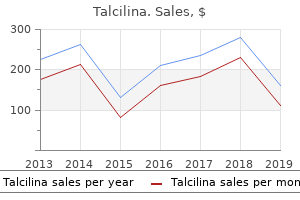
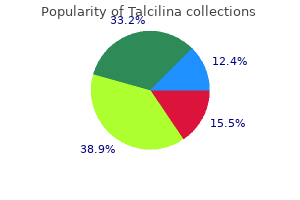
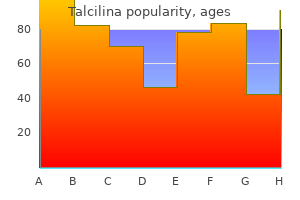
Talcilina
Margaret P. Adam, M.D. - University of Washington School of Medicine
- Seattle, Washington
Talcilina: 500 mg, 250 mg, 100 mg
Talcilina 100mg otcHeterochromic Iridocyclitis of Fuchs this is a low-grade continual cyclitis treatment for uti from e coli generic talcilina 100 mg, the one obvious options of that are a lightening of the colour of the affected iris and the presence of a few keratic precipitates on the cornea infection jaw bone 500 mg talcilina for sale. The iris becomes atrophic virus going around schools generic 100mg talcilina overnight delivery, loses its markings and readily transilluminates in circumscribed areas antibiotics for urinary tract infection in dogs purchase talcilina 500mg amex, and a cataract frequently develops. The situation is usually mentioned to be associated with some disturbance of the sympathetic nerve supply which controls the chromatophores, accounting for the depigmentation and the tone of the blood vessels. When the blood vessels are dilated, white cells escape and get deposited on the cornea as precipitates. During cataract surgery, fine filiform haemorrhage from the alternative angle has been observed to happen as soon as the anterior chamber is opened-this is referred to as Amsler signal. Geographical Choroidopathy this could be a distinct scientific entity of unknown aetiology in which there are acute, recurring, well-defined lesions affecting the pigment epithelium. The earliest changes consist of yellowish-grey areas on the degree of the pigment epithelium associated with some swelling of the overlying retina however no inflammatory cells within the vitreous. Acute lesions last weeks to months however the illness has a chronic, recurring course. It progresses over a number of years and is characterized by the prevalence of additional acute lesions. Fluorescein angiography reveals relative hypofluorescence corresponding with the gray lesion. Over the next 3 months, pigment epithelial and retinal swellings subside and the centre of the lesion takes on a gray appearance with a lighter colored margin. Fluorescein angiography at this stage shows a relative hyperfluorescence on the margin of the lesion, while the centre of the lesion remains hypofluorescent. After three months, fluorescein research present uniform hyperfluorescence of the lesion lasting throughout the angiogram. The differential analysis is choroidal sclerosis, placoid pigment epitheliopathy, pigment epithelitis and serpiginous choroidopathy. The scientific image resembles an insidiously disseminated choroiditis characterised by a quantity of, confluent foci of exudate and scar formation affecting mainly the superficial portion of the choroid. The macula is regularly concerned with peripapillary and macular geographic lesions. Fluorescein angiography and histological studies reveal disappearance of the choriocapillaris and the pigment epithelium. Ophthalmoscopy shows small, greyish, disc-like or circular confluent lesions and choroidal scars with slight pigment dispersion, leading to depigmentation in a serpiginous configuration. Therapy consists of prednisolone in combination with antitubercular medication, if evidence suggests a tubercular aetiology. Acute retinal pigment epithelitis: this condition has a characteristic acute onset with a reasonably fast resolution over 6�12 weeks and supreme restoration of regular imaginative and prescient. The typical lesion is a dark greyish spot which is well outlined in the acute and later phases. The lesions form in two or four clusters in the macular space and could also be unilateral or bilateral. Fluorescein angiographic findings are minimal within the acute stage however hyperfluorescence comparable to the preliminary halo-like zone can ultimately be seen. Acute Multifocal Placoid Pigment Epitheliopathy this disease impacts each the eyes in healthy subjects of both sex between the ages of 20 and 30 years. Spontaneous decision with good visual restoration is common, although the syndrome might be a manifestation of a diffuse systemic inflammatory condition. The major lesion appears to be an obstructive vasculitis at the level of the choriocapillaris leading to ischaemic damage and focal swelling of the retinal pigment epithelial cells. This offers rise to the attribute ophthalmoscopic look of cream-coloured placoid lesions over the posterior pole inside the equatorial area. Fluorescein angiography exhibits patchy, irregular choroidal filling, progressively outlining these lesions which mask the background fluorescence. Each area is stained with fluorescein in the course of the later stages without significant leakage of dye. Upper respiratory symptoms, altered sensitivity to medication and elevated levels of gamma globulin favour a viral or an immune complicated mechanism. The differential prognosis contains multifocal choroiditis, main retinal pigment epithelial detachment and acute epithelitis. Rapid lack of central imaginative and prescient is often adopted by immediate resolution of the lesions with important visible enchancment continuing a quantity of weeks after the obvious ophthalmoscopic improvement. The alteration within the retinal pigment epithelium is everlasting but adjustments in the choriocapillaris are minimal. Masquerade Syndromes these embody a bunch of illnesses which mimic anterior or posterior uveitis in their medical options but the aetiopathogenesis is completely different, being usually neoplastic or often ischaemic. Acute leukaemia, iris melanoma, juvenile xanthogranuloma, small round cell malignancies, anterior segment ischaemia, reticulum cell sarcoma or giant cell lymphoma are a few of the circumstances which can current in this method. In addition to the investigations detailed in general uveitis, cytological and immunohistological studies of aqueous and vitreous specimens assist in establishing the analysis. On the opposite hand, the blood provide to the choroid, being basically segmental, results in the formation of lesions restricted to isolated areas. The richness of anastomoses within the anterior part of the uveal tract precludes isolated vascular lesions. Massive expulsive haemorrhage may happen in the choroid in situations with sclerosis of the partitions of the choroidal vessels, which give means on sudden lowering of the intraocular pressure throughout surgical procedure for cataract or glaucoma. The visible acuity returns to normal within 3�6 months in most cases however some subjective signs persist. Argon laser burns may be utilized to coagulate the leak if the oedema has continued for 3 months or longer. Examination and management: l There is a circular swelling seen in the macular area usually concerning the size of the optic disc. The oedema may be superficial or deep to the retinal pigment epithelium, so that the affected space is raised above the extent of the retina and is surrounded by a attribute ringshaped reflex. Recurrences are frequent and produce extensive degeneration, which is called retinal pigment epithelium decompensation. Complications that may occur following central serous retinopathy are geographic atrophy of the pigment epithelium and choriocapillaris, invasion of the subpigment epithelial space by new vessels with development to a fibrovascular scar and tearing of the retinal pigment epithelium. A rise in intraocular pressure occurs, initially with an open anterior chamber angle showing neovascularization, but later as fibrosis takes place the angle zips up, leading to an intractable neovascular glaucoma. Panretinal photocoagulation of an ischaemic retina prevents the event of neovascular glaucoma. If the ocular media are hazy, as incessantly seen, anterior retinal cryopexy could be as effective. A trabeculectomy with adjuvant administration of mitomycin C or a drainage implant is used to control the raised intraocular strain. Irregular lacunae in the pigmentary epithelium may usually be seen with retroillumination with a slit-lamp or transillumination by contact illumination. Essential (Progressive) Atrophy of the Iris this disease of unknown aetiology is characterised by a slowly progressive atrophic change in the tissues of the iris, which leads to the whole disappearance of huge parts of this tissue. The disease normally begins insidiously in early adult life by the event of huge areas of atrophy which coalesce and progress to type lacunae.
