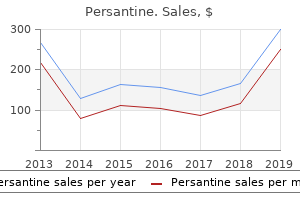
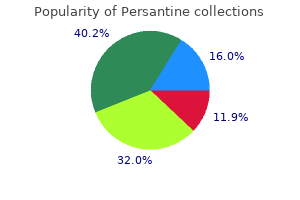
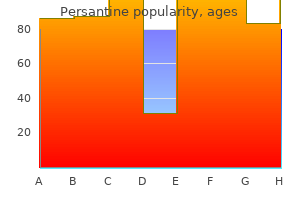
Persantine
Edward Buckley, M.D. - Department of Neurology
- Duke University Medical Center
- Durham, NC
Buy generic persantine 100mg on-lineGleason Score New Gleason Grade 5year biochemical relapsefree survival lenging and sometimes the usage of immuno histochemical stains might be required [112] medicine man gallery 100 mg persantine. Gleason sum scores of three + three medicine 377 cheap 100mg persantine, three + four medications like xanax buy persantine 25 mg on line, 4 + 3 medications 44334 white oblong order 25mg persantine overnight delivery, eight, and 9/10 instantly translate to Grades 1, 2, 3, four, and 5, respectively. These grade teams correspond to a fiveyear biochemical threat free survival based on radical prostatectomy grade of 96% (grade 1), 88% (grade 2), 63% (grade 3), 48% (grade 4), and 26% (grade 5) (Table 28. For occasion, grade 1 is the lowest grade and >95% of sufferers may have no detectable recurrence as much as five years after radical prostatectomy. Antibodies that demonstrate a complete absence of basal cells might help diagnose invasion. Important elements for this important divergence are: (i) the number of cores taken because more cores lead to a higher concordance, (ii) the size of tumour as a result of a larger tumour reduces concordance as the small core will not be representative of the whole tumour, (iii) using a tertiary grade in prostatectomy specimens, and (iv) interobserver variability [109, 110]. Further histological or molecular markers are needed to better riskstratify patients in choosing acceptable remedy [119�121]. In the submit radiotherapy setting, some cancer recurrence exhibits profound therapy effect that precludes grading. Occasionally, each forms of cancer (with and with out treatment effect) might be seen in the identical biopsy. It additionally appears predictive for biochemical relapse following radical prostatectomy and radiotherapy [123�127]. Gene promoter hypermethylation is a molecular mechanism of gene silencing, commonly observed in lots of cancers. Popularised in the last decade, it includes an lively decision to not deal with the patient instantly; as a substitute the patient is saved beneath shut followup. Cancers are normally handled on the first signs of subclinical development (Table 28. Importantly, treatment at progression seems to be as efficient as if it had been delivered on the time of prognosis for many males. Several affected person and tumour characteristics had been discovered to be predictive of later biopsy progression and deferred remedy. However, the procedure remained unpopular because of frequent complications of incontinence and impotence. But in subgroup evaluation of intermediate (significant) and excessive danger (nonsignificant), there was a discount in allcause mortality. A lengthy decrease midline incision is made and a node dissection is now carried out for patients with intermediate and highrisk disease. Deflating the balloon of the catheter, and utilizing the catheter as a sling, the prostate is lifted up and the bladder is dissected away from the prostate. The return of continence after surgical procedure could additionally be gradual, with many men regaining continence by two to three months, however recovery continues as a lot as one year. Most academic collection report longterm continence rates of 80�95% by one yr; nevertheless, continence rates from populationbased studies are often much less. Pelvic ground workouts pre and postoperatively may help regain continence; nevertheless, if lasting more than one year, the insertion of a synthetic urinary sphincter might be required. Like continence, reported charges of potency preservation range widely, starting from forty to 82% in men younger than 60 years when each nerves are preserved and drops to 20�60% when just one nerve is preserved. Recovery of sexual operate typically happens steadily within 6�24 months following surgical procedure. Bladder neck stenosis, seen when the circulate turns into weaker or poor flow with worsening storage signs. Some templates embrace clearing the common iliac nodes to the ureteric crossing, suggesting 75% of all anatomical touchdown sites are cleared with this approach [152]. Intraoperative problems embody blood loss requiring blood transfusion, rectal harm, and ureteral injury. Laparoscopic approaches decrease bleeding charges, however carry the additional dangers of laparoscopic access and insufflation, as well as patient positioning. Perioperative issues include anastomotic leak, deep vein thrombosis, pulmonary embolus, and wound infection. Late complications include urinary incontinence, impotence or erectile dysfunction, and bladder neck stenosis. Urinary incontinence, normally stress incontinence as a end result of harm to the exterior urethral sphincter. Complications embrace lymphocele, lymphedema (scrotal and or lower limb), deep vein thrombosis, and pulmonary embolism. With no highquality head tohead comparative trials, radiotherapy is a vital various to surgery for healing remedy. Unsurprisingly up to 41% of sufferers may have insufficient coverage of the goal volume. The use of dose escalation, complete pelvic radiation (including regional lymph nodes) and androgen deprivation. Shortterm (three to six months) neoadjuvant (three months prior) and concurrent (three month after) androgen deprivation is beneficial for those with intermediaterisk disease, whereas those with highrisk disease ought to obtain neoadjuvant (three months prior), concurrent, and long run adjuvant (24 months after) androgen deprivation [157�159]. The impression on sexual function will not be apparent for upto two years and are sometimes exacerbated with the concurrent use of androgen deprivation [160]. Longterm dangers embrace urethral stricture, recto-urinary fistula, and radiation cystitis, which although uncommon may be severely debilitating for the patient and provide advanced administration challenges for the physician. This method delivers extremely conformal radiotherapy over shorter interval, which can now be achieved safely with using better ontreatment imaging and imageguided radiotherapy [41, 162, 163]. Radioactive implants are either permanently placed in the prostate (I125 halflife 60 days, or Pd103 halflife 17 days [164]) or radiation may be delivered via hollowcore catheters (Ir192) hooked up to momentary implants during hospitalisation. Androgen deprivation can be used to shrink the prostate previous to brachytherapy to facilitate seed placement, with the caveat of extra unwanted effects (Table 28. Lifestyle modifications exercise, give up smoking, reduce alcohol consumption, weight reduction. Annual lipid profile, lifestyle modifications give up smoking, weight loss, exercise program. Hypoglycaemics metformin, antihypertensives, statins, aspirin, toremifene (improves lipid profile). The optimal treatment method, due to this fact, usually necessitates multiple modalities to achieve native control in addition to controlling the highly probably microscopic illness. If lymph node dissection yielded nodal involvement, choices are both early or delayed hormonal therapy. Alternatively, brachytherapy may be offered; however, repeat biopsies shall be required to reveal viable most cancers cells. Combined therapy on the time of radical therapy (usually within six months) is considered an adjuvant remedy modality. The next most common websites were lung (46%) adopted by liver (25%), pleura (21%), and adrenal glands (13%). Interestingly, an inverse relationship was seen between lung and bone metastasis, suggesting unbiased mechanisms of metastatic spread. These signs could manifest, depending on the tumour burden of the individual patient.
