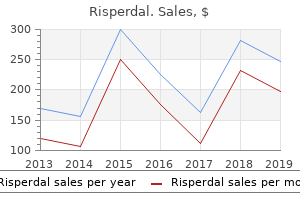
Risperdal
Katie B. Clarkson, M.D. - Greenwood Genetic Center
- Columbia, South Carolina
Generic risperdal 3mg onlineTacrolimus: elevated ciclosporin concentration and toxicity � keep away from concomitant use medications vs medicine order risperdal 3mg fast delivery. Ursodeoxycholic acid: unpredictably increased absorption and raised ciclosporin ranges in some patients treatment diabetes buy risperdal 4 mg on line. Over 2�6 hours peripherally or 1 hour centrally Dilute 50 mg in 20�100 mL with sodium chloride zero medicine 4 the people buy risperdal 4 mg without a prescription. Cidofovir is eradicated primarily by renal excretion treatment whooping cough risperdal 2 mg visa, each by glomerular filtration and tubular secretion. Use with probenecid might cut back the excretion of cidofovir to some extent by blocking tubular secretion, though 70�85% has nonetheless been reported to be excreted unchanged within the urine within 24 hours. Administer 2 hours earlier than dialysis session to benefit from peak focus without having delayed clearance. Pharmacokinetics of cidofovir in renal insufficiency and in steady ambulatory peritoneal dialysis or high-flux haemodialysis. After oral absorption cilazapril is quickly metabolised within the liver to cilazaprilat, the bioavailability of which is about 60%. Peak plasma concentrations of cilazaprilat happen within 2 hours of an oral dose of cilazapril. Antibacterials: focus elevated by erythromycin � contemplate reducing cilostazol dose. Antifungals: focus possibly elevated by ketoconazole � consider lowering cilostazol dose. Calcium-channel blockers: concentration increased by diltiazem � contemplate reducing cilostazol dose. Ulcer-healing drugs: focus elevated by omeprazole � consider decreasing cilostazol dose. The drug should be used with nice caution if administered to sufferers with a creatinine clearance <25 mL/min. Dose can additionally be lowered to 50 mg twice daily if used with medication which have an effect on its clearance. Cimetidine is partially metabolised within the liver to the sulfoxide and to hydroxymethyl cimetidine. About 50% of an oral dose, and 75% of an intravenous dose, is excreted unchanged within the urine in 24 hours. After an oral or parenteral dose of 300 mg, blood concentrations stay above that required to provide 80% inhibition of basal gastric acid secretion for 4 to 5 hours. Potentially hazardous interactions with other medicine Alpha-blockers: effects of tolazoline antagonised. Anti-arrhythmics: elevated focus of amiodarone, flecainide, lidocaine procainamide and propafenone. Antifungals: absorption of itraconazole and ketoconazole lowered; posaconazole focus lowered � keep away from; terbinafine concentration increased. Antimalarials: keep away from concomitant use with artemether/lumefantrine; metabolism of chloroquine, hydroxychloroquine and quinine inhibited. Antipsychotics: presumably enhanced impact of antipsychotics, chlorpromazine and clozapine. Antivirals: concentration of atazanavir lowered; concentration of raltegravir and saquinavir possibly increased � keep away from; keep away from for 12 hours before and 4 hours after rilpivirine. Cytotoxics: presumably enhances myelosuppressive results of carmustine and lomustine; focus of epirubicin and fluorouracil elevated; avoid with erlotinib; presumably lowered absorption of lapatinib; possibly lowered absorption of pazopanib � give at least 2 hours earlier than or 10 hours after cimetidine. Parathyroid carcinoma and first hyperparathyroidism: 30 mg twice daily increasing to a maximum of 90 mg 4 instances a day. Hormone antagonists: metabolism of tamoxifen to energetic metabolite inhibited � avoid. The major circulating metabolites are inactive, and are renally excreted, with 80% of the dose recovered in the urine, and 15% in the faeces. The elimination of metabolites happens as follows: one third in the urine (unchanged as metabolites and glucuronide conjugates) and two thirds within the faeces. Antidiabetics: might enhance glucose tolerance and have an additive effect with insulin or sulphonylureas. Lipid-regulating medicine: increased threat of myopathy in combination with statins and ezetimibe (do not exceed 10 mg of simvastatin and 20 mg of rosuvastatin1) � keep away from concomitant use with ezetimibe. Subjects with average renal impairment excreted on common 7% of a single dose as unchanged ciprofibrate over ninety six hours, in contrast with 6. Oxociprofloxacin seems to be the main urinary metabolite and sulfociprofloxacin the first faecal metabolite. About 40�50% of an oral dose is excreted unchanged in the urine and about 15% as metabolites. Up to 70% of a parenteral dose could also be excreted unchanged inside 24 hours and 10% as metabolites. Faecal excretion over 5 days has accounted for 20�35% of an oral dose and 15% of an intravenous dose. Antidepressants: metabolism of duloxetine inhibited � avoid; keep away from with agomelatine. Ciclosporin: variable response; no interaction seen locally; some reports of increased nephrotoxicity. Cytotoxics: possibly decreased excretion of methotrexate; focus of erlotinib elevated. Theophylline: presumably increased risk of convulsions; elevated levels of theophylline. Do not take milk, iron preparations, indigestion cures or phosphate binders simultaneously ciprofloxacin orally. Long term use in extreme renal impairment can lead to the sufferers turning into nauseous. Single agent remedy: 50�120 mg/m as a single dose every 3�4 weeks or 15�20 mg/ m2 every day for five days each 3�4 weeks. Aminoglycosides: elevated danger of nephrotoxicity and presumably ototoxicity with aminoglycosides, capreomycin, polymyxins or vancomycin. Cytotoxics: increased risk of ototoxicity with ifosfamide; increased pulmonary toxicity with bleomycin and methotrexate. More than 90% of the platinum from a dose is protein bound inside 2 to four hours; only the unbound fraction has important antineoplastic activity. Excretion of intact drug and metabolites is especially within the urine however is incomplete and extended: as a lot as about 50% of a dose has been reported to be excreted in urine over 5 days, and platinum could additionally be detected in tissue for several months afterwards. The unbound fraction, which is extra rapidly cleared (20�80% within 24 hours), may be actively secreted by the renal tubules.
