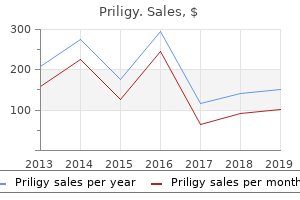
Priligy
Robert J. Lipinski, Ph.D - University of Wisconsin – Madison
- Madison, Wisconsin
Order 60mg priligy free shippingGreater than 200 repeats will cause the historically acknowledged fragile X syndrome erectile dysfunction johannesburg discount priligy 90 mg with visa, which is a common reason for mental incapacity in boys erectile dysfunction exercise video order 90 mg priligy amex. Bolded features and findings represent those that can be significantly helpful for narrowing medical analysis psychological reasons for erectile dysfunction causes discount priligy 30mg fast delivery, as they can be more specific for the related condition pump for erectile dysfunction buy priligy 60 mg. In addition, mitochondrial diseases are difficult multisystem illnesses, affecting these organ systems dependent on excessive levels of energy manufacturing, together with the mind, heart, and skeletal muscle. Onset is usually in the sixth decade of life, with a speedy development and imply survival of lower than 10 years after prognosis. Symptomatic ataxias due to structural lesions are often the straightforward ataxias to diagnose and often the best to deal with. In addition to attainable strokes and tumors, a structural trigger that may commonly trigger ataxia is superficial siderosis. This dysfunction is caused by the deposition of free iron and hemosiderin along the surfaces of the involved constructions, namely the cerebellum, brainstem, and temporal lobes. One of the frequent types of persistent cerebellar ataxia is alcoholic cerebellar degeneration, typically seen in middleaged males with a historical past of chronic alcohol abuse. This presents mainly with ataxia of gait and the lower extremities, with less impairment seen within the higher extremities or with speech. Onset could be either speedy or slowly progressive, and signs can improve with strict abstinence from alcohol. This disease is likely related not solely to the directly poisonous results of alcohol on the mind but additionally to thiamine deficiency, as studies have proven a dependable inverse relationship between serum vitamin B1 ranges and the diploma of cerebellar atrophy. Paraneoplastic cerebellar degeneration is being increasingly recognized as a frequent cause of ataxia, with multiple cerebellar specific antineuronal antibodies described. The generally associated cancers are smallcell lung, breast, and ovarian cancers, and Hodgkin lymphoma. These syndromes often comply with a subacute, but relentlessly progressive course, with poor response to steroids, intravenous immunoglobulin or plasma exchange, though Hodgkin lymphoma might respond. Survival ultimately is determined by the underlying tumor sort, if it can be discovered. The present mainstays of remedy are bodily, occupational, and speech therapy. Physical therapists should be aware that sufferers with cerebellar dysfunction incessantly have impaired motor studying, so instructions should be explicit throughout coaching. Social workers, psychologists, psychiatrists and genetic counselors are additionally necessary members of the multidisciplinary ataxia staff. For symptomatic ataxias, therapy of the underlying cause is best, such as correcting nutritional deficiencies, avoiding toxins, treating underlying malignancies or immunomodulation. Buspirone, as much as 30 mg twice daily, has been shown in small case sequence to be efficient for some patients. Both varenicline (1 mg twice daily) and riluzole (1 mg twice daily) have each been reported in isolated patients to be effective to enhance gait ataxia. However, longterm use of varenicline has not been studied, and both medicines are quite costly and unlikely to be lined by insurance coverage in the United States. Treatment of related symptoms that usually accompany ataxia, corresponding to tremor, dystonia, or parkinsonism, could be approached with appropriate medications for those situations. Active analysis continues into diseasemodifying therapies for the ataxias, focusing primarily on the polyglutamine disease. Research into the effectiveness of free radical scavengers, similar to alphalipoic acid, mitochondrial stabilizers (like coenzyme q10 and creatine), and antiexcitotoxic agents, similar to amantadine and riluzole, is underway. There have been some benefits seen in animal studies, but much less dramatic enchancment in human studies so far. Other areas of research embrace gene remedy and stem cell remedy, in addition to less invasive choices like transcranial magnetic stimulation to the cerebellum. The first scientific description is found within the works of a well-known seventeenthcentury anatomist and doctor, Sir Thomas Willis. In the Nineteen Forties, Swedish neurologist, Karl Ekbom, published a series of manuscripts describing the number of symptoms of this dysfunction and its negative impact on sleep and high quality of life. He additionally noted the familial nature of this dysfunction and association with pregnancy, anemia, and other medical circumstances. He reported that the dysfunction is pretty widespread, could be disabling, and is well recognized if physicians realize it. Therefore it was just lately advised that the name of the disorder should be officially changed to Willis�Ekbom syndrome. There are 4 essential diagnostic standards and three supportive non-essential medical options. The first essential criterion is an urge to move the legs, often accompanied or caused by uncomfortable and unpleasant sensations in the legs. The most common descriptions are creeping, crawling, pulling, squeezing, itching, tingling, or restlessness. These sensations are normally bilateral, however they are often asymmetric and normally are experienced as deep "within the muscles or bones. The second essential criterion is an urge to move or unpleasant sensation that begins or worsens in periods of relaxation or inactivity, such as laying or sitting. An urge to move legs often accompanied or brought on by uncomfortable and unpleasant sensations in the legs 2. The urge to move or the disagreeable sensations begin or worsen in periods of rest or inactivity corresponding to laying or sitting 3. The urge to transfer or disagreeable sensations are partially or completely relieved by motion similar to strolling or stretching, no less than so lengthy as exercise continues four. The urge to move or unpleasant sensations are worse within the evening or at evening Supportive nonessential medical options 1. Intermittent and relapsing clinical course, especially at the beginning of the illness three. The third essential criterion is that the urge to transfer or unpleasant sensations are partially or totally relieved by motion such as walking or stretching, a minimum of so long as the activity continues. Finally, the fourth important criterion is that the urge to move or unpleasant sensation is worse within the evening or at evening than during the day, or might only occur in the evening or night time. It is tough to decide if this nighttime worsening is because of the fact that durations of inactivity. Associated nonessential options include sleep disturbances, an intermittent and relapsing scientific course (especially firstly of the disease), and in any other case normal physical and neurological examination. Younger patients tend to have more waxing and waning signs, while these older than age 50 may need a more abrupt onset, with extreme and fixed signs. There are some clues that may be useful in differentiation of those situations. Both sexes and all ethnicities are affected; nevertheless, incidence is much higher in Caucasians and ladies. Neurological examination is essential to rule out other neurological issues.
