of the best eye, whereas the right one carries visual data from the lateral half of the retina of the proper eye and the medial half of the retina of the left eye. With the lens it transmits and focuses light into the attention, and protects the internal ocular constructions. The visual cortex Located in the occipital lobe of the mind, where the final processing of the neural alerts from the retina takes place and vision happens. The occipital lobe is on the most posterior portion of the mind, with six separate areas in the visible cortex. The ear the auditory tube (eustachian tube) is the communication between the center ear and the nasopharynx. The blood supply is derived from numerous arteries, primarily from the exterior and internal carotid. Chapter 54 Hearing the ear has two key features: to assist with steadiness (equilibrium) and to allow us to hear the sounds around us. The auricle and exterior acoustic meatus (external auditory canal) compose the external ear. The external ear capabilities to gather and amplify sound, which is transmitted to the middle ear. The uneven shape introduces delays in the path of sound assisting in sound localisation. The arterial supply is composed of the posterior auricular artery, the anterior auricular department of the superficial temporal artery, and the occipital artery, which also contributes. The vestibule and semicircular canals are related to vestibular function (balance). The walls of the bony labyrinth are continuous with the encircling temporal bone. The internal features of the bony labyrinth carefully observe the contours of the membranous labyrinth; a delicate, interconnected community of fluid-filled tubes the place the receptors are discovered. The walls of the bony labyrinth are made up of dense bone, apart from two small areas located near the cochlear spiral. The spherical window consists of a thin, membranous partition separating the perilymph of the cochlear chambers from the air-filled center ear. Collagen fibres connect the bony margins of the oval window on the base of the stapes. Perilymph, which closely resembles cerebrospinal fluid, flows between the bony and membranous labyrinths. The bony labyrinth could be subdivided into the vestibule, three semicircular canals and the cochlea. The center ear the vestibule the key operate of the center ear (tympanic cavity) is that of bony conduction of sound by way of transference of sound waves in the air collected by the auricle to the fluid of the internal ear. The center ear extends from the tympanic membrane to the oval window containing the bony conduction parts of the ossicles. The fluid-filled chambers throughout the vestibule are usually steady with the semicircular canals. The cochlea Tympanic membrane the tympanic membrane is an oval, skinny, semi-transparent membrane separating the external and middle ear. Air vibrations collected by the auricle are transferred to the cell tympanic membrane, which then transmits the sound to the ossicles. A bony, spiral-shaped chamber, it accommodates the cochlear duct of the membranous labyrinth. Blood provide to the inside ear the interior auditory artery supplies the whole membranous labyrinth passing through the inner auditory meatus, dividing into three branches. Ossicles the organ of Corti From the deep surface of the tympanic membrane to the oval window is a series of movable bones, the ossicles, malleus (hammer), incus (anvil) and stapes (stirrup). These serve to transmit and amplify sound waves from the air to the perilymph of the internal ear. This is located within the cochlea and is referred to as the receptor organ of listening to. When an individual is continually exposed to an odour, the notion of the odour will diminish and stop inside minutes, the loss of notion only includes that particular odour. We are always assessing the air that we inhale, this can alert us to potential risks, for instance, the presence of smoke. This aqueous secretion incorporates mucopolysaccharides, immunoglobulins, proteins (such lysozyme) and numerous enzymes. A pigmented-type of epithelial cell can be positioned within the nasal mucosa (membrane), the explanation for its pigmentation is unknown. The nasal epithelium incorporates the receptor cells, possessing a terminal enlargement above the epithelial floor, with approximately 8 to 20 olfactory cilia. The trigeminal nerve (cranial nerve V) sends fibres to the olfactory epithelium detecting caustic chemicals, similar to ammonia. The cribriform plate of the ethmoid bone, separated at the midline by the crista galli, includes a selection of small foramina, the olfactory nerve fibres traverse this. The nostril incorporates between 10 and 100 million olfactory receptor neurons which line the olfactory epithelium that lines the nasal mucosa in the nasal cavity which might be capable of detect odours. The ends of the axons kind spherical glomeruli, each of them receives enter from the same olfactory receptor. Specialised receptor cells (olfactory receptor neurons) of the olfactory epithelium in the nostril detect smells. Olfaction depends on the binding of odourant molecules to receptors that are located on the receptor cells. Olfaction has complicated techniques of coding, displaying differing methods for coding the receptor stimulus.
SANQI (Panax Pseudoginseng). Oratane. - Are there safety concerns?