Buy 3 mg risperdal fast deliveryIncreased numbers of small lymphocytes medicine januvia purchase risperdal 2 mg, some resembling plasma cells ("plasmacytoid lymphocytes") with abundant basophilic cytoplasm medicine escitalopram discount 3 mg risperdal mastercard, are common treatment under eye bags cheap risperdal 3 mg otc. Hairy Cell Leukemia the median age of patients with this illness is roughly fifty five years medicine grace potter discount risperdal 3 mg online, and the male:female ratio is about four:1. In most sufferers, the neoplastic B-lymphoid cells affect primarily the bone marrow and spleen, inflicting splenomegaly, monocytopenia, and neutropenia in most patients. The illness, which accounts for about 2% of grownup leukemias, predisposes to bacterial infections due to neutropenia, but in addition causes diminished cell-mediated immunity. Some patients produce other rheumatologic problems, together with systemic sclerosis, polymyositis, and polyarteritis nodosa. Nearly all sufferers with this illness have palpable splenomegaly, typically to gargantuan measurement, and about 40% have hepatomegaly. In addition to cytopenia in one or more cell strains, peripheral smears in about 85% of cases reveal bushy cells-small- to medium-sized lymphoid cells that possess a spherical, kidneyshaped, oval or bilobed, and commonly eccentric, nucleus with ground-glass chromatin, but absent or inconspicuous nucleoli, and plentiful, pale blue cytoplasm with quite a few irregular, skinny, floor projections resembling hairs. Because of related fibrosis, bone marrow aspiration usually ends in a dry faucet. Bone marrow biopsies are often hypercellular and classically reveal interstitial infiltration with mononuclear cells possessing plentiful cytoplasm and outstanding cell borders, creating a "fried-egg" appearance. The fibrosis produces a net-like pattern affecting areas of bushy cell infiltration. In contrast to the B-cell lymphomas, classification of mature T-cell lymphomas based on cell of origin is tough 530 due to our limited understanding of T-cell ontogeny. T-Cell Prolymphocytic Leukemia this dysfunction accounts for about 2% of grownup small lymphocytic leukemias and is primarily a disease of people more than 50 years old, with most patients having impressive splenomegaly. Skin nodules or diffuse papular rashes happen in about 25% of instances; pleural effusions or ascites happen in about the identical number. The major laboratory discovering is a very high white cell rely, exceeding 200 � 109/L in about two-thirds of sufferers. The diagnosis is established on peripheral blood films, where most leukocytes are prolymphocytes, with a well-defined central nucleolus and a deeply basophilic cytoplasm that always demonstrates blebs or protrusions. These cells are bigger than regular small lymphocytes, however in 20% of circumstances of T-cell prolymphocytic leukemia (the small-cell variant), the cells are small, with more condensed nuclear chromatin and no obvious nucleolus on routine staining, but nucleoli are detectable, nonetheless, on electron microscopy. Bone marrow biopsies show heavy infiltration that might be interstitial, nodular, diffuse, or combined. The most distinguished clinical characteristic is splenomegaly, current in about 50%; lymph node enlargement is rare. The white cell rely is elevated due to an increased number of large granular lymphocytes, which usually appear regular and have round or oval, eccentric nuclei with condensed chromatin and abundant basophilic cytoplasm containing small or giant purplish granules. Bone marrow involvement is variable and often minimal, the everyday sample being intrasinusoidal. Patients with neutropenia usually have normal immature granulocytes but decreased neutrophils (maturation arrest), and sufferers with thrombocytopenia characteristically show adequate or elevated megakaryocytes. Patients current acutely with fever, cytopenias, lymphadenopathy, and hepatosplenomegaly. Peripheral blood smear exhibits large atypical lymphocytes with nice cytoplasmic granules and irregular, hyperchromatic nuclei. The bone marrow involvement is variable and could additionally be related to hemophagocytosis. Most patients have acquired the infection at an early age via breast milk or publicity to blood, and the lifetime cumulative risk of later growing leukemia or lymphoma, which happens at a median age of about fifty five years, is approximately 2%. The typical scientific options include generalized lymph node enlargement, hypercalcemia, hepatosplenomegaly, and skin lesions, which could be nodules, papules, or a diffuse scaly rash. Some patients have opportunistic infections from decreased cell-mediated immunity. The lymphomatous variant consists of generalized lymph node enlargement with out circulating leukemic cells. The continual variant has outstanding skin lesions, principally an exfoliative course of, but no hypercalcemia. Peripheral blood smears classically present pleomorphic lymphocytes, with clumped chromatin, prominent nucleoli, and lobated nuclei. Bone marrow involvement is common and generally the cells are quite pleomorphic with prominent nucleoli. The bony buildings could seem abnormal due to increased osteoclastic exercise. The neoplastic lymphocytes secrete chemokines that drive bone resorption, resulting in hypercalcemia and osteolytic lesions. Adult T-cell leukemia/lymphoma is a neoplastic course of arising from T-regulatory cells, which function to suppress the immune system. This proliferation of T-regulatory cells and the consequent immunosuppression correlates with the frequent opportunistic infections seen in these sufferers. From these areas, it could disseminate to distant sites, such as the gastrointestinal tract, cervical lymph nodes, and the skin, the place nodules and ulcers could form. When the illness originates outdoors the nasal cavity, systemic symptoms can occur. The lymphoma cells commonly are intermingled with numerous benign cells, such as small lymphocytes, histiocytes, eosinophils, and plasma cells, making the illness typically seem inflammatory quite than neoplastic. They might have irregular and elongated nuclei, usually undergoing mitosis, with granular chromatin. Hepatosplenic T-Cell Lymphoma Hepatosplenic T-cell lymphoma is a disorder of the innate immune system, arising from cytotoxic / T-cells. It classically arises in adolescents and young men, however a subset is associated with immunosuppression, especially sufferers exposed to azathioprine. The major medical function is marked hepatosplenomegaly without lymphadenopathy, normally accompanied by thrombocytopenia. In the liver and spleen, the neoplastic cells are medium sized and percolate by way of the hepatic and splenic sinuses. The marrow biopsy exhibits interstitial or intrasinusoidal infiltration with medium- to large-sized lymphoid cells with a rim of pale cytoplasm. Mycosis Fungoides and S�zary Syndrome this disorder happens mostly in adults, with a male: female ratio of about 2:1. It is a cutaneous T-cell lymphoma that begins as flat areas of skin scaling and erythema that might be asymptomatic or pruritic. At various intervals, however sometimes after several years, it may progress to cause dusky red to violaceous plaques-sharply demarcated lesions which would possibly be elevated above the encompassing normal skin. Sometimes, lymph nodes are enlarged, however biopsies commonly show a reactive pattern, quite than neoplastic infiltrates. If the disease continues to advance, the following stage is the formation of cutaneous tumors. Only then does the lymphoma are most likely to unfold to extracutaneous websites, typically, lymph nodes, spleen, liver, and lungs. Confident pathologic diagnosis of mycosis fungoides may be very difficult, especially within the early levels, and numerous pores and skin biopsies, generally taken over intervals of months to years, could also be necessary before the characteristic findings are clearly current.