Cheap priligy 90 mg with mastercardTherefore erectile dysfunction daily pill buy cheap priligy 60mg on-line, spinal wire injury above sacral ranges might interrupt the command for sphincter rest experimental erectile dysfunction drugs priligy 90mg free shipping. Since most spinal wire harm is above S2 erectile dysfunction viagra does not work discount priligy 30mg, micturition is usually affected in spinal cord-injured patients xyrem erectile dysfunction order 90mg priligy with mastercard. The urinary retention that outcomes from interrupting this message is potentially lethal and should be treated, sometimes with catheterization, with some urgency. However, for our current purposes, we simply think about giant and small caliber, or diameter, fibers. It is of nice advantage that each one movement-serving fibers are myelinated and conduct motion potentials very rapidly. Rapid conduction of action potentials in motoneuron axons innervating skeletal muscle tissue allows fast execution of motion commands. Moreover, quick motor corrections within the face of sudden obstacles are enabled by fastconducting sensory fibers, such as these serving proprioception. Any delay in both muscle management or sensory suggestions would inevitably impair motion. Another group of enormous diameter fibers are sensory axons that help the perception of touch and contribute to the sensory feedback essential for voluntary actions. Small caliber fibers serve a range of varied features that can be broadly categorized as sensory and autonomic. Small diameter major afferent fibers carry sensory data that will result in perceptions of ache or temperature. Other small diameter main afferent fibers carry details about pleasurable touch. Still other small caliber fibers are efferents, postganglionic axons from autonomic ganglion neurons that target heterogeneous tissues and produce a broad variety of homeostatic results. They are a heterogeneous group of syndromes attributable to numerous etiologies that end in damage to peripheral nerve fibers, their myelin sheaths, or each. The symptoms of neuropathies depend on the sort or kinds of peripheral fibers damaged, which in flip differ across etiologies. Traumatic injury, meaning harm as a end result of physical influence, cutting, tearing, or crushing, of a peripheral nerve causes indiscriminate damage to each large and small nerve fibers and therefore has motor and sensory penalties. Compression neuropathies, such as the common carpal tunnel syndrome, come up from trauma, repetitive use, ischemia, and sure from elements but to be found. Several metabolic and autoimmune diseases target peripheral nerve fibers that have a selected molecular signature or metabolic vulnerability. For example, the hyperglycemia and plasma hyperosmolality current in diabetic sufferers tend to selectively damage giant diameter sensory fibers serving contact and cause largely sensory scientific signs. GuillainBarrďż˝ syndrome is an autoimmune situation that causes an acute and, in most people, transient demyelination of enormous diameter fibers, thereby inflicting primarily motor signs. Finally, diverse inherited neuropathies target developmental packages important to the development of specific subsets of nerve fibers, causing correspondingly numerous sets of signs. The longest nerves are most susceptible to neuropathies caused by trauma or environmental publicity. Furthermore, since all tissues distal to the site of harm may be affected, the most common neuropathies contain the ft, located on the distal finish of our longest nerves. Because the palms also are susceptible to long-nerve injury, patients frequently present with symptoms in a glove and stocking distribution. For causes which are additionally associated to nerve length, neuropathies produce sympathetic dysfunction much more regularly than parasympathetic dysfunction. Recall that parasympathetic ganglia are very close to their targets; thus, parasympathetic postganglionic axons are quick. In contrast, sympathetic postganglionic axons that innervate sweat glands and cutaneous blood vessels, including vessels supplying the nail beds, are long and extensively distributed. In sum, the predominant fiber sorts affected in most neuropathies are (1) giant diameter motor-serving axons, (2) giant diameter sensory fibers involved in contact, (3) small diameter sensory fibers involved in signaling ache and temperature, and (4) small diameter sympathetic fibers innervating cutaneous blood vessels and sweat glands. Damage to large diameter fibers produces weak point by interfering with motoneuronal innervation of skeletal muscle. For example, a neuropathy may trigger foot drop, or it may lead to an inadequate grip. Deficits in proprioception, which is dependent upon massive diameter proprioceptive fibers, can exacerbate motor symptoms, leading to "clumsiness. In contrast to the adverse indicators ensuing from damage to fibers involved in motor management, sensory fiber harm typically results in paresthesias and optimistic signs, as explained earlier. The sensory penalties, ensuing from damage to fibers supporting ache and temperature perception, are sometimes dysesthesias. Dysesthesias range tremendously, ranging from an unpleasant sensation of pins and needles to an insupportable burning pain. Autonomic motor symptoms are primarily negative so that small diameter neuropathies may be accompanied by flushed and dry pores and skin due to a lack of vasoconstriction and sweating. Changes in the appearance of nails because of interruption of the vascular provide to the nail mattress are additionally a typical symptom. This association is another evolutionary inheritance from our quadrupedal ancestors. Note that these territories appear primarily as horizontal slices via the trunk but as longitudinal slices within the limbs. Limb dermatomes really share the same orientation as trunk dermatomes in a quadruped. Thus, in a person on all fours, the orientations of the dermatomes in trunk and limbs are roughly parallel. The prime of the pinnacle, face, and oral cavity are innervated by the fifth cranial nerve (see Chapter 5). The innervation of the ear (not shown) is shared by the C2 spinal nerve and a number of other cranial nerves. B: Nerve territories differ considerably from dermatomes in shape and orientation. The few examples illustrated here show that nerve territories can reduce throughout dermatomes. For example, the territory provided by the median nerve consists of components of dermatomes from segments C6 to C8. The territory of the lateral cutaneous nerve consists of parts of a number of lumbar dermatomes. In other cases, notably within the trunk, nerve territories are considerably smaller than dermatomes. For instance, the ventral rami from the thoracic nerves innervate no more than a quarter of the corresponding thoracic dermatome. The varicella zoster virus initially causes chickenpox, often in younger youngsters. At the time of the preliminary infection, virus particles could also be taken up by sensory neuron terminals and retrogradely transported again to the sensory afferent somata.