Purchase talcilina 500 mg otcIn fetal life infection japanese horror movie trusted talcilina 500 mg, the choroid plexus occupies many of the lateral ventricle and then steadily decreases in size antibiotic drugs buy talcilina 500 mg low price. Formation of the anterior commissure (the first commissure to seem throughout development) is followed by the event of the hippocampal commissure and the corpus callosum (around the fourth month) oral antibiotics for acne yahoo answers 100mg talcilina amex. These commissures are formed by axons that stretch from one hemisphere to the opposite utilizing the embryonic lamina terminalis as a bridge antibiotic xifaxan side effects purchase talcilina 500 mg with mastercard. Initially, the hippocampus seems as a ridge derived from the medial cortical wall. Spinal-cord malformation: Part 1: A unified principle of embryogenesis for double spinal-cord malformations. Hirschsprung disease and Hypoganglionosis in adults: Radiologic findings and differentiation. Syndrome of occipitoatlantoaxial hypermobility, cranial settling, and Chiari malformation kind I in sufferers with hereditary problems of connective tissue. Neuronal migration within the creating cerebral cortex: Observations based on realtime imaging. Pathways of trunk neural crest cell migration within the mouse embryo as revealed by vital dye labelling. Multipolar migration: the third mode of radial neuronal migration within the creating cerebral cortex. Specifically, the caudate and putamen derive from the ganglionic eminences within the ventrolateral part of the telencephalic ventricle, whereas the pallidum originates from lateral and medial hypothalamic analogs. The corpus striatum assumes a striated look following the crossing of fibers that join the telencephalic vesicles to the diencephalon and brainstem. Diagnosis of Chiari I malformation and associated syringomyelia: Radiological and neurophysiological research. Lipomas of the cauda equina and other fatty tumors associated to neurospinal dysraphism. Even-numbered rhombomeres control the apoptotic elimination of neural crest from oddnumbered rhombomeres within the chick hindbrain. Transnasal odontoid resection followed by posterior decompression and occipitocervical fusion in youngsters with Chiari malformation Type I and ventral brainstem compression. Connectivity between neuronal populations necessitates technology of impulses along the cell membrane and actions of neurotransmitters in addition to the assist of the nonexcitable glial cells. The shape of the neurons, characteristics of the axons and dendritic arborizations, in addition to the receptive zones of the neurons can also have an result on synaptic connectivity and decide their actions. In summary, it controls all of the activities that preserve the person and species. These functions are completed at mobile ranges by the neurons and are enhanced by way of supportive glial cells. Neurons maintain certain common structural and morphological traits that enhance their actions and correlate intently with their features. Following an harm, these structures might undergo changes or assume completely different positions within the neurons. Myelin, the masking of sure axons, plays an important function in nerve conduction and displays degenerative changes specifically ailments. Glial cells kind the skeleton of the nervous system, display several types, and participate in a wide range of supportive functions that collectively maintain the optimal environment for neuronal activity. Presence of molecules such as fibronectin, laminin, and mobile adhesion molecules could account for the mechanism by which neurons migrate alongside processes of certain glial cells and not others. Macroglia Macroglia are classified into astrocytes, oligodendrocytes, and ependymal cells. They are current in both grey and white matter and possess processes that department repeatedly in an irregular trend and assume starlike configurations. Astrocytes set up contacts with the nonsynaptic parts of the neurons and kind perivascular end toes that stretch to the blood capillaries. Glial cells present the optimum milieu for neuronal operate by balancing the ionic concentration throughout the extracellular space. They present vitamins, discard metabolites and cellular particles, and sharpen neuronal alerts, preventing ephapsis or cross talk by forming a protective myelin sheath. The glial cells mediate the extent of impulse move, exercise of neurons, and frequency of excitation. Thus, adjustments within the glial cell membrane potentials might happen because of the fluctuation within the potassium ion concentration, which, in flip, is affected by stage of the generated impulses. Bergmann glial cells of the cerebellum lie at the Purkinje layer, sending several processes with short aspect branches that ascend and envelop the Purkinje cell dendrites. They are numerous in the fetus and newborn however quickly lower in quantity (absolutely or relatively) as myelination progresses. A few oligodendrocytes that occupy areas near blood capillaries are known as perivascular oligodendrocytes. They additionally keep the traditional focus of potassium, which is essential for neuronal exercise, by eradicating after which facilitating its return to the blood. Glycogen breakdown and launch of glucose is completed by the motion of norepinephrine upon receptor molecules within the astrocytes. During embryonic improvement, precursors of astrocytes (radial glial cells) guide the migration of the growing neurons. The superficial processes of astrocytes extend to the surfaces of the brain and spinal twine to kind the exterior glial limiting membrane and expansions that attach to the pia mater (pia�glial layer). They play a serious position in providing a type of scaffolding, or structural help, on which the neurons and their processes are assembled. Astrocytic processes ensheath the initial segments of axons and the naked segments at the nodes of Ranvier. Protoplasmic astrocytes are located primarily in the gray matter and have shorter processes, whereas fibrous astrocytes have longer processes and are positioned primarily within the white matter. This tumor could cause a rise in intracranial pressure, headache, nausea, and vomiting. Supratentorial glioma might produce a shift of the pineal gland, third ventricle, and anterior cerebral arteries, whereas infratentorial tumors are most likely to produce hydrocephalus. Neuron Perineural oligodendrocyte Modified astrocytes are classified into M�ller cells and Bergmann glial cells. In the peripheral form (type 1), sufferers exhibit caf�-au-lait flat cutaneous pigmented spots and Lisch nodules in the iris in childhood. Adults with this type of neurofibromatosis show enhance within the quantity and dimension of the cutaneous spots and in addition develop neurofibromas. The latter are benign tumors normally located on the skin or in the subcutaneous tissue. Mental retardation, epilepsy, spinal deformities, and tumors corresponding to gliomas and pheochromocytoma could complicate this type of the disease.