Risperdal: 4 mg, 3 mg, 2 mg
Buy risperdal 2 mg with mastercardF: A biopsy demonstrates replacement of the marrow by uniformly spaced treatment menopause cheap 2mg risperdal overnight delivery, massive treatment yeast infection child 2mg risperdal visa, immature cells with folded nuclei and ample cytoplasm symptoms 9 days after iui purchase 4 mg risperdal fast delivery. C: High-power view of a bone marrow biopsy reveals a hypercellular bone marrow with uniformly spaced medications quit smoking purchase 3mg risperdal, massive immature hematopoietic cells with abundant eosinophilic-staining cytoplasm and bilobed nuclei. B: Aspirate smears show increased numbers of irregular promyelocytes with weird cytoplasmic granulation together with typical Auer rods (shown on the left), massive coarse granules (shown in the right central area), and fantastic, dust-like eosinophilic granules. B: Close examination of the abnormal promyelocytes in this case reveals nice, dust-like eosinophilic granules within the cytoplasm. C: A bone marrow biopsy reveals alternative of bone marrow by monotonous sheets of uniformly spaced bilobed immature hematopoietic precursors. A: Blood smear exhibits elevated numbers of irregular bilobed promyelocytes with hypogranular cytoplasm and thrombocytopenia. These giant immature hematopoietic cells with folded nuclear contours can be confused with monocytic blasts. B: Bone marrow biopsy demonstrates a monotonous proliferation of uniformly spaced giant cells with characteristic bilobed (buttock-like) nuclei and ample cytoplasm. A: Core biopsy at 380 prognosis of acute promyelocytic leukemia with sheets of promyelocytes and absence of myeloid maturation. A: Hypocellular aspirate smear demonstrates uncommon, irregular, closely granulated promyelocytes. B: Bone marrow biopsy exhibits architectural distortion suggesting important marrow fibrosis and replacement by a monotonous immature hematopoietic cell population. Higher magnification of the biopsy (inset) discloses monotonous foci composed of uniformly spaced immature, bilobed hematopoietic precursors. The ideograms of chromosomes 9 and eleven and the respective by-product chromosomes are to the left in color, and the corresponding G-banded chromosome pairs are to the proper. A: Aspirate smear with elevated blasts and a dysplastic mature erythroid precursor displays irregular nuclear contours (arrow). B: Aspirate smear reveals a quantity of giant hypogranular bands (arrows) and a dysplastic erythroid precursor with asymmetric binucleation is situated just under the centrally situated hypogranular band. C: Aspirate smear reveals elevated blasts and two dysplastic micromegakaryocytes (arrows). B: Low-power magnification of aspirate smear demonstrates hypercellular marrow fragments consisting exclusively of monotonous sheets of primitive 386 mononuclear cells. C: High-power view of aspirate smear discloses nucleolated undifferentiated blasts. B: Aspirate smear demonstrates immature myeloid precursors, a few of which present the presence of quite a few main granules within the cytoplasm. A: Blood smear displays a spectrum primarily immature and uncommon mature myeloid precursors. A: Aspirate smear exhibits a leukemic blast population composed principally of promyelocytes that might be confused with a case of acute promyelocytic leukemia. B: Myeloperoxidase stains present strong diffuse staining that obscures nuclear morphology. C: A hypercellular clot part consists virtually solely of huge blasts with "open" chromatin sample (vesicular nuclei), two to three small nucleoli, and indented nuclear contours. B: An aspirate smear demonstrates the identical dimorphic blast population composed of monocytes and myeloblasts (open and closed arrows, respectively). A: Blood smear reveals a particular dimorphic blast inhabitants consisting of immature nucleolated myeloblasts and mature monocytes. B: Aspirate smear stained with butyrate esterase shows positive staining in only the larger sized monocytic blast population. A: Blood smear shows a dual population of small and huge blasts, myeloblasts and monoblasts, respectively. On the left aspect are three mature monocytic blasts characterized by large size, low nuclear-to-cytoplasmic (N:C) ratios with considerably condensed chromatin, absent nucleoli, irregularly folded nuclear contours, and vacuolated, finely granular, neutral-staining cytoplasm. The proper higher nook of the slide accommodates three myeloblasts characterized by medium-size, larger N:C ratios, open chromatin, and scant cytoplasm. A small mature lymphocyte with closed chromatin is present in the best lower nook. B: Myeloperoxidase staining demonstrates sturdy granular cytoplasmic staining in a subpopulation of blasts. Undifferentiated monoblasts with excessive N:C ratios, open chromatin, nucleoli, and basophilic-staining cytoplasm are present in the upper panels, promonocytes within the middle panels, and differentiated monocytic blasts with closed chromatin pattern and lobulated nuclei are proven within the lower panels. B: Bone marrow aspirate features promonocytes characterised by massive size with low nuclear-to-cytoplasmic (N:C) ratios, nuclei with reasonably open chromatin, folded nuclear contours (some kidney bean-shaped), absent nucleoli, and agranular, slightly basophilic-staining cytoplasm. For comparison, an arrow points to a small mature lymphocyte with larger N:C ratio and condensed chromatin. A: this peripheral smear exhibits leukocytosis consisting of enormous undifferentiated blasts with low to moderate N:C ratios and basophilic-staining cytoplasm. C: Butyrate esterase stains are unfavorable on this specific case of acute monoblastic leukemia. A benign histiocyte situated near the bottom of the slide serves as inner constructive management. B: Butyrate esterase stains present localized positivity restricted to the perinuclear granules, confirming the monocytic origin for this case of acute monoblastic leukemia with heavily granulated blasts. A: Increased cellularity and architectural distortion, similar to swirling and lining up of individual marrow cells (so-called Indian filing), counsel the presence of significant bone marrow fibrosis. B: Large, monotonous-appearing, wide-spaced, immature hematopoietic cells that substitute the complete marrow cavity. E and F: Immunohistochemistry for lysozyme stains with equal intensity in each the benign histiocytes and leukemic monoblasts. B: A bone marrow aspirate smear exhibits monotonous sheets of monoblasts displaying open chromatin with multiple prominent nucleoli and vacuolated, basophilic-staining cytoplasm. A: Monoblasts encompass a large, benign histiocyte with long tentacles of cytoplasmic projections filled with dark-staining pigment (likely iron) on this case of acute monoblastic leukemia. B: In the identical case, the 2 decrease cells are monocytic leukemic blasts and the bigger cell in the upper space is a benign histiocyte. Histiocytes, normally "innocent" benign bystanders in marrow illnesses, are characterized by oval-shaped nuclei, smooth nuclear contours, "bland" chromatin patterns, and ample neutralstaining cytoplasm. C: Positive butyrate esterase staining is seen within the quite a few leukemic monoblasts (on the right) and a benign histiocyte (long arrow). A peripheral blood smear shows two circulating promonocytes and a small mature lymphocyte. The two promonocytes are characterised by massive measurement, low N:C ratios, distinctly lobulated nuclear contours, and ample "agranular" neutral-staining cytoplasm. B: A high-power view of a bone marrow aspirate smear reveals monoblasts with bilobed nuclei reminiscent of the microgranular variant of acute promyelocytic leukemia.
