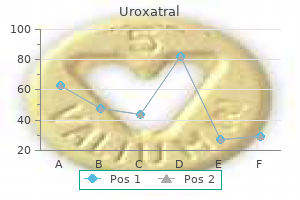
Uroxatral
Brian Murphy, RN - Critical Care Department
- Little Company of Mary Hospital
- Evergreen Park, IL
Order uroxatral 10 mg fast deliveryIn sufferers with coronary artery illness prostate cancer definition generic uroxatral 10 mg, excessive reduction in diastolic blood strain can compromise myocardial blood move during diastole and induce ischemia prostate quadrants cheap uroxatral 10 mg without a prescription. Therapy have to be individualized based on the perceived risks of myocardial ischemia prostate 5k greensboro buy generic uroxatral 10 mg on line, with a objective to maintain diastolic blood strain >65 mmHg man health georgia erectile dysfunction gallery generic uroxatral 10mg free shipping. All patients with persistent symptomatic heart failure should receive ongoing schooling in way of life modifications to improve their high quality of life, together with discount in dietary sodium, participation in average cardio exercise actions as tolerated, and relevant self-monitoring and self-efficacy behaviors as described in Chapter thirteen. Physical training has been proven to be safe and related to improved practical capacity in patients with coronary heart failure with each preserved and decreased ejection fraction. Sildenafil at doses ranging from 25 mgͱ00 mg daily has been proven to be nicely tolerated in patients with heart failure with useful capacity that permits sexual activity. These brokers also needs to be used with warning in patients taking alpha-adrenergic receptor blockers for remedy of prostatic hypertrophy. Most sufferers with continual coronary heart failure respond well to optimal medical therapy, with reduction in congestive indicators and symptoms and improved practical capacity. These patients should be adopted inside the follow setting of the first care provider and/or heart specialist at three- to six-month intervals as decided by the severity of signs. Patients with high-risk options (hospitalizations, a number of comorbidities) ought to be seen more incessantly and may benefit from referral to specialized coronary heart failure facilities as described in Chapter thirteen. Oncedaily medications and fixed-dose mixture medications should be used when feasible to simplify the medical routine. It is necessary to interact the affected person in a non-judgemental manner to elicit limitations to full adherence, and develop plans to tackle these barriers. Most patients would prefer to take fewer tablets and are naturally skeptical of lifelong prescriptions. A simple evaluation of all medicines at every visit, with the acknowledged intention to find any which may be now not needed, and a quick reinforcement statement for the aim of the drugs to be continued may enhance adherence. Medical decision-making for ambulatory heart failure sufferers is usually thought-about to be advanced due to the underlying advanced pathophysiology, polypharmacy, and excessive risk of mortality and different opposed clinical outcomes. Medical document documentation for every coronary heart failure affected person encounter should include a complete evaluation of typical and atypical symptoms, an in depth physical examination that features typical and atypical signs of congestion, a comprehensive assessment that includes assertion of the illness stage (per American College of Cardiology and American Heart Association guidelines), the functional class (per New York Heart Association classification), the quantity status of the patient (hypovolemic, optimum, or hypervolemic), evaluation of optimization of medical and device therapy, and an announcement on affected person self-management education (Table 9. Incorporation of mixed nursing and physician participation throughout patient encounters is another useful technique for optimization of therapy and schooling. Assessing and grading congestion in acute heart failure: a scientific statement from the Acute Heart Failure Committee of the Heart Failure Association of the European Society of Cardiology and endorsed by the European Society of Intensive Care Medicine. Is worsening renal perform an ominous prognostic sign in patients with acute heart failure? Amiodarone or an implantable cardioverterdefibrillator for congestive coronary heart failure. Efficacy and security of sildenafil citrate in men with erectile dysfunction and chronic heart failure. Patients with severe limitation of useful capability have a excessive risk of hospitalization and dying, independent of ejection fraction. If no reversible causes of disease progression are identified, patients should be evaluated for superior therapies (cardiac transplantation or mechanical circulatory support), or if not eligible for such therapies, for palliative care and hospice referral. It is affordable to contemplate reduction of dose or withdrawal of neurohormonal antagonist therapy in sufferers with advanced heart failure and insupportable unwanted effects. It is affordable to consider deactivation of implantable cardiovertor defibrillators in sufferers with