- Dosing considerations for Panax Pseudoginseng.
- What is Panax Pseudoginseng?
- Bleeding, improving blood flow, pain, swelling, high cholesterol levels, chest pain (angina), high blood pressure, dizziness, sore throat, prostate cancer, and other conditions.
- How does Panax Pseudoginseng work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96872

5 mg oratane visaThis test is optimistic in: Retrocecal appendicitis: Positive in proper leg Intrapelvic pus-Positive in each legs acne 19 years old purchase 20mg oratane with visa. This test is positive in: Retrocecal appendicitis Any collection of pus of blood on psoas muscle acne in children buy oratane 20 mg lowest price. Rectal tenderness: There is tenderness during rectal examination in case of rectal appendicitis acne 6 months after stopping pill cheap 20 mg oratane amex. Eyelids: Two eyelids-upper eyelid and decrease eyelid: z Upper eyelid is larger acne on scalp buy generic oratane 5mg on line, more movable z Lower eyelid is smaller z Both eyelids meet one another at medial and lateral angles z Palpebral fissure is the realm between the eyelids z During close position: Upper eyelid covers full eye z During opened eye: Upper eyelid covers higher margin of cornea Lower eyelid covers decrease margin of cornea. Orbicularis oculi-its tone and contraction are answerable for closing of eyelids, when levator palpebrae superior is relaxed. Both of them are steady with one another on the lateral fringe of aponeurosis of levator palpebrae superioris. Glands open into lateral a half of superior fornix by twelve ducts Nerve provide: Parasympathetic secretomotor nerve provide: Lacrimal nucleus of facial nerve Preganglionic fibers attain pterygopalatine ganglion via nervus intermedius, and larger petrosal nerve Postganglionic fibers be part of maxillary nerve Zygomatic branch of zygomaticotemporal nerve Lacrimal nerve Lacrimal gland Sympathetic postganglionic nerve supply: From nerves spherical internal carotid plexus Deep petrosal nerve Nerve of pterygoid canal Maxillary nerve Eye Disease 671 Zygomatic nerve Lacrimal nerve Lacrimal gland Lacrimal Duct Tear circulates throughout cornea to lacus lacrimalis Tear enters into lacrimal canaliculi by way of lacrimal punctum Canaliculi open into lacrimal sac Lacrimal sac lies behind medial palpebral ligament and upper blind finish of nasolacrimal duct (1. This lacrimal fold prevents air from getting into into nasolacrimal duct and reaching lacrimal sac. Sclera: � Opaque posterior fibrous white half � It is pierced by optic nerve space is called lamina cribrosa. Cornea: � It is the continuation of sclera-inferiorly � It is in contact with aqueous humor posteriorly � Blood supply-avascular, no lymphatic drainage- nourishment occurs through diffusion from: � Aqueous humor � Capillaries at its edge. Suspensory ligament of iris is attached with its posterior surfaces � Ciliary muscles: They run compound of two types of smooth of muscular tissues: 1. Meridional fibers: They run backwards from sclero corneal junctions to ciliary processes 2. Constricts the pupil: � In relation to accommodation � In presence of shiny gentle. Dilator pupillae dilates the pupil in presence of: � Light of depth � Fright as a result of extreme sympathetic activity. Lens Biconvex clear structure-enclosed in a transparent capsule z It is situated posterior to posterior chamber and anterior to vitreous body, encircled by iris z Lens consists of: Elastic transparent capsule Cuboidal epithelium-confined to anterior surface of the lens Lens fibers-formed from epithelium at the equator of lens make up the majority of fibers. The pull of this ligament makes the elastic lens flattened-so that eye can be targeted on the item. Oculomotor nerve supplies: � Superior rectus � Inferior rectus � Medial rectus � Inferior indirect. Visual axes of each eyeballs remain parallel Simultaneous contraction of medial rectus of one eye and lateral rectus of different eye. It is especially as a result of: � Contraction of each medial recti � Simultaneous relaxation of each lateral recti � Visual axes are shut together. Divergence: Movement of two eyeballs towards temporal side-visual axes of both