Risperdal 2 mg with visaThere are pores and skin naevi from puberty and a predisposition to basal cell carcinoma in sun-exposed pores and skin symptoms yeast infection buy risperdal 2 mg low cost, medulloblastoma and ovarian fibromas medications related to the female reproductive system cheap risperdal 3mg with mastercard, and so on medicine 6 clinic purchase 4mg risperdal. There are haemangioblastomas of the retina and cerebellum symptoms heart attack purchase risperdal 3mg fast delivery, early onset renal carcinomas and phaeochromocytomas (tumours of sympathetic nervous tissue). There is a subset with a sample of high expression of some genes and low expression of others that Genes reply nicely to therapy and Each row is another subset with the a special reverse pattern that exhibits gene a poor response. Initiation and progression of cancer involves acquisition of a quantity of genetic changes that convey selective advantages on cells and leads to progressive lack of development management, combined with the ability to grow at distant sites (see Chapter 55). There is a long history of examine of tumours on the genetic level and well-established genetic checks used routinely within the prognosis of most cancers. It is hoped that genomically guided therapeutics will permit for extra exact targeting of drugs, with improved outcomes and discount of unwanted facet effects. Some chromosomal rearrangements are extremely attribute of specific malignancies. Performing cytogenetic research is particularly troublesome for solid tumours and can be time consuming and expensive. The high sensitivity of these molecular strategies following treatment allows detection of small populations of tumour cells, predicting relapse, lengthy before any scientific indication. Genetic testing and remedy of most cancers Tumours that look the identical microscopically could also be very different of their development patterns and response to therapy. In some instances, genetic checks are helpful in predicting their probable response, permitting therapeutic agents to be focused extra exactly toward the tumours most likely to be controllable. Some such differences are attributable to certain genetic modifications themselves, so that discovery of a tumourspecific genetic change can counsel new therapies. Genetic testing of tumour specimens is now commonly carried out previous to initiation of remedy with these medicine. Analysis of cancer genomes Rapid sequencing of whole genomes (Chapter 68) provides the potential for characterizing those particularly of cancer cells. The aim is to provide an inventory of the various sorts of mutation that accumulate in cancer cells and contribute to their abnormal behaviour. Any variations between the latter point out genetic abnormalities within the tumour, and should play a task in contributing to the tumour phenotype. It is hoped that this approach will lead to discovery of recent genetic markers that will eventually make clear tumourigenesis, as well as identify new diagnostic and prognostic tools, and new drug targets. Genetic testing in most cancers analysis Chromosomal research of cancer cells typically reveal multiple abnormalities in chromosome number and construction. However, only 9 years later Archibald Garrod published Inborn Errors in Metabolism, proposing a relationship between human inheritance and metabolic disease and thereby laying the foundations of human biochemical genetics. He proposed that such patients lack exercise of a specific enzyme necessary to perform a particular biochemical response. Noting that 60% of affected people have been the offspring of unaffected first cousins, he proposed the defect can be inherited as a recessive. The black pigment turned out to be oxidized homogentisic acid, a by-product of tyrosine; its breakdown is affected in these patients and the condition is indeed inherited as a recessive. Of the 20 amino acids required as constituents of human proteins, 11 could be synthesized in the body, however the remaining nine are important dietary constituents. These are: histidine, isoleucine, leucine, lysine, methionine, phenylalanine, threonine, tryptophan and valine. Some enzymes acquire organic activity only after affiliation with cofactors and in some circumstances. Effectofmolecularsize Enzyme defects during which the substrate is a readily diffusible, small molecule, can affect parts of the body distant from the location of motion of the enzyme. When the substrate or product is a non-diffusible macromolecule corresponding to a mucopolysaccharide, pathological adjustments are generally restricted to the location of action of the enzyme (Chapter 62). Pleiotropiceffects A single-gene defect can have a number of phenotypic outcomes (known as pleiotropy) when the substrate and/or product of the enzyme for which that gene codes contributes to a number of features. A single-gene defect may cause malfunction of more than one pathway if a number of enzymes require the same cofactor, or share a typical subunit, or the same activating, processing or stabilizing protein. In I-cell illness, the failure to add mannose 6-phosphate to a number of enzymes blocks lysosomal uptake of all of them. Problems requiring quick consideration As a basic rule, if any of the problems described on this chapter are suspected, the recommendation is diagnostic testing and a management plan. Phenotypichomology the pathological features because of a defect in one enzyme may be proven by different diseases in the occasion that they perform in the identical space of metabolism, as with the mucopolysaccharidoses (Chapter 62). Partial enzyme deficiencies can additionally be complicated when their penalties symbolize subsets of full scientific phenotypes. Enzyme deficiencies and illness Generalityofrecessivestatus Most of our 200 or so at present recognized inborn errors of metabolism are inherited as recessives, as a end result of most enzymes are produced in appreciable excess and the 50% deficiency in a mutant heterozygote goes unnoticed. However, if the response is a rate-limiting step, or the product of the faulty gene is a part of a multimeric complicated, the disorder can manifest in the heterozygous state and be classed as dominant. Some of the enzymes involved in porphyrin synthesis are examples of this principle (see Chapter 61). Dark pigment is deposited within the earwax, cartilage, together with the pinna, and joints (ochronosis), inflicting arthritis. Newborns current with vomiting and abnormal muscle tone, continuing to demise within a few weeks. Management Consumption of enormous volumes of water, alkalinization of the urine and use of cystine chelating agents corresponding to penicillamine. The latter conversion is carried out by cystathione synthase (or cystathione -synthetase), deficiency of which is the primary reason for homocystinuria, with prior elevation of serum homocysteine. Methionine synthase requires a methyl spinoff of vitamin B12 (methylcobalamin) as cofactor. Homocystinuria is associated with seizures, thromboembolic episodes and osteoporosis. Management Cystathione synthase requires pyridoxal phosphate as a cofactor and administration of pyridoxine can often ameliorate the condition Most are partially or fully treatable with excessive doses of vitamin B12. A vegan diet can create phenocopies of homocystinuria because of dietary deficiency of vitamin B12. Tyrosinaemia Hereditary tyrosinaemia Type 1 is relatively common (1/700) in French-Canadians within the Saguenay-Lac Saint Jean area of Quebec (rare elsewhere), attributable to a splice donor website mutation in intron 12 of fumarylacetoacetate hydrolase. It is detectable in infants, whose urine has the odour of cabbages, due to their excretion of succinylacetone, a mitochondrial toxin. All are ultimately broken down by glycolysis, following conversion to the monosaccharides, glucose, galactose and fructose, or saved as glycogen. The failure to utilize these three sugars successfully accounts for most defects of carbohydrate metabolism. All are uncommon and their management is usually aimed toward promoting alternative pathways of energy era.