Order talcilina 500mg without a prescriptionSenile Ectropion Involutional ectropion usually develops on account of laxity of the suspensory system of the lower eyelid antibiotic 3 days uti talcilina 100mg, and the medial and lateral canthal ligaments antibiotic resistance oxford purchase 500mg talcilina, permitting the lid to fall away from the globe infection after sex purchase talcilina 100mg with visa. Surgical therapy: In mild-to-moderate entropion a horizontal spindle of conjunctiva 7�8 mm lengthy antibiotic skin infection cheap talcilina 100 mg on line, four mm excessive and no much less than 5 mm beneath the punctum is excised and sutured to its margins. If the ectropion is most pronounced in the mid-section of the decrease lid, full-thickness lid shortening is really helpful in that space. A line is drawn three mm inferior to the lid margin following the contour of the decrease lid. A pores and skin flap is prepared and a full thickness lid shortening then performed on the lateral canthus as previously described. The excess skin is pulled gently upwards and outward, removed and the skin margins sutured with 7-0 silk. Traction sutures are kept at the level of meeting of the lid margin and are taped to the forehead on the finish of the procedure. Excess skin is Ectropion Eversion of the lid margin and eyelashes away from the globe is identified as ectropion. Acquired, which can be further subdivided into: l Involutional or senile l Cicatricial l Paralytic l Mechanical 2. Congenital the functions of the decrease eyelid are safety of the attention and working of the lacrimal pump. Age and gravity trigger a sluggish relaxation of the lid buildings, particularly the canthal ligaments and the orbicularis, which kind the suspensory system of the lid. Chronic publicity in longstanding ectropion can lead to punctal phimosis, and keratinization of the lid margin and palpebral conjunctiva. A affected person with ectropion is symptomatic because of the epiphora induced and the chronic conjunctivitis caused by exposure. A medial ectropion could be corrected by a modified Lazy T operation, in which a medial vertical pentagon of full-thickness lid is excised 4 mm lateral to the lower punctum as well as an infrapunctal wedge of tarsal conjunctiva and inferior lid retractors. The canaliculi should be recognized and guarded throughout surgery at the medial canthus. In the presence of an entire ectropion, the decrease retractors or the capsulopalpebral tissues have to be reattached as nicely. Whole or split-skin grafts, or flaps of skin are taken from the upper lid, behind the ear or the inner higher arm. Each case have to be handled on its own deserves and can often train the ingenuity of the surgeon. Symblepharon this can be a condition where adhesion of the lid to the globe takes place. Any trigger which produces uncooked surfaces on two opposed areas of the palpebral and bulbar conjunctiva will lead to adhesion if the areas are allowed to stay involved during the means of healing. Bands of fibrous tissue are thus shaped, stretching between the lid and the globe, involving the cornea if this has also been injured. The bands may be slim, however are extra incessantly broad, and should extend into the fornix in order that the lid is totally adherent to the eyeball over a substantial area (symblepharon posterior). Bands limited to the anterior elements not involving the fornix are called symblepharon anterior. Pronounced adhesions trigger impairment of mobility of the attention leading to diplopia. Treatment: the prevention of symblepharon by the early and frequent use of a glass rod or therapeutic bandage contact lens is of the utmost significance. There may be no information as to the constraints of the sclera and tarsus, and nice care has to be exercised lest the globe be punctured. The attachments are launched and the uncooked areas covered with conjunctival, buccal mucous membrane or amniotic membrane grafts. The prevention of the re-formation of adhesions is much more difficult, a therapeutic contact lens could also be used to separate the raw surfaces. Paralytic Ectropion Paralytic ectropion is commonly brought on by a paralysis of the facial nerve, in Bell palsy, parotid surgical procedures, trauma and tumours similar to an acoustic neuroma. Initial conservative remedy with taping of the lids and the use of lubricants allows time for restoration of the palsy. In this operation the palpebral aperture is shortened by uniting the lids at the outer canthus. The edges of the higher and decrease lids are freshened for the requisite distance, the lashes excised, after which sutured collectively as in central tarsorrhaphy. In long-standing paralysis associated with laxity, shortening of the lid and reattachment of the lateral minimize edge to Whitnall ligament could additionally be needed as described in the therapy of involutional ectropion. Associated lagophthalmos brought on by weak point of the superior orbicularis may need taping of the lids at night time or a gold weight placed pretarsally. Cicatricial Ectropion Cicatricial ectropion is commonly the outcomes of burns, trauma and chronic inflammations of the pores and skin which shorten the anterior lamina of the eyelid, i. Treatment of cicatricial ectropion requires launch and leisure of the scarred tissues, and an elongation of the pores and skin muscle lamina by some form of blepharoplasty. Larger scars have to be excised and the encompassing pores and skin Ankyloblepharon this is adhesion of the margins of the 2 lids. Blepharophimosis that is the situation during which the palpebral fissure seems to be smaller than normal. In acquired blepharophimosis the outer angle is commonly normal, however is obscured by a vertical fold of pores and skin formed by eczematous contraction of the skin following prolonged epiphora and blepharospasm (epicanthus lateralis). Mere narrowing of the palpebral aperture is usually called blepharophimosis and may be congenital. The situation could require no therapy, disappearing spontaneously after the irritation has subsided. Elevation of the upper lid is basically a perform of the levator palpebrae superioris, assisted by the frontalis and M�ller muscle. Ptosis is the time period given to a drooping of the upper lid, often because of paralysis or faulty improvement of the levator palpebrae superioris. A purely mechanical ptosis may occur due to deformity and elevated weight of the lid brought about by trachoma or tumour. An obvious drooping of the lid-pseudoptosis-may happen as a result of lack of assist as in phthisis bulbi or anophthalmos. Congenital l Simple l Complicated-associated with ocular motor anomalies, blepharophimosis syndrome and Marcus Gunn ptosis 2. Acquired l Neurogenic l Myogenic l Aponeurotic l Mechanical the condition may be unilateral or bilateral, partial or complete. In the traditional eye the upper lid margin rests halfway between the higher border of the pupil and the limbus. It could additionally be as a result of contraction of the lids from cicatrization or a congenital deformity, ectropion, paralysis of the orbicularis, proptosis due to exophthalmic goitre, orbital tumour, and so forth. Owing to publicity, the cornea turns into keratinized and regularly keratitis sets in.
