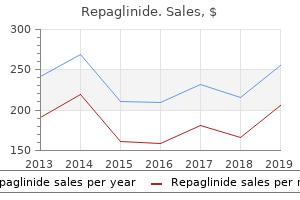
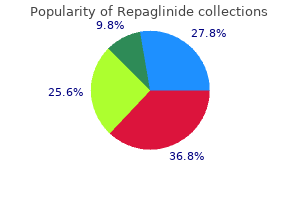
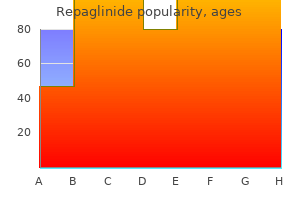
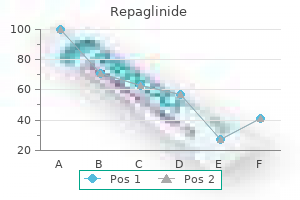
Repaglinide
Marc E. Stone, MD - Associate Professor of Anesthesiology
- Program Director, Fellowship in Cardiothoracic Anesthesiology
- Mount Sinai School of Medicine
- New York, New York
Purchase repaglinide 2mg overnight deliveryThis urine quantity is necessary in avoiding spikes in extracellular fluid volume glucose blood quant buy discount repaglinide 2 mg online, as nicely as for related elimination of phosphorus metabolic disease hyperparathyroidism purchase repaglinide 1mg otc, larger weight center molecules diabetes insipidus blood test buy repaglinide 2mg with mastercard, and protein-bound uremic toxins diabetes test machine india discount 0.5mg repaglinide with mastercard. It could also be that the loss of residual kidney operate in such circumstances is an unavoidable worth that must be paid. Intradialysis and end-dialysis hypertension can happen in about 15% of dialysis patients and have been related to the next death danger (Inrig, 2009). Sympathetic and renin�angiotensin overactivity in addition to endothelial dysfunction even have been linked to this situation. If hypertension recurs in a affected person after being nicely controlled by quantity subtraction, the most probably explanation is that the affected person has returned to a state of volume excess. The imply variety of antihypertensive medication prescribed for incident hemodialysis and peritoneal dialysis patients is 2. Prescription patterns of these drugs vary by dialysis modality, and substantial changes in prescription patterns of betablockers, renin�angiotensin system antagonists, and calcium channel blockers occur from the sixth month on. Furthermore, prescription classes differ by comorbidity, race/ethnicity, and age, however little by intercourse (St Peter, 2013). The incontrovertible fact that serum plasma renin exercise is overtly high in some dialysis patients and inadequately suppressed in volume-expanded patients offers a pathophysiologic rationale for use of these drugs. Other unwanted facet effects are cough, skin rash, alteration of style, and, hardly ever, agranulocytosis or angioedema. Many show a documented cardioprotective impact within the setting of myocardial ischemia or infarction. Carvedilol, an alpha/beta-blocker, reduces morbidity and mortality in dialysis patients with systolic dysfunction (Cice, 2003). Importantly, the chance of major cardiovascular events was halved in the atenolol group as in contrast with the lisinopril group, to the point that the protection monitoring board for the research recommended early termination of the trial. Prazosin has been related to first-dose syncope, so the first dose have to be administered at bedtime. Beta-adrenergic blockers have a excessive incidence of unwanted effects, corresponding to drowsiness, lethargy, and depression. Non-selective beta-blockers need to be used cautiously in sufferers with an inclination toward pulmonary edema or bronchial asthma and in patients already being treated with some calcium channel blockers. Beta-blockers have an antagonistic impact on serum lipids; they might also have an antagonistic effect on cell potassium uptake, tending to increase the serum potassium level. They can masks the signs of hypoglycemia and augment insulin-induced hypoglycemia. All might cause bradycardia and interfere with reflex tachycardia following quantity depletion. Water-soluble beta-blockers atenolol, nadolol, and bisprolol are removed substantially by hemodialysis and must be preferentially administered postdialysis. These drugs are frequently used for the therapy of volume-resistant hypertension in dialysis sufferers. Calcium channel blockers should be used very cautiously in combination with beta-adrenergic blockers, as a outcome of congestive heart failure can be precipitated. Other unwanted effects are ankle edema, headache, flushing, palpitations, and hypotension. Calcium channel blockers are excreted primarily by the liver, their pharmacokinetic profile is unaltered in chronic renal failure and by dialysis (Table 33. As famous above, there seems to be increased tonic sympathetic activity in dialysis sufferers, so use of central sympatholytic medicine, which inhibit sympathetic outflow by stimulating alpha-adrenoreceptors in the mind stem, is theoretically engaging. One facet good thing about clonidine is its usefulness in the therapy of diarrhea due to autonomic neuropathy. Moreover, methyldopa and clonidine are relatively inexpensive-often an necessary consideration. Moxonidine added to other antihypertensive medicine was nicely tolerated in one examine of patients with superior renal failure, and was corresponding to nitrendipine by method of efficacy (Vonend, 2003). A low, nonhypotensive dose of this drug produces a sustained reduction in directly recorded sympathetic exercise in dialysis sufferers (Hausberg, 2010). For clonidine these include sedation, dry mouth, depression, and postural hypotension. Guanabenz and guanfacine are much less prone to trigger rebound hypertension however are costlier. No No No No No Yesa Yesa Yesa Yesa Yesa Yesa No Yesa Yesa Yesa Yesa Yesa Yesa Yesa Yesa Yesa zero. None of the drugs in the table undergoes substantial elimination throughout continuous ambulatory peritoneal dialysis. The use of this drug in dialysis patients with heart failure is therefore unwarranted. Methyldopa could trigger hepatotoxicity or a positive direct or oblique Coombs check, interfering with cross-matching of blood. Methyldopa, clonidine, and guanfacine are excreted substantially by the kidneys, and dosage reductions may be required. Guanabenz is metabolized by the liver and requires no dosage adjustment in renal failure. They usually require addition of a sympatholytic or beta-blocking drug because they have a tendency to trigger reflex tachycardia. Side effects of each medicine relate primarily to this reflex tachycardia and ensuing palpitations, Chapter 33 / Hypertension 589 dizziness, and worsening of angina pectoris. Hydralazine is efficient and inexpensive, but could cause a lupus-like syndrome at dosages of greater than 200 mg per day. Because of diminished renal excretion of its energetic metabolite(s), the utmost allowable dosage should be reduced in dialysis patients. Minoxidil has been associated with pericarditis and is mostly prevented in ladies due to hypertrichosis. The short-acting formulation of nifedipine was used as a first-line drug for severe hypertension prior to now, however is now not recommended, as there at the second are numerous reviews documenting myocardial, cerebral, and retinal ischemia after its use. The long-acting preparation of nifedipine or other long-acting calcium antagonist, or clonidine, should be used as an alternative as first-line remedy. Hypertensive emergencies are outlined as increases in arterial strain that, if sustained for a few hours, would trigger irreversible organ damage. Hypertensive encephalopathy, hypertensive left ventricular failure, hypertension related to unstable angina/myocardial infarction, hypertension with aortic dissection, and cerebral hemorrhage/brain infarction are such emergencies. The signs of thiocyanate toxicity are nausea, vomiting, myoclonic movements, and seizures. Hydralazine 10�20 mg given slowly intravenously is a well-tried alternative, but this drug must be avoided in ischemic heart disease. The controversies of diagnosing and treating hypertension amongst hemodialysis patients.