Generic risperdal 3mg free shippingIncreased danger of myopathy in severe renal failure as a end result of medicine qhs order risperdal 4 mg with mastercard elevated daptomycin ranges medications on carry on luggage order 3 mg risperdal visa. In preclinical studies it has been proven that renal clearance of darbepoetin is minimal (up to 2% of whole clearance) treatment 100 blocked carotid artery cheap 3mg risperdal overnight delivery. Once a pre-filled pen has been faraway from the fridge and dropped at treatment carpal tunnel discount risperdal 2 mg without prescription room temperature it have to be used within 7 days. Antifungals: focus elevated by ketoconazole � keep away from concomitant use; avoid with itraconazole. Antivirals: avoid concomitant use with fosamprenavir, atazanavir, indinavir, lopinavir, ritonavir, saquinavir and tipranavir. Antimalarials: focus of lumefantrine elevated; possibly increases focus of quinine. Antivirals: avoid with boceprevir or telaprevir; concentration lowered by efavirenz � regulate dose; concentration of both medicine elevated with indinavir; focus lowered by lopinavir, additionally focus of lopinavir elevated � keep away from; concentration of maraviroc increased, contemplate lowering dose of maraviroc; focus lowered by saquinavir. Lipid-lowering medication: probably increased risk of myopathy with atorvastatin and rosuvastatin, keep away from with rosuvastatin; probably increases pravastatin focus; keep away from concomitant use with simvastatin. Following a single oral dose of [14C]-labelled dasatinib, approximately 89% of the dose was eliminated inside 10 days, with 4% and 85% of the radioactivity recovered in the urine and faeces, respectively. Most common opposed results of dasatinib embrace fluid retention, gastrointestinal disturbances, and bleeding. Fluid retention could also be severe, and may end up in pleural and pericardial effusion, pulmonary oedema and ascites. It is quickly metabolised within the liver and the main metabolite, daunorubicinol, can be energetic. It is excreted slowly in the urine, primarily as metabolites with 25% excreted inside 5 days. Manufacturer has not carried out any studies in renal failure but because of low renal clearance use doses as for regular renal function. Deconjugation of the glucuronidates within the intestine and subsequent enterohepatic recycling are more probably to occur. It is excreted mainly in the faeces via bile, as metabolites and as unchanged drug. Theophylline: focus of theophylline elevated, consider decreasing theophylline dose. Increased risk of potentially deadly renal failure and cytopenias in sufferers with other comorbidities who additionally had a complicated haematological condition. During scientific trials, increases in serum creatinine of >33% on 2 consecutive events (sometimes above the higher limit of the normal range) occurred in about 36% of sufferers. Cases of acute renal failure have been reported following postmarketing use of deferasirox. Since deferiprone is eradicated mainly through the kidneys, there may be an increased risk of complications in sufferers with impaired renal perform. Reddish-brown discolouration of the urine reported in 40% of thalassaemia sufferers undergoing deferiprone remedy. Deferiprone eliminated aluminium in vitro from blood samples of forty six sufferers present process chronic haemodialysis. Deferiprone eliminated the aluminium faster and extra successfully from higher molecular weight proteins than desferrioxamine. Effectiveness of deferiprone (L1) releasing the aluminium sure to plasma proteins in continual renal failure. It is 40% protein-bound and has no affinity for corticosteroid-binding-globulin (transcortin). Elimination takes place primarily via the kidneys; 70% of the administered dose is excreted within the urine. Ciclosporin: uncommon stories of convulsions in sufferers on ciclosporin and high-dose corticosteroids; increased half-life of deflazacort. Vaccines: high dose corticosteroids can impair immune response to vaccines; avoid concomitant use with live vaccines. Degarelix is injected to kind a subcutaneous depot, and the pharmacokinetics of the drug is strongly influenced by the focus of the injected solution. Retinoids: attainable elevated risk of benign intracranial hypertension, keep away from concomitant use. Following a single 150 mg dose of demeclocycline hydrochloride in normal volunteers, 44% (n = 8) was excreted in urine and 13% and 46%, respectively, were excreted in faeces in two patients inside 96 hours as active drug. Four metabolites of desferrioxamine have been isolated from urine of patients with iron overload. The following biotransformation reactions were discovered to happen with desferrioxamine: transamination and oxidation yielding an acid metabolite, beta-oxidation additionally yielding an acid metabolite, decarboxylation and N-hydroxylation yielding impartial metabolites. The urine might seem orange/red in sufferers handled with desferrioxamine for severe iron intoxication. Manufacturer advises to use with warning in renal impairment besides these on dialysis because the metal complexes are excreted through the kidney. In haemodialysis patients treated with desferrioxamine post dialysis, the half-life has been found to be extended to 19 hours between dialysis periods. Anecdotally, escalating doses of up to 2 g, three times a week have been successfully used for iron overload in sufferers on haemodialysis. In remedy of acute iron poisoning, effectiveness of treatment relies on an enough urine output. Approximately 40% of the dose is excreted in the urine and 42% within the faeces over a 10 day interval and primarily within the type of conjugated metabolites. Approximately 27% of the dose is eradicated in the urine during the first 24 hours. Less than 1% of the energetic substance is excreted unchanged within the energetic type, as desloratadine. In patients with ischaemic heart illness, infuse more slowly � increased risk of acute ischaemic event. As a peptide, desmopressin is predicted to undergo catabolism to its constituent amino acids, with subsequent recycling of the amino acid in the body pool. Rheumatic disease: - intra-articular, intrasynovial: based on preparation and dimension of joint - delicate tissue infiltration: 1. The slower metabolism of the synthetic corticosteroids with their lower protein-binding affinity could account for his or her elevated efficiency in contrast with the natural corticosteroids. Antifungals: increased danger of hypokalaemia with amphotericin � keep away from concomitant use; metabolism possibly inhibited by itraconazole and ketoconazole; caspofungin concentration possibly reduced (may have to increase dose). Antivirals: concentration of indinavir, lopinavir, saquinavir and telaprevir presumably decreased; avoid with rilpivirine; focus probably elevated by ritonavir. After metabolic transformation in the liver (hydroxylation and carboxylation), the pharmacologically inactive metabolites are utterly excreted, primarily by the kidneys (90%), but also in the bile. The primary elimination route for dexketoprofen is glucuronide conjugation in the liver adopted by renal excretion. Dexketoprofen ought to be used with warning in uraemic patients predisposed to gastrointestinal bleeding or uraemic coagulopathies.
African Palm Oil (Palm Oil). Risperdal. - What is Palm Oil?
- Decreasing symptoms of malaria.
- How does Palm Oil work?
- Are there any interactions with medications?
- Are there safety concerns?