eyes move away from one another. It is especially due to: � Contraction of both lateral recti � Relaxation of both medial recti. Visual course of During seeking to an object Light rays from the item is refracted and brought to the concentrate on retina. The picture formed is in inverted position, which is made upright by cerebral cortex. Cells answerable for visible course of z Rods: They are responsible for dim imaginative and prescient, evening vision or scotopic imaginative and prescient Total number is 12 million. Function of rods z Responsible for dim imaginative and prescient, evening vision or scotopic vision z Do not resolve particulars or boundaries of the thing (visual acuity) z Do not resolve the color of the object (color vision) z Vision of rod is black, white or combination of black and white, i. Function of cones z They are responsible for light vision, photic vision or day gentle imaginative and prescient z Responsible for acuity of imaginative and prescient z Responsible for color imaginative and prescient. Dark Adaptation It is the process by which the person is in a position to see the thing in dim light. Cause of darkish adaptation Increased sensitivity of rods as a result of increased resynthesis of rhodopsin. Field of Vision Part of exterior world seen by one eye when it in mounted in a single course. Monocular vision: In this imaginative and prescient each eye is used individually for imaginative and prescient of particular object. Visual pathway and website of lesions to be delt during dialogue of 2nd cranial nerve-optic nerve Pupillary reflexes to be delt during discussion of 3rd cranial nerve; optic nerve. Spectrum of colours is-according to wavelengths from maximum to minimum: z Red z Orange z Yellow z Green z Blue z Indigo z Violet. Complementary colour: these are pair of two colours which when combined produce white shade. Color delicate areas of retina z Peripheral a half of retina is devoid of cones-so this space is insensitive to paint, sensitive to black, white and gray solely Eye Disease 681 Central a part of retina-fovea centralis-mostly cones-sensitive to paint z Retinal sensitivity to blue is highest-next green then yellow. For measurement of visual acuity: Following things are used: z Snellen chart z Pinhole occluder z Pocket dimension close to vision test card z Rosenbaun card-in case of bed ridden sufferers. Foreign physique sensation with itchy sensation: Allergic conjunctivitis Winter conjunctivitis. Redness of eye: Trauma Infection Allergy Increased strain in the eyes Occasionally coughing or recurrent vomiting Use of contact lens producing irritation. The main causes are: z Acute conjunctivitis z Acute iritis z Narrow angle glaucoma z Corneal abrasion. The following inquiries to be requested in case of pink eye z History of damage to eye z History of injury to eye in his family z History of coughing or some other straining z History of any related ache z History of any related discharge z Any impact of light z History of sporting contact lens. Involvement of deeper structures: Iritis Uveitis Glaucoma-acute angle Chlamydial conjunctivitis. Spot: May precedes retinal detachment Flashes of sunshine: Aura of migraine Retinal hemorrhage Posterior vitreous detachment. Difficulty in seeing in dim light: Retinal degeneration Vitamin A deficiency Myopia. Colored spots around gentle: Lenticular opacities Corneal opacity Narrow angle glaucoma. Loss of vision: Sudden loss: Due to vascular trigger: � Ischemia-involving-retina, optic nerve or brain � Hemorrhage: � Anterior chamber � Posterior chamber � Vitreous physique � Age associated macular degeneration. Gradual loss: Due to slowly progressive: � Degeneration or deposition � Cataract � Open angle glaucoma. Painful lack of imaginative and prescient: � Uveitis-anterior � Keratitis � Optic neuritis � Giant cell arteritis � Disease of orbit. Painless loss of imaginative and prescient: � Cataract � Diabetic neuropathy � Optic neuropathy � Retinal vein occlusion, retinal artery occlusion � Open angle glaucoma. Transient loss of imaginative and prescient: Due to transient ischemia: � Giant cell arteritis � Amaurosis fugax � Vertebra basilar insufficiency.