Order priligy 90mg on lineHemiballism and hemichorea are considered to symbolize two extremes of the same dysfunction cost of erectile dysfunction injections discount priligy 60mg without prescription. In most cases impotence forums priligy 30 mg amex, the movements remit completely inside several months erectile dysfunction protocol download free proven 60mg priligy, both spontaneously or following short-term pharmacological therapy cost of erectile dysfunction injections cheap priligy 60 mg overnight delivery. Treatment is aimed at the underlying reason for the lesion, which typically is a focal stroke. In addition, dopamine receptor antagonists assist lower the prevalence of extra movements and due to this fact help patients, particularly in the preliminary weeks. Hyperglycemia secondary to diabetes mellitus is the second most typical explanation for hemiballism. In hyperglycemic hemiballism, movements are transiently present for as long as blood sugar is abnormal. The pathophysiology of this just lately acknowledged disorder, most prevalent in individuals of East Asian origin, is unknown and worthy of research. For a relatively rare disorder, hemiballismus is very well-known amongst medical professionals. For years, hemiballism was thought to outcome solely from a lesion of the subthalamic nucleus contralateral to the affected limbs. The interpretation is that, because of loss of the worldwide inhibition supplied by the hyperdirect pathway, the somatomotor cortex turns into overly excitable. Essentially, hemiballism has been used for many years to teach students the role of the subthalamic nucleus in suppressing motion. A: A 34-year-old man with a stroke in the right center cerebral artery presented with left-sided hemiballism. Affected areas embody cerebral cortex and various other small areas within the striatum and pallidum (arrows). Note that radiological conference is that the left facet of the mind is illustrated on the right and right aspect of the mind on the left. Unfortunately, this enticing teaching gadget can no longer be employed in good faith. Lesions that produce hemiballism are discovered within the putamen, thalamus, or deep white matter and occasionally, in about 20� 25% of cases, in the subthalamic nucleus. Does this neuropathological discovering mean that our interpretation of the function of subthalamic nucleus operate is all mistaken The concept that the subthalamus facilitates basal ganglia output and thereby depresses movements is still broadly accepted. An understanding of the pathophysiology involved in these nonconventional however extra representative circumstances of hemiballism represents an intriguing puzzle for future investigators. In the direct pathway, info from broad areas of sensorimotor cortex-somatosensory and first motor cortices, supplementary motor and premotor areas-reaches the putamen by way of unmyelinated corticostriatal axons. Through elimination of the tonic inhibition of thalamic neurons, engagement of the direct pathway leads to a rise in the discharge of thalamic neurons. An enhance in thalamic activity is handed on to motor control centers, facilitating the initiation of the selected action. The web effect of the direct pathway is the activation of a centered ensemble of cells in somatomotor cortex. Neurons in somatomotor cortex (M1) are usually inactive however discharge before initiating a movement. The resulting disinhibition of thalamic cells facilitates somatomotor cortex and finally movement. B: Multiplying the signal of each connection within the direct pathway (top) yields a internet facilitatory impact (bottom). Therefore, when placed in collection, striatal inhibition of pallidal inhibition causes disinhibition, which, as you recall from Chapter 24, has the web effect of accelerating discharge fee. The direct pathway solely works as a result of pallidal cells discharge tonically, rendering them sensitive to inhibitory influences from striatum. Indeed, pallidal cells in addition to cells in substantia nigra pars reticulata discharge tonically at rates of 50�100 Hz. In the direct pathway, the striatum, inside globus pallidus, and substantia nigra pars reticulata are the only nuclei that are thought of part of the basal ganglia. Therefore, when cortical enter engages the direct pathway, the output of the basal ganglia decreases. Because the basal ganglia output to thalamus is inhibitory, a lower in basal ganglia output leads to more activity in thalamic and consequently cortical neurons, and issues occur. Imagine having to use a modified alphabet in which a is b, b is c, and so forth until z is a. Typing or writing a single word (uif in place of the) could be feasible only through deliberate action. Then think about having to employ the same level of conscious effort to have the ability to walk across a room, converse, deliver food to the mouth, and so on. The gait of affected people becomes shuffling, involving small steps with little or no clearance above the bottom in the course of the swing section. The parkinsonian tremor includes the thumb and forefinger transferring as if rolling pills and thus has been referred to as a pillrolling tremor. There are two routes by which a loss of dopaminergic neurons may lead to a poverty of movement. The second route via which a loss of dopaminergic tone may impression the initiation of actions is thru dopaminergic modulation of the direct and indirect pathways. As a consequence of dopaminergic neuronal loss, the direct pathway is now not facilitated through actions mediated by D1 receptors. Additionally, D 2 receptor-mediated despair of the indirect pathway declines with the lack of the dopaminergic nigrostriatal pathways. In sum, the behavioral results are (1) issue in initiating movements due to disfacilitation, that means a decrease in excitation, of the direct pathway and (2) exuberant suppression of movements through disinhibition of indirect pathways. Unfortunately, people handled with dopamine alternative over an prolonged time period often stop responding well to the treatment. They could freeze up because the final dose of L-Dopa wears off, or they may develop extra tic-like movements due to drug-induced dyskinesia (tardive dyskinesia, as mentioned earlier). In some sufferers, the freezing and hyperkinetic states alternate in a state of rapidly alternating on and off states with altogether too brief intervals of consolation between. The unlucky consequences of long-term L-Dopa therapy enhance in likelihood with remedy duration, main some to delay L-Dopa therapy of sufferers within the early levels of disease. The logic of this tactic is clear: delaying the start of L-Dopa remedy will delay the arrival of debilitating unwanted aspect effects consequent to long-term use. This in turn moderates the danger of developing dyskinesia and decreases the dosage of dopaminergic drugs that a patient requires. The development of dopamine substitute therapy in the Sixties was revolutionary as a result of it significantly improved the lives of patients and continues to do so to today. An actual remedy for Parkinson illness remains a hope for the lengthy run however is only prone to come after an understanding of why dopamine cells die is achieved. External globus pallidus cells in turn inhibit subthalamic neurons, causing a internet disinhibition because of the back-to-back inhibitory indicators.