- Vitamin A deficiency.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97083
Generic 3 mg risperdal free shippingPancuronium distributes rapidly into extracellular fluid and the initial neuromuscular blockade produced will depend upon the height drug focus on this fluid medications 247 buy risperdal 3mg amex. Since extracellular fluid volume is elevated in chronic renal failure such patients might require a larger initial dose of pancuronium and a 45% improve in dose requirement has been reported in patients with end-stage renal failure symptoms 9f anxiety discount risperdal 3mg overnight delivery. Antifungals: absorption of itraconazole and ketoconazole lowered; avoid with posaconazole symptoms tonsillitis cheap risperdal 2mg free shipping. Antivirals: concentration of atazanavir and rilpivirine reduced � keep away from concomitant use; concentration of raltegravir and saquinavir possibly increased � avoid medicine wheel wyoming 4mg risperdal. Cytotoxics: presumably decreased excretion of methotrexate; keep away from with erlotinib and vandetanib; probably decreased lapatinib absorption; presumably reduced absorption of pazopanib. Metabolites are excreted mainly (about 80%) in the urine, with the remainder being excreted in faeces via the bile. As with all opiates, use with excessive caution in sufferers with impaired renal perform. It is often detoxified by conjugation with glutathione but could accumulate after paracetamol overdosage and cause tissue injury. Circulating carboxy-terminal fragments are filtered by the kidney, but are subsequently damaged to even smaller fragments throughout tubular reuptake. Parathyroid hormone is efficiently faraway from the blood by a receptormediated process in the liver and is damaged down into smaller peptide fragments. The fragments derived from the amino-terminus are further degraded throughout the cell whereas the fragments derived from the carboxyterminus are released again into the blood and cleared by the kidney. These carboxyterminal fragments are thought to play a job in the regulation of parathyroid hormone exercise. The general exposure and Cmax of parathyroid hormone have been barely elevated (22% and 56%, respectively) in a bunch of eight male and 8 feminine subjects with mild-to-moderate renal impairment (creatinine clearances of 30 to eighty mL/min) compared with a matched group of 16 topics with regular renal function. Excretion is principally via the urine with about 70% of a dose showing as inactive metabolites. No unchanged parecoxib is discovered in the urine with solely trace quantities within the faeces. Cytotoxic brokers: lowered excretion of methotrexate (possible increased risk of toxicity); elevated threat of bleeding with erlotinib. Diuretics: elevated danger of nephrotoxicity; potential antagonism of diuretic impact; elevated risk of hyperkalaemia with potassium-sparing diuretics. Parecoxib should be used with warning in uraemic sufferers predisposed to gastrointestinal bleeding or uraemic coagulopathies. After oral administration of 3H-paricalcitol, solely about 2% of the dose was eradicated unchanged within the faeces, and no father or mother drug found within the urine. Approximately 70% of the radioactivity was eliminated in the faeces and 18% was recovered in the urine. Monitor calcium and phosphate ranges no less than monthly, extra incessantly throughout dose titration. Paricalcitol solution for injection contains 30% v/v of propylene glycol as an excipient. Isolated instances of central nervous system depression, haemolysis, and lactic acidosis have been reported as poisonous results associated with propylene glycol administration at excessive doses. Urinary excretion of unchanged paroxetine is mostly less than 2% of dose while that of metabolites is about 64% of dose. About 36% of the dose is excreted in faeces, probably through the bile, of which unchanged paroxetine represents lower than 1% of the dose. Anti-arrhythmics: probably inhibits propafenone metabolism (increased threat of toxicity). Anti-epileptics: antagonism (lowered convulsive threshold); concentration lowered by phenytoin and phenobarbital. Antipsychotics: focus of clozapine and possibly risperidone elevated; metabolism of perphenazine inhibited, cut back dose of perphenazine; presumably inhibits aripiprazole metabolism, reduce aripiprazole dose; concentration presumably increased by asenapine; increased threat of ventricular arrhythmias with pimozide � avoid. The 4 principal pazopanib metabolites account for less than 6% of the publicity in plasma. Therefore, exercise of pazopanib is principally dependent on mother or father pazopanib publicity. Antivirals: keep away from concomitant use with atazanavir, indinavir, ritonavir, saquinavir & boceprevir. In haemodialysis patients, a hundred thirty five mcg Pegasys is equivalent to a a hundred and eighty mcg dose in the common population. To cut back the incidence and severity of skin reactions, a steroid (equivalent to four mg of dexamethasone) must be given the day earlier than, the day of, and the day after pemetrexed remedy. There has been a case report of a affected person having severe rhabdomyolysis with pemetrexed in combination therapy with carboplatin. Phase I and pharmacokinetic research of pemetrexed administered each 3 weeks to advanced cancer sufferers with regular and impaired renal function. Alteration of pemetrexed excretion within the presence of acute renal failure and effusions: presentation of a case and evaluate of the literature. It is mainly excreted within the urine as disulfides, along with some S-methyl penicillamine and unchanged drug; a small amount could also be excreted within the faeces. Dose in haemodialysis is from Drug Dosage in Renal Insufficiency by Seyffart G and Drug Prescribing in Renal Failure, 5th version, by Aronoff et al. Urinalysis should be carried out weekly for the first two months of therapy, after any change in dosage, and month-to-month thereafter. Potentially hazardous interactions with different medicine Anti-arrhythmics: elevated risk of ventricular arrhythmias with amiodarone � avoid concomitant use; attainable increased danger of ventricular arrhythmias with disopyramide. Antibacterials: increased danger of ventricular arrhythmias with moxifloxacin and parenteral erythromycin � avoid concomitant use with moxifloxacin; elevated danger of ventricular arrhythmias with parenteral pentamidine and telithromycin. Antipsychotics: elevated threat of ventricular arrhythmias with amisulpride, droperidol and phenothiazines � keep away from concomitant use with amisulpride and droperidol. Antivirals: elevated threat of hypocalcaemia with parenteral pentamidine and foscarnet; elevated danger of ventricular arrhythmias with saquinavir � avoid. It is primarily excreted unchanged by the kidneys (30�90% excreted by kidneys within 24 hours). Pentostatin pharmacokinetics and dosing suggestions in sufferers with gentle renal impairment. The affected person was dialysed for four hours 1�2 hours after receiving the pentostatin to remove any remaining drug. Pentostatin treatment for a patient with continual type grownup T-cell leukaemia present process haemodialysis. Anticancer drug renal toxicity and elimination: dosing pointers for altered drug perform.