Purchase talcilina 500mg on-lineThis cortical space is considered the next visual affiliation zone infection en la garganta purchase talcilina 250 mg otc, which receives can you drink on antibiotics for sinus infection buy 100mg talcilina, in its posterior half virus file scanner buy talcilina 250 mg amex, main input from the occipitotemporal cortex virus leg pain cheap 250mg talcilina fast delivery, representing the contralateral visual field. Immediately lateral to the parahippocampal (fusiform) gyrus, the occipitotemporal gyrus makes its course. This projection constitutes the first olfactory heart (Brodmann space 34), which receives and processes olfactory data received from the lateral olfactory stria. Uncal herniation is a situation by which the uncus in addition to the medial portion of the temporal lobe is forced to herniate over the sharp margin of the tentorial notch into the posterior cranial fossa, often as a end result of unilateral supratentorial mass (hematoma or tumor). The swollen uncus may compress the oculomotor nerves and the posterior cerebral arteries and the crus cerebri on the other aspect. Patients with uncal herniation exhibit indicators of ipsilateral or bilateral oculomotor palsy, which incorporates mydriasis (pupillary dilatation) adopted by downward and lateral deviation of the attention, and eventual exterior ophthalmoplegia. Telencephalon 137 towards the anterior fringe of the tentorium (Kernohan notch phenomenon). Irregularities in respiration starting from Cheyne� Stokes respiratory to respiratory arrest additionally happen. They might occur as a end result of a lesion, infarct, or tumor affecting the uncus, the amygdala, and probably the gustatory area. Due to involvement of the temporal lobe, cognitive features, corresponding to reminiscence, orientation, and a spotlight may, also be impaired. In the central herniation (Central Syndrome) the diencephalon and elements of the temporal lobe are displaced by way of the tentorial notch inferiorly (descending tentorial displacement) into the posterior cranial fossa. This downward shift, a probably deadly growth, places an undue pull on the small pontine branches of the basilar artery and lacerates them, producing "Duret hemorrhage" within the ventral and paramedian areas of the upper pons and midbrain. This bleeding may be seen radiographically in the midline at the pontomesencephalic junction. A Kernohan notch may develop on the crus cerebri, compressing the corticospinal tract and producing ipsilateral hemiparesis, a false localizing sign often identified as Kernohan�Woltman syndrome. If the herniation is confined to the diencephalon, the condition may be reversible; nevertheless, herniation that entails the midbrain and higher pons results in deep coma, posturing, Babinski signal with pupillary abnormality (nonresponsive pupil), dysconjugate eyes, and respiratory hyperventilation. In the late stage, deep coma continues and unresponsive and dilated pupils with flaccid palsy of the extremities develop. Ascending central herniation could be confirmed radiographically by an unusually small and even obliterated quadrigeminal cistern. It may also involve the occipitotemporal area (the silent cortical area), which is concerned with the storage of reminiscences from the visual and auditory methods. Bilateral degeneration of the caudate nucleus, dorsomedial putamen, globus pallidus, and locus ceruleus are seen. Loss of the neuronal axons within the cortical white matter and degeneration of the lateral tuberal and dentate nuclei granular cell layer of the cerebellum are also visible. A striking dilation of the lateral ventricles and sparing of the substantia nigra are additional characteristic findings. Damage to this big selection of cortical areas might end in epileptic seizures combined with amnesia, nonfluent aphasia, auditory hallucinations, and the "d�j� vu" phenomenon. Impaired social conduct including lack of appreciation of etiquette, disinhibition, and pacing are additionally noticed. Caudal to the lateral occipital sulcus, the descending occipital gyrus makes its appearance. This lobe also consists of the cuneus and lingual gyrus, which are clearly seen medially. The cuneus, which is bounded rostrally by the parieto-occipital sulcus and caudally by the calcarine fissures, receives visible impulses from the lower quadrant of the alternative visual area. Inferior to the calcarine fissure and medial to the collateral sulcus, the lingual gyrus makes its appearance, receiving enter from the higher quadrant of the other visible field. Rostral to the occipital pole, the lunate sulcus runs vertically between the striate and peristriate cortices. The lunate sulcus, which contains the parastriate cortex, is crossed at its higher and decrease ends by the superior and inferior polar sulci, respectively. Enclosed between the polar sulci is the macular area of the first visible (striate) cortex. A rostral region of this lobe, which lies between the lamina terminalis and the posterior olfactory sulcus, is termed the subcallosal gyrus (paraolfactory gyrus). It is also linked via the diagonal band of Broca to the periamygdaloid cortex. Through this thalamic nucleus, the hypothalamus influences the activities of the cingulate gyrus. This gyrus tasks to the entorhinal cortex and influences the hypothalamus through fibers of the fornix. Due to these various connections, somatic and visceral responses may be elicited by stimulation of the anterior part of cingulate gyrus. It continues anteriorly with the anterior perforated substance and is surrounded by an incomplete circular sulcus. This sulcus is deficient rostrally and inferiorly the place the limen insula is located. Continuation of the insular cortex is marked by the opercular areas of the frontal, parietal, and temporal lobes. It receives enter from the ventral posterior nucleus, medial geniculate body, dorsomedial thalamic nucleus, and pulvinar and intralaminar nuclei, maintaining ipsilateral connections with the primary and secondary somatosensory cortex, inferior parietal lobule, and the orbitofrontal cortex. It has been is suggested that the insular cortex plays an essential modulatory function within the perception and recognition of fantastic contact, auditory impulses, and taste, and is assumed to be associated with language function. This kind of herniation also causes compression of the interventricular foramen of Monro and the lateral ventricle on the same side, leading to asymmetrical ventricles (dilated contralaterally and narrowed ipsilaterally). Obstruction of the ventricular system produces a noncommunicating type of hydrocephalus. Subfalcine herniation could be related to coma and posturing and can be deadly it if progresses to central herniation. It lies on the lateral aspect of the gyrus Retzius, an inconstant protrusion from the posterior part of the parahippocampal gyrus inferior to the splenium. The frontal lobes are related by the forceps minor, an extension of the genu of the corpus callosum. Fibers of the trunk and splenium form the tapetum, which constitutes the roof and the lateral walls of the posterior and inferior horns of the lateral ventricle. Agenesis of the corpus callosum, a uncommon congenital condition, is characterized by an entire or partial failure of the corpus callosum to develop, ensuing within the look of Probst bundles. These bundles run in a rostrocaudal direction within each half of the cerebral hemisphere and substitute the fibers that cross the midline and join the two hemispheres of the brain. Chromosomal abnormality, inherited genetic issues, prenatal infections, toxic or traumatic accidents, and metabolic problems are thought-about as possible causes of this situation. It has been proposed that a molecular dysfunction that undermines the signaling mechanism essential within the development of the elements of the corpus callosum occurs on this situation, as properly as other abnormalities collectively generally recognized as ciliopathies.