Buy priligy 60mg without prescriptionThe corticospinal tract (cst) continues to travel in the center third of the cerebral peduncles erectile dysfunction at age 28 discount priligy 90 mg mastercard. Although nonetheless current free sample erectile dysfunction pills buy 30 mg priligy, the cerebral peduncles are oriented more dorsoventrally than is the case more caudally erectile dysfunction drugs and heart disease discount 90mg priligy with mastercard. Just anterior to this part jack3d causes erectile dysfunction purchase 90 mg priligy free shipping, axons from the cerebral peduncles be part of the inner capsule of the forebrain. As they near their thalamic vacation spot, the medial lemniscus (ml) and spinothalamic tract (stt) are poorly delineated. Consequently, damage in this area normally impairs the function of each pathways. The medial longitudinal fasciculus at this degree serves to join gaze management facilities with extra caudal areas containing extraocular and neck motoneurons. The pulvinar, another thalamic nucleus essential in vision, seems as a pillow (pulvinar is Latin for cushion or pillow) atop the part. The optic tract (ot) carries visual info from the retina into the lateral geniculate nucleus, wrapping around the cerebral peduncles alongside the way. The neighboring positions of the optic and corticospinal tracts underlie the scientific syndrome of contralateral paralysis and hemianopia that follows harm on this region. Clear indicators of the midbrain at the mesodiencephalic junction embrace: � Red nucleus: the supply of the rubrospinal tract essential in descending motor management � Superior colliculus: A region essential in coordinating orienting actions � Cerebral peduncles: Containing corticospinal, corticobulbar, and corticopontine fibers � Substantia nigra: Consisting of the pars reticulata, carrying the output of the basal ganglia to targets together with the superior colliculus, and the pars compacta, the supply of dopamine in the striatum � Posterior commissure: Connects fibers on both facet of the dorsal mid-brain necessary in coordinating a bilateral reaction to visual stimuli the medial lemniscus and spinothalamic tracts remain in about the same relative location as extra caudally as they close to their targets within the posterior thalamus. Three thalamic nuclei are already visible: � the medial geniculate nucleus processes auditory information from both ears and projects to the first auditory cortex. Although not attached to the mind at this point, the mammillary our bodies, an essential a part of the "limbic system" concerned in memory, are seen floating below the part. The mammillary our bodies take part within the Papez circuit, which is important in each reminiscence and emotion (see Chapter 7). The mammillary our bodies degenerate as a outcome of thiamine deficiency, giving rise to an amnesic syndrome referred to as Korsakoff syndrome. Korsakoff syndrome, widespread in sufferers with superior alcoholism, causes a deficit in explicit memory whereas leaving implicit reminiscence relatively intact. An illustrative story involves the neurologist �duoard Clapar�de, who positioned a pin in his hand and then shook hands with a Korsakoff syndrome affected person, causing the affected person to expertise a short pricking pain. Such subconscious memories that influence our actions without producing acutely aware awareness are termed implicit reminiscences. The combination of mesencephalic and diencephalic buildings present on the midbrain� diencephalon junction are listed in Box 6-10. The jack-of-all-trades character of the brainstem matches the array of features served by specialized tissues of the top. The head has a mouth, ears, eyes, and an airway that helps respiration and speech. The brainstem serves the pinnacle, enabling the numerous tissues of the pinnacle to look around, hear, speak, ingest solids and liquids, and sense head position with respect to gravity. The brainstem even contributes to the control of visceral function and postural control of the physique. The features of the spinal cord are less varied, being restricted to somatosensory, somatomotor, and autonomic motor capabilities. The concrete functions of the forebrain-smell, imaginative and prescient, hormone release-are additionally fewer than these of the brainstem. Because the brainstem is so integral to life as we all know it, even a small lesion within the brainstem may be devastating, almost inevitably damaging a number of capabilities. Understanding and remembering the capabilities and construction of the brainstem takes effort and might feel overwhelming. Yet, millimeter for millimeter or milligram for milligram, the brainstem is worth it in phrases of diagnostic energy. The forebrain leaves the hard work of keeping us alive to the brainstem and spinal wire while taking full credit score and holding complete accountability for all the lofty functions that we get pleasure from. In essence, "life" is possible, but actually not as rich with out the myriad contributions of the forebrain. On an anatomical level, as we noticed in Chapter three, the human telencephalon has taken twists and turns that render its threedimensional visualization daunting. On a useful degree, what the telencephalon "does" is extra complex and nuanced than even the most expert use of language can depict. Indeed, whole books and library sections are dedicated to understanding every of the capabilities which are coated in this chapter. Linguistic limitations together with instructional constraints drive us to cut back mind areas, connections, pathways, and circuits into words, sentences, and paragraphs. Even so, the ultimate aim of providing future physicians with sufficient understanding of the mind to fuel their future careers is attainable. As you know, a elementary embryological division happens between the diencephalon and telencephalon. The hypothalamus is important to maintaining body homeostasis, responding to physiological challenges, and to expressing