Selegiline
Thomas W. Sadler, Ph.D. - Senior Genetics Scholar
- Greenwood Genetic Center
- Greenwood, South Carolina
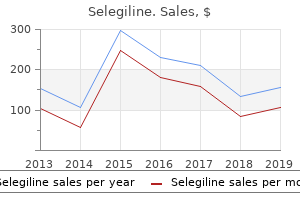
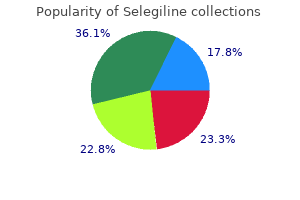
Cheap selegiline 5 mg otcEven in the scenario of a provoked thrombosis symptoms gluten intolerance purchase 5mg selegiline, an in depth family history must be documented for early-onset stroke; early myocardial infarction; and blood clots in the veins medications54583 buy selegiline 5mg mastercard, arteries treatment gonorrhea generic 5mg selegiline fast delivery, or lungs medicine purchase 5mg selegiline amex. The pivotal position of the endothelium in sustaining a steadiness between antithrombotic and prothrombotic activities, as influenced by endotoxins, viruses, and immunomodulatory cytokines. The neonate is relatively deficient in most procoagulant and anticoagulant proteins. Blood move characteristics within the new child are unique due to the high hematocrit, small-caliber vessels, low blood pressure, and particular areas of vascular fragility. The levels of most procoagulant and anticoagulant proteins increase throughout gestation; subsequently, probably the most immature toddler has the bottom levels of these proteins and is on the highest danger for either bleeding or thrombotic problems. Vitamin K is a fat-soluble vitamin that induces the post-translational -carboxylation of the vitamin K-dependent substances (factors 2, 7, 9, and 10; protein C; and protein S). This carboxylation step occurs after the protein is synthesized within the liver and should occur for the vitamin K-dependent coagulation issue to bind calcium, the bridge to the membrane surface on which these proteins type complexes with different members of the clotting cascade and catalyze subsequent reactions. Vitamin K deficiency successfully renders these proteins unable to bind to a floor. Most of the vitamin K in adults originates from the food regimen and from bacterial production within the gut. Such infants may experience diffuse bleeding and even central nervous system hemorrhage at 3-5 days of life. In the evaluation of bleeding in a new child, the clinician ought to Physical Examination an important determination is whether or not or not the affected person appears acutely or chronically ill, together with very important signs and progress parameters. The nose should be examined for ulcers or anatomic bleeding websites, and the center ought to be examined for the presence of murmurs (as occur in anemia and endocarditis). Joints should be examined for persistent arthropathy (as happens in hemophilia) or joint laxity (as happens in Ehlers�Danlos syndrome), and the extremities are examined for thumb or radial anomalies (thrombocytopenia�absent radius syndrome, or Fanconi anemia). The abdomen and lymph nodes should be examined for the presence of hepatosplenomegaly and adenopathy. The examination of the pores and skin should embody a search for pallor, hematomas, petechiae, ecchymoses, telangiectasias, poor wound therapeutic (large or irregular scars), lax (loose) skin, and varicose veins (possible deep venous thrombosis). Petechiae are pinpoint, flat, darkish pink lesions brought on by capillary bleeding into the pores and skin. All information are expressed because the imply followed by the upper and decrease boundaries encompassing 95% of the conventional population. All values offered as the imply by the higher and decrease boundaries encompassing 95% of the population. Hematomas are accumulations of blood within the pores and skin or deeper tissues; in the skin, hematomas are raised and palpable. Bruises must be described intimately, including whether or not hematomas are related to bruises and whether or not petechiae are present. Purpura refers to any group of disorders characterised by the presence of dark-red, purplish, or brown lesions of the skin and mucous membranes. The discoloration is attributable to the leakage of purple blood cells from affected vessels. Purpuric lesions can be brought on by abnormalities of the platelets, of coagulation proteins, or of vessel walls. Coagulation Screening Tests After obtaining a history and performing a physical examination, the clinician must determine the need for a hemostatic evaluation. The history is more likely to be the most sensitive screening device for a significant bleeding dysfunction, though its use in a very younger child, particularly before toddler age, is proscribed and a spotlight should shift to the perinatal and household history. For patients with medical clues of a coagulation disorder, the initial screening studies should assess the clotting components and platelet operate. When insensitive laboratory reagents fail to detect clinically vital deficiencies (most frequent in mild factor 9 deficiency). Epistaxis (1) Duration, frequency, seasonal tendency (2) Associated trauma (nose choosing, allergy, infection) (3) Resultant anemia, emergency division evaluation, cautery b. Oral (gingiva, frenulum, tongue lacerations, bleeding after tooth brushing, after dental extractions requiring sutures/ packing) c. Bruising (number, sites, size, raised [other than extremities], spontaneous versus trauma, knots within middle, skin scarring) d. Musculoskeletal (1) Hemarthroses, unexplained arthropathy (2) Intramuscular hematomas b. Deep (1) Circumcision (2) Central nervous system bleeding (3) Gastrointestinal bleeding (4) Cephalohematoma (5) Unexplained anemia or hyperbilirubinemia (6) Delayed cord separation, bleeding after cord separation c. Onset, period, quantity (number of pads), frequency, persistence after childbirth b. Bleeding at childbirth (onset, length, transfusion requirement, history of traumatic supply, recurrences with subsequent pregnancies, spontaneous abortions) E. The gadgets simply listed should be applied to immediate members of the family, especially a historical past of straightforward bruising, epistaxis, excessive bleeding after surgery, menorrhagia, excessive bleeding after childbirth, or a family historical past of others with identified or suspect bleeding issues. Bleeding Time the bleeding time is an indirect measure of platelet quantity and a more direct measure of platelet function, vascular integrity, and platelet interplay with the vascular subendothelium. As such, the bleeding time should be abnormal in patients with thrombocytopenia, platelet operate abnormalities, abnormal collagen (Ehlers�Danlos syndrome), and von Willebrand disease. Platelet Function Analysis Platelet function evaluation was initially recommended as a screening take a look at for von Willebrand illness and platelet operate defects. Its sensitivity and specificity are inadequate for prognosis, but it could have utility as a display screen for extreme platelet function defects in very small infants where fast outcomes are wanted and size prohibits collection of huge volumes of blood wanted for platelet aggregation testing. Thrombin Time and Reptilase Time the thrombin time and reptilase time are tests that measure the conversion of fibrinogen to fibrin. The thrombin time is delicate to heparin effect, whereas the snake venom reptilase time remains regular in the presence of heparin. Both the thrombin time and the reptilase time are prolonged by uremia, by dysfibrinogenemia, and by low fibrinogen levels (<75 mg/dL). Common complaints embrace prolonged, frequent nosebleeds; gum bleeding; prolonged bleeding after tooth extraction; menorrhagia; and easy bruising with or with out petechiae formation. Mucocutaneous bleeding is normally related to abnormalities of platelet quantity or operate, of platelet cofactors, or of the vessel wall. After exposure to the viral infection, an antibody that binds to the platelet membrane develops, resulting in the untimely destruction of the antibody-coated platelets in the spleen. To rule out heparin impact, the thrombin time is in contrast with the reptilase time. If the thrombin time is considerably longer than the reptilase time, heparin is current within the pattern. The household should be suggested that the kid must avoid actions that enhance the risk of head damage.