Repaglinide 2mg with mastercardScattered lymphocytes and plasma cells are seen inside the lamina propria and there are often focal nodular collections of small lymphocytes blood glucose 550 buy repaglinide 2 mg line. These collections frequently include a mix of B- and T-cells and may be primarily based on follicular dendritic cell networks diabetes type 2 for dummies repaglinide 0.5 mg online. In most instances diabetes type 2 powerpoint generic 1mg repaglinide with amex, the appearances are inadequate for a prognosis of residual lymphoma diabetes signs mayo buy 2mg repaglinide with amex. Some, however no all of those will eventually present molecular regression but there may be a prolonged time lag between histological and molecular regression 1677. In the absence of histological evidence of residual lymphoma, the scientific significance of a persistent clonal inhabitants stays unsure. Eventually, these areas turn out to be confluent to form sheets of cells indistinguishable from the cells of a diffuse giant B-cell lymphoma. In circumstances with each low- and high-grade parts, genetic studies have con- 60 Tumours of the abdomen firmed the transformation of low-grade to high-grade lymphoma within the majority of circumstances 1263 while in different instances each parts seem clonally unrelated, suggesting the event of a second major lymphoma 1184, 1491. Mantle cell lymphoma Mantle cell lymphoma of the abdomen is often a element of multiple lymphomatous polyposis of the gastrointestinal tract and sometimes encountered outdoors this clinical context 1380. However, this translocation seems to be much less widespread in high-grade lesions 1435, 95. Trisomy three has been detected in as much as 60% of instances in some studies utilizing each metaphase and interphase methods 2134, 2137, however this discovering has not been confirmed by other studies 1434. The translocation t(1;14) (p22; q32) has additionally been described in a small proportion of cases 2138 and this is related to elevated survival of tumour cells in unstimulated cell tradition. Study of the third complementary determining area of the immunoglobulin heavy chain gene reveals a pattern of adjustments associated with the generation of antibody variety and increased antigen binding affinity 131. Bcl-6 protein has also been described in high-grade lymphomas whereas being absent from lowgrade lesions 1425. In these regions, T-cell lymphoma may characterize as much as 7% of gastric lymphomas 1741. It has lately been demonstrated that some gastric T-cell lymphomas show features of intraepithelial T lymphocyte differentiation. Hodgkin disease Hodgkin illness could contain the gastrointestinal tract but that is usually secondary to nodal disease. The time taken to obtain remission in these sufferers varies from 4-6 weeks to 18 months. The stability of those remissions remains to be decided; one research has reported a relapse in 10% of patients after a imply follow-up interval of 24 months 1338 while others have discovered sustained remissions for as much as six years 801. Involvement of the resection margins and advanced stage are poor prognostic options, however not with the addition of chemotherapy 1262. Irrespective of therapy modality, the only vital unbiased prognostic variables are stage and tumour-grade 260, 1653, 1262, 320, 383. Other low-grade B-cell lymphomas Although the lymphoid tissue in the stomach accommodates all of the B-cell populations encountered in nodal lymphoid tissue, other low-grade B-cell lymphomas, corresponding to follicle centre cell lymphomas, are very rare and often indistinguishable from their nodal counterparts. Diffuse massive B-cell lymphoma these lymphomas are morphologically indistinguishable from diffuse giant B-cell lymphomas that come up within lymph nodes. There is complete destruction of the gastric glandular structure by massive cells with vesicular nuclei and prominent nucleoli. Burkitt lymphoma Although uncommon, classical Burkitt lymphomas may be encountered within the abdomen fifty five. The morphology is equivalent to that of Burkitt lymphoma encountered elsewhere, with diffuse sheets of medium sized cells with scanty cytoplasm and round/oval nuclei containing small nucleoli. These tumours encompass most gastric and intestinal mesenchymal tumours earlier designated as leiomyoma, cellular leiomyoma, leiomyoblastoma and leiomyosarcoma 80, seventy six, seventy eight, seventy nine, 1227. Currently, the terms leiomyoma and leiomyosarcoma are reserved for these tumours that show easy muscle differentiation, histologically or by immunohistochemistry. The ratio of the age-adjusted incidence rates for Blacks and Whites is bigger for sarcomas (3 to 1) than for carcinomas (2 to 1). They are most common within the abdomen (60-70%), followed by small intestine (20-30%), colorectum and oesophagus (together < 10%) 1227. The bigger tumours protrude intraluminally or to the serosal facet, and will have a massive extragastric part that masks the gastric origin. Intraluminal tumours are often lined by intact mucosa, but ulcera- tion happens in 20-30% of instances. Larger tumours could endure huge haemorrhagic necrosis and cyst formation leaving solely a slim rim of peripheral viable tissue; malignant tumours could form complicated cystic masses. Tumours with moderate cellularity and focal nuclear palisading can resemble nerve sheath tumours. Histological assessment of malignancy is essentially based on mitotic counts and dimension of the lesion. However, large tumours (especially over 10 cm) with no detected mitotic exercise might develop late recurrences and even metastases. Mitotic activity is the primary criterion, namely these tumours with over 10 mitoses per 10 hpf are thought of highgrade. These c-kit mutations have been proven to characterize gain-of-function mutations leading to ligand-independent activation (autophos- A B C. C An epithelioid sample comparable to the earlier designation of leiomyoblastoma. The most common mutations appear to be in-frame deletions of 3-21 base pairs, adopted by point mutations and occasionally described insertions 475, 713, 1018, 1289. Leiomyomas are composed of bland spindle cells showing low or reasonable cellularity and slight if any mitotic exercise. Leiomyosarcomas are tumours that present histologically and immunohistochemically evident clean muscle differentiation. Tumours with mitotic counts exceeding 10 mitoses per 10 excessive power fields are classed as highgrade. Glomus tumours Lesions similar to glomus tumours of peripheral delicate tissue happen predominant- ly within the gastric antrum as small intramural masses (1-4 cm in diameter, common 2 cm). One-third manifests as ulcer, one-third as bleeding, and one-third is asymptomatic. The tumour cells have small, uniform nuclei and mitotic exercise is virtually absent. Multiple glomus tumours with apparent intravascular spread have been described 666. Granular cell tumour Lesions much like these in peripheral soft tissues are sometimes encountered within the abdomen, the place they principally occur as small submucous nodules and fewer generally as intramural or subserous lots. These lesions occur predominantly in middle age, and present a powerful predilection for Blacks. Schwannomas these lesions are rare in the gastrointestinal tract, but the abdomen is their most typical website inside the digestive system. Schwannomas are usually covered by intact mucosa and principally contain the muscularis propria. Histologically, gastrointestinal schwannomas often show a spindle cell pattern like mobile schwannoma with vague nuclear palisading.
Diseases - Occult spinal dysraphism
- Tuberculous meningitis
- Kantaputra Gorlin syndrome
- Fetal hydantoin syndrome
- Free sialic acid storage disease
- Mucolipidosis type 3
- Hypercalcemia, familial benign type 3
- Acropectoral syndrome
Cheap 2mg repaglinide with mastercardFibrolamellar carcinoma of the liver: a tumor of adolescents and young adults with distinctive clinicopathologic features diabetes mellitus type 2 cpg malaysia order 0.5 mg repaglinide otc. Precursor lesions of oesophageal cancer in a low-risk inhabitants in China: comparison with high-risk populations diabetes type 2 how to cure cheap repaglinide 0.5 mg on-line. Status of c-myc blood sugar optimizer complaints buy generic repaglinide 0.5mg online, p53 and retinoblastoma genes in human papillomavirus positive and unfavorable squamous cell carcinomas of the anus diabetes mellitus type 2 genes repaglinide 2 mg on-line. Clonal p53 mutation in major cervical cancer: association with human-papillomavirusnegative tumours. Morphological lesions related to human primary invasive nonendocrine pancreas most cancers. Loss of heterozygosity in 11q13-14 areas in gastric neuroendocrine tumors not related to multiple endocrine neoplasia sort 1 syndrome. Benign schwannoma of the gastrointestinal tract: a clinicopathologic and immunohistochemical examine. Carcinoma of the extrahepatic biliary tract: a clinicopathological and immunohistochemical examine. Granzyme B-expressing peripheral T-cell lymphomas: neoplastic equivalents of activated cytotoxic T cells with choice for mucosa-associated lymphoid tissue localization. Clinical relevance of remodeling development factor alpha, epidermal progress factor receptor, p53, and Ki67 in colorectal liver metastases and corresponding major tumors. Somatic mutations of the beta-catenin gene are frequent in mouse and human hepatocellular carcinomas. Low prevalence of monoclonal B cells in Helicobacter pylori gastritis patients with duodenal ulcer. De Vita S, Sacco C, Sansonno D, Gloghini A, Dammacco F, Crovatto M, Santini G, Dolcetti R, Boiocchi M, Carbone A, Zagonel V (1997). Characterization of overt B-cell lymphomas in patients with hepatitis C virus an infection. Allelic deletions on chromosome 11q13 in a quantity of endocrine neoplasia type 1-associated and sporadic gastrinomas and pancreatic endocrine tumors. Hepatitis C virus antibodies and liver disease in sufferers with porphyria cutanea tarda. Outcome of lymph node involvement in sufferers with the Zollinger-Ellison syndrome. Pseudocystic liver metastases in patients with carcinoid tumors: report of three circumstances. Primary liver most cancers in genetic hemochromatosis: a clinical, pathological, and pathogenetic examine of fifty four instances. Trisomy three in marginal zone B-cell lymphoma: a research primarily based on cytogenetic evaluation and fluorescence in situ hybridization. Detection of monoclonality in low-grade B-cell lymphomas utilizing the polymerase chain response depends on primer selection and lymphoma type. Goseki grading in gastric most cancers: comparability with current methods of grading and its reproducibility. Doki Y, Shiozaki H, Tahara H, Kobayashi K, Miyata M, Oka H, Iihara K, Mori T (1993). Dolcetti R, Viel A, Doglioni C, Russo A, Guidoboni M, Capozzi E, Vecchiato