feelings. The thalamus, or dorsal thalamus, consists of about a dozen nuclei with features primarily targeted on sensory, motor, emotional, or executive processing. Nearly all inputs destined for the cerebral cortex have only oblique entry to the cortex through a synapse in the thalamus. Primary motor (M1), somatosensory (S1), and auditory (A1) cortices, and a small bit of main visible cortex (V1) are evident. The giant Sylvian fissure or lateral sulcus (dashed line) divides the temporal cortex, housing auditory cortex, from parietal and frontal cortices, whereas the central sulcus (not labeled) separates the M1-containing frontal lobe from the S1containing parietal lobe. Additional cortical areas seen are the prefrontal cortex, an area important to organizing behavior; parietal affiliation cortex the place sensory inputs are integrated; and inferotemporal cortex where visual objects are recognized and their that means understood. B: A mid-sagittal view of the brain reveals the thalamus (T), hypothalamus (H), and most of primary visible cortex. The cingulate gyrus, posterior part of the orbitofrontal cortex, parahippocampal gyrus, and fornix (f) wrap around the diencephalon. In this chapter, we discuss the following cortical areas: � Primary sensory cortices are important way-stations for somatosensory, visible, and auditory notion. Information arrives in the hippocampus, and memories are shipped out of the hippocampus to other regions of cerebral cortex for storage. Pierre Paul Broca, a French neurologist who made quite a few and varied contributions to our understanding of forebrain perform, initially used the time period "limbic" to refer to constructions that border (limbus is the Latin word for "border") the diencephalon. These constructions included the cingulate gyrus, hippocampus, orbitofrontal cortex (ofc), parahippocampal gyrus (phg), and fornix. Today, anterior thalamus, amygdala, and the hypothalamus together with the mammillary bodies, are additionally thought of to be limbic constructions.
Cheap 60 mg priligy with visaMoreover erectile dysfunction medications side effects generic priligy 30 mg overnight delivery, vestibular projections to the cerebellum also contribute to the motor coordination of postural stability and eye actions with head place and physique movement erectile dysfunction causes young males discount priligy 30mg line. The secondary sensory neuron in the visual system that corresponds to a vestibular nucleus neuron is within the retina erectile dysfunction in young males causes 90mg priligy otc. Of course impotence quotes priligy 60mg fast delivery, no retinal (or geniculate or visual cortex) neuron tasks to a motoneuron or even to a motor control middle. The contrast between visible and vestibular pathways highlights the extreme motor emphasis of the vestibular system. Under normal, all-is-well conditions, the output of the vestibular system is totally motor in character. However, when vestibular well-being is challenged, vestibular notion involves the fore, together with autonomic distress. Putting on glasses with a poor prescription, spinning, or diving from a excessive board all can elicit an disagreeable notion of vertigo or disequilibrium. From thalamus, vestibular data reaches areas close to the pinnacle representation in somatosensory cortex. Stimulation within "vestibular" cortical areas most incessantly produces a way of motion, imbalance, or vertigo, more proof that vestibular perception is restricted to impaired situations. Vestibular pathways additionally reach brainstem and cortical areas concerned in homeostasis. Connections between vestibular and brainstem areas such because the nucleus of the solitary tract may assist the uncomfortable bodily feeling that accompanies falling. First, vestibular information is important to spatial orientation and the sense of self in house. The comorbidity, or coincidence, of tension disorders and signs reflective of vestibular dysfunction-dizziness, vertigo, disequilibrium, and nausea-may result from the sturdy influence of vestibular inputs on emotional and homeostatic systems. Response to static tilts of peripheral neurons innervating otolith organs of the squirrel monkey. Physiology of peripheral neurons innervating semicircular canals of the squirrel monkey. The large amount of neural territory dedicated to gaze management displays the distinctive importance of sustaining a gradual gaze when so desired or, alternatively, of changing the direction of gaze when needed. Brain circuits exert exquisite control over the place and orientation of the visual axis between the pupil and the fovea. We effortlessly maintain our gaze regular, never even excited about this as a task or an accomplishment. To illustrate the difference to your self, examine the way you fare attempting to both learn or write whereas strolling. Mothers bond with their youngsters by way of mutual gaze, which elicits oxytocin release within the mom, which in turn facilitates attachment and nurturing behavior. This loop between gaze, hormone launch, and attachment circling back to gaze is important to establishing the mother�child bond. Gaze may also facilitate bonds between different individuals, including between individuals and their pet canine. Although these judgments might not all the time be warranted, they definitely stem from a fundamental reality that eye actions, as with facial expressions and posture, are an expression of self and mood. Most folks fixate primarily on the eyes and mouth of a face and decide, with high accuracy, the emotion expressed therein. Abnormal face-scanning patterns are associated with harm to the amygdala (see Chapter 7) and with psychiatric illnesses corresponding to schizophrenia and autism spectrum dysfunction. The resulting scanpaths map both points of fixation (dots) and saccades (lines) between factors of fixation. The scanpaths of control (A) and schizophrenic (B) people are shown as the subjects look at a neutral face (A1, B1), a happy face (A2, B2), and a tragic or somber face (A3, B3). As illustrated by these representative scanpaths, schizophrenic subjects spend far less time fixating on the eyes and mouth, the most emotionally salient features of a human face, than do management subjects. In distinction to management subjects who confirmed comparable scanpaths regardless of the goal expression (A1� A3), schizophrenic subjects adopted more normal scanpaths when looking at a sad face (B3) than at impartial (B1) or pleased (B2) faces. Associated with the different scanpaths, schizophrenic topics judged unhappy faces as accurately as did controls, but were worse at detecting neutral and pleased faces. C: Control youngsters, youngsters with autism spectrum dysfunction and impaired language growth (C1), and youngsters with autism spectrum disorder and regular language improvement (C2) had been shown a video of two younger girls in a restaurant speaking about whether or not to send again disgusting food. Control teenagers (not shown) and youngsters with autism spectrum disorder and language impairment fixated totally on the eyes of the 2 faces in the video. In distinction, youngsters with autism spectrum disorder and regular language expertise fixated on eyes far much less. Furthermore, the amount of time spent fixating on the mouth was immediately correlated and the amount of time fixating on the eyes not directly correlated to language expertise amongst subjects with autism spectrum dysfunction. Schizophrenia Res fifty five: 159�70, 2002, the place a full dialogue of these interesting results may be discovered, with permission of the writer, Elsevier. J Child Psychol Psychiatry 50: 834-42, 2009, where these intriguing outcomes are discussed totally, with permission from the writer, John Wiley & Son. Eye actions dictate our perceptual reality even when we gaze steadily at an object. Such visual fading happens in a very motionless person, a person with none head or eye movements. Small eye actions, less than a level in dimension, called microsaccades, circumvent this drawback and forestall images from fading. During fixation, we unconsciously make one to two microsaccades every second, and this is sufficient to prevent visual fading. Thus, though nonetheless pictures disappear, small eye movements are enough to restore image perception, thus offering a transparent demonstration of the significance of adjustments in luminance across time and space as the important stimuli for vision (see Chapter 15). Eye actions are straightforward to elicit even in young youngsters and may be quantitatively measured. Consequently, attention has targeted just lately on using eye movement abnormalities as diagnostic instruments for schizophrenia and other developmental psychiatric problems. One hope is that eye motion abnormalities can serve as biomarkers of psychiatric illness, permitting for early detection, diagnosis, and the evaluation of potential therapeutic interventions. Another risk exists, which is that eye motion abnormalities may contribute to the pathophysiology of psychiatric illness. The patient with bilateral amygdala harm described in Chapter 7 supports this idea. When she looked at the eyes, she performed usually in detecting fearful expressions. Determining the extent to which irregular eye movements trigger psychiatric dysfunction, past simply serving as potential biomarkers of disease, stays an intriguing question for the future. Yet head and eye place are unequal companions because eye actions contribute greater than do head movements to gaze shifts, small and enormous alike. Saccades, fast ballistic eye actions, are faster and require much less preparatory time than probably the most rapid head movements. Since gaze stabilization and gaze shifts depend principally on eye actions, we focus our examination of gaze control on the oculomotor system, the pathways concerned in controlling extraocular muscular tissues.
Priligy: 90 mg, 60 mg, 30 mg
Purchase 90mg priligyIf taping is happening for publication purposes impotence at 70 purchase 60 mg priligy visa, the videographer ought to attempt to importance of being earnest generic priligy 60mg visa seize a complete protocol so as to erectile dysfunction treatment san diego buy priligy 90mg have all the salient options gonorrhea causes erectile dysfunction 30mg priligy for sale, within the occasion further video is requested from a reviewer at a later level. In circumstances where a affected person has poor mobility and has limited bodily independence, a second individual should be obtainable if the videographer needs assistance. In many situations, the affected person may be examined and videotaped without the presence of members of the family. However, in certain instances, a family member may have perception into how a particular movement is elicited. Some sufferers might have the help of the member of the family during taping, significantly in patients with dementia who might benefit from the presence of a familiar face. However, no more than one family member ought to be current during the taping, as it might influence the quality of the final video. Also the patient must be asked the setting by which the motion is most outstanding. While particular sections of the protocol are being taped, the videographer must additionally concentrate on movements that might be occurring elsewhere. Ultimately, time and expertise are needed to make a clean transition between videography and the medical appointment and to maintain the move of the workday. Some sufferers might need to be videorecorded under suboptimal circumstances, corresponding to within the emergency room, intensive care unit, or while having an acute event in an examination room. In such instances, the videographer should try to videotape the elements of the physique concerned as very best while positioning the affected person safely. In this case, mobile phone or smartphone cameras (now fairly ubiquitous in public use) can be utilized to film the episodes at house. The episodes