250mg talcilina saleThe extraocular muscular tissues are completely different from other striated muscles in the physique in sure necessary features triple antibiotic ointment trusted talcilina 500mg. They are small in size with a small motor unit and one motor axon supplying solely six muscle fibres bacteria doubles every 20 minutes order talcilina 100 mg visa. They have specialized muscle spindles and there are two several varieties of muscle cells antimicrobial 220 250mg talcilina overnight delivery, small and enormous inside each muscle antibiotic quick guide purchase 500mg talcilina otc. The large fibres are located centrally, have a fast twitch response and have a single motor finish plate. To control their actions all these muscle tissue are supplied with fascial verify ligaments intimately linked with the perimuscular sheath, Tenon capsule and the periosteum. The Action of the Extraocular Muscles these rotate the eye round a centre of rotation, which lies within the horizontal plane some 12 or 13 mm behind the cornea, and in each motion of the globe each muscle is involved to some extent, both by contraction or inhibition Table 25. Rotation around the vertical axis whereby the globe is turned from side to facet 2. Rotation across the horizontal axis whereby the globe is turned upwards and downwards, and three. Rotation around the anteroposterior axis-an involuntary motion of torsion; intorsion when the higher pole of the cornea rotates nasally, extorsion when temporally. Thus, when the superior rectus acts upon the globe within the major place, it not solely pulls the attention upwards but additionally inwards and intorts it. Similarly, when the inferior rectus acts the eye is pulled downwards and inwards and extorted. The superior and inferior indirect muscular tissues rotate the attention nasally (intorsion) and temporally (extorsion). Since the obliques are inserted behind the centre of rotation, their efficient action is to pull the back of the eye forwards and inwards. Therefore, when the superior oblique contracts, if the globe is in the primary position, the primary impact is intorsion but it additionally rotates the attention downwards and outwards; the inferior oblique primarily causes extorsion but additionally rotates the globe upwards and outwards. The superior rectus and inferior oblique act simultaneously to move the eye instantly upwards, the upward motion brought on by every muscle being summated, while the inward motion and torsion of the superior rectus is strictly compensated by the outward movement and opposite torsion of the inferior oblique. In the first position, three-quarters of its efficiency is dedicated to vertical rotation and one-quarter to torsion. Abduction of one eye is accompanied by adduction of the other- which is identified as a conjugate motion. The only exception to this rule is the bilateral adduction of the eyes in convergence and abduction of both eyes in divergence (dysconjugate movements). Elevation of each eyes is accompanied by slight abduction (divergence), depression by slight adduction (convergence). In these movements the muscles which contract collectively are known as synergists; those which endure inhibition, antagonists. Thus in rotation to the best (dextroversion) the synergists are the right lateral rectus and left medial rectus, while the antagonists are the proper medial rectus and left lateral rectus. In rotation upwards synergists are the proper and left superior recti primarily and the right and left inferior obliques secondarily. The antagonists are the best and left inferior recti and proper and left superior obliques. Nervous Control of Ocular Movements Laws Governing the Neural Control of Ocular Movements Laws governing the neural control of ocular actions are as follows. Equal and simultaneous innervation flows from the brain to a pair of synergistic (yoke) muscular tissues which contract concurrently in conjugate binocular movements. For instance, in laevoversion, the lateral rectus of the left eye and medial rectus of the proper eye obtain an equal and simultaneous flow of innervation; during convergence, both medial recti; and so on. Sherrington regulation of reciprocal innervation: During the initiation of an eye fixed movement, elevated innervation to an extraocular muscle is accompanied by simultaneous inhibition (a reciprocal decrease in innervation) of the direct antagonist of the contracting muscle of the identical eye. Finally, these intermediate centres are linked with the vestibular apparatus whereby they turn into associated with the equilibration reflexes and the cerebral cortex so that voluntary movements and participation in the higher reflexes involving notion become possible. The oculomotor, or third cranial nerve, provides all of the extrinsic muscles besides the lateral rectus and superior indirect. The superior oblique is supplied by the trochlear (fourth) nerve and the lateral rectus by the abducens (sixth) nerve. The cells nearest the midline in path of the anterior part of the third nucleus are smaller than the others: they kind the Edinger�Westphal (and Perlia) nucleus which supplies fibres to the ciliary muscle (accommodation) and sphincter pupillae (constriction of the pupil). A single, central, caudally located nucleus innervates each levator palpebrae superioris muscle tissue. Paired bilateral subnuclei that innervate the superior recti have crossed projections that cross by way of the alternative subnucleus and be a part of the nerve of the other side. Paired bilateral subnuclei with uncrossed projections innervate the medial recti, inferior recti and inferior indirect muscles. Parasympathetic input to the sphincter muscle of the iris and ciliary body arises from the single Edinger�Westphal nucleus. The clinical relevance of figuring out this innervation pattern is to distinguish nuclear from non-nuclear third nerve palsy. A bilateral third nerve palsy with out ptosis indicating sparing of the single levator subnucleus and a unilateral third nerve palsy with contralateral superior rectus involvement and bilateral ptosis are each indicative of compulsory nuclear involvement. Unilateral ptosis, unilateral inner ophthalmoplegia and unilateral exterior ophthalmoplegia with regular contralateral superior rectus function are conditions that exclude a nuclear lesion. Nearly, if not fairly, all of the fibres decussate within the superior medullary velum and are distributed to the superior indirect muscle of the opposite aspect. Hence, vascular and other lesions of the sixth nucleus are very liable to be accompanied by facial paralysis on the same facet. All the fibres of the sixth nerve are distributed to the ipsilateral lateral rectus. The peculiarities of distribution of the fibres from the third, fourth and sixth nuclei to muscles partly on one facet and partly on the alternative facet of the body present that the nervous mechanism of coordination of those muscles is extremely complicated. The intermediary mechanism coordinating the actions of these nuclei is also complicated. These fibres have essential features in the coordination of movements and equilibration, that are so intimately related with imaginative and prescient. The nuclei are additionally interrelated through this bundle in order that coordination of the two eyes is maintained. So long as the fixation level (F) is imaged on every macula, the fixation reflex maintains the posture of the eyes steady by an equality of muscular tone (thin solid black arrows). The afferent path is: (a) retinae n optic nerve n chiasma n right optic tract; (b) lateral geniculate physique n proper optic radiations n striate space of occipital cortex; (c) peristriate occipital cortex. The frontal cortex has an area which controls quick fixational eye actions to the alternative side.