Order oratane 20mg onlineTypes of uvula Absent uvula: Surgical removing for obstructive sleep apnea syndrome acne treatment for sensitive skin discount oratane 5 mg with visa. Bobbing uvula: Rhythmic pulsation of uvula related to aortic regurgitation-Muller sign acne genetics cheap 20 mg oratane visa. Localized reddening of anterior pillars Localized crimson coloured nontender reddening of anterior pillars acne antibiotics discount 5 mg oratane with mastercard. Causes of exudates on posterior pharynx Viral Streptococcal Epstein-Barr virus Mycoplasma pneumonia Chlamydia pneumonia Neisseria gonorrhoeae Candidiasis Diphtheria acne tretinoin cream 005 generic 30mg oratane overnight delivery. Abdomen ought to be exposed from xiphisternum to symphysis pubis and if required genitalia should be uncovered Hernia sites ought to be properly uncovered. Causes: Normal Cachexia Starvation Malignant disease-carcinoma of esophagus and stomach. Localized distension: Symmetrical round umbilicus-small bowel obstruction Asymmetrical involvement: � Liver � Spleen. Shape of stomach on lateral inspection Cupid bow profile: Midpoint between two bow branches coinciding with umbilical retraction because of localized peritonitis. Umbilicus Normally umbilicus is slightly retracted and inverted-it is the center of stomach. Abnormalities of Umbilicus Protuberances: Most widespread protuberances are: Eversion: Umbilical scar is everted and flushed with pores and skin causes are: � Obesity with flushed stomach � Ascites. Inspection of Abdominal Wall Abdominal respiratory motion: During inspiration abdomen expands and through expiration abdominal wall retracts 618 Clinical Methods and Interpretation in Medicine In respiratory muscle weakness-respiration turns into abdominal-this is called stomach paradox. Normally stomach movement is equal in each side: case of peritonitis, the belly movement is absent- In this is known as silent stomach. It is normally because of: � Prevention an infection unfold within the peritoneal cavity � Prevention unfold of ache of peritoneal irritation. Visible peristalsis can be seen in following conditions: � In case of pyloric stenosis: � In normal condition-peristaltic wave-a sluggish wave passes from left to proper hypochondrium. In long-standing obstruction with gastric dilatation, the swelling may be current in left mid and lower quadrants. Abnormal pores and skin markings: Ecchymoses: these are bruises because of intraperitoneal or retroperitoneal hemorrhage-seen in periumbilical areas or in the flanks: these are generally seen in: � Necrotizing acute pancreatitis (3%) � Ruptured pregnancy (1%) Striae. The websites of scars are: � Right subcostal scar � Midline incision and scar � Paramedian scar � Suprapubic scar � Appendectomy scar � Hernia scar. Abdominal venous sample: the collateral venous circulation of belly wall-due to obstruction. Caput medusae present tuff of veins radiating from umbilicus as spokes of a wheel or nest of snake; draining the blood from portal veins to inside mammary rostally and inferior mammary caudally through subcutaneous veins of belly wall. Release the stress of the caudal end of vein and then the rostral end of the vein. By above methods, path of venous move may be decided: Blood flow from below upwards-inferior vena cava Blood circulate from above downwards-superior vena cava Blood flow away from umbilicus-portal vein obstruction. Pigmentation on the belly wall: Linear pigmentation from beneath the umbilicus-Linea nigra- indicators of being pregnant. Signs of constant software of heat-commonly related to chronic pancreatitis. Inspection of hernial websites: To see any obvious thing coming out-in normal place, throughout any kind of straining (coughing, sneezing). Light palpation must be carried out to defect: Stiffness of rectus abdominis muscles To detect superficial lump tenderness To detect rebound tenderness. Generalized-over whole abdomen-generalized peritonitis- in this case the stomach will be board-like. In few cases stroking the stomach gently with pin-may produce increased sensation because of inflammation of parietal peritoneum. As a results of expansile pulsation, your arms will be apart away from each other. By similar strategies detect rightside of abdominal aorta by transferring fingers to right aspect. Common femoral vessels: They can be palpated by inserting the fingers just below the inguinal ligament, midpoint between symphysis pubis and anterior superior iliac backbone. They are firm, rounded, confluent, fastened in umbilical area and epigastric area along left border of aorta. Palpation of liver: During liver palpation-following info ought to be sought. Inferior margin of liver will contact the tip of the fingers with all the above maneuvers, repeat these maneuvers whereas transferring the palms from lateral to medial areas and cross from proper hypochondrium to epigastrium. Tenderness may happen from: Congestion of