Persantine: 100 mg, 25 mg
Order 100 mg persantine visaIf a urethral stricture is suspected symptoms after flu shot persantine 25 mg cheap, confirmation of the analysis is achieved either by direct visualisation (cystoscopy) or imaging (cystourethrogram) symptoms of colon cancer discount persantine 100mg with mastercard. Images are taken in an indirect view to visualise the complete length of the urethra 4 medications at target generic persantine 25mg without a prescription. A urethrogram is carried out with the affected person lying in a 30� oblique position with the bottom leg flexed symptoms hepatitis c order persantine 25mg visa. A 12Fr catheter is placed into the fossa navicularis and the balloon inflated with 2 ml of water. Once the bladder is sufficiently distended with distinction, a voiding cystourethrogram could be performed. This investigation gives information on the positioning and size of stricture in addition to the presence of a urethral diverticulum or fistula. In some cases, cystoscopy can be utilized to dilate a soft stricture underneath vision utilizing the scope simultaneously investigating. However, tight or lengthy strictures will at all times require a urethrogram to achieve details about the urethra upstream of the stricture before planning treatment. If the presentation is retention of urine with failure of urethral catheterisation, a suprapubic catheter ought to be positioned, followed by mixed antegrade and retrograde urethrogram to assess the stricture. Dilation is completed to stretch the stricture without causing damage to result in additional scarring. This is obvious when important bleeding occurs which signifies tearing of the stricture. The term bougie is derived from the word Bujiyah � an Algerian port recognized for the best wax candles and thin wax tapers had been found to make glorious dilators. Using this system, a number of filiforms might be passed until the true lumen was identified. Nearly 50% of all strictures recur, however a quantity of, complicated, or lengthy strictures (>2 cm) are much more likely to recur. These are a series of curved steel instruments, sequentially growing in diameter. It is usually safer to start with a mediumsized dilator to scale back the danger of this complication. These dilators are additionally helpful in serving to to determine the location of a stricture when performing an open reconstruction. These are inserted over a guidewire, which has been handed into the bladder cystoscopically. This all but negates the chance of causing a false passage and appears to be much less traumatic. Because this is managed, the stricture is split rather than torn or shorn, and therapeutic is by reepithelializing of the reduce surface. After each dilation and urethrotomy, a catheter is often placed for at least 24 hours to reduce infective complications related to extravasation of urine [54]. Once the stricture has been divided or dilated, the affected person would possibly require common intermittent selfdilation. Following the procedure, cure may be anticipated in approximately 40�70% of patients [55]. Many would argue that once a stricture has recurred, the following step in management should be urethroplasty [57]. The most commonly used graft is buccal mucosa, which can be utilized for both augmentation and substitution. Buccal mucosa has a pandermal plexus allowing it to be harvested and thinned with out interrupting the vasculature [58]. Fullthickness grafts (including the inside prepuce) include a separate intradermal and subdermal plexus joined by speaking vessels. They should be treated with extra care and kept free from haemolytic streptococcal infection, thus making them more fastidious than buccal mucosal grafts [59]. This entails the mobilisation of a patch of skin whereas preserving its blood supply intact. The preliminary layers of dissection include pores and skin, Campers fascia (fatty tissue), and Colles fascia which is a continuation of Scarpa facia in the abdominal wall. Next the bulbospongiosus muscle with its masking of deep perineal fascia (Gallaudet fascia) shall be dissected. The urethra can then be mobilised from the corporal bodies as essential and the sound or catheter used to information the location of urethral incision. The approach used is decided by the length of stricture and individual surgeon choice or experience. Longterm success charges for this procedure are high starting from 91 to 99% [60�62]. The perfect stricture length for this procedure is generally accepted to be less than 2 cm [61]; however, some suggest a stricture size of no more than 1 cm because of the danger of chordee [63]. One common criticism of the anastomotic urethroplasty is the interruption of blood flow throughout the corpus spongiosum attributable to full transection. The success charges are related for both, 88�89% and 88�89% for dorsal and ventral grafting techniques, respectively [68, 69]. To perform a dorsal patch urethroplasty without mobilisation of the urethra, the transventral dorsal inlay urethroplasty technique was developed in 2001. Palminteri took this one step further and carried out a combination of dorsal and ventral grafting without mobilisation of the urethra, with a median success price of 91% [68, 71]. Another approach to restrict the amount of mobilisation for the urethra is the lateral onlay urethroplasty first described by Barbagli in 2005 [72]. Only one side of the urethra must be mobilised; subsequently, blood supply to the corpus spongiosum is maintained on the contralateral aspect. This additionally avoids a ventral urethrotomy in the thickest a part of the spongiosum, theoretically leading to less intraoperative blood loss. Barbagli described this process in six patients with a success rate of 83% at seventy seven months observe up [71]. Techniques for treatment of penile urethral strictures range by the kind of tissue used: pedicled flap, buccal mucosa, or fullthickness pores and skin and by whether a single stage or twostaged method is used. This strategy also allows for the option of an augmentation urethroplasty with a buccal mucosal graft if required. In this process, a longitudinal stricturotomy is made, and an ellipse of graft is patched to the incised urethra, thus widening the lumen. Debate remains as to whether dorsal or ventral stricturotomy and patch is preferable. Conversely, a ventral incision permits for less mobilisation of the urethra and the corpus spongiosum may be closed over the graft to give support and a wealthy vascular mattress.