N, Macri S, Fornasarig M, Boiocchi M (1999). High prevalence of activated intraepithelial cytotoxic T lymphocytes and increased neoplastic cell apoptosis in colorectal carcinomas with microsatellite instability. Hepatitis B and C virus infection, alcohol ingesting, and hepatocellular carcinoma: a case-control research in Italy. Site, measurement, multicentricity, association with a quantity of endocrine neoplasia kind 1, and malignancy. Congenital pancreatoblastoma in BeckwithWiedemann syndrome: an rising affiliation. The accumulation of p53 abnormalities is associated with development of mucosa-associated lymphoid tissue lymphoma. Pregnancy complicated by solid-papillary epithelial tumor of the pancreas, pulmonary embolism, and pulmonary embolectomy. Squamous carcinoma of the oesophagus: histological criteria and their prognostic significance. Serous oligocystic and ill-demarcated adenoma of the pancreas: a variant of serous cystic adenoma. Survival and causes of death in patients with inflammatory bowel disease: a population-based research. Consistent genetic alterations in xenografts of proximal stomach and gastro-esophageal junction adenocarcinomas. Metastatic breast carcinoma involving the gastric antrum and duodenum: computed tomography appearances. Tylosis associated with carcinoma of the oesophagus and oral leukoplakia in a large Liverpool family - a evaluation of six generations. Hepatitis B virus X protein and p53 tumor suppressor interactions within the modulation of apoptosis. Emi M, Fujiwara Y, Nakajima T, Tsuchiya E, Tsuda H, Hirohashi S, Maeda Y, Tsuruta K, Miyaki M, Nakamura Y (1992). Frequent loss of heterozygosity for loci on chromosome 8p in hepatocellular carcinoma, colorectal cancer, and lung most cancers. Emi M, Fujiwara Y, Ohata H, Tsuda H, Hirohashi S, Koike M, Miyaki M, Monden M, Nakamura Y (1993). Well-differentiated adenocarcinoma mimicking complete-type intestinal metaplasia within the stomach. Cowden syndrome and Lhermitte-Duclos disease in a family: a single genetic syndrome with pleiotropy Alpha-smooth muscle actin-positive perisinusoidal stromal cells in human hepatocellular carcinoma. Subclassification of gastrointestinal stromal tumors based mostly on analysis by electron microscopy and immunohistochemistry. Eskelinen M, Lipponen P, Marin S, Haapasalo H, Makinen K, Ahtola H, Puittinen J, Nuutinen P, Alhava E (1991). Espinosa A, Berga C, Martin P, V, Sanchez V, Diaz J, Segura J, Escuder J, Barbod A (1998). Familial pancreatic adenocarcinoma: affiliation with diabetes and early molecular analysis. Occult dysplasia is disclosed by Lugol chromoendoscopy in alcoholics at high risk for squamous cell carcinoma of the esophagus. Hepatosplenic T-cell lymphoma: sinusal/sinusoidal localization of malignant cells expressing the Tcell receptor gammadelta. Survival and prognostic components in 212 Italian sufferers with genetic hemochromatosis. Surgical pathology of the anal canal: a review of the latest literature on the anatomy and pathology. Intestinal metaplasia types and the danger of gastric cancer: a cohort research in Slovenia. Glucagon, glicentin and pancreatic polypeptide-like immunoreactivities in rectal carcinoids and associated colorectal cells.
Discount repaglinide 1 mg onlineHepatic artery ligation or transarterial embolization are different therapeutic modalities treatment diabetes lady finger buy repaglinide 0.5 mg visa. There are occasional reports of transformation of childish haemangioendothelioma to angiosarcoma 1708 blood glucose without blood cheap 1 mg repaglinide. Cavernous haemangioma this is the most incessantly occurring benign tumour of the liver diabetes test miami buy discount repaglinide 0.5 mg. It is extra frequent in females diabetes type 1 death rate repaglinide 2mg fast delivery, and occurs at all ages however is least common in the paediatric age group. It is thought to increase in size and even rupture throughout being pregnant, and in addition might enlarge or recur in patients on oestrogen therapy. When sectioned they partially collapse as a outcome of the escape of blood and have a spongy appearance. Lesions are sometimes composed of blood-filled vascular channels of various size lined by a single layer of flat endothelial cells supported by fibrous tissue. Thrombi in numerous phases of organization with areas of infarction may be current, and older lesions show dense fibrosis and calcification. In sclerosed haemangiomas, most or all the vessels are occluded and typically are only demonstrable by stains for elastic tissue. Angiomyolipoma the lesion is defined as a benign tumour composed of variable admixtures of adipose tissue, smooth muscle (spindled or epithelioid), and thick-walled blood vessels. The age range of angiomyolipoma is from 30-72 years, with a mean of 50 years 1373. Angiomyolipomas are often single, with 60% located in the best lobe, 30% in the left lobe, 20% in each lobes and 8% in the caudate lobe 1373. They are sharply demarcated however not encapsulated, fleshy or firm and, when sectioned, with a homogeneous yellow, yellow-tan or tan appearance, depending on their content of fat. Angiomyolipomas are composed of adipose tissue, smooth muscle and thick-walled, typically hyalinized blood vessels in varying proportions. The microscopic appearances are extensively varied and will imitate a quantity of malignant tumours. A attribute feature of angiomyolipoma is the presence of extramedullary haematopoiesis. Mesenchymal tumours 193 Solitary fibrous tumour Solitary fibrous tumour has an age range from 32-83 years (mean, fifty seven years) 1270. Solitary fibrous tumour usually reveals alternating cellular and relatively acellular areas. The cellular areas encompass bundles of spindle cells arranged haphazardly or in a storiform sample. In some instances the cells are organized round ectatic vessels in a haemangiopericytoma-like sample. Nuclei of the spindle cells are uniform and lack pleomorphism, however these tumours could bear malignant change as evidenced by the presence of foci of necrosis, prominent mobile atypia, and mitotic activity in the range of 2-4 mitoses/10 hpf 1270, 514. The relatively acellular areas of solitary fibrous tumour contain ample collagen bundles with thin, stretched-out tumour cells. Inflammatory pseudotumour this lesion is outlined as a benign, nonneoplastic, non-metastasizing mass composed of fibrous tissue and proliferated myofibroblasts, with a marked inflammatory infiltration, predominantly plasma cells 318. Inflammatory pseudotumours are solitary (81%) or less usually a number of (19%) 1275 and often intrahepatic, however some can involve the hepatic hilum. They vary in measurement from 1 cm to massive masses involving a complete lobe, and are agency, tan, yellow-white or white. Some inflammatory pseudotumours are probably the residuum of a resolved bacterial abscess, while others could additionally be associated to Epstein-Barr virus an infection eighty two, 318. They are composed of inflammatory cells in a stroma of interlacing bundles of myofibro- blasts, fibroblasts, and collagen bundles. The majority of inflammatory cells are mature plasma cells, however lymphocytes (and occasional lymphoid aggregates or follicles), in addition to eosinophils and neutrophils, may be present. Macrophages, typically showing xanthomatous modifications, occasional granulomas and, rarely, phlebitis involving portal vein branches or outflow veins, may be seen. Lymphangioma and lymphangiomatosis Lymphangioma is a benign tumour characterised by multiple endothelial-lined areas that vary in size from capillary channels to massive, cystic areas containing lymph. The vascular areas are lined by a single layer of endothelial cells, though papillary projections or tufting may be seen. The cells rest on a basement membrane and the supporting stroma is usually scanty. Hepatic lymphangiomatosis, typically accompanied by lymphangiomatosis of the spleen, skeleton, and different tissues, may represent a malformation syndrome. Diffuse lymphangiomatosis involving the liver and a number of organs is related to a poor prognosis. Pseudolipoma Pseudolipoma is believed to characterize an appendix epiploica connected to the Glisson capsule after changing into detached from the big bowel 1609. Lesions are usually a small, encapsulated mass of fats situated in a concavity on the floor of the liver, the fats typically displaying necrosis and calcification 891. Focal fatty change Focal fatty change of the liver is characterized by a quantity of, contiguous acini exhibiting macrovesicular steatosis of hepatocytes, with preservation of acinar structure 804. About 45% of circumstances of a sequence of focal fatty change occurred in sufferers with diabetes mellitus 632. Embryonal sarcoma A malignant tumour composed of mesenchymal cells that, by light microscopy, are undifferentiated. Symptoms include stomach enlargement, fever, weight loss, and nonspecific gastrointestinal complaints 1840. Rarely, the tumour invades the vena cava and grows into the right atrium, mimicking a cardiac tumour 561. Embryonal sarcoma is often situated in the right lobe of the liver, and varies from 10-20 cm in diameter. Gross sections reveal a variegated floor with glistening, solid, grey-white tumour tissue alternating with cystic, gelatinous areas and/or red and yellow foci of haemorrhage or necrosis. Embryonal sarcoma consists of malignant stellate or spindle cells which are compactly or loosely arranged in a myxoid stroma. Tumour cells usually present outstanding anisonucleosis with hyperchromasia; large cells which could be multinucleated are seen in lots of cases. A attribute feature is the presence of eosinophilic globules of various measurement, typically many per cell, within the cytoplasm. Entrapped bile ducts and hepatocellular components are sometimes current within the peripheral areas of those tumours. The spindle, stellate and giant cells usually present no morphological evidence of differentiation, but immunohistochemical studies in a couple of cases have demonstrated widely divergent differentiation into each mesenchymal and epithelial phenotypes, most likely from a primitive stem cell 1460. Until lately the prognosis of embryonal sarcoma has been very poor, with a median survival of less than one yr after diagnosis 1840. The survival has tremendously improved within the last sev- eral years with some patients dwelling five or more years after mixed modality therapy (surgical resection, radiotherapy, and chemotherapy). Kaposi sarcoma this lesion is outlined as a tumour composed of slit-like vascular channels, spindle cells, mononuclear inflammatory cells, with an admixture of haemosiderinladen macrophages. It includes portal areas however can infiltrate the adjoining parenchyma for short distances, and is characterized grossly by irregular, variably-sized, red-brown lesions scattered throughout the liver.