liver-due to distension of the hepatic capsules. Significance of firm and exhausting margin of liver: Very onerous margin-tumor Sharp margin-cirrhosis Margin neither sharp nor hard-congestive Nodules on the liver: Large nodules nontender-neoplasm, metastatic carcinoma Small nodules-cirrhosis. The circumstances responsible are: Tricuspid regurgitation Constrictive pericarditis. Above two situations may be distinguished by: Inspiratory increase in systolic pulsation magnitude seen in tricuspid regurgitations (especially held in mid or late inspiration) however not in constrictive pericarditis. Palpability of inferior border of liver is nonspecific, as a end result of it could be palpable in following situations in absence of hepatomegaly: Chronic obstructive lung disease Pleural effusion Pneumothorax. Problems Regarding Liver Jaundice: It is outlined as yellow to vary discoloration of skin and mucous membrane and bulbar conjunctiva. The pseudojaundice is as a outcome of of: Subconjunctival fats: this is assortment of yellow fats in conjectural folds, never to pericorneal area. It consists of central arteriole (body of the spider), and radiating vessels (legs of spider). They may be differentiated from: Cherry angioma: Round venous, associated with aging. The circumstances where spider nevi are generally discovered: Liver disease-alcoholic cirrhosis Combination of alcohol and hepatitis C associated Pregnancy-2nd to fifth months of gestation Thyrotoxicosis Malnutrition. Mechanisms concerned in cirrhosis are: Increased ratio of serum estradiol to testosterone. Fetor hepaticus: It is a special odor coming out of the mouth in hepatocellular disease with porto-systemic shunt. If happens because of accumulation of dimethylsulfide within the breath- simulating rotten egg and garlic. It may happen: Hepatoma Ten % instances of metastasis Much much less widespread in localized or disseminated inflammatory processes. Hepatic arterial murmur: It occurs in: Hepatoma Hepatic secondary few cases hepatitis. Difference between venous hum and arterial murmur: Arterial murmur is systolic Venous hum is each systolic and diastolic Venous hum originates from a communication between umbilical vein and abdominal wall veins. The gallbladder could also be palpated within the following conditions: Mucocele of gallbladder: When gallstone is impacted at the neck of uninfected, collapsed, empty gallbladder. Mucus is repeatedly secreted into the gallbladder making it distended and palpated. Carcinoma head of pancreas: this enlarged head of pancreas compresses and obstructs the widespread bile duct, making gallbladder passively distended.
Buy oratane 10mg onlineThe depth and position of the bladder can be gauged by the free aspiration of urine by way of this needle acne jeans review buy 40 mg oratane visa. Entry into the bladder is confirmed by the loss of resistance, at which level the catheter is superior as the trocar is withdrawn acne 1cd-9 cheap oratane 5mg overnight delivery. The catheter should be advanced far sufficient into the bladder in order that the balloon, when inflated, is well within the bladder acne 7061 generic 30mg oratane fast delivery. Contrast research Radio-opaque distinction media could additionally be used to demonstrate the gastrointestinal, biliary, vascular and urinary tracts acne 30 years old generic 20mg oratane fast delivery. They can either be used to stipulate anatomical constructions directly, or else be concentrated physiologically in an organ (indirect imaging). Barium sulphate is insoluble and is used extensively to analyze the gastrointestinal tract. Gastrograffin is a water-soluble contrast medium used if leakage from the gastrointestinal tract into the peritoneal cavity is most likely going. A barium swallow is used to evaluate the oesophagus and a barium meal to analyze the stomach and duodenum. Progress of contrast can be observed by fluoroscopic screening, using a picture intensifier. The risk of life-threatening anaphylactic reactions with the newer, low-osmolar, nonionic brokers is minimal however these are still recognised complications of intravascular administration. Local anaesthetic (mixed with a 1:200,000 concentration of adrenaline if appropriate) is used to supply a field block. The skin and subcutaneous tissue is incised in an ellipse to incorporate the swelling and a aircraft is developed across the swelling. Usually a clean airplane of loose areolar tissue is current around these swellings that can be developed by sharp dissection using scissors. Special care is required in the case of a sebaceous cyst where pores and skin incision ought to encircle the punctum to avoid opening the cyst. After excision is completed, haemostasis is ensured and the subcutaneous tissue approximated using absorbable suture. Imaging Radiological imaging has a central function in the administration of surgical sufferers and should information various therapeutic procedures. A