Order 100mg persantineThis can provide useful information on a suspected damage and can determine the practical status of the contralateral kidney [15] treatment 3 phases malnourished children buy discount persantine 100mg on line. In such cases treatment resistant depression order persantine 100 mg with mastercard, renal angiogram could show damage to the renal artery or its segmental branches symptoms 5-6 weeks pregnant generic 25 mg persantine otc. The conservative administration has a low failure fee (1%) and may save kidneys that may in any other case be misplaced throughout tried restore [3] symptoms 9f diabetes discount 25 mg persantine fast delivery. However, through the conservative administration, shut monitoring is vital to recognise want for added intervention or surgical procedure. Some patients with penetrating renal trauma can be managed conservatively as well. For instance, nearly 90% of patients with stab wounds posterior to the anterior axillary line can be managed 196 11 Kidney and Ureter Trauma Table eleven. However, intervention is predicted by the need for continued fluid and blood resuscitation, perirenal haematoma size >3. But in instances of persistent extravasation or urinoma, administration is normally profitable with ureteral stenting or nephrostomy tube placement. Most injuries will heal with conservative strategy, however there can be an elevated fee of complications [26, 27]. Absolute indications for renal exploration are: Lifethreatening renal haemorrhage with hemodynamic instability, regardless of the mode of injury [28] An expanding or pulsatile perirenal hematoma recognized intraoperatively [28, 29]. Inconclusive imaging and a preexisting abnormality or an by the way diagnosed tumour might require surgery even after minor renal damage [30]. The management of renal harm may be influenced by the choice to discover or observe related belly injuries [31. For isolated renal trauma, surgery must be performed utilizing a transperitoneal approach with early vascular management previous to opening the Gerota fascia [32, 33]. General ideas of renorrhaphy embrace: Examination of the lacerations, together with repairing of the injured vessels and conserving as much of the parenchyma as potential. If a polar harm happens or if nonviable tissue is present, a partial nephrectomy could also be essential. The use of haemostatic brokers and sealants in reconstruction are helpful for efficient haemostasis [34]. The overall fee of sufferers who undergo a nephrectomy during exploration is round 13%, usually in patients with penetrating injuries and higher rates of transfusion necessities, haemodynamic instability, and higher harm severity scores [35]. Mortality price is larger in patients requiring nephrectomy, but reason for deaths are normally the related accidents quite than the renal trauma alone [38]. Grade V vascular accidents are typically treated with nephrectomy as a result of repair is normally not profitable [39]. Similarly, in gunshot injuries brought on by a highvelocity bullet, reconstruction could be troublesome, and nephrectomy is often required [41]. However, preliminary or repeated embolisation for the higher grade accidents can forestall a nephrectomy in more than 75% of sufferers. Radiological embolisation is indicated in sufferers with lively bleeding from renal harm but with out another indication for immediate surgical exploration. In the absence of an expanding haematoma with haemodynamic instability, associated multiorgan eleven. Each harm ought to be managed on its advantage regardless of conservative or surgical method. Renal exploration might be required if bleeding continues or affected person turns into unstable. Delayed bleeding can happen within several weeks of the damage and is normally managed with selective angiographic embolisation [46]. Percutaneous embolisation is commonly profitable in these instances, however surgical procedure may be required to restore large fistulas. Persistent giant quantity extravasation usually responds well to stent placement or nephrostomy drainage [27]. Renal restore could be required if persistent urine leakage regardless of conservative measures. A assortment of extravasated urine turns into walledoff by fibrous tissue however stays in communication with the renal pelvis [47]. The wall of the cavity turns into ultimately kind of lined with urothelium, and in flip, this results in calcification and heterotopic bone formation. Perinephric abscess formation may be managed with percutaneous drainage or open drainage. Early problems (within 30 days of the injury): 1) There is a small but actual danger of delayed haemorrhage. The lowered blood supply causes renal ischaemia, resulting in extra renin excretion in an effort to enhance the blood strain to increase renal blood supply. Risk elements for iatrogenic ureteric trauma embody superior malignancy, prior stomach or pelvic surgical procedure or irradiation, inflammatory processes. A list of frequent procedures with associated risks of ureteric damage is listed in Table eleven. Penetrating ureteral trauma is the most prevalent Procedure Gynaecological Vaginal hysterectomy Abdominal hysterectomy Laparoscopic hysterectomy Urogynaecological (antiincontinence/ prolapse) Colorectal Ureteroscopy Mucosal abrasion Ureteral perforation Intussusception or avulsion 0. Nonspecific features embrace belly or flank pain, infection/sepsis, haematuria, ileus, vomiting, and indicators of urinary obstruction (hydronephrosis and decreased renal function). However, postoperative or traumarelated suspicion: a renal ultrasound can show variable levels of hydronephrosis or a urinoma. Careful assessment must be made for a vesicovaginal fistula as a result of these might nicely coexist with the ureteral injury [56]. Partial ureteric accidents can be repaired instantly with a stent or urine diversion by a nephrostomy tube. Stenting is helpful because it provides canalization and may decrease the danger of ureteric stricture [52]. However, if the ureter is accidently ligated with suture or transected, an open repair is required. Later recognition Injuries which are diagnosed late are normally handled first by a nephrostomy tube with or without a stent [52]. These patients can current with peritonitis and anuria, urinoma, sepsis, wound or vaginal leakage, and flank ache. This includes resuscitation, therapy of sepsis, and a percutaneous nephrostomy inserted to divert urine and relieve the obstruction. After the acute section, a cystoscopy, examination under anaesthesia, and retrograde pyelogram research are required earlier than definitive administration. The endourological remedy of small ureteral fistulae and strictures is safe and effective in chosen instances [58], but an open surgical restore is commonly needed. For uretero and vesicovaginal fistulas repair with interposition of intact layer of wholesome tissue is important. Debridement of necrotic tissue Spatulation of ureteral ends Mucosatomucosa anastomosis Tensionfree anastomosis Absorbable sutures Ureteral stenting External drain Isolation of damage with peritoneum or omentum this is the preferred and most reliable method of repairing an injured ureter [56, 59]. A long submucosal tunnel is made within the Boari flap, and the ureter is drawn down this into the bladder. The flap is closed in the line of the opening in the bladder utilizing two layers of fine absorbable suture.