Repaglinide: 2 mg, 1 mg, 0.5 mg
Trusted repaglinide 1mgThe cells usually seem round and small diabetes mellitus risk factors buy generic repaglinide 0.5mg online, both arranged as single cells or clustered in abortive blood glucose monitor japan buy repaglinide 1 mg online, lacy gland-like or reticular formations diabetes mellitus type 2 hyperglycemia purchase repaglinide 0.5mg. Desmoplasia is more pronounced and related irritation is much less evident in diffuse cancers than in the intestinal carcinomas diabetes type 1 child order repaglinide 0.5mg visa. Adenosquamous carcinoma this lesion combines an adenocarcinoma and squamous cell carcinoma; neither quantitatively prevails. A tumour with a distinct boundary between the two elements might characterize a collision tumour. Tumours containing discrete foci of benign-appearing squamous metaplasia are termed adenocarcinomas with squamous differentiation (synonymous with adenoacanthoma). Squamous cell carcinoma Pure squamous cell carcinomas develop rarely within the abdomen; they resemble squamous cell carcinomas arising elsewhere within the body. Undifferentiated carcinoma these lesions lack any differentiated options past an epithelial phenotype. Further analysis of this heterogeneous group using histochemical strategies could allow their separation into different types. Other uncommon tumours include mixed adenocarcinoma-carcinoid (mixed exocrineendocrine carcinoma), small cell carcinoma, parietal cell carcinoma, choriocarcinoma, endodermal sinus tumour, embryonal carcinoma, Paneth cell richadenocarcinoma and hepatoid adenocarcinoma. These two lesions present both intestinal and diffuse elements (Laur�n classification). Elevated carcinomas with papillary, granular or nodular patterns and a red colour are extra usually well or moderately differentiated, tubular or papillary tumours with intestinal options; typically a preexisting adenoma is recognizable. Flat, depressed, poorly differentiated carcinomas could comprise residual or regenerative mucosal islands. In the penetrating variant, (including two sub- B classes: PenA and PenB) the invasion of the submucosa is more intensive than in the two above-mentioned variants. PenA is defined by a pushing margin, and is much less frequent than PenB, which penetrates muscularis mucosae at multiple websites. The prognosis is worse in PenA carcinomas (in contrast to adenocarcinomas of the colon, the place a pushing margin is associated with a better prognosis). The coexistence of more than one of the described patterns ends in the mixed variant 950. C Precursor lesions Gastritis and intestinal metaplasia Chronic atrophic gastritis and intestinal metaplasia commonly precede and/or accompany intestinal sort adenocarcinoma, notably in high-incidence areas 780. If gastritis persists, gastric atrophy occurs followed by intestinal metaplasia, starting a series of modifications that may end in neoplasia, especially of intestinal kind cancers. In contrast, diffuse gastric cancers typically come up in a stomach lacking atrophic gastritis with intestinal metaplasia. Stromal reactions the 4 common stromal responses to gastric carcinoma are marked desmoplasia, lymphocytic infiltrates, stromal eosinophilia and a granulomatous response. The granulomatous response is characterised by the presence of single and confluent small sarcoid-like granulomas, typically accompanied by a reasonably intense mononuclear cell infiltrate. Grading Well differentiated: An adenocarcinoma with well-formed glands, typically resembling metaplastic intestinal epithelium. Moderately differentiated: An adenocarcinoma intermediate between well differentiated and poorly differentiated. Poorly differentiated: An adenocarcinoma composed of highly irregular glands that are acknowledged with difficulty, or single cells that remain isolated or are organized in small or large clusters with mucin secretions or acinar constructions. They can also be graded as low-grade (well and reasonably differentiated) or high-grade (poorly differentiated). The two glands on the left exhibit complete intestinal metaplasia, others present the incomplete kind. These findings present that incomplete intestinal metaplasia has a combined gastric and intestinal phenotype reflecting an aberrant differentiation program not reproducing any regular grownup gastrointestinal epithelial phenotype 1574. Several proposals have been made for the terminology of the morphological spectrum of lesions that lie between non-neoplastic modifications and early invasive cancer, including the recent international Padova classification 1636. Intraepithelial neoplasia Intraepithelial neoplasia (dysplasia) arises in both the native gastric or of intestinalized gastric epithelia. Pyloric gland adenoma is a form of intraepithelial neoplasia arising in the native mucosa 2066, 1885. In the multi-stage theory of gastric oncogenesis, intraepithelial neoplasia lies between atrophic metaplastic lesions and invasive cancer (Table three. Problems associated with diagnosing gastric intraepithelial neoplasia embody the distinction from reactive or regenerative adjustments associated with active Indefinite for intraepithelial neoplasia Sometimes, doubts come up as to whether a lesion is neoplastic or non-neoplastic. In such cases, the dilemma is usually solved by chopping deeper ranges of the block, by acquiring extra biopsies, or after removing possible sources of mobile hyperproliferation. In native gastric mucosa, foveolar hyperproliferation may be indefinite for dysplasia, displaying irregular and tortuous tubular constructions with epithelial mucus depletion, a excessive nuclear-cytoplasmic ratio and loss of cellular polarity. Large, oval/round, hyperchromatic nuclei associate with outstanding mitoses, normally located close to the proliferative zone within the mucous neck area. In intestinal metaplasia, areas indefinite for intraepithelial neoplasia exhibit a hyperproliferative metaplastic epithelium. The glands may seem closely packed, lined by cells with massive, hyperchromatic, rounded or elongated, basally positioned nuclei. The cyto-architectural alterations are inclined to lower from the bottom of the glands to their superficial portion. Intraepithelial neoplasia It has flat, polypoid, or slightly depressed growth patterns; the flat sample might lack any endoscopic modifications on conventional endoscopy, but shows an irregular look on dye endoscopy. In Western international locations, the time period adenoma is applied when the proliferation produces a macroscopic, normally discrete, protruding lesion. Gastric adenomas are much less common than hyperplastic polyps; overall, they account for roughly 10% of gastric polyps 1843. They tend to come up in the antrum or mid abdomen in areas of intestinal metaplasia. Morphologically, adenomas may be described as tubular (the most common), tubulovillous, or villous; the latter two have also been known as papillotubular and papillary. Low-grade intraepithelial neoplasia this lesion reveals a slightly modified mucosal architecture, together with the presence of tubular buildings with budding and branching, papillary enfolding, crypt lengthening with serration, and cystic adjustments. Homogeneously blue vesicular, rounded or ovoid nuclei are often pseudostratified within the proliferation zone located on the superficial portion of the dysplastic tubules. High-grade intraepithelial neoplasia There is increasing architectural distortion with glandular crowding and distinguished cellular atypia. Gastric carinoma 47 Polyps Hyperplastic polyps Hyperplastic polyps are one of many commonest gastric polyps. They include a proliferation of surface foveolar cells lining elongated, distorted pits extending deep into the stroma. In a minority of instances, carcinoma develops inside the polyps in areas of intestinal metaplasia and dysplasia. The pleomorphic, hyperchromatic, normally pseudostratified nuclei typically are cigar-shaped. Progression of intraepithelial neoplasia to carcinoma Carcinoma is recognized when the tumour invades into the lamina propria (intramucosal carcinoma) or through the muscularis mucosae. Some gastric biopsies contain areas suggestive of true invasion (such as isolated cells, gland-like structures, or papillary projections).