variety of imaging methods at the moment are obtainable that present data on the construction and performance of systems and organs. Further data can be gained after administration of oral, rectal or intravenous distinction. Three-dimensional reconstruction can be performed to assess relationships between constructions and aid within the discrimination of abnormalities. Plain radiography Radiographs account for the best proportion of all imaging examinations. X-rays penetrate the physique and cast a picture either on film or on a fluorescent screen. The image is fashioned by the variations in attenuation of the x-ray beam by various tissues, producing a two-dimensional impression of a three-dimensional construction. On a plain radiograph, bone absorbs most x-rays and seems radio-opaque (white), whereas fuel and fats take in few x-rays and appear radiolucent (dark). If x-ray power (kilovoltage) and publicity time are altered, tissues of varying densities could be visualised. Other calcified tissues, similar to most urinary tract stones, old tuberculous lymph nodes and calcified atheromatous plaques, are radio-opaque. Foreign supplies, corresponding to steel or glass, are additionally radio-opaque, however wood and plastic are radiolucent and invisible to x-rays. Therefore, pointless investigations ought to be averted and radiation exposure of sufferers and workers should be minimised. As the inverse square law determines radiation fall-off with distance, employees should preserve a long way from the x-ray source throughout publicity. The carrying of x-ray-sensitive film badges is used to monitor the quantity of radiation acquired by staff, and protective lead aprons should be worn when employees are in exposed situations. Ultrasonography it is a protected, noninvasive, painless method that enables the visualisation of stable internal organs. Calcified tissue, corresponding to stones, causes an abrupt and marked change in acoustic impedance, resulting in nearly full reflection of ultrasound and a posterior acoustic shadow. Ultrasonography of the pelvis Imaging � 127 is aided by a full bladder, as this provides a fluid-filled, nonreflective window to scan the pelvic organs. Special probes have now been developed for insertion into various body orifices, corresponding to rectum, vagina and oesophagus, and likewise through laparoscopic and endoscopic tools. These probes can be placed closer to the target organ, allowing the utilization of higher-frequency sound that has lower penetration but greater resolution. Ultrasound is reflected from the purple blood cells, the movement of which causes a frequency shift associated to the rate. This is used to generate an audible signal that can be used to evaluate whether or not move is regular or irregular. The time period duplex ultrasonography is used when the gray scale typical ultrasound is combined with Doppler ultrasound. This layer is equipped with two units of nerves, one stimulating the muscular tissues to chill out so that the artery is allowed to widen, and the other one causing the circular muscles to contract, making the artery become narrower. The inner layer of endothelium consists of flat epithelial cells that are packed intently together and which is continuous with the endocardium of the center. The flat cells Capillaries are tiny blood vessels, of roughly 520 micrometres diameter. Capillary walls are just one cell thick, which allows exchanges of fabric between the contents of the capillary and the encompassing tissue fluid. This layer is so thin that molecules similar to oxygen, water and lipids can pass by way of them by diffusion and enter the tissues. Waste merchandise similar to carbon dioxide and urea can diffuse again into the blood to be carried away for elimination from the body. Capillaries are so small the red blood cells need to change its shapes in order to move through them in single file. The move of blood within the capillaries is managed by structures known as precapillary sphincters. These structures are located between arterioles and capillaries and contain muscle fibres that permit them to contract. When the sphincters are open, blood flows freely to the capillary beds of body tissue. Fluid trade between the capillaries and the body tissues takes place on the capillary bed. The strain is at its greatest nearer the center but decreases because the blood moves away from the heart. Three factors regulate blood strain they usually include: neuronal regulation through the autonomic nervous system; hormonal regulation adrenaline, noradrenaline, renin and others; and auto-regulation by way of the renin-angiotensin system composition of the blood, such as a decrease in oxygen level and pH of the blood or an increase in the carbon dioxide level. These receptors send impulses to the cardiovascular centre which in turn enhance the sympathetic stimulation to the blood vessels inflicting a rise in blood pressure.