Buy discount persantine 100mg on lineAge (years) Spontaneous acute retention Precipitated acute retention a) 45�54 55�64 65�74 75�84 >85 Any age b) 45�54 55�64 65�74 75�84 >85 Any age 1 symptoms in early pregnancy buy persantine 25 mg lowest price. While histological prevalence was extra dramatic: <30 years (0%) medications post mi persantine 100 mg fast delivery, 41�50 years (23%) medications pictures purchase 25 mg persantine fast delivery, 51�60 years (42%) treatment definition statistics discount 25mg persantine overnight delivery, 61�70 years (71%), 71�80 years (82%), and > eighty years (>88%) [28]. Studies of total prostate volume of men of their 30s revealed that total prostate volume averaged 25 cm3, and this increased to 45 cm3 for men of their 70s. Elicitation of red flag symptoms similar to haematuria, incontinence, and dysuria may necessitate pressing investigations. Prostate size is estimated by feeling from side to side of 540 27 Prostate Benign Prostatic Hyperplasia the prostate the variety of index finger widths, where one fingerbreadth is alleged to represent roughly 15 g. Need to balance dangers and benefits of having clinically vital disease identified. A urinalysis ought to be performed to detect blood, glucose, leucocytes, and nitrites. Haematuria on urinalysis ought to be investigated with a versatile cystoscopy and upper tract imaging. Measurements can also elucidate the presence of polyuria and nocturnal polyuria (which may be the trigger of symptoms). Treatment modalities available: 1) Watchful waiting and conservative remedy 2) Medical administration: 3) Monotherapy a) Combination therapy 4) Surgical administration 27. Roughly talking, greater than onethird of sufferers symptoms are likely to enhance, more than onethird stay the identical, and a less than onethird worsen [58]. Conservative interventions [59] embrace: score discount or peak flow fee enchancment between S. Blocking these receptors mediates leisure of the tissues, thereby easing the flow of urine by way of the decrease urinary tract [63]. Some of the blockers have also been shown to trigger apoptosis of the prostatic epithelium, which can also contribute to their effect [64]. The 1 receptors are situated mainly within the urinary tract specifically the 1 subtype; nonetheless, the 2 receptors are also positioned elsewhere within the physique together with blood vessels which accounts for some of the undesirable sideeffects of blockers, especially the less selective ones similar to phenoxybenzamine [65, 66]. The different types depend upon their uroselectivity; uroselevtive 1ablockers include Tamsulosin and alfuzosin and nonselective 1blockers are doxazosin and terazosin [67]. The primary side effects of blockers are mild, occur in about 15% of patients, and embrace (more frequent with nonneuroselective blockers): orthostatic hypotension, headache, dizziness, asthenia, drowsiness, and ejaculatory issues. Tamsulosin has a decrease fee of orthostatic hypotension however a better probability of ejaculatory problems. Intraoperative floppy iris syndrome during cataract surgical procedure is a crucial aspect effect to bear in mind when commencing patients on blockers especially tamsulosin which could be seen in as much as 86% of patients and about 15% with alfuzosin [68, 69]. However, in skilled palms, intraoperative floppy iris syndrome can be anticipated and compensatory strategies employed (such as topical atropine preoperatively, iris retractors, pupil expansion ring, or use of viscoadaptive ophthalmic viscosurgical system with reduced fluidic parameters) to stop problems leaving excellent visible outcomes [67]. Lifestyle modifications embody: Reduction of fluid intake within the night Avoidance of irritant substances. Education about the illness, pure historical past of it, potential issues and reassurance are additionally important. However, an up to date metaanalysis with longterm outcome information just lately demonstrated that there was no distinction in symptom 27. Patients should be initially be reviewed after 4�6 weeks of remedy and then every 6�12 months [4]. Similarly, there was a 55% relativerisk discount for want for surgical intervention as in comparison with the placebo groups. Adverse occasions are often nicely tolerated and include erectile dysfunction, altered libido, ejaculatory issues (lowvolume ejaculate), and infrequently, gynecomastia and breast tenderness. Combination remedy was significantly higher in decreasing the danger of illness development. Combination therapy also supplies larger symptom enchancment profit than both monotherapy regimens alone. Combination remedy has related adverse event profiles to different remedy modalities [44]. Then it must be determined whether or not hospital admission is required or if an ambulatory care programme is appropriate for the patient. Indications for hospital admission embrace: urosepsis, gross haematuria, residual volume > 1 l, postcatheterisation diuresis, unusual symptomatology, and those unable to cope with a urethral catheter or ambulatory care programme [82, 87]. Since then, five randomised managed trials and a Cochrane evaluate have been performed. Presentation of males with persistent urinary retention is varied and can be asymptomatic or lowvolume micturition, increased frequency or hesitancy, nocturnal enuresis, a palpable however painless bladder, or indicators of chronic renal impairment [95, 97]. Initial evaluation of these males should contain a urinalysis for indicators of infection, a renal panel blood check. It is crucial to get patients to full a threeday voiding diary which incorporates the volumes of voided urine; this allows the calculation of ratio of daytime to nighttime urine quantity voided. The causes of nocturnal polyuria embrace congestive coronary heart failure, obstructive sleep apnoea, nephrotic syndrome, autonomic neuropathy, chronic kidney illness, venous insufficiency, neurologic diseases like Parkinson and Alzheimer illnesses, and idiopathic [98]. Oedemaforming states result in nocturnal polyuria because of the mobilisation of the oedema during recumbency which the kidneys course of and produce urine at night time. In persistent kidney disease, the kidneys are maximally concentrating the urine and this results in an increased urine manufacturing at night time. The mainstay of analysis is with a threeday voiding diary with volumes voided to be included. This is followed by an intensive history and examination targeted to the causes listed beforehand. Conservative measures such as fluid restriction six hours earlier than bedtime has restricted affect. Loop diuretics taken 6�10 hours before bedtime have additionally been shown to have some restricted impression. Important potential side effects embrace hyponatraemia (14%), headache, nausea, dizziness, and peripheral oedema. This treatment is at present not licenced for the remedy of nocturnal polyuria. Just the place to cut through the bladder neck is a matter of surgical desire and coaching. Wherever the bladder neck is incised, the patient have to be warned of retrograde ejaculation. The purpose of the operation is to remove enough of the obstructing tissue from the cranial internal zone of the prostate to enable the bladder to empty freely. There are several completely different styles of transurethral resection, nonetheless, the most commonly used is the technique described first described by Blandy. Great care is taken to preserve the verumontanum as a result of the intramural sphincter lies so close to it. The neurovascular bundles to the penis are additionally very close to the membranous urethra and diathermy have to be used sparingly of their neighborhood.