1mg repaglinide for saleIn the United States managing diabetes 24 order repaglinide 2 mg without a prescription, hemoperfusion cartridges are expensive and have been discontinued by some producers blood glucose procedure buy 0.5 mg repaglinide mastercard, and with a brief shelf life of 2 years diabetic reaction generic repaglinide 0.5 mg without a prescription, may not be available in certain urban cities (Shalkam diabetes medications that promote weight loss buy repaglinide 1mg with visa, 2006). If a drug is equally properly removed from the blood by hemoperfusion and hemodialysis, then hemodialysis is most popular: potential issues of cartridge saturation are averted, and the incidence of hemoperfusion problems similar to thrombocytopenia and leukopenia is reduced; plus, with hemodialysis, any coexisting acid�base or electrolyte disturbances could be handled. Clear advantages of continuous remedy over repeated conventional treatments for drug rebound stay to be demonstrated. Continuous hemoperfusion has been used successfully in theophylline and phenobarbital toxicity, and continuous hemodiafiltration has been utilized in ethylene glycol and lithium toxicity (Leblanc, 1996). Poisons have varied molecular characteristics that make them roughly amenable to extracorporeal elimination. Dialyzability of a poison is possible only if it might be extracted from the plasma compartment, if a significant proportion of its complete physique shops may be eliminated, and if extracorporeal clearance contributes a significant quantity to total clearance. Removal from the plasma compartment is greatest reflected by the dialyzer extraction ratio, which may be calculated as (A-V)/A, where A represents the influx (prefilter or precolumn) concentration of the solute to be removed, and V represents the dialyzer outflow concentration. The quantity of toxin that may be eliminated by extracorporeal therapy is significantly affected by the quantity of its distribution within the physique. The ratio of extracorporeal elimination to endogenous removing is dependent upon the endogenous clearance of a selected poison and the present condition of the physique organs (liver and/or kidney) that normally Chapter 20 / Use of Dialysis and Hemoperfusion within the Treatment of Poisoning 371 D. Extracorporeal modalities have totally different molecular weight cutoffs; strategies that use diffusion such as hemodialysis normally have an approximate cutoff of 5,000 Da, whereas convection- and adsorption-based methods are able to removing poisons that are in extra of fifty,000 Da in dimension. However, at larger focus (such as in overdose), protein binding of a drug can become saturated; underneath such conditions, a higher proportion of the drug is unbound or "free," which is then available for elimination by extracorporeal therapy. Thus, even when a hemodialysis or hemoperfusion therapy extracts many of the drug present in the blood flowing through the extracorporeal circuit, the amount of drug removed throughout a single therapy session will symbolize only a small proportion of the total physique drug burden. Subsequently, further drug will enter the blood from tissue shops, generally inflicting a recurrence of the poisonous manifestations. On the opposite hand, even transiently decreasing the blood focus of many medication may mitigate sure necessary toxic results of these brokers. The development of high-cutoff hemodialysis membranes (with increased pore dimension of 8 to 10 nm) might permit clearance of bigger toxins and molecules as giant as 50 to 60 kDa. Typical sorbents are activated carbons (charcoals), ion trade resins, or nonionic exchange macroporous resins. Sorbent particles have been rendered biocompatible by coating the floor with a polymer membrane. The cartridges comprise various quantities of sorbent, the smaller ones being designed for pediatric use. A detailed comparative evaluation of in vivo performance of the varied brands of cartridges has been published (Ghannoum, 2014). The hemoperfusion circuit is much like the blood aspect of a hemodialysis circuit and contains an air detector and a venous air lure. Standard hemodialysis blood pumps and machines (without use of dialysis solution) are often used to drive the blood through the tubing and cartridge. The hemoperfusion cartridge must be primed in a vertical place with the arterial (blood inlet) facet dealing with downward. Once the cartridge has been primed, a bolus dose of heparin (usually 2,000� 3,000 units) is administered into the arterial line, the cartridge is kept inlet aspect down, and blood circulate through the cartridge is begun. As a rule, because of some adsorption on the sorbent, more heparin may be required for a hemoperfusion therapy. A single 3-hour therapy will considerably decrease the blood levels of most poisons for which hemoperfusion is effective. More prolonged use of a hemoperfusion cartridge is inefficient, as a result of the charcoal tends to become saturated. On the opposite hand, a continuous hemoperfusion therapy could need to be extended for several days until clinical improvement or a nontoxic blood degree is achieved. Hemoperfusion units could must be changed each 4 hours in the center of steady remedy. All extracorporeal methods require vascular entry by way of a central line, and this process itself is subject to problems. Hypophosphatemia during dialysis can be averted by supplementing the dialysis answer with phosphate as mentioned in Chapter 10. Performing dialysis for poisoning in a patient with metabolic or respiratory alkalosis can provoke or worsen alkalemia except the dialysis solution bicarbonate concentration is appropriately lowered. In sufferers with each severe uremia and poisoning, it might be dangerous to perform a protracted high-clearance dialysis session initially. During a dialysis remedy for a metformin-associated lactic acidosis in a markedly uremic patient, enrichment of dialysate with an acceptable quantity of urea in an try to attenuate the manifestations of the disequilibrium syndrome has been successfully performed (Doorenbos, 2001). Adsorption or activation of coagulation elements has additionally been noticed not often and could also be clinically significant in sufferers with liver failure. Fluid and electrolyte imbalances may be potential issues and require frequent monitoring. Activated charcoal should be given to patients presenting within four hours of ingestion. Concomitant ingestion of reasonable quantities of ethanol markedly increases the chance of liver harm. In adults, severe aspirin poisoning is normally accompanied by metabolic acidosis with respiratory alkalosis, whereas in youngsters, isolated metabolic acidosis is often encountered. The Done nomogram (Done and Temple, 1971), relating serum ranges and time of ingestion to consequence, gives some concept of the seriousness of salicylate poisoning in children, but is less used in grownup poisoning. Despite the reality that the drug is about 50% proteinbound, aspirin is properly removed by hemodialysis. Hemodialysis ought to be contemplated when coma Chapter 20 / Use of Dialysis and Hemoperfusion within the Treatment of Poisoning 375 is extended, particularly when problems of coma, such as pneumonia, threaten. Removal with hemodialysis using a synthetic membrane dialyzer equals that of hemoperfusion (Palmer, 2000). The chances of digoxin-induced arrhythmias are 50% and 90% at serum levels of two. Treatment consists of correction of hypokalemia, hypomagnesemia, and alkalosis and administration of oral-activated charcoal. For these reasons, solely 5% of the physique load will be removed by a 4-hour hemodialysis remedy. Plasmapheresis performed quickly after Fab fragment administration promotes elimination of the Fab�digoxin complexes (Zdunek, 2000), and high-cutoff membranes such as Theralite can be utilized for this function also (Fleig, 2011). In dialysis sufferers, Fab therapy stays most popular over hemoperfusion or plasmapheresis. Although Fab has been used successfully in patients with coexisting renal failure, digoxin could additionally be released from the Fab�digoxin complicated, leading to a rebound in toxicity, perhaps requiring a second remedy (Ujhelyi, 1993).
Cinchona. Repaglinide. - Dosing considerations for Cinchona.
- Hemorrhoids, varicose veins, colds, leg cramps, influenza, malaria, fever, cancer, mouth and throat diseases, enlarged spleen, muscle cramps, loss of appetite, and stomach discomforts such as bloating and fullness.
- What is Cinchona?
- Are there any interactions with medications?