Buy generic selegiline 5mgAmblyopia have to be handled with occlusion of the sound eye medications containing sulfa generic 5 mg selegiline, often for a quantity of years nail treatment order selegiline 5mg free shipping, until secure visual acuity may be demonstrated symptoms ruptured spleen buy selegiline 5mg line. Several genes inflicting main congenital glaucoma treatment hyperthyroidism discount 5mg selegiline visa, often autosomal recessive, have been recognized. The cornea may be cloudy due to edema ensuing from elevated intraocular strain. The cornea additionally enlarges and the axial length of the eye could improve with elevated intraocular pressure. If glaucoma presents after the age of 5 years, it is called major juvenile open-angle glaucoma. The natural historical past of untreated main congenital glaucoma is blindness resulting from progressive corneal opacification and optic nerve damage. Treatment is surgical although eye stress reducing drugs such as topical blockers and topical or oral carbonic anhydrase inhibitors could also be used as temporizing measures. Even with treatment final visual acuity is worse than 20/50 in more than 50% of the sufferers. Secondary glaucoma might present equally to major glaucoma however is associated with other components corresponding to ocular trauma, irritation, extended steroid use, or cataract. The differential analysis of congenital glaucoma contains situations that show corneal opacities (Table 32. Photophobia is noticed in infants with corneal trauma, corneal deposits, cystinosis, and irritation (uveitis). Corneal opacification can be found in infants with corneal dystrophies, metabolic storage diseases corresponding to mucopolysaccharidoses, and forceps-related obstetric trauma. The diagnosis of primary congenital glaucoma or secondary glaucoma is usually confirmed by performing an examination with the affected person underneath anesthesia. The baby needs to be quiet and very cooperative in order to get an correct intraocular pressure reading and a careful examination of the cornea and anterior phase constructions. The prognosis rests on a constellation of abnormal ocular findings, together with elevated intraocular stress, corneal enlargement, anomalies of the drainage angle, and indicators of harm to the optic nerve along side medical history. Inflammation can contain any or all of those constructions, and phrases similar to iritis, iridocyclitis, choroiditis, and chorioretinitis are used to designate which portion of the uveal tissue is involved. Anatomic location similar to anterior, posterior, intermediate, or panuveitis are useful in determining etiology (Table 32. A cataract and/or glaucoma may end result from inflammation within the eye or persistent use of steroids used to quiet the irritation. The pupil may have an irregular shape on account of adhesions to the underlying lens (posterior synechiae). Because uveitis may be brought on by infections, trauma, autoimmune issues, and may be idiopathic, analysis of the purpose for the uveitis requires a thorough pediatric bodily examination in addition to supplementary radiologic and laboratory testing. In boys, haplotype testing for human leukocyte antigen B27 could also be indicated due to the affiliation between iritis and pauciarticular arthritis that may later evolve into ankylosing spondylitis. The management of iritis in children is the elimination of intraocular irritation. In some cases of noninfectious uveitis, local therapy with topical corticosteroid drops or periocular corticosteroid injections could control the inflammation. Short programs of corticosteroids could additionally be used, however corticosteroid-sparing medication are the 1st-line therapy for long-term use because of the many unwanted effects of corticosteroids. Toxoplasmosis caused by the intracellular parasite Toxoplasma gondii is the most typical explanation for posterior uveitis in youngsters. Most ocular toxoplasmosis within the pediatric age group might be acquired from the mom during being pregnant. In some cases, the an infection is inactive at delivery and goes unrecognized until irritation occurs. The analysis of toxoplasmosis is predicated on clinical findings, intracranial calcification in some kids, and laboratory exams for particular immunoglobulin G and immunoglobulin M antibodies. When treatment is indicated, it entails using 1 or extra antimicrobial medicine. The most common remedy consists of combination remedy with pyrimethamine and sulfadiazine. Intravitreal clindamycin with dexamethasone may be as effective as systemic therapies. These entities include retinoblastoma, leukemia, lymphoma, juvenile xanthogranuloma, and an intraocular foreign body. The lacrimal gland, positioned in the superotemporal orbit, is the primary producer of tears; accent lacrimal glands in the upper eyelid supplement its output. The lacrimal drainage apparatus begins with puncta on the nasal side of the upper and decrease eyelid margins. The puncta proceed as canaliculi that course nasally to empty into the lacrimal sac. Typically, the infant has epiphora and a mucopurulent discharge that causes matting of the eyelids starting at about 1 month of age. Pressure applied to the lacrimal sac with a finger or cotton swab often ends in reflux of cloudy fluid from the puncta. Topical antibiotics can be utilized to lower purulence however this likely leads to resistant organisms. Lacrimal sac therapeutic massage may push fluid via the mucosal membrane and thereby open the duct, but the strain applied to the lacrimal sac needs to be forceful. A silicon stent may be placed to preserve an open duct, which increases the success of long-term patency. These situations require surgical procedure to re-form the canalicular system and puncta and repair the fistula if current. Chronic tearing occurs in congenital glaucoma in addition to blepharospasm and photophobia. These infants current with a bluish mass in the nasoorbital region under the medial canthal tendon. An encephalocele or dermoid cyst can also appear to be a bluish mass however will lie above the medial canthus. On event, the dilated sac is accompanied by bulging of the nasal mucosa at the distal finish of the nasolacrimal duct. Decompression is accomplished by relieving the distal obstruction by probing the nasolacrimal duct, removing any nasal cyst, and probably putting a stent. Causes of red eye include infection of the ocular floor (cornea, conjunctiva, and sclera), allergy, intraocular irritation, glaucoma, overseas physique, and trauma. Signs that ought to elevate considerations for a serious etiology of red eye are in an immunocompromised host, extreme ache, proptosis, limitation of eye movements, opacified cornea, abnormal pupil response, or lack of response to remedy. In taking the history, the examiner should inquire about laterality, onset, associated sicknesses, contact with others with "pink eye," the presence of pain or itching, the characteristics of any discharge (watery, mucoid, purulent), and blurring of imaginative and prescient.
Diseases - Cushing syndrome, familial
- Neuroma biliary tract
- Arhinia choanal atresia microphthalmia
- Toxocariasis
- Forbes disease
- Hyposmia nasal hypoplasia hypogonadism
- X chromosome, monosomy Xp22 pter
- Dysphonia, chronic spasmodic
Cheap 5mg selegilineThe pulmonary valve closure is due to this fact delayed and of decreased intensity and is often inaudible medicine joji cheap 5 mg selegiline. When the ejection sound occurs on the upperright sternal border or on the apex medications kidney failure buy 5mg selegiline otc, a bicuspid or stenotic aortic valve illness is usually recommended treatment lower back pain purchase selegiline 5 mg without prescription. In contrast to ejection clicks medications joint pain purchase selegiline 5mg with mastercard, right-sided cardiac murmurs are accentuated with inspiration. Left-sided coronary heart auscultatory abnormalities range little with the respiratory cycle. In the case of the aortic ejection click, the sound is often nicely separated from S1. However, the pulmonary ejection click on is often closer to S1 than is an aortic click on. In some reasonable to extreme instances, the pulmonary ejection click happens concurrently S1. If one perceives a break up S1, one is more than likely hearing an ejection click on because the causes of a real cut up S1 are very uncommon. It is more than likely attributable to sudden tension of the ventricles, enough to produce sound vibrations throughout the myocardial wall. Vibrations within the atrioventricular valve itself, as properly as in the chordae, may contribute to the sound. When heard on the apex, S3 is considered left ventricular in origin, and when heard on the lower left sternal border, S3 is prone to be proper ventricular in origin. An apical S3 of soppy to reasonable depth is readily heard in most youngsters and younger adults. An S3 in association with tachycardia is termed a gallop and could also be attributable to lesions related to left or right ventricular diastolic overload or diminished ventricular compliance. Opening Snap the opening snap, present solely in rheumatic mitral valve stenosis when the anteromedial leaflet is immobile, is heard early in diastole, normally above the apex, and is of medium frequency. Because the leaflets are fused, the downward motion of the opening valve is all of a sudden checked, ensuing within the opening snap. The opening snap and the S3, though comparable in timing, can never occur collectively in the identical patient. It occurs with atrial contraction in opposition to a high resistance and is therefore heard just earlier than S1. The S4 is thought to be brought on by a forceful atrial contraction in opposition to a poorly compliant left ventricle. The sound is readily heard in adults with vital persistent hypertension or left ventricular cardiomyopathy and, except for its timing, sounds very related to an S3. In a young child with complete anomalous pulmonary venous return, low pulmonary vascular resistance, and significantly elevated proper ventricular and pulmonary blood flow, a loud right ventricular S4 (as nicely as S3) may be heard as part of a quadruple rhythm on the decrease left sternal border. Whereas an S3 may be heard in a normal adolescent and could be physiologic, the S4 only occurs in a pathologic situation. Non-Ejection Click Non-ejection clicks are heard at the apex and happen one third to half of the way in which between S1 and S2. The sound is attributable to the sudden tensing of the posterior mitral valve leaflet as it prolapses into the left atrium; in rare circumstances, there could also be multiple mid-systolic clicks. Turbulence might come up as a result of � high flow by way of abnormal or normal valves � regular flow by way of slender or stenotic valves or vessels � backward or regurgitant move via incompetent leaky valves � circulate via congenital or surgical communications � anemia with high flows and discrete decreased blood viscosity Not all cardiac murmurs point out heart problems. The clinician ought to be capable of determine and describe the next seven characteristics of coronary heart murmurs: 1. Location: on the chest wall with regard to � space the place the sound is loudest (point of maximal intensity) � area over which the sound is audible (extent of radiation) 4. The pulmonary ejection click on is best heard at the upper-left sternal border, whereas the aortic ejection click on is often finest heard on the apex. The click on arises either from sudden tension of the semilunar