Order 40 mg oratane mastercardIf carried out skin care knowledge buy oratane 10 mg visa, the interviewer ought to see the immunization card In grownup skin care laser clinic generic oratane 30mg visa, yearly influenza vaccination must be done in affected person with cardiovascular acne needle order 5 mg oratane otc, pulmonary skin care tips order oratane 20 mg fast delivery, renal, hematological problems. Patient with persistent renal illness and older (65 years), should obtain pneumococal vaccine once solely Patient with alcoholism, myeloma, lymphoma, cirrhosis, func tional asplenia ought to receive pneumococcal vaccine Only in case of useful asplenia or anatomical asplenia pneumococcal vaccine should be taken in every 6 years. Hepatitis B vaccination ought to be given to: z Intravenous drug customers z Dialysis workers z Staff of endoscopy unit z Sexual partner of hepatitis B virus service z Multiple sexual partners z Hemophiliac sufferers Haemophilus influenzae kind B vaccine to be given to children. To Patient thinks whether the interviewer may be trusted to offer the small print of himself. In this case, the interviewer has to gain confidence of the affected person, in order that patient will give correct informative historical past. Sometimes, the interviewer ought to be silent for someday when the affected person begins emotional reactions like, crying, annoying throughout answering the questions. This allows the patient to release the tension and offers correct history when questioning will be started. History Taking from the Confused Patient Sometimes the patient could confuse the interviewer in the following processes: z When the patient provides affirmative answer to all of the direct questions from the interviewer, he has to say the that means of the questions, in order that the affected person will answer to the point. In case of mentally unwell patient (depression, anxiety, neurosis, manic depressive psychosis): the history could also be inconsistent and will give different sorts of historical past of illness having no sequential chronological order. Again he has told that he has retrosternal chest pain exacerbated Art of Interviewing to a Patient 17 z by intake of food. So the interviewer has to know that which pain is earlier If possible, the interviewer has to name the patient next day to listen the extra factors relating to the history. Allowing the affected person to cry, the interviewer has to wait, and to offer a tissue paper to rub his or her eyes After recovering from the crying episode, most patient starts telling story Only the interviewer has to spice up at regular intervals during dialog. In this case, the interviewer (clinician) has to call security guard to regulate the scenario by taking the patient in the different room and makes her or him to understand the cause. When the rapport will be established between the affected person and the interviewer, the patient will be calm and quiet and begins giving historical past. Quartan fever: Paroxysms of fever are separated by two intervening normal day Example: Plasmodium malariae. Quotidian fever: In this type, fever paroxysms occur every with every day contact of baseline. Double tertian malaria-where two distinct groups of Plasmodium vivax alternatively sporulating every forty eight hours ii. Two distinct teams of Plasmodium falciparum mature in different days, thus ensuing fever twice a day. Double quartan fever: this type of fever paroxysms occur with two unbiased teams of Plasmodium malariae, so febrile paroxysms occur on two successive days followed by a febrile day. It is found in active acute tuberculosis, bacterial meningitis, abscess, encephalitis. Relapsing fever: It is characterised by febrile attacks, every lasting for several days separated by afebrile intervals of some duration. Pel-Ebstein fever: In this case episodes of fever final for a number of hours to several days followed by afebrile period of days or weeks. The affected person often dips the thermometer in heat water, or place it involved with heat supply, heated the bulb by friction, bed clothes or with mucous membrane of the mouth. Infections: 34 Clinical Methods and Interpretation in Medicine Monoleptic fever: A continued fever with only one paroxysm Polyleptic fever: A fever with two or more paroxysms, typical of malaria Miliary fever: A fever characterised by profuse sweating and productions of minute vesicles containing fluid in sweat follicles, typical of past epidemics Fatigue fever: Elevation of physique temperature following excessive and continued muscle exhaustion Neuroleptic malignant syndrome: 1 to 2 days after intake of neuroleptic medicine (antipsychotic drugs) the affected person develops hyperthermia (temperature > 106�F), lead-pipe rigidity, altered mental standing, tachycardia, tachypnea, progressive metabolic acidosis, myoglobinuria and renal failure. This state of affairs can be falsely identified as worsening of psychotic symptoms leading to increase of neuroleptic medicine Extreme pyrexia: Temperature >106�F. The causes are: Cerebrovascular accident Major cardiac occasions following cardiac arrest Malignant hyperthermia Neuroleptic malignant syndrome. Malignant hyperthermia: this inherited dysfunction of muscle sarcoplasmic reticulum cause speedy increase in intracellular calcium. Following publicity to inhaled succinylcholine anesthetics patient precipitates sustained muscle contraction. As a end result the patient develops rigidity, hyperthermia, rhabdomyolsis, metabolic acidosis and