- How does Cinchona work?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96418
Order repaglinide 1 mg visaIn this case diabetes insipidus protocol repaglinide 1 mg with mastercard, the move fee of the cleared stream is solely 60% of the inlet circulate fee diabetes test strips buy cheap repaglinide 1mg online. If the inlet circulate fee is 400 mL/min diabetes symptoms of high sugar purchase repaglinide 1 mg amex, the move rate of the cleared stream could be 0 diabetes signs headache cheap 1 mg repaglinide. Thus, a dialyzer extraction ratio of 60% interprets right into a dialyzer clearance of zero. However, the amount of blood cleared is limited by the circulate rate of 50 mL/min; although 99% of the blood is cleared, 99% of 50 mL/min is a low number. When the blood circulate price is increased, the blood is just partially cleared of urea due to less time spent within the dialyzer, but despite the precise fact that the extraction ratio falls as blood move fee is increased, the quantity of blood cleared of urea nitrogen keeps growing because the blood move rate is elevated. If the extraction ratio remained constant at 60%, a doubling of the blood move fee would double the clearance. The theoretical maximum clearance of a dialyzer (for a given solute) at infinite blood and dialysate circulate rates is identified as the K0A and has models of mL/min. Doubling the floor area of the membrane in a dialyzer will roughly double the K0A. The K0 may be elevated by making the membrane thinner, by adjusting its porosity, and by optimizing the fluid path of dialysate within the dialyzer using spacer yarns and other features. Each isopleth (curved line) represents a unique effectivity dialyzer, the place dialyzer effectivity is expressed as dialyzer K0A. Each isopleth (curved line) represents a special dialyzer having a special K0A worth. To use the nomogram, find the blood move price on the horizontal axis, then transfer as a lot as the dialyzer K0A being used, and browse of the expected dialyzer urea clearance on the vertical axis. Theoretical clearance values have been adjusted to extra intently reflect expected values in vivo. The advantages of a "highefficiency" (high K0A) dialyzer turn into obvious primarily when the blood move rate is excessive. Then the bigger dialyzers with thinner, extra efficient membranes are able to hold the extraction rate high, maximizing the rise in dialyzer clearance. For a situation where a uniform resolution is working by way of the dialyzer, one can calculate the elimination rate (in mg/min or mmol/min) of a given solute. In the idea of clearance described earlier, the blood was treated as a easy fluid. At a hematocrit of 30%, a blood circulate of 400 mL/min is mostly a plasma flow price of 280 mL/ min and an erythrocyte move rate of 120 mL/min. What is measured on the dialyzer inlet and outlet are the plasma levels of a given waste product. For instance, if the outlet plasma urea nitrogen stage is forty mg/dL, the urea focus in erythrocytes may have been decreased to about that degree also. In truth, very little creatinine or phosphorus is removed from purple blood cells during passage by way of the dialyzer. When calculating the elimination price of creatinine or phosphorus in mg/min or mmol/min, one must use the plasma circulate rate as an alternative of the blood flow fee. As noted, urea is dissolved in erythrocytes and plasma water and is removed from each during passage via the dialyzer. Approximately 93% of plasma is water (depending on its protein concentration), and about 72% of an erythrocyte is water. The correction for blood water becomes necessary when utilizing the dialyzer clearance to compute how a lot urea is being eliminated during a dialysis session. For solutes like creatinine and phosphorus which might be removed from the plasma compartment only passage via the dialyzer, the amount of removing is about 93% of Chapter three / Physiologic Principles and Urea Kinetic Modeling 43 6. Dialyzer clearance of urea (and different solutes) is dependent upon the dialysis resolution circulate price as nicely. A faster dialysis resolution circulate price increases the efficiency of diffusion of urea from blood to dialysate although the effect is usually modest. A flow price of 800 mL/min will improve urea clearance by about 5%�8% when a highefficiency dialyzer is used and when the blood circulate fee is larger than 350 mL/min. Such a lowered dialysate circulate fee may cause substantial discount in dialyzer clearance. Above that, the rise in effectivity is sort of small, particularly with some of the newer dialyzers the place the dialysis resolution flow path has been optimized. Because highmolecular-weight solutes transfer slowly via options, they diffuse poorly by way of the membrane. As a end result, the extraction ratio for molecules larger than urea shall be lower than that of urea; plus, to calculate clearance, this decrease extraction ratio must be multiplied by the plasma flow fee, and never the blood circulate rate. When we communicate of dialyzer effectivity, we refer primarily to the flexibility of a dialyzer to remove small solutes. The flux of a dialyzer refers to its capacity to remove very large molecules similar to 2microglobulin. Usually high-flux dialyzers could have a water permeability larger than 15�20 mL/hr per mm Hg. Urea is manufactured by the liver from amino acid nitrogen by way of ammonia and is the principal way in which nitrogenous waste merchandise are excreted from the body. Using a mathematical mannequin known as urea kinetics, one can compute both the speed of removal and production of urea. The extent of urea removing gives us a measure of the adequacy of dialysis, and the quantity of urea nitrogen technology provides an estimate of dietary protein consumption. The Kt/V urea was popularized by Gotch and Sargent of their reanalysis of the National Cooperative Dialysis Study (1985). Largely due to this research, guidelines teams have beneficial a minimum Kt/V value of no less than 1. The Kt/V urea is a dimensionless ratio representing volume of plasma cleared of urea (Kt) divided by the urea distribution quantity (V). K is the dialyzer blood water urea clearance (L/hr), t is dialysis session length (hours, hr), and V is the distribution volume of urea (liters, L), which is close to total physique water. K three t = L/hr 3 hr = L V=L (K 3 t)/V = L/L = dimensionless ratio If we ship a Kt/V of 1. Remove 20 L Tank V = 40 L How is Kt /V related to the "fish waste" reduction ratio Remove 40 L Tank V = 40 L How is Kt /V associated to the "fish waste" discount ratio On eradicating the fish, the whole 40 L (V) is drained and changed with clean water. Remove 1 L Tank V = 40 L Amount cleared (Kt) = 40 L Tank V = forty L Kt/V = 40/40 = 1. Chapter 3 / Physiologic Principles and Urea Kinetic Modeling forty seven reduction ratio is 100%. With a 1-L cup, one removes 1 L of dirty water and replaces it with 1 L of clean water. Taking out solely a small quantity at a time keeps the fish pleased and permits it to stay in the tank throughout cleaning. If one does this forty instances, then a total of 40 L (40 � 1 L) could have been "cleared," and the Kt will be 40.
Cheap repaglinide 1 mg on lineSeveral research document an excellent level of diagnostic accuracy and value effectiveness diabetes oatmeal discount repaglinide 1 mg fast delivery, and the take a look at exhibits much less variability than different checks of iron status (Fishbane diabetes type 1 research paper buy repaglinide 2 mg fast delivery, 2001) diabetes type 2 hypo symptoms generic repaglinide 0.5 mg on-line. Intravenous iron could additionally be administered on an episodic foundation as needed when iron deficiency develops diabetes insipidus johns hopkins buy repaglinide 2mg amex, or by the repeated administration of small doses to preserve iron balance. However, these dietary supplements are related to poor efficacy and troublesome unwanted side effects, similar to constipation, dyspepsia, bloating, or diarrhea. Three randomized trials have compared oral iron with either placebo or no iron therapy in hemodialysis patients; not one of the three was able to demonstrate any efficacy for oral iron. For sufferers on peritoneal dialysis, oral iron is much more handy than intravenous iron. Since these sufferers expertise much less continual blood loss, oral iron could also be enough to maintain iron stores. Oral iron often is given as ferrous sulfate, fumarate, or gluconate, in a dosage of 200 mg of elemental iron per day. The timing of the Chapter 34 / Hematologic Abnormalities 603 iron dose is essential; ideally, iron should be taken on an empty abdomen to optimize efficacy. The main sites of iron absorption are the duodenum and proximal jejunum, and gastrointestinal signs are proportional to the amount of elemental iron offered to the duodenum at a single time; discount of symptomatology could require altering the oral preparation, using pediatric dosages at extra frequent intervals, or even taking the iron dosage with meals. A common downside with oral iron is constipation, which can be partially managed, if needed, with stool softeners or laxatives. Phosphorus binders, antacids, histamine-2 antagonists, and proton-pump inhibitors may all inhibit the absorption of oral iron dietary supplements. Four preparations can be found in the United States: Iron dextran, ferric gluconate, ferumoxytol, and iron sucrose. Intravenous iron remedy has superior availability and efficacy compared with oral iron therapy. In hemodialysis patients, the goal hemoglobin stage is difficult to obtain with out intravenous iron therapy. As a outcome, most hemodialysis patients will require intravenous iron regularly. In distinction, intravenous therapy prices extra, and its security profile is less clear than that of oral iron. One is to deal with established iron deficiency with a repletive 1,000-mg dose administered over 8�10 consecutive hemodialysis therapies. Alternatively, since iron deficiency occurs so regularly in hemodialysis patients, a weekly upkeep dose of 25�100 mg may be used. A recent observational research discovered the repletion method to have larger efficacy in contrast with upkeep dosing (Kshirsagar, 2013a), while not obviously rising the risk for cardiovascular events (Kshirsagar, 2013b). However, a repletion technique may have a greater an infection danger in contrast with bolus therapy (Brookhart, 2013). When intravenous iron is required for peritoneal dialysis patients, infusions of 250 mg of iron could additionally be administered