valve or from sudden distention with lateral stress at the root of the aorta or pulmonary artery. An aortic ejection click could also be heard within the presence of a traditional aortic valve (as in severe tetralogy of Fallot with a big aortic root); a pulmonary ejection click on may be heard with a traditional pulmonic valve (as in Eisenmenger syndrome with a big pulmonary root). However, the pulmonary ejection click on, best heard at the upper-left sternal border, is healthier heard on expiration than inspiration. An ejection click or a sharp sound current on the upper-left sternal border, louder with expiration or heard only on expiration, is attribute of pulmonary valve stenosis. Pitch: the frequency range of the murmur, typically described as low, medium, or high-pitched 6. The scientific diagnosis of a traditional ejection or innocent murmur should solely occur within the setting of an otherwise normal historical past, physical examination, and look (Table 8. Thorough auscultation within the cooperative patient ought to include listening in the principal areas (tricuspid, pulmonary, mitral, and aortic) of the precordium with each the bell and diaphragm of the stethoscope and with the patient within the supine, sitting, and standing positions. Mid-systolic to late-systolic murmurs start halfway via systole and are sometimes heard in affiliation with the mid-systolic clicks and insufficiency of mitral valve prolapse. Early diastolic murmurs are decrescendo in nature and come up from either aortic or pulmonary valve insufficiency (regurgitation). Mid-diastolic murmurs are diamond-shaped and occur due to both (1) increased circulate throughout the conventional tricuspid or mitral valve or (2) regular move throughout an obstructed or stenotic tricuspid or mitral valve. Late diastolic or crescendo murmurs are created by stenotic or narrowed atrioventricular valves and occur throughout atrial contraction. Holosystolic murmurs, starting abruptly with S1 and continuing at the same depth to S2, are graphically shown as a rectangle. Ejection murmurs are crescendo-decrescendo or diamond-shaped murmurs that will come up from narrowing of the semilunar valves or outflow tracts. The rising-and-falling nature of the murmur reflects the durations of low flow initially and finish of ventricular systole. The resulting murmur that extends past the S2 has been classically termed "steady. The early diastolic or decrescendo murmur occurs in association with closure of the semilunar valves (second coronary heart sound) and tapers by way of half or all of diastole. The mid-diastolic murmur rises and falls in depth with atrial quantity coming into the ventricle. The late systolic or crescendo diastolic murmur occurs late in diastole with atrial contraction, before systole, and ascends to the primary coronary heart sound. The holosystolic or pansystolic murmur begins abruptly with the primary coronary heart sound (S1) and proceeds on the same intensity to the second coronary heart sound (S2). The ejection systolic or crescendo-decrescendo murmur begins with the onset of volume ejection from the guts. As the circulate increases, the murmur varies each in depth and frequency and subsequently tapers as the interval of ejection ceases, before the S2. The early systolic murmur begins, as does the holosystolic murmur, abruptly with S1 but terminates in mid-systole with the cessation of shunt move. The late systolic murmur begins nicely after S1, commencing in mid- to late systole in affiliation with the development of valve insufficiency and proceeds at this depth to S2. The continuous murmur begins in systole and proceeds as a lot as and thru the second coronary heart sound, proceeding by way of half or all of diastole.
Generic 5mg selegiline free shippingMany other antiepileptic medicines 5 asa medications discount 5mg selegiline visa, including topiramate treatment notes buy selegiline 5mg with mastercard, lamotrigine medicine 5113 v selegiline 5mg without prescription, valproic acid medications like tramadol purchase 5mg selegiline fast delivery, and benzodiazepines, have had some efficacy in isolated instances, however this response is unpredictable. The child might current with febrile or afebrile seizures, often with regular psychomotor development preceding the onset of seizures, and infrequently with a household historical past of epilepsy. The seizures are generalized or unilateral clonic seizures; myoclonic seizures appear later (and may not be a serious feature of the disorder, despite the name), between 8 months and four years of age; and focal seizures and atypical absences could happen. Antiepileptic drugs that may worsen seizures or be ineffective in Dravet syndrome embrace phenytoin, lamotrigine, carbamazepine, oxcarbazepine, and vigabatrin. Childhood the paroxysmal problems of childhood (2-12 years) are given in Table 30. Typically, there are symptom-free intervals lasting weeks to months, and recurrence is unpredictable. There may be a strong family history of migraine, and there appears to be some overlap of the cyclic vomiting with migraine. Children may have phonic tics (such as tongue clicking or throat clearing), motor tics (such as blinking, sniffing, or shrugging), or any combination of both. The presentation of migraines in youngsters may also be markedly different than that in adolescents and adults; "migraine equivalents" are paroxysmal disorders that are strongly related to the later development of migraines and will share related underlying pathophysiologic mechanisms. This temporal affiliation has led to the misconception that the stimulant medications have triggered the tics. Tourette syndrome is identified when a child has had multiple motor tics and at least 1 phonic tic current for longer than 1 12 months. Other tic disorders may be purely motor or purely phonic, and are classified in accordance with their signs and length (transient vs. Sleepdisorders � Peak presentation: age 2-7 years � Classical features: occurring a quantity of hours after falling asleep ("around midnight"), nonstereotyped behaviors, screaming, agitation, and inconsolability regardless of being apparently awake, no memory of scary imagery � Acuity: low � Prognosis: excellent, although youngsters with frequent episodes may have to be monitored by their parents to prevent harm throughout a panicked state Night terrors and confusional arousals. Night terrors are a common phenomenon in kids and are most frequent in boys aged 5-7 years. Up to 15% of youngsters youthful than 7 years have skilled some type of these episodes. The assaults are characterized by sudden arousal from sleep, usually screaming in terror, and then crying with agitation and tachycardia. There could also be vigorous and potentially injurious motor activity in older kids, corresponding to running or hitting the bed or wall. The striking characteristic of these episodes is that the child is inconsolable but seemingly awake. Prior sleep deprivation, febrile illness, emotional stress, and a few drugs (sedatives/hypnotics, neuroleptics, stimulants, antihistamines) may be precipitants. In distinction to the experience of nightmares, youngsters are amnestic for the events and their distress in night time terrors. Confusional arousals are less dramatic assaults with related origin from slow-wave sleep and are more typical in youthful children. Nocturnal frontal lobe seizures happen throughout sleep and may have weird hypermotor behaviors similar to rolling, turning, picking, yelling, and fumbling. In school-aged kids, benign rolandic epilepsy manifests itself as seizures when coming out of sleep with gurgling, salivation, hemifacial and hemibody twitching, and sometimes partially preserved consciousness of the event. Important distinguishing historical elements between seizures and parasomnias are the time of onset (seizures: shortly after falling asleep or early in the morning), length (most seizures final 1-2 minutes, and parasomnias can have a considerably longer duration), and any associated tongue chew, urinary incontinence, or insidious behavioral or developmental regression. Approximately 15% of children have walked of their sleep, especially within the 2-3 years old age group, and a pair of. There is a family history of sleepwalking and other parasomnias in 60-80% of patients. These episodes of apparent unresponsiveness and "automatisms" could be mistaken for focal dyscognitive seizures or a postictal state. Repetitive purposeless actions may be performed by children on the autism spectrum or with cognitive disabilities. Combined with unresponsiveness, these behaviors may be mistaken for automatisms in focal dyscognitive seizures. The necessary features that distinguish such habits from epileptic activity are the setting in which it happens, the variable content and duration of the "attacks," and the whole failure of the episodes to interrupt extra stimulating actions. Acute Symptomatic Seizures and Occasional Seizures Febrile convulsions stay one of the most widespread causes of occasional seizures in early childhood. Head harm is more widespread in childhood than in infancy, however the record of other potential causes of seizures, including brain tumor, intracranial an infection, and poisoning, may be very similar. In addition, some metabolic and neurodegenerative issues manifest in childhood, not in infancy (Table 30. There is a gaggle of idiopathic partial epilepsies starting in children with out abnormalities on neurologic examination or neuroimaging studies, and incessantly, with a household historical past of epilepsy. The seizures are brief and stereotyped in an individual, though they differ amongst patients. The sharp waves or spikes have a characteristic construction and are sometimes very frequent, growing during sleep. Brief hemifacial motor seizures with anarthria and drooling are typical, frequently when coming out of sleep. Consciousness is often preserved, though this may not be true with longer seizures. A somatosensory aura involving the tongue, cheek, or gums could precede the motor seizure. Many seizures happen at night as tonic-clonic seizures, presumably secondary generalized with unwitnessed partial onset. If seizures are infrequent and nocturnal, the option of no remedy must be discussed. Benign childhood epilepsy with occipital paroxysms varieties a subset of idiopathic partial epilepsies of childhood. There are 2 kinds of this subset: 1 with early onset (peak onset at 3-5 years), nocturnal seizures with tonic eye deviation, and vomiting; and another with later onset (peak onset at 7-9 years) characterised by seizures beginning with visual signs, which is according to an occipital origin. These are additionally referred to as Panayiotopoulos syndrome and the benign occipital epilepsy of Gastaut, respectively. Hemiclonic seizures or the automatisms of temporal lobe complicated seizures usually comply with based on whether the seizure spreads to suprasylvian or infrasylvian areas. A severe headache could comply with the visible auras and a analysis of childhood migraine is often thought-about. The discharges are current when the eyes are closed and may disappear with eye opening. There is a few controversy concerning the specificity of the electroclinical features and whether these cases are true variants of benign childhood epilepsy. The absence seizures are easy, or more often, sophisticated with delicate automatisms or different motor options. Absence seizures are very frequent, occurring daily, however they generally respond well to antiepileptic remedy.