Buy generic risperdal 2 mg onlineThus symptoms testicular cancer risperdal 4 mg sale, careful parental analysis is strongly recommended earlier than genetic counseling medicine cups discount risperdal 4mg amex. References Bourneville D: Scl�reuse tub�reuse des circonvolutions c�r�brales: Idiote et epilepsie h�mipl�gique symptoms 0f parkinson disease cheap 2mg risperdal mastercard, Arch Neurol (Paris) 1:81 medicine omeprazole 20mg purchase risperdal 2mg with mastercard, 1880. Report of the diagnostic standards committee of the National Tuberous Sclerosis Association, J Clin Neurol 7:221, 1992. Saada J, et al: Prenatal diagnosis of cardiac rhabdomyomas: Incidence of associated cerebral lesions of tuberous sclerosis advanced, Ultrasound Obstet Gynecol 34: a hundred and fifty five, 2009. A and B, Two youngsters with fibrous-angiomatous lesions in the nasolabial folds and cheeks. A and B, Gingival and subungual fibromata (arrow in A factors to subungual fibroma). Neurofibromas not often develop in kids youthful than 6 years of age but are present in 48% of 10-year-olds and 84% of 20-year-olds. They might improve in dimension and number at puberty, throughout being pregnant, and between 50 and 70 years of age. The complications of neurofibromatosis may be divided into these which are structural (macrocephaly, segmental hypertrophy, scoliosis, pseudoarthrosis, cardiac defects, vascular stenoses and aneurysms), these which are practical (seizures, speech and learning issues, hypertension, mental deficits), and those that relate to neoplasia. Screening for structural and functional issues may be accomplished effectively via comprehensive physical evaluation each 6 months. Rather, clinicians following affected people ought to keep a high index of suspicion and consider particular indicators and symptoms as they develop. All newly recognized patients should have an ophthalmologic examination after which be adopted yearly through 6 years of age to rule out an optic pathway glioma; thereafter, their incidence is uncommon. Thirty-nine % of kids with an optic pathway glioma involving the optic chiasm develop precocious puberty. The quickly progressive (dysplastic) form of scoliosis nearly at all times develops between ages 6 and 10 years. Caf� au lait macules over 5 mm in best diameter before puberty and over 15 mm following onset of puberty. Ninety-nine p.c have six or more macules greater than 5 mm in diameter by 1 year of age. Neurofibromas (a heterogeneous benign peripheral neural sheath tumor) occurring as discrete dermal masses, focal cutaneous or subcutaneous growths, dumbbell-shaped intraforaminal spinal tumors, or diffuse plexiform neurofibromas. Seizures or electroencephalographic abnormalities in roughly 20%; mental incapacity in 2% to 5%, with learning disability, hyperactivity, or speech problems in 50%; cerebral vascular compromise; headaches; hydrocephalus; enlarged corpus callosum; scoliosis, often early, severe and progressive; pectus excavatum; hypoplastic bowing of decrease legs, with pseudoarthrosis at birth; osseous lesions with localized osteosclerosis, rib fusion, spina bifida, absence of patella, dislocation of radius and ulna, native overgrowth, and scalloping of vertebral bodies with deformed pedicles; sphenoid wing dysplasia; osteopenia and osteoporosis; cutaneous nevi, lipomata, angiomata, neurofibroma in kidney, stomach, heart, tongue, and bladder; syndactyly; glaucoma, ptosis, corneal opacity, doubtlessly malignant melanoma of iris; malignant peripheral nerve sheath tumors; precocious puberty; verrucous nevus; pheochromocytoma; pruritus; pulmonic stenosis; vascular hyperplasia of the intima and media leading to Moyamoya progressive cerebral vascular disease, Neurofibromatosis Syndrome 665 Survival is shortened, with a mean age of sixty one. Whole gene deletion is related to large numbers and early appearance of cutaneous neurofibromas, more extreme cognitive involvement and sometimes somatic overgrowth, giant hands and ft, and dysmorphic facial options. References Von Recklinghausen F: Ueber die multiplen Fibroma der Haut und ihre Beziehung zu den multiplen Neuromen, Berlin, 1882, Hirschwald. National Institutes of Health Consensus Development Conference Statement: Neurofibromatosis. DeBella K, et al: Use of the National Institutes of Health criteria for analysis of neurofibromatosis 1 in kids, Pediatrics 105:608, 2000. Kaas B, et al: Spectrum and prevalence of vasculopathy in pediatric neurofibromatosis type 1, J Child Neurol 28:561, 2013. Note the caf� au lait spots, axillary freckling, and pectus excavatum (A�C) and Lisch nodules (D). Fibrous dysplasia of the bone and both "caf� au lait" macules or a hyperfunctioning endocrinopathy is sufficient to establish a analysis. Craniofacial lesions develop before 5 years of age and will lead to cranial nerve compression with serious penalties similar to blindness or deafness. Any bone can be involved, however the cranium base and the proximal femur are most commonly concerned. The sexual precocity within the feminine is often unusual in character, with menstruation earlier than improvement of breasts, typically with no pubic hair. In boys, bilateral or unilateral testicular enlargement (Leydig cell hyperplasia) with penile enlargement, and secondary sexual traits develop. The accelerated maturation coincident with sexual precocity might lead to early attainment of full stature, in order that grownup top could be relatively short. Thyrotoxicosis happens incessantly, and postoperative thyroid storm has occurred on rare events. Mutations at position Q227 and V224 have been identified in isolated fibrous dysplasia. This explains the remark that the endocrinologic abnormalities in McCune-Albright syndrome are the results of autonomous hyperfunction of the endocrine glands quite than being centrally mediated, although puberty may become central secondarily. The variable medical expression is determined by the relative number of mutant cells in addition to by the tissues and areas of the body concerned. Multiple areas of fibrous dysplasia, often unilateral, most commonly in lengthy bones and pelvis; can also embody cranium, facial bones (causing macrocephaly and facial asymmetry), ribs, and occasionally the backbone; may lead to deformity, pain, fractures, scoliosis. Irregular brown pigmentation, referred to as caf� au lait spots with "coast of Maine" borders, mostly over sacrum, buttocks, nape of the neck, and upper backbone; unilateral in approximately 50% of patients; the pattern of the pigmentary changes often follows the Blaschko strains. Albright F, et al: Syndrome characterised by osteitis fibrosa disseminata, space of pigmentation and endocrine dysfunction, with precocious puberty in females: Report of five circumstances, N Engl J Med 216:727, 1937. It has been confused with ParkWeber syndrome, by which vital arteriovenous fistulas are a characteristic. There could also be disproportionate growth, which requires epiphyseal fusion or removal of the suitable phalanx. Leg swelling can be bothersome, and ulcers and other persistent pores and skin difficulties may occur. However, within the rare situation in which the extremity reaches gigantic proportions or secondary clotting difficulties happen, amputation is critical. Vascular malformations of the viscera, brain, eyes, urinary and gastrointestinal tracts, and other areas ought to at all times be appeared for in this extremely variable disorder. Magnetic resonance imaging is the most effective noninvasive imaging approach to evaluate patients with vascular malformations. Congenital or early childhood hypertrophy of often one, but often a couple of, limb; the decrease limb is involved in 95% of instances, the higher limb in 5%, and both are concerned in 15%. Asymmetric facial hypertrophy; microcephaly; macrocephaly brought on by a big brain; intracranial calcifications; eye abnormalities similar to glaucoma, cataracts, heterochromia, and a Marcus Gunn pupil. Macrodactyly, disproportionate growth of the digits whether or not massive or small; syndactyly; polydactyly; oligodactyly; congenital hip dislocation, atrophy. Hyperpigmented nevi and streaks, neonatal and childhood ulcers and vesicles, cutis marmorata, telangiectasia. Visceromegaly; capillary malformation of the intestinal tract, urinary system, mesentery, and pleura; aberrant major blood vessel; lymphectasia; insignificant arteriovenous fistula.