over 1�2 hours. Because of the upper expected necessary issue to understand in regards to the safety of intravenous iron is that it has not been properly studied. The best understood complication of intravenous iron remedy is the uncommon incidence of anaphylactoid-type reactions. These are characterized by the abrupt incidence of hypotension, dyspnea, flushing, and again ache. Such reactions are less incessantly noticed, and have a tendency to be of milder depth with the nondextran types of iron. Iron is a vital development issue for microorganisms, and intravenous iron remedy has the potential to make iron extra readily available to these pathogens. In addition, in vitro studies counsel that iron treatment may interfere with phagocytic operate of white blood cells. Early retrospective research found higher serum ferritin ranges in hemodialysis sufferers to be related to elevated danger of infection. In contrast, a large, prospective, multicenter study (Hoen, 2002) discovered no relation between serum ferritin or remedy with intravenous iron and risk of bacteremia. The current literature on this subject stays inconclusive (Brookhart, 2013), however a prudent method could be to keep away from intravenous iron remedy during acute infectious episodes. A potential harmful effect of vascular oxidation could be an acceleration of atherosclerotic processes. This is probably true for all present types of iron dextran, however notably the high molecular weight variety (Chertow, 2006). In nonuremic patients, instant allergic reactions to intravenous iron dextran have been reported. An essential explanation for an obvious hypo- often occur inside 5 minutes of injection but may be delayed by forty five minutes or extra. For this purpose, epinephrine and different means to treat anaphylaxis must be at hand when intravenous iron dextran is run. Importantly, Walters and Van Wyck (2005) reported that virtually all extreme reactions occur with the check dose or first therapeutic dose. Milder instant hypersensitivity reactions to iron dextran infusion embody itching and urticaria. Delayed reactions can manifest as lymphadenopathy, myalgia, arthralgia, fever, and headache. Intravenous sodium ferric gluconate is a nondextran type of iron used in the United States since 1999 and in Europe for several a long time. As mentioned above, adverse reactions are in all probability less frequent and fewer severe than those seen with iron dextran. Intravenous sodium ferric gluconate may be administered to hemodialysis sufferers in the amount of 1,000 mg given in divided doses over eight consecutive treatments. Intravenous iron sucrose was approved to be used in the United States in 2000 and has been in use in Europe for a few years. Like sodium ferric gluconate, the other broadly used nondextran type of iron, reports usually point out an excellent security and efficacy profile. No critical antagonistic reactions occurred in 665 hemodialysis sufferers receiving eight,583 doses of the drug (Aronoff, 2004). The drug could additionally be administered as iron substitute remedy, a hundred mg for 10 consecutive doses, or as a weekly dose of 25�100 mg. Ferric pyrophosphate citrate (Triferic) is an iron compound designed to be added to the dialysis resolution with the aim of including a small quantity of iron to the affected person during every dialysis therapy. Often, the bleeding may be apparent, as in sufferers undergoing surgery, menstruating women, or these with accidents involving the vascular entry. In patients on dialysis, the underlying reason for inflammation may not be readily obvious.
Discount 1 mg repaglinide free shippingFor these reasons blood glucose serum levels repaglinide 0.5mg with mastercard, some observers have suggested that pancreatoblastoma represents the paediatric counterpart of acinar cell carcinoma managing your diabetes care cheap repaglinide 2mg fast delivery. Although this proposal is attractive in many ways diabetes journal articles purchase repaglinide 1 mg with visa, pancreatoblastoma Pancreatoblastoma 245 Solid-pseudopapillary neoplasm G blood sugar checker generic repaglinide 1 mg mastercard. Adler Definition A usually benign neoplasm with predominant manifestation in younger ladies, composed of monomorphic cells forming stable and pseudopapillary buildings, incessantly showing haemorrhagic-cystic adjustments and variably expressing epithelial, mesenchymal and endocrine markers. Epidemiology Solid-pseudopapillary neoplasm is uncommon but has been acknowledged with rising frequency lately 946, 1192, 1358. It accounts for about 1-2% of all exocrine pancreatic tumours 359, 941, 1280. It happens predominantly in adolescent women and younger ladies (mean 35 years; range 8-67 years) 1781, 1072. Moreover, only very few girls developed a strong pseudopapillary neoplasm after long-term use of hormonal contraceptives 359, 436, 1655. Clinical options Usually, the neoplasms are found by the way on routine physical examination or they cause belly discomfort and pain 1358, often after stomach trauma 945. Administration of contrast medium results in enhancement of the strong tumour parts. On angiography, the neoplasms are normally hypovascular or mildly hypervascular lesions with displacement of surrounding vessels 2153. Fine needle aspiration cytology performed under radiological control shows monomorphic cells with spherical nuclei and eosinophilic or foamy cytoplasm 234, 2119, 2140. Macroscopy the neoplasms current as giant, spherical, solitary lots (average measurement 8-10 cm; range, 3-18 cm), and are often fluctuant. The cut surfaces reveal lobulated, gentle brown strong areas, zones of haemorrhage and necrosis, and cystic areas full of necrotic particles. Occasionally, the haemorrhagic-cystic modifications involve virtually the complete lesion so that the neoplasm may be mistaken for a pseudocyst. A few tumours have been found to be attached to the pancreas or even in extrapancreatic areas 812, 914, 945. A Tumour spread Only few metastasizing solid-pseudopapillary neoplasms have been reported 359, 1358. Common metastatic sites embody regional lymph nodes, the liver, peritoneum, and greater omentum 300, 2209, 1358. Histopathology In giant neoplasms, in depth necrosis is typical and the preserved tissue is normally discovered in the tumour periphery beneath the fibrous capsule. B the pseudocystic neoplasm is hooked up to the spleen, and exhibits haemorrhagic necrosis. In both patterns, the uniform polyhedral cells are organized round delicate, usually hyalinized fibrovascular stalks with small vessels 1395. In the solid parts, disseminated aggregates of neoplastic cells with foamy cytoplasm or cholesterol crystals surrounded by foreign body cells may be discovered. The spaces between the pseudopapillary buildings are crammed with red blood cells. The hyalinized connective tissue strands might include foci of calcification and even ossification 1193. The round to oval nuclei have finely dispersed chromatin and are sometimes grooved or indented. Mitoses are usually rare, but in a number of instances prominent mitotic exercise is noticed 1358. The neoplastic tissue is often nicely demarcated from the traditional pancreas, though a fibrous capsule could additionally be absent and invasion of tumour cell nests into the encircling pancreatic tissue could happen 1193, 1358. Consequently, benign showing solid-pseudopapillary neoplasms should be categorised as lesions of uncertain malignant potential. In this strong space, the uniform tumour cells are separated by vascular hyalinized stroma. Cytokeratin is detected in 30% 946 to 70% 963, 2195, depending on the method of antigen retrieval utilized. Solid-pseudopapillary neoplasm 247 Usually, the staining for keratin is focal and faint. Positive immunoreactivity for trypsin, chymotrypsin, amylase and/or phospholipase A2 has been reported 166, 1072, 1192, 1226, 1844, however has not been confirmed by most different authors 812, 945, 1282. Similarly, focal positivity for glucagon, somatostatin and/or insulin has been described in some tumours 1226, 2021, 2147, however was not detected in most different instances 1072, 1282, 1844. Neurosecretory-like granules have been described in a number of tumours 867, 880, 1684, 2119, 2147. Intermediate cell junctions are hardly ever noticed and microvilli are missing, but small intercellular spaces are frequent. An unbalanced translocation between chromosomes 13 and 17 leading to a lack of 13q14qter and 17p11pter has been described in one solid-pseudopapillary neoplasm 616. Local spread or dissemination to the peritoneal cavity has been reported within the context of abdomi- Ultrastructure the neoplastic cells have round or markedly indented nuclei containing a small single nucleolus and a slender rim of marginated heterochromatin. Zymogen-like granules of variable sizes (500-3000 nm) are conspicuous, probably representing deposits of alpha-1-antitrypsin. The contents of those granules generally dis- nal trauma and rupture of the tumour 1060. Even in patients who had native unfold, recurrences 359, 999, or metastases 234, 1192, 1642, long disease-free durations have been recorded after initial analysis and resection. Only a couple of patients have died of a metastasizing solid-pseudopapillary neoplasm 1192, 1395. Perineural invasion, angioinvasion, or deep invasion into the encompassing tissue point out malignant behaviour, and such lesions are categorised as solid-pseudopapillary carcinoma. Venous invasion, a high degree of nuclear atypia, mitotic exercise and prominence of necrobiotic cell nests (cells with pyknotic nuclei and eosinophilic cytoplasm) have been reported to be related to malignancy 1358. Ultrastructurally, the cells present plentiful mitochondria and lack zymogen and neuroendocrine granules. Differential prognosis consists of endocrine tumour 1454 and stable pseudopapillary tumour. Nonmucinous, glycogen-poor cystadenocarcinoma A massive, encapsulated mass with cystic spaces lined by serous adenoma like part and malignant-appearing columnar epithelium. The tumour cells are unfavorable for mucins and present oncocytic options by electron microscopy 533. Clear cell carcinoma A carcinoma composed of clear cells, rich in glycogen and poor in mucin, morphologically resembling renal cell carcinoma 941. Adenocarcinomatous, anaplastic, or intraductal papillary components can be discovered 1781. Ciliated cell carcinoma this lesion exhibits the pattern of ductal adenocarcinoma, but incorporates many ciliated cells, as demonstrated at the ultrastructural degree 1781.