Selegiline: 5 mg
Cheap selegiline 5mg free shippingThe child must be relaxed and ought to be given an trustworthy explanation of the procedure medications covered by blue cross blue shield buy selegiline 5 mg amex. The examiner ought to use loads of lubricant and will perform the rectal examination very gently counterfeit medications 60 minutes effective 5 mg selegiline. Lateralizing pain symptoms yeast infection women 5mg selegiline with amex, masses symptoms 5 weeks into pregnancy proven 5 mg selegiline, and the presence and character of stool within the rectum are assessed. Clues to an organic and at instances extra serious explanation for stomach ache are noted in Table 10. Furthermore, peritoneal indicators, which suggest a "surgical stomach," most frequently brought on by peritonitis are famous in Table 10. Family history can additionally be optimistic for dysfunctional pain syndromes (constipation, irritable bowel, dysmenorrhea, and lactase deficiency). However, a striking lymphocytosis may recommend gastroenteritis or a systemic sickness. Overreliance on the whole blood depend alone can cause delay in reaching the proper diagnosis. Laboratory Evaluation After a cautious history is obtained and thorough bodily examination is performed, the prognosis or a short list of attainable diagnoses must be apparent. Urinalysis the urinalysis is a crucial and helpful laboratory take a look at in the evaluation of stomach pain. The presence of ketones and a excessive particular gravity counsel poor food consumption and dehydration. A being pregnant check must be performed on postpubertal girls, no matter sexual activity historical past. The presence of both white cells and micro organism signifies a urinary tract an infection; both discovering alone is in all probability not adequate for that diagnosis. White blood cells may be present in the urine from irritation attributable to an inflammatory mass adjoining to the bladder or ureter; hematuria could also be seen with nephrolithiasis. Complete Blood Cell Count the hemoglobin and hematocrit ranges can reveal anemia brought on by acute or chronic blood loss (as with ulcers, inflammatory bowel illness, Meckel diverticula) or the anemia of chronic disease (as with systemic lupus erythematosus, inflammatory bowel disease). The white blood cell depend indicates the potential of infection or blood dyscrasias. In uncomplicated acute appendicitis, the white blood cell depend ranges from regular values to as excessive as sixteen,000. A very high white blood cell count (>18,000/mm3) indicates intestinal gangrene, perforation, peritonitis, or abscess formation, however this rely can also be excessive in acute bacterial gastroenteritis, streptococcal ailments, pyelonephritis, pelvic inflammatory illness, hemolytic uremic syndrome, and pneumonia. In studies of youngsters with acute appendicitis, 95% had neutrophilia, but solely half had leukocytosis within the first 24 hours. Imaging Evaluation Multitudes of imaging studies are available; none should be obtained until the patient has been examined. The chest movie helps assess the presence of a lower lobe pneumonia, which often causes extreme abdominal ache, particularly in small children. Of those that are limited to patients with critical sickness, 46% of the outcomes are optimistic. Plain belly radiographs could additionally be useful to verify the presence of intestinal obstruction, pneumatosis intestinalis, renal or biliary tract calculi, calcified fecaliths, or intestinal perforation (pneumoperitoneum�free air). If free air or intestinal obstruction is suspected, the stomach movies should include a flat and upright or decubitus view of the abdomen to show the air-fluid interface. This finding routinely makes the analysis of appendiceal dysfunction and confirms the need for appendectomy. If an inflammatory Ultrasonography Ultrasonographic examination is right for kids. It is usually painless, available, emits no radiation, requires no intravenous distinction materials, and may be carried out without sedation. Lower-abdominal gynecologic pain in females, especially in adolescent females, could be confused with appendicitis. Pelvic ultrasonography demonstrates pathologic processes of the ovaries and fallopian tubes, the dimensions of the uterus, and the presence of free fluid in the pelvis. Gallstones, a dilated thick-walled gallbladder, or a dilated common bile duct may be visualized by ultrasonography; all three help the diagnosis of biliary illness. Ultrasonography also particulars the character of belly lots, differentiating cystic from strong masses, and could be useful in demonstrating free fluid or abscesses. The anatomy of the urinary tract is nicely defined by ultrasonography; nephromegaly may be seen with pyelonephritis. Abdominal ultrasonography is an excellent screening methodology for detecting intussusception and midgut volvulus. If an ileus or intestinal obstruction is current, interpretation of the ultrasonographic examination turns into difficult because of the a number of air-filled loops of intestine. Contrast Studies In some situations, sure bowel lesions are best delineated with a distinction medium positioned in the bowel, both in an higher gastrointestinal collection or by enema. If a colonic obstruction is suspected, corresponding to in Hirschsprung disease, the appropriate distinction materials is a barium enema. However, the sensitivity and specificity of contrast enema for detection of Hirschsprung disease is approximately 70% and 83%, respectively. If the suspicion is high for the illness, the patient must be referred for further evaluation with either suction rectal biopsy or anorectal manometry. If the presence of gastrointestinal perforation is possible, whatever the etiology, a water-soluble agent ought to be used as an alternative of barium. Malrotation of the midgut with a volvulus in infants and older youngsters is often seen on ultrasonography but could be diagnosed by an higher gastrointestinal research. In the toddler who presents with an acute stomach and bilious vomiting and in the older baby who manifests chronic stomach ache and intermittent vomiting, the oral barium contrast examine is highly reliable to rule out causes of obstruction such as intestinal malrotation with midgut volvulus or different causes for anatomic obstruction (duodenal internet, annular pancreas, superior mesenteric artery syndrome). Intussusception is each diagnosed and handled via barium enema; nonetheless, preliminary prognosis is possible with ultrasonography. The sudden onset of severe, diffuse ache, along with the suggestion of a soft, nontender mass in the right upper quadrant of the abdomen in a beforehand nicely younger baby constitute the classical picture of intussusception. Twenty-four hours later, the ache was much more extreme in the right-lower quadrant, where localized peritoneal signs have been obvious. The radiographic movie of the abdomen reveals an enormous calcified density within the right-lower quadrant; it proved to be an appendiceal fecalith at surgical procedure. The longitudinal scan of the best lower quadrant (B) reveals a shadowing appendicolith (curved arrow) in a thick-walled appendix, typical of appendicitis. Sedation with morphine is useful for comforting the child and for performing a useful examine. The weight of the barium column typically completely reduces the intussusception, eliminating the necessity for surgical intervention. This research ought to at all times be carried out in session with a surgeon and with the kid prepared to go to the working room in case of failure of discount or perforation of the colon. Successful hydrostatic reduction of the intussusception is completed in 50-75% of circumstances.