Buy risperdal 2 mg mastercardDeepest layer of the transversospinal system with brief fibers taking an especially transverse course medicine to help you sleep risperdal 2 mg mastercard, thereby offering stronger rotation medicine x topol 2015 buy discount risperdal 2mg on line. The portion of the occipitofrontalis which passes from the galea aponeurotica to the eyebrows symptoms joint pain and tiredness risperdal 2mg discount. The portion of the occipitofrontalis which passes from the supreme nuchal line to the galea aponeurotica treatment 4 sore throat order risperdal 3mg without prescription. Displaceable, helmet-like, superficial tendon for the two elements of the epicranius. It lies towards the periosteum and is hooked up to the supreme nuchal line and to the external occipital protuberance. It closes the eyelids and assists the move of tears into the lacrimal sac and into the nostril. Fibers located within the eyelids passing from the medial palpebral ligament and the adjacent bones to the lateral palpebral ligament. Arises from the medial palpebral ligament and adjacent bones, thus encircling the eye. It curves across the lacrimal canaliculus, extends partially behind the lacrimal sac and radiates into the palpebral a half of the orbicularis oculi muscle beneath the medial palpebral ligament. Muscle medial to the corrugator supercilii that radiates from the orbicular oculi into the skin of the medial a half of the eyebrow. The main part of the orbicularis oris including the portion which takes a hook-like bend externally below the purple portion of the lips. Transverse muscular connection between the proper and left depressor anguli oris muscle tissue below the chin. Closes jaw and, together with the temporal and medial pterygoid muscle tissue, determines the degree of masticatory energy. Arises from the zygomatic arch proximal to the mandibular joint and discocapsular system. Action: Together with fibers of the temporal muscles, it ensures lateral stabilization of the discocapsular system throughout laterotrusal movement. Action: Elevation and retraction of the mandible, fixation of the pharynx when swallowing; cf. Arises by two heads (variant: three heads), one from the discocapsular system, the opposite from the pterygoid fossa. The superior head determines the velocity at which the discocapsular system is pulled again into place. It programs obliquely downward and backward and is a synergist to the temporalis and masseter muscle tissue. It lies on the buccinator muscle and extends from the angle of the mouth deeply so far as the pharyngeal constrictor muscle. Fascia covering the masseter muscle, part of which attaches below the parotid on the higher finish of the zygomatic arch. External connective tissue investment of the temporalis muscle between the superior temporal line and the zygomatic arch. Arches to connect the 2nd to 5th cervical vertebrae with the lower cervical and higher thoracic vertebrae. Its fibers additionally lengthen from the vertebral our bodies to the transverse processes with the C6 transverse process as the central point. An intermediate tendon situated above the jugular vein divides it into two bellies. Superficial layer of cervical fascia that surrounds the sternocleidomastoid and trapezius muscle tissue. It is attached to the anterior margin of the manubrium, the clavicle and the mandible. Layer that spreads between the 2 omohyoid muscle tissue and is connected to the posterior margin of the manubrium and clavicle. Layer that lies between the vertebral column and pharyngeal constrictors as nicely as the esophagus, covers the scaleni muscle tissue and accommodates the sympathetic trunk and phrenic nerve. Connective tissue investing the neurovascular bundle (carotid artery, jugular vein and vagus nerve) and continuous with the pretracheal layer. It has an intermediate tendon which acts on the lesser horn of the hyoid bone via a connective tissue sling. It accompanies the posterior belly of the digastric muscle and might cross by way of it through a fissure. Muscle that occasionally (4%) crosses the pectoralis major muscle parallel and proximal to the sternum. Continuation of the internal intercostal muscle tissue from the rib angle to the vertebrae. Internal portion of the interior intercostal muscles separated by the intercostal vessels. Situated on the internal surface of the anterior thoracic wall, it radiates obliquely upward from the sternum to costal cartilages 2-6. Medial a part of the diaphragm arising from the lumbar vertebral bodies, intervertebral discs and fibrous arches. It covers the pectoralis main muscle, is hooked up to the clavicle and sternum and is continuous with the axillary fascia. Tendinous arch between the body and transverse strategy of L1 or L2 forming the passageway for the psoas muscle. Tendinous arch over the quadratus lumborum muscle between the transverse means of L1 and the twelfth rib. Membrane that replaces the exterior intercostal muscle tissue anteriorly between the costal cartilages. Covering of the rectus abdominis muscle fashioned by the aponeuroses of the flat abdominal muscles. Connective tissue fibers arching downward to the pubis on the medial attachment of the inguinal ligament. Curved band of fibers passing upward from the medial attachment of the inguinal ligament and forming the medial lining of the superficial inguinal ring. Group of fibers of the exterior oblique aponeurosis ascending obliquely medial to the superficial inguinal ring. Group of fibers of the external oblique aponeurosis ascending lateral to the superficial inguinal ring. Fibers arching from the aponeurosis of the transversus muscle into the pectineal ligament. Elastic band arising from the belly fascia and linea alba and increasing sling-like onto the penis. Weak space of the back bordered by the latissimus dorsi, exterior abdominal indirect m. Inner inguinal ring on the transition of the transversalis fascia into the internal spermatic fascia.
References - Haldar P, Pavord ID, Shaw DE, et al. Cluster analysis and clinical asthma phenotypes. Am J Respir Crit Care Med 2008; 178: 218-224.
- Harvey S, Harrison DA, Singer M, et al: Assessment of the clinical effectiveness of pulmonary artery catheters in management of patients in intensive care (PAC-Man): A randomised controlled trial, Lancet 366:472-477, 2005.
- Magon N, Kalra S: The orgasmic history of oxytocin: love, lust, and labor, Indian J Endocrinol Metab 15(Suppl 3):S156nS161, 2011.
- Bleiziffer S, Eichinger WB, Hettich I, et al Prediction of valve prosthesis-patient mismatch prior to aortic valve replacement: which is the best method? Heart 2007; 93:615-620.
- Whitehouse RW, Batterbury M, Jackson A, Noble JL. Prediction of enophthalmos by computed tomography after iblowouti orbital fracture. Br J Ophthalmol 1994;78:618-620.
- Turunen A: Spinal changes in patients with congenital aplasia of the vagina, Acta Obstet Gynecol Scand 46:99n106, 1967.
- Purkayastha S, Tekkis P, Athanasiou T, et al. A Comparison of Open vs. Laparoscopic abdominal rectopexy for full-thickness tectal prolapse: a meta-analysis. Dis Colon Rectum 2005;48:1930-40.
|