Diseases - Myoneurogastrointestinal encephalopathy syndrome
- Brachydactyly type C
- 22q11.2 deletion syndrome, rare (NIH)
- Furunculous myiasis
- Cardiofaciocutaneous syndrome
- Retinal telangiectasia hypogammaglobulinemia
- Connexin 26 anomaly
- Neuroacanthocytosis
- Blepharospasm
- Ectodermal dysplasia hypohidrotic hypothyroidism ciliary dyskinesia
Cheap 100 mg persantine free shippingWhere there has been previous hypospadias repair treatment receding gums 100 mg persantine with mastercard, the corpus spongiosum medicine research order persantine 25mg line, dartos fascia symptoms ms women cheap persantine 25mg visa, and ventral shaft pores and skin are sometimes deficient medicine 75 purchase 25 mg persantine visa, and in this scenario, a free graft substitution could be extra appropriate. Once the flap of skin has been mobilised, the strictured phase of uretha is laid open and the skin graft anastomosed to the reduce edges. Longterm overall stricture free rates of a McAninch single stage penile pores and skin flap for anterior urethral stricture are 95, 89, eighty four, and 79% at 1, three, 5, and 10 years, respectively [74]. The urethra is laid open by a ventral incision from the meatus until wholesome urethra is encountered. Clearly a singlestage approach is helpful to the affected person the place possible as a outcome of it avoids long periods of discomfort and incapacity. It can additionally be extra widespread in males than girls due to lack of urethral attachments to the pubis in girls [77]. If the dorsal vein ruptures, the ensuing haematoma additionally contributes to the distraction defect. Where none of those signs are current, an attempt at urethral catheterisation can be the mechanism of injury is stretching of the urethra attributable to cephalad motion of the bladder, prostate, and membranous urethra through the trauma. In the acute setting, an ultrasound guided suprapubic catheter could must be placed and urethrogram deferred. If the patient is being taken to theatre for administration of other accidents, an ontable urethrogram may be carried out if the affected person is secure. While beneath anaesthetic, an attempt at major endoscopic realignment and urethral catheter insertion may be made with little threat of morbidity. Ultimately, a suprapubic catheter can at all times be sited if urethral catheterisation fails. The solely indications for immediate exploration are the discovering of concomitant injury to the bladder neck, vagina, or rectum and for removal of a bony fragment. When open exploration is carried out in these cases, an attempt at urethral realignment can be made. Overall, major realignment reduces stricture formation in roughly a 3rd of circumstances [79]. Early open exploration does, nonetheless, result in larger charges of incontinence and erectile dysfunction [80]. The vast majority of sufferers might be managed with suprapubic catheterisation alone and urethroplasty carried out after approximately three months once fractures have healed and haematoma resolved. Often the defect is quite wide, and in depth mobilisation of the urethra is required. In these cases, adjunctive manoeuvres such as splitting of the crura or infrapubectomy can be used to reduce the gap between the 2 ends. A extensive oval opening is made into the urethra by way of the scar tissue, and the spatulated bulbar urethra is then anastomosed to it. An ellipse is cut out from the anterior lower a part of the symphysis, and an endtoend anastomosis made after spatulating the urethra. An different approach removes the complete symphysis and enwraps the anastomosis in omentum to forestall scar formation. Extravasation of contrast at damage website without distinction visualised in proximal urethra or bladder. Suprapubic cystostomy and delayed restore or primary endoscopic realignment in selected sufferers delayed repair V Complete or partial disruption of posterior urethra with associated tear of the bladder neck, rectum, or vagina Primary open repair Extravasation of distinction at urethral damage site presence of blood within the vaginal introitus in women. The aetiology is primarily neurogenic but could also be vasculogenic, related to pudendal artery injury. There is currently controversy as to whether revascularisation before urethral reconstruction is of profit. It could reduce the incidence of ischaemic restenosis and reduce longterm erectile dysfunction [83, 84]. After delayed urethroplasty, the overall restricture rate is lower than 10% and the impotence fee approximately 5% [81]. Lesions additionally overlap of their look such that a biopsy, swabs, and scrapings are often required to establish a diagnosis. Development of a multidisciplinary genital dermatology service would be higher for crossspecialism opinion and more exact prognosis. Management of urethral strictures has moved back and forth between enthusiasm for endoscopic management and urethral reconstruction. With improvements in endoscopic tools in the Eighties and selfdilating catheters becoming extra freely out there, endoscopic management was the firstline treatment in most urology departments. This led to a restricted exposure in coaching to be taught urethroplasty, and it remained a minority choice until quite recently. With the popularisation of buccal mucosal grafts and the improved outcomes and suppleness of use that they provided, urethral reconstruction has begun to reestablish its place in repairing urethral strictures. There are now many more skilled surgeons and surgical departments providing urethroplasty and reducing what is normally a lifelong stricture problem and dependency on urethral dilation. Comparison of the efficacy and safety of oral fluconazole and topical clotrimazole in sufferers with candida balanitis. Treatment of major firstepisode genital herpes simplex virus infections with acyclovir: results of topical, intravenous and oral therapy. The Oslo research of untreated syphilis; an epidemiologic investigation of the pure course of the syphilitic an infection based upon a restudy of the BoeckBruusgaard material. United Kingdom National Guideline on the Management of Trichomonas vaginalis 2014. Balanitis xerotica obliterans: epidemiologic distribution in an References 683 20 21 22 23 24 25 26 27 28 29 30 31 32 33 equal entry well being care system. Clinical parameters in male genital lichen sclerosus: a case sequence of 329 sufferers. Plasma cell balanitis: scientific and histopathological options � response to circumcision. Causes, presentation and survival of fiftyseven sufferers with necrotizing fasciitis of the male genitalia. Simple urethral dilatation, endoscopic urethrotomy, and urethroplasty for urethral stricture disease in adult males. Internal urethrotomy within the management of anterior urethral strictures: longterm followup. Internal urethrotomy versus dilation as therapy for male urethral strictures: a prospective, randomized comparability. What is the most cost effective remedy for 1 to 2cm bulbar urethral strictures: societal strategy using decision evaluation. The vascularization of skin autografts and homografts; an experimental research in man. Longterm followup of bulbar endtoend anastomosis: a retrospective analysis of 153 patients in a single center experience.