Purchase selegiline 5 mgMultiple seizure sorts could have the identical transient basic description medications qd selegiline 5 mg with amex, corresponding to "twitching" or "staring hair treatment discount selegiline 5mg mastercard. This is clinically relevant because improper classification can result in symptoms vitamin b12 deficiency cheap 5mg selegiline overnight delivery inappropriate therapy; for example treatment 5th metacarpal fracture discount selegiline 5 mg, some antiepileptic drugs for focal seizures will exacerbate generalized seizures. Clonic actions are rhythmic, nonsuppressible, positionindependent jerking movements (low frequency, high amplitude) caused by involvement of the motor cortex. With atonic seizures, the lack of tone is sudden but transient, and the affected person is shortly responsive afterward. Automatisms are semipurposeful movements that usually occur with impairment of consciousness both throughout or after a seizure, and can be very useful for figuring out a spell as a seizure. They could also be a perseveration of an activity in progress at ictal onset, corresponding to turning pages of a e-book, or novel semipurposeful actions arising in the course of the seizure. These novel actions are most often a mix of masticatory, oral, and lingual actions (lip smacking or grimacing) and simple fragmentary limb movements, such as twiddling with a held object or pulling at clothes. In infants, orofacial automatisms are extra likely than complicated gestures and have to be distinguished from the traditional habits of infants. Impairment of consciousness, outlined as an alteration in awareness of external stimuli, may be combined with a whole loss or impairment of responsiveness to exterior stimuli. Assessment of consciousness throughout seizures is commonly tough, significantly in younger children. It is possible to be unresponsive due to an lack of ability to converse or articulate clearly (aphasia, apraxia, or paralysis). It can additionally be possible to be aware of external stimuli, however to have altered awareness, usually demonstrated by complete amnesia for occasions instantly earlier than, during, or after the seizure, which implies that memory was not acquired through the seizure due to ongoing neuronal dysfunction. It is feasible to have complicated motor behaviors without lack of complete consciousness or amnesia; frontal lobe seizures commonly have this presentation, and should be rigorously distinguished from nonepileptic occasions. Both focal and generalized seizures may be related to impairment of consciousness; the term dyscognitive is used to describe this symptom. Seizure etiology was previously divided into idiopathic, cryptogenic, and symptomatic. The terms genetic, structural, metabolic, and unknown are presently used to characterize presumptive etiologies (Table 30. The medical symptoms and signs of focal seizures replicate the functional anatomy of the region of the mind undergoing the abnormal neuronal discharge. These terms have been replaced by the more descriptive phrases focal seizure with impairment of consciousness or focal dyscognitive seizure within the case of complicated partial seizures, and focal seizure without impairment of consciousness for simple partial seizures. Examples of auras include an epigastric rising sensation; nausea; visible, auditory, or olfactory hallucinations; or limbic symptoms such as concern or a sensation of d�j� vu. This is generally provoked by movement, excitement, and positioning, and can be suppressed or halted by gently repositioning the affected limb. In newborns, jitteriness (high frequency, low amplitude) may also be mistaken for clonic seizure exercise; this tends to be stimulus-provoked and suppressible. The time period tonic refers to a change in tone as a manifestation of seizure activity, which clinically presents as stiffening or arching. Atonic seizures refer to seizures the place a sudden, temporary loss of tone in the neck or complete physique causes a head nod or fall to the ground. Nonepileptic occasions similar to migraines or syncope may have a prodrome, further highlighting the worth of a complete history in distinguishing kinds of events. The progressive symptoms of some seizures after the preliminary aura reflect the spread of the abnormal electrical discharge past the region of onset, which is why an in depth historical past is critical for evaluating paroxysmal spells and figuring out the chance that they symbolize seizure activity. Seizures with clear electrical abnormalities but minimal or absent physical symptoms are commonly referred to as electrographic seizures or subclinical seizures. Subclinical electrographic seizures, notably throughout sleep, can be related to deterioration in development, conduct, consideration, and studying. Focal motor seizures produce rhythmic jerking (clonic) actions of the limb or limbs contralateral to the primary motor cortex involved. Other focal motor seizures embody involuntary turning of the pinnacle and eyes in 1 direction (version), vocalization, and speech arrest. There may be tonic stiffening and extension of the arm ipsilateral to the seizure onset. Involvement of the sensory cortex produces easy somatosensory experiences corresponding to paresthesia or numbness, often with a dysesthetic high quality, and visual, auditory, olfactory, or gustatory phenomena. Some of those sensory phenomena could be quite complex, including structured visible hallucinations, sensations of depersonalization, and affective symptoms such as anxiousness or fear. Epileptic phenomena are a uncommon cause for such phenomena, and a broad differential prognosis must be thought-about for paroxysmal spells the place the primary symptoms are sensory or affective. Consciousness is impaired in most generalized seizures, but not in all; as an example, brief myoclonic seizures and a few atonic seizures is most likely not related to any impairment of consciousness. Simple absence seizures include only motionlessness and a clean stare lasting for a quantity of seconds, with instant postictal reanimation. Lip-smacking, fumbling, or looking out hand actions, or convulsive swallowing can seem throughout longer seizures, or preictal actions could additionally be continued in a slow, automated manner. Paroxysmal alterations in autonomic perform may also accompany absence seizures, together with pupillary dilation, pallor, flushing, sweating, salivation, piloerection, or a mix of those. Absence seizures which are extra sometimes accompanied by eyelid fluttering, facial twitching, or myoclonic jerks of the trunk or extremities are referred to as sophisticated absence seizures. Atypical absence seizures are described as absence seizures with a much less abrupt starting and end, with extra pronounced modifications in muscle tone, and of longer period. Distinctions must be made between the medical options of absence seizures, focal dyscognitive seizures, and episodic daydreaming (Table 30. Staring spells which are extended beyond 15-20 seconds are much less likely to symbolize absence seizures because of incorrect period. Staring spells in infants and toddlers are additionally unlikely to symbolize absence seizures because of incorrect age of onset. Children with extended staring spells, particularly beginning at a younger age, are at greater danger of partial-onset seizures or behavioral spells. The tonic section begins with sudden sustained contraction of facial, axial, and limb muscle groups, and there could additionally be an initial involuntary stridorous cry or a moan secondary to contraction of the diaphragm and chest muscular tissues towards a partially closed glottis (the ictal cry). The tonic contraction is maintained for seconds to 10s of seconds, during which time the kid falls if standing, is apneic and will become cyanotic, could chew the perimeters of their tongue, and may pass urine. The clonic part of the seizure begins when the tonic contraction is repeatedly interrupted by momentary rest of the muscular contraction. This gives the looks of generalized jerking because the contraction resumes after each relaxation. At the tip of the clonic part, the body relaxes and the patient is unconscious with deep respiration.
Scrophula Plant (Figwort). Selegiline. - Eczema, itching, psoriasis, and hemorrhoids.
- What is Figwort?
- Dosing considerations for Figwort.
- How does Figwort work?