Talcilina 250 mg with mastercardAn injury to the suprascapular nerve produces atrophy of the supraspinatus and infraspinatus muscle tissue and associated weakness of the lateral rotation (arm will be in a pronated place near the chest wall) and abduction of the arm as a lot as antibiotics for uti missed period order talcilina 500mg on-line 15� ranging from the midline antimicrobial needleless connectors discount talcilina 250 mg without a prescription. Thus antibiotic antimycotic purchase talcilina 500 mg free shipping, initiation of abduction of the arm from the vertical position next to the chest becomes inconceivable antibiotics for dogs after teeth cleaning purchase talcilina 100mg free shipping. Inability to use the hand on the affected aspect to comb the again of the pinnacle and, when writing, a continuing have to displace the medium being written upon away from the affected facet towards the intact aspect are some of the indicators that a affected person experiences because of suprascapular nerve palsy. Pain sensation is confined to the posterior 234 Neuroanatomical Basis of Clinical Neurology shoulder. Compression at the spinoglenoid notch spares the supraspinatus but impacts the infraspinatus; thus, initiation of abduction is preserved. Atrophy and flattening of the supraspinous and infraspinous fossae within the elderly may not be diagnostic because of wasting of these muscular tissues with growing older. This will elicit a extreme ache if the suprascapular nerve is entrapped, significantly inside the suprascapular foramen. The nerve to the subclavius (C5, C6), because the name implies, supplies the subclavius muscle, which acts as a cushion that stops rupture of the subclavian artery in clavicular fracture. Pain and paresthesia exacerbated by extension of the forearm on the elbow and eventual impairment of the cutaneous sensation in the lateral half of the forearm can also, though uncommonly, be observed on this harm. Heavy objects placed on the forearm and supported by the elbow might particularly compress the lateral antebrachial cutaneous department of this nerve. Due to the overlap between sensory branches of the lateral antebrachial cutaneous nerve and the superficial branches of the radial nerve that offer the lateral forearm, sensory deficits is probably not outstanding. For the same reason, damaged lateral antebrachial nerve can be surgically removed and used as a graft. Coracobrachialis can be tested by flexing in opposition to resistance the laterally rotated arm. It pierces the coracobrachialis muscle, runs between the biceps brachii and brachialis where it lies close to the radial nerve, and continues to the forearm, lateral to the tendon of biceps brachii as the lateral antebrachial cutaneous nerve. The musculocutaneous nerve provides the flexors of the elbow similar to coracobrachialis, brachialis, and biceps brachii and offers articular branches to the elbow joint. It also supplies cutaneous innervation to the lateral facet of the forearm by way of the lateral antebrachial cutaneous nerve. The department to the coracobrachialis arises earlier, whereas branches that supply the biceps brachii and brachialis emanate from the nerve after piercing the coracobrachialis. The lateral pectoral nerve (C5, C6, C7) is larger than the medial pectoral nerve and passes inferior to the clavicle and across the subclavian vessels earlier than it reaches the axillary fossa where it accompanies the thoracoacromial artery and provides the pectoralis major muscle after piercing the clavipectoral fascia. The lateral twine offers rise to the lateral root (C5, C6, C7), which joins the medial root from the medial twine and varieties the median nerve. Intactness of the lateral pectoral nerve is examined in the supine place by flexing the arm whereas the forearm extended and the contralateral shoulder is pressed towards the examination table. Terminal Branches of medial wire the medial twine provides rise to the medial pectoral, medial brachial, medial antebrachial, and ulnar nerves, in addition to to the medial root to the median nerve. Integrity of the pectoralis minor could be tested by asking the affected person to extend his arm and move his/her shoulder anteriorly whereas the examiner hand pushes the shoulder in the different way. It may be replaced by Injury to the musculocutaneous nerve, although uncommon, outcomes from a fracture of the humerus, shoulder dislocation, positioning of the arm during surgery, entrapment inside a hypertrophied coracobrachialis muscle, and from hereditary neuralgic amyotrophy. Common manifestations of this harm are atrophy of the biceps brachii and flattening of the anterior surface of the arm, weakened flexion of the arm, markedly weakened flexion of the forearm, weakened supination, and instability of the shoulder joint. This nerve travels medial to the brachial artery and basilic vein and supplies cutaneous fibers to the medial floor of the distal third of the arm. The anterior department innervates the skin of the anterior surface of the medial forearm all the method down to the wrist to join with the cutaneous branches of the ulnar nerve. The posterior department supplies the corresponding areas on the posterior floor of the medial forearm, establishing communication, in the identical method, with the sensory branches of ulnar and radial nerves. In the decrease medial arm, the ulnar nerve runs between the olecranon and medial epicondyle after which in the ulnar nerve sulcus on the medial epicondyle of the humerus accompanied by the superior ulnar collateral artery. In the proximal and distal thirds of the arm, the ulnar nerve receives blood provide from the adjoining ulnar collateral arteries, making potential to use this segment of the nerve for transplant in evulsion accidents. It then enters the cubital tunnel, which is bounded anteriorly by the medial epicondyle and medially by the medial collateral ligament and fibrous capsule. The roof of the tunnel is shaped by a fibrous band that connects the medial epicondyle to the olecranon and the tendinous origin of the flexor carpi ulnaris. It descends additional between the 2 heads of the flexor carpi ulnaris and then between the flexor carpi ulnaris and medial half of flexor digitorum profundus to which it supplies motor innervation. During its course in the forearm, the ulnar nerve is accompanied by the corresponding vessels. Proximal to the wrist, the ulnar nerve provides rise to the dorsal and palmar cutaneous branches. The dorsal cutaneous department runs deep to the decrease part of the flexor carpi ulnaris after which programs ahead to the dorsal floor along the medial border of the hand, superficial to the flexor retinaculum. It supplies the dorsal surfaces of the fifth digit, the adjacent sides of the fourth digit, and the medial side of the third digit with the exception of areas supplied by the median nerve. The palmar cutaneous branch arises from the midanterior forearm and supplies the pores and skin of the medial facet of the palm. The superficial terminal branch supplies palmaris brevis and the skin of the palm, the fifth digit, and the medial aspect of the fourth digit. Through the deep terminal department, the ulnar nerve innervates the hypothenar, interossei, two medial lumbricals, and the adductor pollicis. Fibers of the ulnar nerve that offer the intrinsic muscles of the hand run throughout the median nerve in about 20% of individuals after which leave the median nerve distal to the elbow to join the ulnar nerve once more (Martin�Gruber anastomosis). This anomalous connection, which is frequently seen on the proper facet, is believed to be an autosomal dominant situation. At the thenar eminence, the deep branch of the ulnar nerve could communicate with the recurrent branch of the median nerve to type the Riche�Cannieu anastomosis. This neural anastomosis permits the ulnar nerve to innervate the abductor pollicis longus, flexor pollicis brevis, opponens pollicis, and the lateral two lumbricals, and enables the ulnar nerve to innervate practically all hand muscular tissues and cutaneous areas. After exiting the canal of Guyon, the ulnar nerve innervates the dorsal and palmar interossei, the adductor pollicis (in about 55% of individuals), the 2 medial lumbricals, and all hypothenar muscles: the abductor, flexor, and opponens digiti minimi. It additionally offers cutaneous innervation to one and a half of the medial portion of the palm and dorsum of the hand via the palmar and dorsal cutaneous branches. In approximately 20% of the inhabitants, the ulnar nerve carries sensation from the pores and skin of the complete fourth (ring) finger and medial half of the fifth finger. Ulnar nerve injuries happen in fractures involving the medial epicondyle, dislocation of the elbow, and entrapment within the Guyon canal. It also can happen because of compression between heads of the flexor carpi ulnaris, extended leaning on the elbow (Vegas neuropathy), sustained flexion of the elbow, cubitus valgus deformity (tardy ulnar palsy), or entrapment inside the cubital fossa (cubital tunnel syndrome). Application of tourniquets, pitching, irritation and calcification of the medial collateral ligament, and positioning on the working table can also contribute to the damage of the nerve.