hemodynamic instability. The affected person is usually younger; he develops palpitation, faintness, headache, nausea, vomiting and cramps, low blood pressure, diaphoresis, ashen, cool moist pores and skin and dilated pupils. Core body temperature is elevated however less than 104�F Heat stroke: There is failure of thermoregulatory system to produce sweating, consequently the core body temperature rises quickly. The provocating elements are: Cardiovascular disease Anticholenergic drugs Diuretics. The causes are: Infectious illnesses: Salmonellosis, brucellosis, legionellosis, Mycoplasma pneumoniae, meningitis with elevated intracranial strain Iatrogenic: Digitalis, beta-blockers. Effects Failure of cellular metabolism Impairs brain perform significantly judgment. At this low level of temperature body is unable to generate warmth, thus the core temperature continues to fall. Temperature of this levels are missed by routine thermometers, thus require thermistors. Causes of Hypothermia yp � Endocrine � Idiopathic � Infectious cases � Mechanical/traumatic publicity and immersion � Hypothalamic harm � Burn � Metabolic/toxic � Neoplastic � Neurologic � Psychosocial � Vascular Hypothyroidism hypoglycemia Advanced age Sepsis Trauma, hemorrhage Drug overdoses, antipyretics Brain tumors Stroke Homelessness, poverty Strokes Physical Examinations 37 Signs and Symptoms of Hypothermia Mild � Confusion � � � � � � � Tachypnea Tachycardia Vasoconstriction Lethargy Shivering Ataxia Dysarthria Moderate Consciousness diminished Dilirium Bradycardia Shivering�stopped Cold diuresis Tachypnea Severe Unresponsive Loss of reflexes Appeared�dead Hypotension Very chilly skin Pulmonary edema Respiratory failure Ventricular fibrillation � Fine motor incoordination Anthropometry Height Human being grows by linear progress in: Infancy Childhood Adolescence, and ends with closure of the epiphyses of the lengthy bones of the extremities. Linear growth requires the presence of: Growth hormone Nutrition (protein, calories, calcium, vitamin D, phosphorus). Mature peak is determined by: Genetic factors Environmental components, mainly nutrition. It should be plotted in the form graph, from which one can decide the nature of growth at a degree of time. After stability of growth shall be reached, peak ought to be measured annually till the age of 60 years. Significant deviation of this development fee results from elevated growth hormone manufacturing consequently from pituitary adenoma. Excessive height: Gigantism: this development happens on account of excess linear progress on the open epiphyses (linear development excess of the predicted by parental height) because of extra production of progress hormone from pituitary tumor Acromegaly: When the epiphyses closes, the growth occur in arms, cranium, mandible and soft tissue thickening without growing the height. Loss of Height Decreased height after skeletal maturity might happen from: Loss of lengthy bone development Loss of cartilage in lower extremity joints (hips and knees) Loss of vertebral height Loss of intervertebral spaces Excessive spinal curvatures. Weight could additionally be acute often due to acute lack of physique tissue, rapid diuresis or acute dehydration. Percent of weight reduction = [(usual weight � present weight)/(usual weight)] � 100 Significant involuntary weight loss can be defined as greater than 5 percent of physique weight a thousand previous 6 months or more than 10 % of body weight in final 1 year. Weight loss could additionally be as a outcome of: Decreased consumption Maldigestion Malabsorption Increased metabolic utilization Increased loss of energy. Lower extremity venus stasis Idiopathic intracranial hypertension Gastroesophageal reflux Urinary stress incontinence Gallbladder disease. Weight (Ibs) Height (inches) 2 Physical Examinations 45 Distribution of fats in the body Fat disposition could additionally be. Subcutaneous fats has descending distribution-mostly concentrated within the upper half of the physique (neck, cheek, shoulder, chest, and higher abdomen). Peripheral distribution: Bitrochanteric diameter is greater than bihumeral diameter. Subcutaneous fats has ascending distribution, mostly concentrated in the lower half of the body (lower stomach, pelvic girdle, buttock and thigh).
References - Ruoslahti E: Structure and biology of proteoglycans, Annu Rev Cell Biol 4:229n255, 1988.
- Davis TM, Wright AD, Mehta ZM, et al. Islet autoantibodies in clinically diagnosed type 2 diabetes; prevalence, and relationship with metabolic control (UKPDS 70). Diabetologia. 2005;48:695-702.
- Liu L, Suzuki K, Nakagata N, et al: Retinoic acid signaling regulates sonic hedgehog and bone morphogenetic protein signalings during genital tubercle development, Birth Defects Res B Dev Reprod Toxicol 95(1):79n88, 2011.
- Aschoff, A.J., Sulman, A., Martinez, M. et al. Perfusionmodulated MR imaging-guided radiofrequency ablation of the kidney in a porcine model. AJR Am J Roentgenol 2001;177:151-158.
- Douketis JD, Johnson JA, Turpie AG. Lowmolecular- weight heparin as bridging anticoagulation during interruption of warfarin: assessment of a standardized periprocedural anticoagulation regimen. Arch Intern Med 2004;164(12):1319-26.
- Bachmann A, Tubaro A, Barber N, et al: 180-W XPS GreenLight laser vaporisation versus transurethral resection of the prostate for the treatment of benign prostatic obstruction: 6-month safety and efficacy results of a European multicentre randomised trial?the GOLIATH study, Eur Urol 65:931-942, 2014.
|