- Are there any interactions with medications?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96455
Purchase 5mg selegiline otcComparison of breast- and formulafed normal newborns in time to first stool and urine medicine cabinets with lights generic selegiline 5mg with mastercard. Densmore An belly mass or stomach fullness in a baby usually becomes apparent when it enlarges enough to be visualized during bathing or palpable on physical examination treatment 2 degree burns selegiline 5 mg without prescription. Hepatomegaly and splenomegaly usually represent systemic illnesses corresponding to an infection medicine app buy selegiline 5mg with amex, hemolysis symptoms thyroid discount selegiline 5mg otc, storage illness, or malignancy. A youngster with an belly mass requires a prompt and thorough work-up with testing guided by history, bodily examination findings, age, and gender. Early surgical referral could help in this work-up following a directed screening method. The duration and character of associated signs are necessary for narrowing the differential diagnosis. A historical past of abdominal trauma ought to be elicited, as solid organ accidents may lead to hematoma, seroma, persistent pseudocyst, or arteriovenous malformation. Infectious disease might have sequelae of cyst, lymphadenopathy, or intraabdominal abscess. A household and sexual history are also pertinent, significantly in adolescent females. Modern prenatal imaging frequently identifies congenital malformations and neoplasms, requiring postnatal imaging and surgical assessment. Physical Examination A full bodily exam must be performed in youngsters with stomach plenty. Attention ought to be paid to the general condition of the child and to indicators of metastatic disease. Enlarged lymph nodes and their locations must be famous, the pores and skin inspected, and the lungs and coronary heart auscultated. Extremities must be evaluated for proof of swelling, venous phlegmasia, or evidence of embolic illness. Genitourinary exam ought to make note of any inappropriate virilization, testicular modifications, and hymenal patency within the case of a feminine with a low pelvic mass. In addition, a neurologic examination may reveal signs of nervous system involvement. The eyes should be rigorously inspected for periorbital ecchymosis, proptosis, squint, opsoclonusmyoclonus syndrome, heterochromia of the iris, Horner syndrome, and scleral icterus. To efficiently perform abdominal palpation in a toddler, the physician must approach the affected person calmly and gently, as probably the most dependable exams are completed in cooperative and relaxed kids. Creative play is typically needed, with using pacifiers or bottles to distract the child from the exam. With the affected person within the supine position, the symmetry of the stomach ought to be inspected, and any visible masses or the presence of ascites ought to be famous. A very enlarged spleen is frequently seen, with fullness of the left facet of the stomach. The presence of tense fluid-filled hernias or distinguished periumbilical veins as sequelae of portal hypertension should be noted. The mass should be localized, and its size, shape, texture, mobility, tenderness, and relation to midline noted. Dull visceral pain performed by slow C nerve fibers could additionally be reported for inflammatory processes within the vascular distributions of the celiac, superior mesenteric, and inferior mesenteric arteries and referred to the epigastrium, umbilical region, or hypogastrium, respectively. When the infected course of contacts the peritoneum, peritoneal quick A nerve fibers enable discrete localization of sharp ache to the stomach wall. Ultrasound is commonly a very useful adjunct within the analysis of an belly mass and is usually obtainable at the bedside. Approximately half of abdominal plenty in older youngsters are brought on by enlargement of the liver or spleen, or each. The liver is normally palpated in the proper upper quadrant and epigastrium extending 1-2 cm below the costal margin. The inferior hepatic margin could additionally be palpated in a thin child, is usually nontender, and strikes with respiration. Detection of liver edge by auscultation utilizing skin scratches has been confirmed unreliable and has been supplanted by means of readily available ultrasound. The spleen is situated in the left upper quadrant and is nonpalpable in most healthy children. The spleen has a rounded tip and may move downward with inspiration and is more superficial than a renal mass. Measurement from the left costal margin to the lower pole of the spleen defines the splenic axis. Masses in the left higher quadrant, especially left renal plenty, could additionally be troublesome to distinguish from an enlarged spleen. In general, the presence of the splenic notch helps identify the mass as a spleen, but nodular plenty, corresponding to Wilms tumors of the kidney, neuroblastomas, and Bezoar Hematocolpos Hydrometrocolpos Pregnancy Inflammatory bowel disease Retroperitoneal hematoma (hemophilia) retroperitoneal teratomas may masquerade as splenomegaly. Hyperinflation of lungs (as occurs in bronchial asthma, bronchiolitis, ipsilateral pneumothorax) may make a normal-sized liver or spleen palpable. Flank masses are the next most frequent, particularly in newborn to toddler-aged children. Renal plenty lengthen caudally, are fixed with respiration, and trigger stomach asymmetry. Lower belly plenty are mostly caused by constipation or urinary retention. A perforated appendix with resulting abscess formation could create a young right lower quadrant mass. Ovarian or uterine tumors usually grow undetected in the pelvis till massive enough to exit the pelvis as a large palpable belly mass. Laboratory and Imaging Studies Screening laboratory data, together with complete blood count with differential and cell morphology, measurements of serum electrolytes, urinalysis, urine being pregnant test when acceptable, and inflammatory markers, are broadly applicable. Liver perform tests, serum amylase, 286 Section three GastrointestinalDisorders Location and nature of Abdominal Masses congenital Hemangioma Choledochal cyst Benign Hemangioendothelioma Hamartoma Malignant Hepatoblastoma Lymphoma Leukemia Hepatocellular carcinoma Sarcoma Wilms tumor Acquired Abscess Hematoma Parasitic illness Hydrops of the gallbladder Splenomegaly. Plain abdominal radiographs could reveal tumor calcifications, organomegaly, extra fecal load, and mass effect upon intestines. Views in no much less than 2 different positions ought to be obtained to appreciate ascites or intestinal obstruction. As a screening modality, ultrasonography is a extremely environment friendly, low-cost, and broadly out there take a look at. These modalities typically provide radiologic prognosis, are invaluable for surgical planning, and are unhampered by bowel gas, a standard limitation of ultrasound. A palpable spleen (2 cm beneath the left costal margin) is a traditional discovering in a baby youthful than three years and could additionally be a traditional discovering in an older baby. Up to 15% of full-term neonates, 10% of kids, and 3% of faculty freshmen have palpable spleens unassociated with a rise in lymphoreticular malignancy and with equal health. Painful splenomegaly generally follows stretching of the splenic capsule with speedy enlargement of the spleen.
5 mg selegiline with amexSignificantly enlarged inguinal nodes may also be present with sexually transmitted infections medications while pregnant cheap selegiline 5mg on-line, similar to syphilis medicine ball slams order selegiline 5mg mastercard, chlamydial urethritis treatment integrity checklist 5mg selegiline overnight delivery, lymphogranuloma venereum symptoms miscarriage buy 5 mg selegiline free shipping, or with urinary tract infection, lymphoma, or abdominal tumors. Mediastinal adenopathy (or mass) could also be detected by the way, or secondary to chest signs, or through the analysis of peripheral however generalized lymphadenopathy. Physical Examination Physical examination should assess common appearance and search for signs or symptoms which will reveal the underlying cause of lymphadenopathy. Examination of the lymphatic system ought to establish the dimensions, quality, and distribution of any abnormal lymph nodes and may assess for the presence of tenderness or changes in the overlying pores and skin or surrounding tissues. Differential Diagnosis the differential analysis of lymphadenopathy is developed in a stepwise style, first by figuring out whether the lymphadenopathy is regional or generalized. Next, the time course of the lymphadenopathy must be defined as acute or as continual, defined as being current for a interval of greater than 4 weeks. Children presenting with prolonged diffuse lymphadenopathy, hepatomegaly or splenomegaly, weight reduction, evening sweats, fevers, recurrent infections, or failure to thrive must be more completely studied. Only after the whole blood cell depend and differential and chest radiograph are analyzed should different diagnostic studies be thought of. Regional Lymphadenopathy the standard child with acute regional lymphadenopathy presents with enlarged nodes, commonly in the cervical area. A thorough history and cautious physical examination should reveal whether or not nodes are definitively concerned, as opposed to other nonnodal structures, such because the parotid gland. In many instances, no other abnormalities are found on examination, and systemic signs are minimal. Laboratory checks should embrace a complete blood cell count and differential in addition to measurement of the erythrocyte sedimentation price and the C-reactive protein. In the kid with fever and a young cervical lymph node, oral antibiotics (with activity against mouth flora, streptococci, and staphylococci) ought to be started; if the lymphadenopathy persists or worsens, intravenous antibiotics are indicated. In contrast, if the lymphadenopathy continues or becomes frank lymphadenitis with erythema and tenderness regardless of antimicrobial therapy, additional work-up is indicated. If an abscess is found, incision and drainage, adopted by acceptable bacterial and mycobacterial cultures and stains, are appropriate. Differential Diagnosis of Head and Neck Lymphadenopathy: Head and Neck Masses Several congenital and acquired lesions of different head and neck buildings, lots of which are benign, may mimic lymphadenopathy and deserve consideration. History and physical examination ought to present enough information to arrive at an acceptable differential diagnosis and evaluation strategy of these mimics. Evaluation and Management Strategies Many previously healthy children with acute lymphadenopathy require few, if any, laboratory or imaging research. No laboratory testing could also be required for well-appearing youngsters whose acute, localized adenopathy could be attributed to an an infection within the vicinity of the node. Acute cervical adenopathy accompanying pharyngitis in children older than 18 months may necessitate a throat tradition for group A Streptococcus. Generalized Lymphadenopathy In the child with generalized lymphadenopathy, the cause may be infectious, immunologic, or malignant. Drugs might cause serum sickness however may produce hypersensitivity reactions with ensuing generalized lymphadenopathy. Medications associated with drug-induced lymphadenopathy include allopurinol, atenolol, captopril, carbamazepine, gold, hydralazine, penicillins, phenytoin, primidone, procainamide, pyrimethamine, quinidine, sulfonamides, sulindac, and tetracyclines. An abnormal complete blood cell count demonstrating anemia, leukopenia, or thrombocytopenia, or radiologic evidence of mediastinal adenopathy or pleural disease is extremely suggestive of malignancy. Excision of a node is most well-liked in some