Buy discount persantine 25 mg onlineInfusion reactions could occur in over 50% of instances of sufferers administered with rituximab or alemtuzumab medicine side effects cheap 25 mg persantine with amex. Although the precise mechanism of infusion reactions is unclear 714x treatment order persantine 25 mg without a prescription, cytokine release from lymphocytes as a result of the antibody-antigen interaction has been proposed as the mechanism medications ending in lol purchase persantine 25 mg otc. In the case of cetuximab treatment hiatal hernia cheap persantine 25 mg line, the anaphylactoid reaction is attributed to the event of galactose-1, 3-galactose. In addition, pretreatment with antihistamines and sufficient monitoring in the course of the infusion might help ameliorate these reactions. In common, the reactions are most severe with the primary infusion and tend to be less extreme with subsequent administrations. Patients present with systemic inflammatory response symptoms of hypotension, pyrexia, and rigors shortly after the infusion, and this will lead to multiple organ failure if not managed aggressively. Infections can occur following treatment with mAbs and can happen as a outcome of acquired immune deficiency following the lack of the normal cells expressing the goal ligand. Some research report an increased threat of 1% to 3% of arterial thromboembolisms among patients handled with bevacizumab. Early clinical trials evaluating trastuzumab together with anthracycline-based chemotherapy in patients with metastatic breast most cancers discovered that 27% of trial individuals, with no earlier cardiac history, experienced symptomatic coronary heart failure or asymptomatic cardiac dysfunction. Subsequent trials have shown that the incidence of heart failure was 2% to 4% and cardiac dysfunction is 3% to 19%. There is a correlation between the presence of the skin rash and response to remedy. Cessation of mAb is dependent on the toxicity and the impact that these antagonistic events have on high quality of life. As with any cancer therapies, clinicians in dialogue with their sufferers need to balance the intent, dangers, and advantages when using mAbs. Five of them are drug conjugates, two are radioconjugates, and two are bispecific antibodies. Rituximab has been used efficiently together with chemotherapeutic agents to augment the antitumor effects. The pharmacokinetics of the agent are influenced by a selection of components including the tumor burden. Early doses are probably to obtain decrease serum levels because the tumor and regular B-cells bind a larger fraction of an administered dose. After the 4th weekly dose, the half-life averages 205 hours with a maximum serum concentration of 486 g/mL. A dose of 500 mg/m2 has been tolerated, but a most tolerated dose has not been identified. Rituximab ought to be infused at an initial rate of 50 mg/h due to toxicity points related to activation of immune effector mechanisms. In most instances, the symptom complex consists of a quantity of of the next: fever and chills, nausea, pruritis, angioedema, asthenia, headache, bronchospasm, throat irritation, rhinitis, urticaria, myalgia, dizziness, or hypertension. The reactions resolve entirely with either slowing the infusion or briefly interrupting it. The infusion-related signs typically lower in incidence with each administration from nearly 80% incidence with the first to around 14% with the eighth. Diphenhydramine, acetaminophen, and intravenous fluids are sometimes required to suppress the symptoms. Once symptoms resolve, the administration of rituximab can be reinitiated at about half the rate of the preliminary infusion. In some uncommon and extreme instances, patients can develop grownup respiratory distress syndrome, myocardial infarction, ventricular fibrillation, or cardiogenic shock. Other uncommon problems embrace the development of tumor lysis syndrome from rapid killing of tumor cells and occasional Stevens-Johnson syndrome with severe mucocutaneous inflammation. When rituximab is administered with chemotherapy, some sufferers have skilled reactivation of hepatitis B. The suppression of normal B-cells by rituximab is variable in period depending on the age of the affected person and the length of treatment, but most patients get well normal B-cell perform within a year of stopping rituximab. It is particularly energetic when utilized in mixture chemotherapy and has turn into a part of ordinary remedy for diffuse massive B-cell lymphoma. It can additionally be getting used more and more to deal with autoimmune illnesses in which autoreactive antibodies play a pathogenetic role. These include idiopathic thrombocytopenic purpura, thrombotic thrombocytopenic purpura, autoimmune hemolytic anemia, and some circumstances of pure pink cell aplasia. It is administered intravenously, has a molecular mass of approximately 145 kDa, and has a half-life of 26 days. Ofatumumab demonstrated higher exercise in rituximab-sensitive or rituximabresistant cell line fashions in contrast with rituximab. Ibritumomab Tiuxetan (Zevalin) Ibritumomab tiuxetan is a murine IgG1 antibody chelated to yttrium-90, a beta-emitting isotope. Tiuxetan is the chelating agent that attaches yttrium-90 to uncovered amino groups in lysines and arginines within the antibody sequence. Like I-131 tositumomab, the ibritumomab tiuxetan therapeutic routine consists of two steps: dosimetry adopted by therapy. Dosimetry is carried out by injecting unlabeled rituximab (250 mg/m2) followed by 5 mCi of indium-111�labeled ibritumomab tiuxetan (containing 1. However, if the biodistribution of the In-111 compound is acceptable, 7 to 9 days after dosimetry dose, the patient receives a therapeutic dose of 250 mg/m2 rituximab adopted by zero. The physical half-life of the isotope is just under three days and the imply half-life of Y-90 exercise in the blood is 30 hours. In preliminary research, platelet counts lower than 50,000/L had been noted in 61% of patients, and neutrophil counts less than 1,000/L had been seen in 57% of sufferers. The danger of extreme thrombocytopenia and neutropenia elevated to 75% in sufferers whose platelet counts were between a hundred and a hundred and fifty K firstly of therapy. Median time to nadir is 7 to 9 weeks and median period of cytopenias is 3 to 5 weeks. The length of the myelosuppression complicates subsequent therapeutic selections. As can be expected, myeloid malignancies and myelodysplasias have been noted in patients surviving more than a yr. Gastrointestinal symptoms (nausea, vomiting, abdominal pain, diarrhea) occur in 10% of sufferers. Human antimouse antibodies or human antichimeric protein antibodies develop in about 4% of circumstances. A basic downside with the radiopharmaceuticals (both I-131 and Y-90) is the long-term compromise of marrow function.