Buy talcilina 500 mg lineImmunocompromised antibiotics for dogs with parvo buy talcilina 250 mg on line, organ-transplant patients virus hunter island buy talcilina 100 mg with mastercard, patients with lymphoma antibiotic pronunciation order talcilina 100mg without a prescription, and aged sufferers who experience waning of varicella-specific immunity are particularly susceptible to antibiotics wiki purchase talcilina 250 mg line this disease. The virus establishes latent infection in perineuronal satellite tv for pc cells of the dorsal root ganglia or sensory ganglia of the cranial nerves. Initially, patients exhibit myalgia, probably fever, fatigue, and nuchal rigidity followed by unilateral dull, imprecise, and diffuse pain. Within a number of days, well-localized lancinating burning ache turns into evident accompanied by herpetic blisters within the area of distribution of the sensory fibers of the ventral rami of the spinal nerves. Virtually all the ventral rami of the thoracic spinal nerves, with one exception of the ventral ramus of T12, run within the intercostal sulci because the intercostal nerves (between the inner and innermost intercostal muscles), innervating the intercostal muscular tissues, thoracic and belly walls, and the gluteal region, as nicely as the higher extremity. In addition to forming the first intercostal nerve, the ventral ramus of the primary thoracic nerve contributes a big branch to the brachial plexus. The ventral ramus of the first thoracic spinal nerve lies dorsal to the stellate ganglion and pursues a course posterior to the cervical pleura (cupola) to reach the space between the anterior and middle scalene muscular tissues. A specific department, the intercostobrachial nerve, arises as the lateral cutaneous nerve from the second intercostal nerve (sometimes the third intercostal nerve) and joins the brachial plexus supplying the skin of the higher part of the medial arm. The higher six intercostal nerves provide the thoracic wall, costal pleura, the diaphragm, and the diaphragmatic pleura and peritoneum, while the decrease 5 intercostal (thoracoabdominal) nerves course between the inner indirect and transverse abdominis muscles, piercing the anterior layer of rectus sheath, innervating the pores and skin and muscle tissue of the anterior abdomen, in addition to the peritoneum. The ninth through the eleventh intercostal nerves pierce the diaphragm and then enter the pass through the interior indirect. The tenth intercostal nerve provides the skin of the umbilicus, whereas the seventh, eighth, and ninth intercostal nerves 248 Neuroanatomical Basis of Clinical Neurology Lesions happen unilaterally, are primarily confined to the thoracic and lumbar segments, and often heal inside weeks. The cutaneous rashes could not at all times be seen significantly in the inguinal area and across the mammary gland. Inflammation and unfold of virions can also contain the ventral and dorsal horns of the spinal wire and related meninges producing occult focal poliomyelitis. It may also spread to the cerebral vasculature causing vasculopathy and vasculitis leading to stroke and meningoencephalitis. When the neuropathic ache (combination of pain and numbness) turns into chronic and persists longer than three months, postherpetic neuralgia will develop. Age, intensity of prodrome, and acute phases of this illness predispose patients to postherpetic neuralgia. Muscle weak spot is anticipated, and when the virus affects the lower 5 or 6 thoracic spinal nerves, stomach muscle palsy could ensue resulting in loss of superficial stomach reflex and potential hernia. Herpes zoster can have an result on the geniculate and trigeminal ganglia, producing herpetic lesions within the skin of the concha of the ear and areas of distribution of the ophthalmic (ophthalmic zoster), maxillary, and mandibular nerves. Ophthalmic nerve involvement is often indicated by rashes on the tip of the nostril and could be accompanied by critical consequence such as keratitis, corneal ulcer, iritis, and even retinal cell necrosis. Rarely, a extreme form of reflex sympathetic dystrophy with causalgia and manifestations of Horner syndrome are seen. Ramsay Hunt syndrome is a consequence of herpes zoster of the geniculate ganglion of the facial nerve (geniculate herpes), which causes vesicular eruption in the concha of the pinna and may produce vertigo, tinnitus, and neuronal deafness. Antivirals (acyclovir) are the mainstay medications in the treatment of the preliminary stage of this condition. Opioids and corticosteroids with tricyclic drugs may be used for treatment of this condition. Cardiac ache, generally felt on the left side of the medial arm, forearm, and fifth digit, is attributed to activation of the sensory neurons throughout the first thoracic spinal phase. The neurons in the first thoracic spinal section present each sympathetic presynaptic fibers to the cardiac plexus and cutaneous fibers to the medial arm, forearm, and fifth digit through the medial antebrachial and brachial cutaneous nerves as nicely as the sensory branches of the ulnar nerve to the medial hand (T8�T1). It has been suggested that the paincarrying afferent fibers from the center to T1 spinal phase that accompany the sympathetic fibers decrease the brink of the sensory neurons within that particular section. This change in neuronal threshold renders the traditional cutaneous impulses that stream to T1 from corresponding dermatomes painful. Others counsel that convergence of pain-carrying afferents from the heart with that of afferents from skin dermatomes onto the same neuronal section ends in mind misinterpretation of the source of the pain as if it is emanating from the corresponding pores and skin dermatomes rather than the guts itself. Contraction of the belly muscles in response to cutaneous stimulation of the stomach confirms the truth that the intercostal nerves subserve twin function of cutaneous and muscular innervation of the anterior stomach wall. Rebound rigidity observed within the anterior abdomen of patients with appendicitis or diverticulitis relies on the truth that irritation of the parietal peritoneum adjoining to the infected appendix stimulates the intercostal nerves that innervate the peritoneum, skin, and stomach muscular tissues producing the observed rigidity. Thoracic spinal nerve roots are not often affected as a result of the restricted rotatory movement between the thoracic vertebrae. When it happens, the prolapse is huge and it more than likely to contain the mid and lower thoracic ranges. However, direct trauma or most cancers metastasis may cause collapse of the thoracic vertebrae and subsequent compression of the thoracic spinal nerve roots. Referred ache from inside organs and herpes zoster have to be considered when coping with thoracic pain. Due to involvement of the lower 5 - 6 thoracic spinal nerves within the innervation of the belly muscles, careful inspection of these muscle tissue in thoracic nerve root accidents could also be essential. Radicular damage to the thoracic spinal nerves causes ache within the corresponding dermatomes, which appears as band as is seen in shingles. Due to the breadth of a thoracic root dermatome, the lateral and ventral components are displaced cranially enabling the dorsal and ventral branches of a thoracic spinal nerve to meet. It entails the mid and decrease thoracic a half of the vertebral column, however generally distal to T8 with T11/T12 as the most common level. Herniated Spinal Nerves 249 disks calcify, and as a result, fragments unfold to trigger nerve root compression. Repetitive or prolonged bending ahead, rotating the spine, poor posture (slouching), driving, and lifting can predispose a person to this type of herniation. Patients experience a sudden extreme onset of mid back ache within the upper again on one or either side of the spine. It could show radiation following dermatomal sample across the ribs, upper extremity, or abdominal wall, exacerbated by coughing or sneezing. Lower thoracic root rupture could cause paralysis of the unilateral belly muscle tissue. However, cutaneous manifestations of herpes zoster and referred ache from diseased pulmonary, cardiovascular, gastrointestinal, or urogenital organs have to be considered when evaluating this condition. Loss of sensation in the whole medial leg, impairment of sweating in the territory of the saphenous nerve, and patellar hyporeflexia are pathognomic for femoral nerve palsy. Manifestations of L5 root lesion, that are widespread, embody pain in the anterolateral leg and center portion of the dorsum of the foot. The muscle throughout the anterior compartment of the leg, which is constantly affected, is the extensor hallucis longus with lack of posterior tibial reflex and preservation of patellar and ankle reflexes. Tibialis posterior reflex is elicited by tapping muscle tendon inferior and anterior to the medial malleolus producing inversion, adduction, and plantar flexion of the foot. However, when S1 can also be concerned, paresis of the extensor digitorum brevis is often noticed.