cases to have the ability to get hold of enough tissue for pathologic research, stains, or cultures. Pharyngeal infection is the commonest reason for regional lymphadenopathy in youngsters (see Chapter 1). Many of these pharyngeal infections are associated with cervical lymphadenopathy and are viral in origin. Frequent viral causes embrace adenovirus, parainfluenza, influenza, rhinovirus, and enterovirus. The chief criticism normally includes pain with swallowing and with speaking, in addition to tender, enlarged lymph nodes within the neck. Systemic manifestations, similar to fever, myalgia, chills, and rhinorrhea can also be present. An examination of the throat sometimes reveals a symmetrically erythematous posterior oropharynx with enlarged tonsils that often comprise exudates. Herpes stomatitis with mucocutaneous involvement and herpes pharyngitis with oropharyngeal vesicles are additionally associated with bilaterally enlarged, tender, non-erythematous cervical nodes. Bacterial an infection of the pharynx is also commonly related to enlarged, tender cervical lymph nodes. Other bacteria can cause pharyngitis and cervical adenopathy, including non�group A streptococci and anaerobic organisms, such as Fusobacterium species. Anaerobic organisms can result in painful oral gingivitis or stomatitis and pharyngitis (Vincent angina) that may progress to peritonsillar abscess. Asymmetry within the tonsils and surrounding tissues, in addition to deviation of the uvula away from the affected aspect may be seen with peritonsillar abscesses, together with unilateral tender, enlarged cervical lymph nodes ipsilateral to the abscess. Complications of acute bacterial pharyngitis can also embody Lemierre syndrome, the findings of which embody high fever and unilateral, lateral neck swelling that could be confused with adenopathy. Lemierre syndrome is due to septic thrombosis of the internal jugular vein (and pulmonary septic emboli), normally attributable to invasion of the bloodstream by Fusobacterium organisms, and should result in immediate hospitalization, blood cultures, remedy with intravenous antibiotics, and imaging of the internal jugular vein through Doppler move ultrasonography or contrast-enhanced computed tomography. Acute cervical lymphadenitis-inflammation of the cervical lymph nodes with tender enlargement-is most likely to happen with group A streptococcal or Staphylococcus aureus an infection. There may or is in all probability not a historical past of sore throat or pharyngeal irritation on examination. Infection with different oral micro organism, including non�group A streptococci and anaerobes such as Fusobacterium or Arcanobacterium species may also occur, presumably with the pharynx as the portal of entry. Usually, these nodes rapidly diminish in measurement after institution of acceptable antibiotic remedy, providing some degree of retrospective diagnosis whereas simultaneously being therapeutic. Acute suppurative cervical adenitis could be seen in infections of the face and scalp and is often attributable to infection with group A streptococci or S. Management of suppuration includes incision and drainage or excision of the suppurative node. Gram stain and bacterial, fungal, and mycobacterial cultures of the drainage should be obtained. Total excision should be carried out if atypical mycobacterial infection is suspected, as a end result of draining fistulas may type if a needle biopsy or partial resection is carried out. Bacterial infections of the pores and skin and soft tissues are common causes of localized lymphadenopathy and adenitis, and may lead to axillary or inguinal adenopathy if these infections originate in the extremities. Any laceration or insect bite that turns into contaminated might yield adenopathy upstream within the nodal drainage basin of the contaminated website. Occasionally, penetrating accidents to the toes occurring by way of damp footwear or in moist areas might yield infections with different bacteria, similar to Pseudomonas aeruginosa. These penetrating infections usually manifest with cellulitis or osteomyelitis; lymphadenopathy is noted during the physical examination. The commonest sites of an infection include the foot or leg, resulting in unilateral inguinal lymphadenitis, and the hand or arm, inflicting axillary lymphadenitis or unilateral irritation of the epitrochlear nodes. In these kids, fever and gentle cervical adenopathy may be the major signs on presentation, or the kid could additionally be considerably sick with excessive fever and pharyngitis.
Buy selegiline 5mg low priceSynovial fluid analysis in childhood is most helpful for confirming or excluding three potential issues: (1) infectious arthritis symptoms of diabetes selegiline 5 mg cheap, (2) hemarthrosis (either secondary to trauma or a coagulopathy) medicine qhs purchase 5 mg selegiline, and very hardly ever (3) crystal ailments similar to gout or pseudogout treatment action group generic selegiline 5mg without a prescription. A 4th condition medications you can take during pregnancy cheap 5 mg selegiline, the rare entity of pigmented villonodular synovitis, is suggested by the aspiration of a "chocolate brown" synovial fluid from the knee. These situations include leukemia, tumor lysis syndrome, renal failure, Down syndrome, Lesch�Nyhan syndrome, and type I glycogen storage illness (von Gierke disease). Biopsies of affected tissue are often essential to confirm a diagnosis for many of the vasculitides. In many kids with vasculitis, this tissue is the pores and skin and session with a dermatologist is helpful to decide which lesions and the placement inside a lesion that will be most probably to yield a prognosis. Likewise, if there has been publicity to tuberculosis, or if a child is immunocompromised, joint fluid aspiration must be strongly thought-about. In rare circumstances, synovial tumors, chronic indolent infections, or international our bodies are detected by biopsy as properly. Most affected kids have morning stiffness, delicate discomfort, swelling, and warmth of the affected joint or joints, however often stay fairly practical and are systemically well. The arthritis normally has a good prognosis and in some instances may finally remit on its own. The arthritis in these subtypes is symmetric and impacts each small and large joints. Involvement of the small joints of the arms and feet, as properly as the wrists, is quite common. Enthesitis-Related Arthritis the older term spondyloarthropathy encompasses a gaggle of ailments that includes ankylosing spondylitis, psoriatic arthritis, inflammatory bowel disease-associated arthritis, and reactive arthritis. Psoriasis usually precedes the event of arthritis, however in a sizable minority, arthritis can precede the pores and skin disease, typically by a few years. Up to 30% of patients with psoriasis also have associated arthritis, with sufferers which have nail involvement being more likely to develop arthritis. Ophthalmologic slit-lamp evaluations are needed at particular intervals to display screen for anterior uveitis, as a result of usually the uveitis is asymptomatic and might progress to affect visual acuity before it causes different signs and signs. All others ought to have evaluations at 6-month intervals for the primary 4 years after analysis, and yearly thereafter. In childhood, the height onset is in the course of the early teen years and infrequently occurs in children younger than 5 years. Constitutional symptoms corresponding to fatigue, poor appetite, and weight loss are frequent. Generalized lymphadenopathy and hepatosplenomegaly are also widespread; pericarditis or pleural effusions may be seen. These children really feel and appear unwell in the course of the fever spikes, however they could seem a lot improved once the fever abates. In many sufferers, the fevers and rashes subside and polyarticular arthritis persists as an isolated manifestation, whereas in different sufferers, the fevers and rashes continue to dominate their medical picture. Cytopenias, particularly thrombocytopenia, are observed, as are hypertriglyceridemia and hypoalbuminemia. Hemophagocytosis is observed in varied tissues, mostly within the bone marrow and cerebrospinal fluid. The arthritis is most often symmetric and polyarticular, and frequently involves the small joints of the hands and ft. Leukopenia, lymphopenia, thrombocytopenia, and autoimmune hemolytic anemia, incessantly with a positive direct Coombs test, are common. Monitoring C3 and C4 ranges helps guide therapy; the levels ought to improve to regular because the sickness is best managed. Laboratory exams and imaging research are used when essential to exclude other sicknesses. Dermatomyositis is extra frequent in girls and may occur at any age; the common age at onset is eight years. These symptoms are sometimes accompanied by delicate muscle pain, fatigue, or poor endurance. Frequent early symptoms include difficulties rising from the floor, climbing stairs, climbing in and out of a minivan, and combing the hair. Similar lesions are seen on the extensor surfaces of the elbows and knees and over the medial malleoli. The distribution of the rash, which may be misdiagnosed as eczema or psoriasis, is an early clue to the prognosis. The periungual capillaries may become grossly dilated and may develop thromboses that can be visualized either with the naked eye or with mild magnification. Some kids develop extra intensive erythroderma that may seem over the shoulders, termed the shawl sign, or in a V-neck distribution on the chest. With severe illness, some patients can also develop vasculopathic skin ulcerations. Typical findings on biopsy embrace perivascular inflammation and perifascicular atrophy. The biopsy may help exclude other potential myopathies corresponding to muscular dystrophies and metabolic myopathies. Localized scleroderma, which incorporates morphea and linear scleroderma, is limited to the pores and skin and subcutaneous tissues, is far more common in childhood, and infrequently progresses to involve inside organs. Systemic sclerosis could be life threatening, because it has the potential to contain inside organs and cause severe and widespread pores and skin disease. Diagnosis the prognosis is typically recommended by the rash and proximal muscle weak point detected on physical examination. There may be elevations in only 1 or a number of enzymes and therefore testing for aspartate aminotransferase, alanine aminotransferase, lactate dehydrogenase, creatine kinase, and aldolase should be performed. The youngster with a characteristic rash, definite proximal muscle weak point, and elevated Morphea Morphea is a patch of hardened pores and skin that seems spontaneously on any part of the body. Systemic Sclerosis Systemic sclerosis usually begins with extreme Raynaud phenomenon, adopted by thickening and tightening of the skin over the digits and palms after which the face, after which by various levels of progressive skin modifications over the extremities and trunk. Difficulty opening the mouth and decreased facial features are signs of facial involvement. As the skin over the hands tightens and hardens, pigment modifications might happen, and flexion contractures of the small joints might develop. Renal disease, pulmonary fibrosis, pulmonary hypertension, esophageal and intestine dysmotility, and cardiac illness might all happen. Anti-Scl-70 antibodies (anti-topoisomerase I) are current in roughly 30-40% of patients with systemic sclerosis and are very particular. The course of systemic sclerosis is variable; sufferers with fast development are likely to have a less favorable outcome. Although less severe than systemic sclerosis, these sufferers can develop life-threatening pulmonary hypertension. The natural historical past of morphea lesions is to gradually fade and soften after an initial period of enlargement.