Generic 2 mg repaglinide free shippingThe cells are arranged as stable lots with areas of cellular pyknosis and necrosis and high mitotic activity diabetic diet meal generic repaglinide 2mg. Mixed epithelial and mesenchymal the largest number of hepatoblastomas (44%) show a pattern combining fetal and embryonal epithelial components with primitive mesenchyme and mesenchymally derived tissues diabetes in senior dogs cheap repaglinide 1 mg online. The primitive mesenchymal tissue consists of a light-weight myxomatous stroma containing massive numbers of spindleshaped cells with elongate nuclei diabetes type 2 images order 0.5 mg repaglinide with amex. The cells could display a parallel orientation with collagen fibers and cells resembling young fibroblasts blood sugar range after eating 0.5 mg repaglinide otc. More mature fibrous septa with properly differentiated fibroblasts and collagen may also be seen. Islands of osteoid-like tissue composed of a smooth eosinophilic matrix containing lacunae filled with a quantity of cells are the hallmark of the mixed lesion. Infantile haemangioendothelioma, the most commonly occurring benign tumour of the liver, is seen nearly exclusively in the first 12 months of life and presents as an asymptomatic mass or, much less incessantly, as congestive heart failure as a end result of speedy shunting of blood through the liver 1708. There is, nevertheless, a single case report of a discrete cystic teratoma contiguous to a hepatoblastoma 331. The one to two-cell thick trabeculae of fetal epithelial hepatoblastoma sample are seen on the best. Areas showing mesenchymal tissue and foci of osteoid-like materials are present, along with areas of epithelial hepatoblastoma. Focal nodular hyperplasia and nodular regenerative hyperplasia may be seen within the first few years of life however are extra frequent in older youngsters 1839. Genetic susceptibility Congenital anomalies are noted in approximately 5% of sufferers (Table 8. Other syndromes with an increased incidence of hepatoblastoma embody Beckwith-Wiedemann syndrome, trisomy 18, trisomy 21, Acardia syndrome, Goldenhar syndrome, Prader Willi syndrome, and kind 1a glycogen storage illness 1585. Increased copy numbers of c-met and K-sam proto-oncogenes and cyclin D1 genes have been described in a case of hepatoblastoma in an adult patient 977. The presence of oval cell antigen has been demonstrated in hepatoblastomas, which helps the stem cell origin of those tumours 1631. Prognosis and predictive elements Prognosis is immediately affected by the ability to resect the lesion entirely, i. Chemotherapy and transplantation have allowed resectability in 90% of circumstances, growing the overall survival to 65-70%. Other elements positively influencing prognosis embrace tumour confined to one lobe, fetal epithelial growth pattern, and multifocal dissemination (rather than unifocal progress pattern within the liver with distant metastases and vascular invasion) 2022. Wotherspoon Definition Primary lymphoma of the liver is outlined as an extranodal lymphoma arising within the liver with the bulk of the illness localized to this web site. Contiguous lymph node involvement and distant unfold may be seen but the major medical presentation is within the liver, with remedy directed to this web site. It is mainly a disease of white center aged males 1043, 1217 although an occasional case has been reported in childhood 1557. Patients are virtually at all times male (M:F roughly 5:1) but are often younger with a imply age of 20 years (range 8-68 years) 334. In distinction to primary lymphoma, secondary liver infiltration is a frequent occurrence, being current in 80-100% of circumstances of persistent leukaemia, 50-60% of instances of non-Hodgkin lymphoma and approximately 30% of circumstances of multiple myeloma 2042, 261. Aetiology A proportion of instances are related to hepatitis C virus infection with and with out combined cryoglobulinaemia 390, fifty six, 1257, 90, 371, 1625, 311. Clinical options probably the most frequent presenting signs are proper upper abdominal/epigastric pain or discomfort, weight loss and fever 1043, 1217. Most cases are solitary or a number of plenty within the liver which can be misdiagnosed as a main liver tumour or metastatic most cancers 1043, 1217. Some cases have been reported with diffuse infiltration of the liver associated with hepatomegaly however and not using a discrete mass, simulating hepatic inflammation 668. Hepatosplenic T-cell lymphomas current with hepatosplenomegaly, normally without peripheral lymphadenopathy and without lymphocytosis. Liver operate checks are usually irregular with average elevation of ranges of transaminases and alkaline phosphatase. Histopathology B-cell lymphoma the overwhelming majority of main hepatic lymphomas are of diffuse giant B-cell type with sheets of huge cells with massive nuclei and outstanding nucleoli. Occasional circumstances of Burkitt lymphoma have been described 759 by which the morphology is typical of Burkitt lymphoma encountered elsewhere within the digestive tract. The atypical lymphoid cells have centrocyte-like cell morphology and surround reactive germinal centres. Lymphoepithelial lesions are fashioned by the centrocyte-like cells and the bile duct epithelium, and these may be highlighted by staining with anti-cytokeratin antibodies. Secondary involvement of the liver by persistent lymphocytic leukaemia and B-cell non-Hodgkin lymphoma tends to present a distribution involving the portal triads although nodular infiltration can also be seen with non-Hodgkin lymphoma and a quantity of myeloma 2042. Hepatosplenic T-cell lymphoma that is characterized by infiltration of the sinusoids by a monomorphic inhabitants of medium sized cells with a reasonable amount of eosinophilic cytoplasm. The nuclei are spherical or slightly indented with reasonably dispersed chromatin and comprise small, normally basophilic, nucleoli. There may be mild sinusoidal dilation and there are occasional pseudo-peliotic lesions. A similar sinusoidal sample of infiltration is seen within the spleen and bone marrow each of which are usually involved by the lymphoma at diagnosis 486, 334. All instances are negative for F1 and optimistic with antibodies for the T-cell receptor. Genetics Hepatosplenic T-cell lymphoma reveals rearrangement of the T-cell receptor gene. Cytogenetic research have shown isochromosome 7q in numerous circumstances and in some this has been present as the only cytogenetic abnormality 524, 48 Prognosis the prognosis of major hepatic lymphoma is mostly poor. Chemotherapy or radiotherapy alone has been reported to be ineffective however combination modalities, including surgical procedure in resectable instances, can provide comparatively good results. Nakanuma Definition Benign and malignant tumours arising within the liver, with vascular, fibrous, adipose and different mesenchymal tissue differentiation. Imaging Imaging studies establish the presence of a space-occupying lesion or lesions within the liver, and should present a diagnosis or differential analysis 1565. It accounts for 8% of all liver tumours and pseudotumours from delivery to 21 years of age, however during the first two years of life it represents 12% of all hepatic tumours and pseudotumours, and for 22% of the benign neoplasms 1839. Lesions involve the right lobe in 75% of cases, the left lobe in 22% and both lobes in 3%. Presentation is typically with stomach swelling, but speedy accumulation of fluid within the tumour may cause sudden enlargement of the abdomen 1841. This tumour-like lesion consists of unfastened connective tissue and epithelial ductal elements in various proportions. Grossly, the reduce surfaces exhibit strong, pink-tan areas and cysts containing a clear fluid.
References - Carlson LE, Speca M, Patel KD, Goodey E. Mindfulness- based stress reduction in relation to quality of life, mood, symptoms of stress, and immune parameters in breast and prostate cancer outpatients. Psychosom Med. 2003;65(4):571-581.
- Staner L, Luthringer R, Macher JP. Effects of antidepressant drugs on sleep EEG in patients with major depression. Mechanisms and therapeutic implications. CNS Drugs 1999;11:49-60.
- O'Regan GM, Sandilands A, McLean WH, et al. Filaggrin in atopic dermatitis. J Allergy Clin Immunol 2009; 124: R2-R6.
- Sharlip ID: Guidelines for the diagnosis and management of premature ejaculation, J Sex Med 3(Suppl 4):309n317, 2006.
- Kakimoto N, Gamoh S, Tamaki J, et al. CT and MR images of pleomorphic adenoma in major and minor salivary glands. Eur J Radiol 2009;69:464-472.
|