Buy 100 mg talcilina with visaIt is usually unilateral virus killer 100mg talcilina visa, males being more commonly affected (2:1) bacteria 68 purchase 500mg talcilina otc, and happens typically within the older population (50�80 years of age) virus from mice generic 500 mg talcilina amex. Ocular indicators embody dilated retinal veins with irregular calibre but no tortuosity antibiotics for acne and the pill order talcilina 100 mg without a prescription. Mid-peripheral retinal haemorrhages are seen in 80% of patients, rubeosis iridis or neovascularization of the iris in 66% and posterior segment neovascularization in 37%. Diabetes mellitus (may produce similar manifestations), however is usually bilateral, with characteristic exhausting exudates. Aortic arch disease caused by Takayasu arteritis, aortoarteritis, atherosclerosis and syphilis should also be appeared for and excluded. If vasospastic calcium-channel blockers Evaluation contains examination of the peripheral pulses, cardiac and carotid auscultation, echocardiogram, recording of the blood stress and investigations for diabetes mellitus and hyperlipidaemia. Treatment: this consists of controlling chronic systemic illnesses corresponding to diabetes mellitus and hypertension. The affected person ought to be suggested to give up smoking and lose weight and reduce cholesterol levels if raised. Vertebrobasilar Insufficiency Aetiopathogenesis: this can be a vasculopathic illness affecting the vertebrobasilar arterial supply. It manifests with signs due to ischaemia of the brainstem and occipital cortex. Risk components embody diabetes mellitus, hypertension, hyperlipidaemia and cervical spondylosis. Clinical options: these include episodes of transient blurred vision occurring bilaterally, lasting a few seconds to a few minutes which are generally accompanied by flashing lights. Other related signs that might be current are transient diplopia, ataxia, vertigo, dysarthria, perioral paraesthesia, dysphasia, hemiparesis or hemisensory loss. The affected person may also give a history of drop assaults (sudden episodes of falling to the bottom without warning or lack of consciousness). Differential prognosis: this contains other causes of transient visible loss Table 31. X-rays of the cervical spine to rule out compressive disease of the cervical backbone (degenerative changes especially osteophytes encroaching on the arterial foramina) are also required. Treatment: this consists of non-specific measures as in occlusive carotid artery disease. Cerebral Haemorrhage and Thrombosis In the occipital cortex, the posterior cerebral artery is usually involved; it provides most of the occipital cortex and much of the temporal lobe. Obstruction of the center cerebral artery produces visual agnosia with a crossed homonymous subject defect affecting, preferentially, the higher quadrants of the sphere by involvement of the inferior optic radiations looping ahead within the temporal lobe. An acute lesion of the premotor frontal cortex affecting the frontal eye field causes a conjugate deviation of the eyes away from the aspect of the lesion as an irritative phenomenon, which is reversed later when paresis units in so the deviation is to the identical facet as the lesion. The pupils are extremely small-an essential diagnostic sign in a comatose affected person. Obstruction of the branches of the basilar artery in the brainstem produces signs relying on the implication of the ocular motor nuclei and the pyramidal tracts. Obstruction of the posterior inferior cerebellar artery provides rise to a characteristic clinical picture resulting from infarction of a wedge-shaped area on the lateral facet of the medulla. Cortical Blindness Aetiopathogenesis: the commonest trigger is bilateral occipital lobe infarction. In both cases, the central macular area is spared with preservation of some central imaginative and prescient as a end result of twin blood supply from the posterior cerebral artery (a department of the vertebral artery), and the posterior communicating artery (a department of the internal carotid artery system). Bilateral occipital infarcts end in cortical blindness characterized by its denial (Anton syndrome). A much less widespread cause is a neoplasm involving the occipital cortex which could possibly be a falcotentorial meningioma or a number of metastases. Migraine it is a periodic, typically unilateral, throbbing or boring headache accompanied by nausea, vomiting, temper changes, fatigue and visual disturbances. The word hemicrania was, with the passage of time, corrupted to hemigranea and then migrania, till the French translation migraine gained acceptance. However, over the past 50 years, attention has been focused on the idea that migraine is analogous to epilepsy and that clinically apparent circulating phenomena are actually secondary to neurophysiological changes in the cerebral cortex. Activation of any considered one of these phases is sufficient for the manufacturing of headache and one phase may appear to dominate in a particular migrainous syndrome. Pharmacological information recommend serotonin receptors as being mainly responsible for triggering the neural origin of migraine. Migraine has been postulated to characterize a hereditary perturbation of serotonergic neurotransmission. Clinical features: Migraine impacts practically 10% of the inhabitants and is characterised by headache, however has been categorized into numerous subtypes according to the constellation of symptoms seen Table 31. When unilateral, in the majority of cases the headache modifications sides to the other side of the top in different episodes. May have focal neurological disturbances with out headache or vomiting and are referred to as migraine equivalents or accompaniments. Migraine with dramatic focal neurological features, thus overlapping with traditional migraine, but within the latter the signs precede the headache whereas in sophisticated migraine they occur at the peak of the headache and persist longer. The term connotes a persisting neurological deficit that is a residuum of a migraine assault or when the neurological deficit outlasts the headache Complicated migraine excess of sleep, emotional stress or bright lights. In migrainous ladies, the attacks are recognized to cease throughout pregnancy after the second trimester. Attacks occur in cycles of several months to a yr, and become much less frequent and less severe with rising age. Characteristic visible disturbances related to classical migraine embrace zigzagging flashing lights (fortification spectra), blurred imaginative and prescient, or a visible field defect lasting 15�30 minutes, normally previous the headache. The onset could be at the top of the headache but, more commonly, it follows the headache. Focal motor deficits, speech dysfunction, paraesthesiae of the extremities, face, tongue or lips and even hemiplegia with total paralysis or weak point on one aspect of the physique (hemiplegic migraine) are all identified to occur. Ophthalmoplegic-ipsilateral paralysis of a quantity of extraocular muscular tissues often happens because the migrainous headache is resolving. Basilar artery migraine-mimics vertebrobasilar arterial insufficiency with bilateral blurring of imaginative and prescient or blindness, diplopia, vertigo, gait disturbances, fashioned visible hallucinations and dysarthria. It is price remembering that the majority of unilateral migraine headaches do, in some unspecified time in the future, change sides, so sufferers who always develop a headache on the identical facet of the pinnacle may have a more critical neurological disorder. If headache precedes the visible signs, even though this will happen in complicated migraine, the risk of different circumstances during which this order of occasions is more likely, corresponding to arteriovenous malformations, mass lesions with cerebral oedema and an epileptiform seizure focus, should be considered and ruled out. Work-up of patients features a detailed historical past and cautious ocular examination together with refraction and neurological examination, ideally by a neurophysician. Hypertension and a low blood sugar level should be appeared for as hypoglycaemic complications may be triggered by stress and fatigue. Treatment: Patients should be requested to avoid all brokers or annoying events identified to set off attacks so far as potential. Patients with infrequent headaches should be advised to take analgesics (such as aspirin, paracetamol, ibuprofen, naproxen sodium, nimesulide) as soon as possible after the onset of the headache.
References - Determan RM, Royakkers A, Wolthuis EK, et al: Ventilation with lower tidal volumes as compared to conventional tidal volumes for patients without acute lung injuryóa preventive randomized controlled trial, Crit Care 14:R1, 2010.
- Satran A, Dawn B, Leesar MA. Congenital ostial left main coronary artery stenosis associated with a bicuspid aortic valve in a young woman. J Invasive Cardiol. 2006;18(3):E114-E116.
- Adam, E.J., Desai, S.C., Lawton, G. Racial variations in normal ureteric course. Clin Radiol 1985;36:373-375.
- Louw JH, Cywes S. Extralobar pulmonary sequestration communicating with the oesophagus and associated with a strangulated congenital diaphragmatic hernia. Br J Surg 1962;50:102.
- Asplund R, Sundberg B, Bengtsson P: Oral desmopressin for nocturnal polyuria in elderly subjects: a double-blind, placebo-controlled randomized exploratory study, BJU Int 83:591, 1999.
- Sanders RJ, Hammond SL: Venous thoracic outlet syndrome, Hand Clin 20:113-118, viii, 2004.
- Tsubokura T, Yamazaki H, Masui K, et al: Comparison of image-guided intensity-modulated radiotherapy and low-dose rate brachytherapy with or without external beam radiotherapy in patients with localized prostate cancer, Sci Rep 8(1):10538, 2018.
|