can then be reviewed at future visits or, more ideally, mailed securely to the doctor for review and storage. It should be explained that the movies are for academic purposes, in addition to for review of the prognosis. Consent for the taping should be obtained presently, and ideally sufferers are knowledgeable forward of their visit that this might be mentioned, as this makes it extra likely for them to give consent to be videotaped. The protocol for each movement disorder should be adopted as intently as possible. Teaching tape for the motor section of the toronto western spasmodic torticollis scale. Methods for digital video recording, storage, and communication of movement issues. Prevalence and indications for video recording in the well being care setting in North American and British paediatric hospitals. Index Indexer: Dr Laurence Errington Note: Vs signifies the differential prognosis of two or extra conditions. Tourette syndrome) 36, 37 dysarthria in cerebellar disorders 70, seventy three dyskinesia 186 stomach dancer 123 medical score scales 186 levodopa 44, ninety four orofacial/limb, acute 152 paroxysmal 112, 114�18 tardive 94, 97, 133, 134 dysphonia, spasmodic (laryngeal dystonia) sixty three, 155�6 dystonia three, 57�65, 163�4, 173, one hundred eighty, 186 acute onset one hundred twenty, 152 vs neuroleptic malignant syndrome 153 classification 57�63 scientific score scales 186 frequent syndromes 62�3 definition fifty seven differential prognosis 61, sixty three, 67 myoclonus 26 tics 38 analysis 63�4 focal fifty seven, fifty nine, 62, sixty three, sixty five, 66, ninety two, 95, 186 functional one hundred twenty, 163�4 generalized 57, fifty nine, 62, sixty five, 155, 186 frequent and severe episodes (dystonicus status) a hundred and fifty five genetics 61, 63�4, 173 imaging a hundred and eighty laryngeal 63, 155�6 myoclonus and 63 oromandibular 63, 94 segmental fifty nine, sixty two, 63, 64, 65, ninety two, 180 tardive 134�5 tremor and 24�5, fifty eight, 67 dystoniaplus and dystoniaplus syndromes fifty eight, 60 training (patient/family), tic issues incl. Xlinked recessive) inheritance ataxias 74�6 dystonias 61 McLeod syndrome 143, 173 Yale Global Tic Severity Scale 188 zinc one hundred forty. Mild recurrent stomach pain is a much less pressing drawback and may be assessed in an hour or two when you have other sufferers with larger precedence problems. Perforated or ruptured viscus Ascending cholangitis o Necrosis of a viscus o Exsanguinating hemorrhage A perforated or ruptured viscus might result in hypovolemic shock (from third-space losses), septic shock (from bacterial peritonitis), or both. Necrosis of a viscus, as in extreme pancreatitis, intussusception, volvulus, strangulated hernia, or ischemic colitis, might trigger hypovolemic or septic shock and electrolyte and acid-base disturbances. Exsanguinating hemorrhage with hypovolemic shock could result from a leaking belly aortic aneurysm, a ruptured ectopic being pregnant, or a splenic rupture; the cause is occasionally iatrogenic, similar to a liver or renal biopsy or a misdirected thoracentesis. Patients with myocardial infarction and aortic dissection sometimes present with stomach pain. These cardiovascular diagnoses must be considered, especially if no native belly indicators can be identified. Patient-Related Problems: the Common calls Appearances are often misleading in acuk belly illness. If the affected person 1w recently received narcotic analgesics or high-dose steroid~, he or she might seem well despite a critical underlying downside. Patients with extreme colic are sometimes restless; these with peritonitis, in contrast. With peritonitis, sufferers could have their knees drawn up to cut back abdominal pressure. Hypotension related wi1:h stomach pain is an ominous sign suggestive of impending hypovolemic, hemorrhagic, or septic shock. Abdominal Pain Does the patient have postural adjustments (lying and standing) within the blood stress and coronary heart price If the supine blood pressure is regular, recheck the blood pressure and coronary heart rate with the affected person standing. Fever associated with belly ache is suggestive of intraabdominal an infection or irritation. Selective History and Chart Review Diagnosis is often depending on a careful history that addresses the following points: 1. Remember that a affected person could complain of diffuse belly ache, but on careful examination, the pain may be found to be localized. Right decrease quadrant: A, appendix (appendicitis,* abscess); 0, ovary (torsion, ruptured cyst. Generalized stomach ache: (1 See situations marked with an asterisk(*, (2 peritonitis (any cause), (3) diabetic ketoacidosis, (4 sickle cell crisis, (5) acute intermittent porphyria, and (6) acute adrenocortical insufficiency ensuing from steroid withdrawal. Patient-Related Problems: the Common Calls Does the patient characterize the pain as severe or mild, burning or knifelike, or fixed or waxing-and-waning, as in colic The pain of a peptic ulcer tends to be burning, whereas that of a perforated ulcer is sudden, fixed, and extreme. An acute onset with fainting is suggestive of perforation of a viscus, ruptured ectopic being pregnant, torsion of an ovarian cyst, or a leaking abdominal aortic aneurysm. A ruptured viscus may be initially associated with localized ache that subsequently shifts or becomes generalized, with the event of chemical or bacterial peritonitis. Thus, in biliary colic, ache is regularly referred to the inferior angle of the right scapula. Pain that will increase with meals, decreases with passage of bowel movements, or does both is suggestive of a hole gut origin. An exception is ache from a duodenal ulcer, which is commonly relieved by the ingestion of meals. The ache of pancreatitis is commonly worse after consuming and could also be relieved by sitting up or leaning forward. Vomiting that happens with the onset of pain frequently accompanies both acute peritoneal irritation and perforation of a viscus.