Cheap selegiline 5mg amexTelega Jaundice treatment centers for drug addiction proven selegiline 5mg, the yellow discoloration of skin and sclerae treatment xerostomia cheap 5mg selegiline overnight delivery, results when the serum degree of bilirubin treatment xeroderma pigmentosum discount 5mg selegiline, a pigmented compound symptoms upper respiratory infection selegiline 5mg on line, is elevated. Microsomal heme oxygenase, located principally within the reticuloendothelial system, catabolizes heme to biliverdin, which is then decreased to bilirubin by biliverdin reductase. It is excreted from the hepatocyte to the canaliculi, through the biliary tree, and into the duodenum. A small amount of urobilinogen is reabsorbed and returned to the liver by way of enterohepatic circulation or excreted by the kidneys. Conjugated and unconjugated are more accurate phrases, as a result of "direct" and "oblique" refer to the van den Bergh response, used for measuring bilirubin. In this assay, the unconjugated fraction is determined by subtracting the direct fraction from the entire and, subsequently, is an indirect measurement. The direct fraction includes each conjugated bilirubin and -bilirubin, an albumin-bound fraction. Conjugated hyperbilirubinemia exists when more than 20% of the total bilirubin or greater than 2 mg/dL is conjugated. If neither criterion is met, the hyperbilirubinemia is classified as unconjugated. Unconjugated hyperbilirubinemia could be attributable to any course of that results in increased manufacturing, decreased delivery to the liver, decreased hepatic uptake, decreased conjugation, or elevated enterohepatic circulation of bilirubin. Conjugated hyperbilirubinemia can happen because of hepatocellular dysfunction, biliary obstruction, and irregular excretion of bile acids or bilirubin. On event, hemolysis interferes with some assays and will lead to a falsely elevated conjugated fraction. If the medical picture is consistent with unconjugated hyperbilirubinemia, the assay must be repeated with a venous sample. Levels of each are markedly elevated (>5- to 10-fold normal) with hepatocellular harm caused by hepatitis, hepatotoxicity, ischemia, genetic or metabolic liver issues. It is necessary to keep in thoughts that aminotransferases replicate cell injury, not liver perform. Temporal developments in serum aminotransferase levels are useful in monitoring illness activity in chronic viral and autoimmune hepatitis. Alkaline Phosphatase Alkaline phosphatase is an enzyme found in bile ducts, bone, intestine, placenta, and tumors. Drugs or toxins None discovered Familial issues: Gilbert syndrome Crigler-Najjar syndromes Lucey-Driscoll syndrome Elevated reticulocyte depend Consider: 1. Alagille syndrome Abnormal findings Yes Supportive remedy No Evaluate for anatomic abnormalities and intrahepatic cholestasis: 1. Fractionation of the alkaline phosphatase isoenzymes might help to determine its site of origin. In the evaluation of conjugated hyperbilirubinemia, an alkaline phosphatase level of higher than three occasions normal signifies cholestasis; a milder elevation is more in preserving with hepatocellular illness. Administration of phenobarbital (5 mg/kg/ day) for five days before the research may increase bile flow and thus can enhance the diagnostic accuracy. Levels are generally very high in main cholestasis and biliary obstruction however solely mildly increased (more than twice normal) in hepatocellular disease. Since many imaging protocols can be utilized relying on the aim of the research, contacting a radiologist prior to ordering the study is beneficial. Albumin Albumin is produced in the liver, and levels can reflect hepatic synthetic function. Serum albumin ranges can be helpful in monitoring development of chronic liver illness and in discriminating an acute illness from a beforehand unrecognized persistent dysfunction. Hypoalbuminemia can be secondary to nephrotic syndrome or a proteinlosing enteropathy. Due to a protracted half-life (20 days), albumin is of limited use in assessing synthetic dysfunction in acute liver failure. Ultrasonography Ultrasound studies are helpful, noninvasive, comparatively cheap diagnostic instruments for the analysis of liver illness. Ultrasonography supplies data on the size and consistency of the liver and spleen and anatomic abnormalities of the biliary tree, gallstones, and hepatic lots similar to cysts, tumors, or abscesses. The utility of ultrasonography is restricted in overweight patients and in sufferers with excessive bowel gas. Doppler ultrasonography also demonstrates dynamic move in hepatic blood vessels and the portal vein; it may possibly establish vascular anomalies of the liver and suggest presence of portal hypertension. Under ultrasound guidance, a needle is passed via the liver and into the biliary tree, and contrast materials is injected. If obstruction is recognized, biliary drainage, if required, may be carried out at the identical time. Liver Biopsy Percutaneous liver biopsy is often essential to decide the purpose for conjugated hyperbilirubinemia. In some instances, a particular sample of injury, such as paucity of bile ducts or bile duct proliferation, could additionally be evident. In other instances, particular markers of illness could additionally be recognized (the distinctive inclusions in 1-antitrypsin deficiency) or measured Scintigraphy Hepatobiliary scintigraphy can assist in the prognosis of biliary atresia. In a wholesome individual, hepatic uptake and excretion of the radionuclide through the biliary system are immediate. An open biopsy may be needed when a large sample of tissue is required or when there are contraindications to the percutaneous approach, such as ascites or coagulopathy. Transjugular liver biopsy can scale back the risk of bleeding in patients with coagulopathy. In the neonate, the causes of jaundice range from a benign, self-limited process related to immaturity of bilirubin excretion (physiologic jaundice) to life-threatening biliary atresia or metabolic problems (galactosemia, fructosemia, tyrosinemia). For instance, physiologic jaundice generally resolves by 1-2 weeks of age, and jaundice associated with breast milk often resolves by the time the infant is 1 month old. Acholic stools usually point out obstruction of the biliary tree; nonetheless, nonpigmented stools may be seen with extreme hepatocellular harm. The clinician should doc the presence or absence of acholic stool in each infant evaluated for jaundice. The heart of the stool ought to be examined as a result of the surface may be frivolously pigmented from sloughed jaundiced cells of the intestinal tract. Delayed passage of meconium may be secondary to cystic fibrosis or Hirschsprung illness. Delayed passage of stools, by itself, can result in increased enterohepatic circulation of bilirubin. Clues to the diagnosis of hyperbilirubinemia are often found within the prenatal and perinatal historical past (Table 15. Breast-feeding is related to higher levels of unconjugated bilirubin and a longer length of jaundice than in formula-feeding. Even when analysis of breast milk jaundice is probably going, conjugated bilirubin ought to be checked because it provides a simple screening tool for liver problems, together with biliary atresia. Infants with metabolic disorders often present with a history of vomiting, lethargy, and poor feeding. Vomiting can also be a symptom of intestinal obstruction including malrotation/volvulus.
References - Ebert TJ, Harkin CP, Muzi M: Cardiovascular responses to sevoflurane: A review, Anesth Analg 81(Suppl 6):S11-S22, 1995.
- Noguera, R.S., Rodriguez, R.C. Open adenomectomy: past, present and future. Curr Opin Urol 2008;18:34-40.
- Moneta G, Partsch B: Compression therapy for venous ulceration. In Gloviczki P, editor: Handbook of venous disorders, vol 1, ed 3, London, 2009, Hodder Arnold, pp 348-358.
- Tyzzer EE. Factors in the production and growth of tumor metastases. J Med Res 1913;28;309.
- Auais A, Adkins B, Napchan G, et al. Immunomodulatory effects of sensory nerves during respiratory syncytial virus infection in rats. Am J Physiol Lung Cell Mol Physiol 2003; 285: L105-L113.
- Tsalik EL, Woods CW: Sepsis redefined: The search for surrogate markers, Int J Antimicrob Agents 34(Suppl 4):S16-S20, 2009.
|