Buy generic persantine 100 mg on lineThe haematological results of recombinant human growth components symptoms precede an illness persantine 25mg low cost, which include myelodys plasia medications known to cause weight gain cheap 25mg persantine visa, are dealt with on web page 617 medicine 122 order 25mg persantine amex. Zinc toxicity can result in symptoms neck pain purchase persantine 25 mg online copper deficiency with consequent anaemia, neutropenia, sideroblastic erythropoi esis and vacuolation of erythroid and myeloid precursors [56]. Chronic benzene publicity can cause erythroid dysplasia (nuclear budding, internuclear bridges and a number of nuclei), neutrophil dysplasia (pseudoPelger�Hu�t cells, hypersegmentation and abnormal mitotic forms), eosinophil dyspla sia (giant granules in precursors) and megakary ocyte dysplasia (nonlobated, hyperlobated or a quantity of nuclei) together with hypoplasia and variable cytopenia [58]. Hypervitaminosis A has been related to anaemia and thrombocyto penia with lowered erythroid precursors and megakaryocytes [59]. Mustard fuel can produce effects just like these of alkylating agents; delayed neutropenia, thrombocytopenia and bone marrow hypoplasia were reported following exposure through the Iran�Iraq struggle [61]. The impact of irradiation on the bone marrow Irradiation of a major proportion of the bone marrow causes a fall in neutrophil and platelet counts. Peripheral blood the blood film might present neutropenia, thrombocy topenia and the features of anaemia. Bone marrow cytology the preliminary change in irradiated bone marrow is pyk nosis and karyorrhexis of haemopoietic cells fol lowed by disappearance of haemopoietic and fat cells and replacement by areas of gelatinous transforma tion. Subsequently, on the site of irradiation, hypo plastic marrow is discovered, with haemopoietic cells being changed by fats. Extensive high dose irradiation of the bone marrow is adopted by aplastic anaemia. Bone marrow histology Initially, there may be necrosis of the bone marrow inside the area that has acquired excessive dose radia tion. Cell loss is initially best adjacent to trabec ulae as extra mature postproliferative cells within the central marrow space are more radioresistant. Problems and pitfalls It is essential to concentrate on previous irradiation and avoid biopsy at such sites. Peripheral blood There is a normocytic or macrocytic anaemia with pink cells being normochromic. There may be increased iron in macrophages and iron in plasma cells [62] and endothelial cells [63]. The latter phenomenon may be famous within the absence of any enhance in macrophage iron [63]. Problems and pitfalls It is essential to pay attention to the chance of excess alcohol intake in interpreting cytopenias and dysplastic options. The neutrophil depend is often regular however the capability of the bone marrow to mount a neutrophil response to infection is lowered and an infection can lead to neutropenia. Bone marrow cytology Erythropoiesis is normoblastic, macronormoblastic or mildly megaloblastic. Siderotic granules are outstanding and there could additionally be ring sideroblasts; typically these are quite a few. Iron stores can be increased; generally haemosiderin inclu sions are current in plasma cells [62]. Megakaryocytes are often increased [63] but a marked decrease has additionally been reported [64]. Aplastic anaemia Aplastic anaemia is a heterogeneous dysfunction characterized by pancytopenia and a hypocellular marrow without any apparent underlying neo plastic course of. The name, although nicely established, is somewhat mis leading since all haemopoietic lineages are involved. Incidence is lower in Europe and North America than in numerous other components of the world. Although some cases of aplastic anaemia outcome from an inherited dysfunction and develop in infancy or childhood, the incidence, in general, will increase with age with two peaks at 10�25 years and above 60 years. Fanconi anaemia is heterogeneous, at least 21 completely different genes having been implicated. Spontaneous improvement of blood counts can happen as a result of a second acquired mutation that corrects or compensates for the inherited mutation [71]. Aplastic anaemia can observe hepatitis that clinically resembles viral hepatitis however proof of a viral aetiology has not been found. Aplastic anaemia can happen in affiliation with acute parvovirus B19 an infection [76]. Aplastic anae mia can be the preliminary presentation of systemic lupus erythematosus [77]. The analysis of aplastic anaemia may be suspected from peripheral blood and bone marrow aspirate findings however trephine biopsy is important for diag nosis. This is due to the frequent problem in obtaining an sufficient aspirate and the variable diploma of hypoplasia in different areas of the marrow. Prior to the development of stem cell trans plantation and immunosuppressive remedy, the prognosis of aplastic anaemia was poor with severe cases having a median survival of less than a 12 months. With immunosuppressive remedy (anti lymphocyte globulin plus ciclosporin) or stem cell transplantation from a histocompatible sibling, 5year survivals of the order of 50�70% can be anticipated. Aplastic anaemia has been categorized, on the premise of peripheral blood and bone marrow options as extreme, very extreme or nonsevere. Aplastic anaemia is assessed as extreme if a minimum of two of three periph eral blood criteria are met � reticulocyte depend much less Table 9. In Shwachman�Diamond syndrome, neutropenia often develops first, with pancytopenia � ensuing from aplastic anaemia � following. Similarly, in amegakaryocytic thrombocytopenia the thrombo cytopenia occurs in advance of pancytopenia. Peripheral blood Severe cases are characterised by pancytopenia and a low reticulocyte count. The anaemia may be normocytic or macro cytic, polychromasia is absent and poikilocytes may be current; generally poikilocytosis is marked. Neutrophils usually have darkish red granules and excessive alkaline phosphatase activity, even in the absence of any obvious infection. Platelets are of regular dimension, in distinction to the big platelets that are widespread when thrombocytopenia is the results of elevated platelet destruction. Macrocytosis and borderline cytopenias could persist following remis sion induced by immunosuppressive therapy. In a minority of sufferers the aspirate is normocel lular or even hypercellular [80,82]. The bone marrow aspirate shows a minimal of a relative enhance in lymphocytes and typically an absolute enhance. As in the aspirate, in the early phases of the illness there can be outstanding haemophagocytosis [32]. Reactive lym phoid aggregates, sometimes with a welldeveloped germinal centre, are additionally elevated, notably early within the illness course and in patients in whom aplastic anaemia develops in the setting of rheuma toid arthritis or systemic lupus erythematosus [32]. Bone marrow histology Trephine biopsy is essential within the prognosis of aplas tic anaemia. Sinusoids are decreased but arterioles and capillaries are normal or increased [85]. A distinctive look has been observed in aplastic anaemia induced by acetazolamide.