Trusted 60mg priligyTactile data arising from the legs travels medially in the fasciculus gracilis (fg) and that from the arms travels more laterally within the fasciculus cuneatus (fc) erectile dysfunction doctor dubai discount priligy 90 mg without prescription. The lateral funiculus accommodates the lateral corticospinal tract (lcst) dorsally and the spinothalamic tract (stt) ventrally problems with erectile dysfunction drugs cheap priligy 30mg with visa. The ventral funiculus contains tracts primarily related to axial motor perform erectile dysfunction by age statistics generic 90mg priligy overnight delivery, such as the ventral corticospinal tract (vcst) erectile dysfunction epocrates generic 30 mg priligy amex. The intermediate gray incorporates preganglionic autonomic neurons however solely in two areas: � T1�L2 segments contain sympathetic preganglionic neurons; � S2�S4 segments include parasympathetic preganglionic neurons. The intermediate horn provides an simply recognizable marker for thoracic segments. Additional preganglionic sympathetic neurons are discovered extra medially, close to the central canal, in an area known of because the intermediomedial cell column. Preganglionic parasympathetic neurons ship their axons out the ventral roots to parasympathetic ganglia typically situated in or very close to the ultimate goal organ. Lumbar sections, L2 is shown right here, are roundish in form, have a large dorsal horn, a lateral ventral horn, and comparatively little white matter. The sacral section proven here, S3, is probably the most caudal a part of the lumbosacral enlargement. It is nearly square in form, has a big dorsal horn, a bulging intermediate gray space, a lateral ventral horn, and almost no white matter. The cervical wire has the greatest proportion of white matter and the lumbosacral cord the least. Segments from the lumbosacral and cervical enlargements, however not from thoracic wire, comprise a lateral ventral horn, reflective of motoneurons that innervate muscles within the distal limb. Photographs reprinted and sections modified with permission from deArmond S et al. The spinal white matter that surrounds the spinal grey on all sides is divided up into anatomical chimneys known as funiculi (singular form is funiculus). The dorsal portion of the lateral funiculus is usually termed dorsolateral, and the ventral portion termed ventrolateral. All long-distance connections between the spinal wire and mind or between spinal segments travel in the funiculi surrounding the spinal gray. The dorsal and ventral horns inside the lumbar and cervical enlargements dwarf these of the thoracic twine. This follows naturally from the far higher sensory innervation density and the higher variety of muscle tissue in the palms and feet relative to the thorax and abdomen. Corresponding to the higher sensory density in the palms and ft, the dorsal horn in the cervical and lumbosacral enlargments is extensive, whereas that within the thoracic twine, where sensory function is most rudimentary, is far smaller. Within the ventral horn, motoneurons that management axial or trunk musculature are situated close to the midline. Thus, thoracic segments contain a slim ventral horn, situated close to the midline, which accommodates motoneurons innervating axial muscles exclusively. The relative amount of white and grey matter also adjustments throughout the segments of the spinal wire. Since all motor tracts descend into the spinal cord from the mind and all sensory tracts ascend from the spinal twine to the mind, the best amount of white matter is situated most rostrally, in cervical segments. The least quantity of white matter is present within the sacral twine and the coccygeal section. Because of the sensory and motor complexity of the limbs, notably the arms, relative to the trunk, the most important space of gray matter is found in the cervical enlargement and the smallest gray space is discovered within the thoracic twine. Sections from the cervical enlargement have an elongated oblong form, thoracic sections seem nearly diamond-shaped, and lumbar sections appear squat and roundish in shape. Sacral sections are almost sq. in form and are instantly recognizable for having nearly no white matter. The marginal zone incorporates many of the neurons critical to the perception of pain and temperature, and these project from the spinal twine to the brain. The substantia gelatinosa is house to interneurons involved within the processing of somatosensory info, especially that resulting from noxious and thermal stimulation. Deep to the superficial dorsal horn, the nucleus proprius processes mild touch information. Finally, the deep dorsal horn serves heterogeneous purposes including processing ache, temperature, and viscerosensory input. Within the ventral horn there are swimming pools of motoneurons containing motoneurons innervating a single muscle. Pools are rostrocaudally oriented and cylindrically shaped neuronal collections that cross spinal segmental boundaries. Motor interneurons fill the ventral horn within the space surrounding the motoneuron swimming pools. In addition to the intermediomedial and intermediolateral cell columns that contain autonomic preganglionic neurons, the intermediate gray incorporates numerous interneurons with necessary roles in remodeling sensory input into skeletal motor output. Axons from dorsal root ganglion cells that respond to mild touch, vibration, and proprioception travel through the dorsal roots and enter the ipsilateral dorsal funiculus, or dorsal column, to travel rostrally. Therefore, on the degree of the cervical twine, axons from essentially the most caudal sacral ganglia, carrying input from the perineum, are located most medially within the ipsilateral dorsal column. This is as a outcome of axons of progressively rostral dorsal root ganglia, carrying input from the legs, trunks, and arms, take up positions progressively increasingly more lateral to that of the afferents from the perineum. Since afferent input always joins the dorsal columns from the lateral aspect, legs are represented most medially and arms most laterally. B: Dorsal root ganglion cells that code for pain and temperature send their central process into the dorsal horn to the marginal zone. Cells in the marginal zone send an axon across the midline within the ventral spinal commissure to the contralateral spinothalamic tract, positioned within the ventrolateral funiculus. C: Corticospinal tract axons that control fine voluntary movements travel in the dorsolateral funiculus because the lateral corticospinal tract. Lateral corticospinal axons depart the dorsolateral funiculus and contact motoneurons within the ventral horn of the cervical and lumbosacral enlargements. Together, the fasciculus gracilis and the fasciculus cuneatus comprise a dorsal column. In sum, each dorsal column carries details about light touch, vibration, and proprioception from the ipsilateral body. Spinothalamic cells situated in the marginal zone carry ache and temperature info across the midline by way of the ventral spinal commissure, just ventral of the central canal gray. Spinothalamic axons journey rostrally throughout the spinothalamic tract of the ventrolateral funiculus to reach the thalamus. In sum, each ventrolateral funiculus contains information about pain and temperature from the contralateral side of the body.
References - World Health Organization Europe. Prevalence of asthma and allergies in children. European Environment and Health Information System (ENHIS) Fact sheet no. 3.
- Twomey, L. T., & Taylor, J. R. (1985). Age changes in lumbar intervertebral discs. Acta Orthopaedica Scandinavica, 56, 496n499.
- Dolan LM, Walsh D, Hamilton S, et al: A study of quality of life in primigravidae with urinary incontinence, Int Urogynecol J Pelvic Floor Dysfunct 15:160n164, 2004.
- Gupta A, Raman JD, Leveillee RJ, et al: General anesthesia and contrastenhanced computed tomography to optimize renal percutaneous radiofrequency ablation: multi-institutional intermediate-term results, J Endourol 23:1099n1105, 2009.
- Etz CD, Halstead JC, Spielvogel D, et al: Thoracic and thoracoabdominal aneurysm repair: Is reimplantation of spinal cord arteries a waste of time? Ann Thorac Surg 82:1670, 2006.
- Otto CM. Valvular aortic stenosis: disease severity and timing of intervention. J Am Coll Cardiol 2006; 47:2141-2151.
|