Cheap persantine 100 mg visaImmunophenotype Flow cytometric immunophenotyping exhibits a combined inhabitants of cells medicine bg order 100 mg persantine with amex. Cytogenetic and molecular genetic analysis Cytogenetic evaluation exhibits either inv(16)(p13 treatment for 6mm kidney stone order persantine 100 mg mastercard. The most frequent further abnormalities are trisomy eight and trisomy 22 (the latter fairly particular for this subtype) symptoms rsv generic persantine 100mg with amex. Molecular analysis is diagnosti cally necessary since the cytogenetic abnormality is refined and can be missed treatment of uti discount persantine 100 mg on-line. Rapid, right diagno sis is of critical importance so that particular targeted therapy can be utilized and early demise from haem orrhage avoided. However, the bone marrow aspirate is necessary in diagnosis since there may be solely infrequent leukaemic cells within the peripheral blood and, in the variant type, the bone marrow usually accommodates a better proportion of typi cal hypergranular cells than does the blood. The predominant cells may be hypergranular promye locytes or hypogranular bilobed promyelocytes with a variable admixture of hypergranular types. Erythroid cells and megakaryocytes are also significantly lowered in quantity however are cyto logically normal. Cytochemistry Cytochemical stains are pointless in typical hypergranular acute promyelocytic leukaemia but 201 could be essential in confirming a diagnosis of the variant type. In the variant type the granules are a lot smaller and could additionally be inconspicuous; the nuclei are sometimes bilobed. Because of their hypergranularity, the leukaemic cells of typical instances can be readily recognized in haematoxylin and eosin (H&E)stained sections of trephine biopsy specimens. A proportion of circumstances of the variant form can additionally be recognized from cyto logical options. There is an accompanying reactive improve in small blood vessels within the bone marrow stroma [17]. During follow up after remedy with arsenic trioxide, elevated osteoblasts surrounding trabeculae have been noticed [21]. Immunophenotype the immunophenotype is very characteristic and diagnostically useful in the variant type. Clinical presentation can include myeloid sarcomas and a sample of tissue infiltration (gums and skin) typical of leukaemia with monocytic differentiation. Peripheral blood the peripheral blood most frequently shows predomi nant monoblasts, with or without promonocytes. Monoblasts are large cells with a round or oval nucleus, a delicate chromatin sample and plenti ful cytoplasm. Bone marrow cytology the bone marrow is usually infiltrated primarily by monoblasts. Bone marrow histology There is usually heavy infiltration by monoblasts with some maturing cells. Cytogenetic and molecular genetic evaluation Cytogenetic evaluation exhibits t(9;11)(p21. Peripheral blood the peripheral movie shows blast cells, dysplastic maturing cells of neutrophil lineage and sometimes increased basophils, which can be partly degranu lated. Bone marrow cytology the bone marrow aspirate reveals increased blast cells and dysplastic maturing cells, often of basophil as nicely as neutrophil lineage. A toluidine blue stain shows metachromatic (pink) staining of granules in basophils and their precursors. Bone marrow histology There is a hypercellular marrow with both blast cells and maturing granulocytes. Terminal deoxy nucleotidyl transferase (TdT) expression is in seen in about half of patients [16]. Bone marrow histology There is an increase of blast cells and often promenade inent trilineage dysplasia. Cytogenetic and molecular genetic evaluation Cytogenetic analysis most often shows inv(3) (q21. Bone marrow cytology A bone marrow aspirate shows elevated blast cells but the quantity may not be very high, generally being lower than 20%. Bone marrow histology There is a rise in blast cells; elevated reticulin deposition and collagen fibrosis are frequent [16]. Bone marrow cytology A bone marrow aspirate reveals elevated blast cells with or without maturation. Bone marrow histology There is an increase in blast cells, with or with out maturation. There is often monocytic differ entiation however granulocytic differentiation and erythroleukaemia are additionally seen. Bone marrow histology There is a hypercellular marrow, most often with monocytic differentiation. Dako clone 376) exhibits � in addition to normal nuclear expression � cytoplasmic expres sion of the protein, which can be used as a surrogate marker for mutation of the gene. There may be a sample of tissue infiltration consistent with monocytic differentia tion. Cytogenetic and molecular genetic analysis Cytogenetic analysis is normally regular however miscel laneous abnormalities are present in 5�15% of instances [16]. In the 2016 revision this is a definitive entity however the mutation must be biallelic. Peripheral blood the peripheral blood reveals blast cells, with or with out maturation. Bone marrow cytology Bone marrow aspiration exhibits elevated myeloblasts, with or with out maturation. Bone marrow histology There is an increase of blast cells, with or without maturation. Criteria were altered in the 2016 revision with del(9q) not being a defining cytogenetic abnormality and with other refinements of the cytogenetic standards being made [25]. Micromegakaryocytes are often present and there may be multinu cleated or other dysplastic megakaryocytes. Cases are included on this category if the sufferers have been beforehand exposed to anticancer chemotherapy or irradiation. Some cases of remedy related myeloid neoplasms comply with autologous or allogeneic stem cell transplantation and some comply with treatment of nonneoplastic issues. Bone marrow histology Stromal changes, particularly reticulin or collagen fibrosis and hypocellularity, are widespread in alkylat ing agentrelated circumstances. Cytogenetic and molecular genetic analysis An abnormal karyotype is seen in about 90% of sufferers. The cytogenetic abnormalities that are seen following exposure to alkylating brokers and associated drugs are usually unbalanced and include abnormalities of chromosomes 5 and 7 and complex karyotypes. Bone marrow cytology In instances associated to alkylating brokers, a bone marrow aspirate could also be difficult to get hold of due to hypocellularity or fibrosis. Cytologically and histologically, the findings are of small to medium sized blast cells with no granules or Auer rods.
References - Leppla D, Browne R, Hill K, et al: Effect of amiloride with or without hydrochlorothiazide on urinary calcium and saturation of calcium salts, J Clin Endocrinol Metab 57(5):920n924, 1983.
- Park J, Keller EE, Reid KI. Surgical management of advanced degenerative arthritis of temporomandibular joint with metal fossa-eminence hemijoint replacement prosthesis: an 8-year retrospective pilot study. J Oral Maxillofac Surg. 2004;62:320-8.
- Ando M, Takao A. Pathological anatomy of ventricular septal defect associated with aortic valve prolapse and regurgitation Heart vessels. 1986;2:117-126.
- Haselkorn T, Zeiger RS, Chipps BE, et al. Recent asthma exacerbations predict future exacerbations in children with severe or difficult-to-treat asthma. J Allergy Clin Immunol 2009; 124: 921-927.
|