advanced heart failure and estimated survival of lower than one yr. Vasodilators and optimistic inotropic brokers may be used acutely and chronically to alleviate symptoms in this population as part of a complete palliative care program. Clinical Assessment the characterization of superior coronary heart failure (Stage D) is primarily decided by the useful capacity of the affected person rather than the left-ventricular ejection fraction. Patients with superior coronary heart failure have poor high quality of life as a end result of severely decreased practical capability despite optimum medical and system remedy. Simple actions of every day dwelling similar to bathing and dressing can induce extreme dyspnea, typically require lengthy, frequent rests to full the duty, and leave the patient feeling exhausted. Other distressing signs on this group included profound fatigue, sleep disturbance, restlessness, lethargy, poor focus, sixty seven hair loss, alteration of style sensation, sexual dysfunction, and anorexia with weight reduction. Careful questioning about symptoms during specific activities is important, as many sufferers slowly curtail activities that produce dyspnea or fatigue without aware acknowledgement of their change in lifestyle, and are available to settle for frequent dyspnea and fatigue with minimal exertion as a "regular" facet of their coronary heart condition. If a severe limitation in functional capability is detected, the affected person should be further questioned about day-to-day changes within the symptoms, since patterns in the day by day severity of symptoms can generally assist determine remedy methods. Specific questions on sleep patterns and the bodily symptoms that interrupt sleep may also be useful to determine strategies to reduce fatigue. Specific information on patterns of meals intake can establish strategies to enhance diet and stamina. Depression, chronic ache, impaired concentration, and an uncomfortable sense of restlessness are widespread symptoms in this stage of the illness. Specific questions on these issues are useful to establish these situations as potential targets for palliative remedy. On physical examination, patients with superior coronary heart failure typically show cachexia (characterized by bitemporal wasting, wasting of the musculature of the shoulder girdle, and generalized muscle atrophy) and seem fatigued. In sufferers with advanced heart failure and lowered ejection fraction, the pulse stress is commonly narrowed, with a thready pulse or pulsus alternans evident on palpation of the radial artery. Laboratory knowledge will usually reveal worsening pre-renal azotemia and hyponatremia. Anemia can additionally be extra common in patients with advanced coronary heart failure, in all probability because of a mixture of factors that reduce pink cell manufacturing and enhance hemodilution. Diuretic resistance is one other scientific marker of low-cardiac-output syndrome in patients with different options of advanced heart failure. Diuretic resistance may be quickly assessed by a spot pattern for urinary sodium concentration one hour after a dose of intravenous loop diuretic. If the diuretic dose is already in extra of furosemide 80 mg (or its equal with other loop diuretics), different strategies together with mixture diuretic therapy (as mentioned in chapters eight and 9) or further intravenous therapy to enhance cardiac output and renal perfusion should be thought of. For patients with heart failure and reduced ejection fraction, imaging may detect an increase in the left-ventricular end-diastolic dimension from prior research, lower in the left-ventricular ejection fraction from prior research, and new or worsening mitral and tricuspid regurgitation. For sufferers with coronary heart failure with preserved ejection fraction, subtle changes in left-ventricular measurement and left-ventricular ejection fraction from the patient baseline may be current, although usually not outside of the conventional vary. Many of the signs and signs of superior coronary heart failure are associated to extreme reductions in cardiac output reserve. Right-heart catheterization may be thought-about to confirm the medical suspicion of decreased cardiac output, and in addition to instantly measure cardiac filling pressures (to rule out quantity depletion as a explanation for the worsening symptoms). Estimated cardiac outputs derived from the Fick formula are extra reliable than thermodilution cardiac output measurements in sufferers with advanced coronary heart failure. It is really helpful to get hold of an electrocardiogram and chest radiograph within the analysis of a affected person with worsening symptoms. Risk Stratification the extreme limitation in practical capacity is an important marker of poor consequence in this inhabitants. A peak oxygen consumption <14 ml/kg/min (or less than 50% of predicted) is related to poor outcome (<85% one-year survival). Other sites of care, including emergency departments, outpatient furosemide-infusion centers, medical houses, or hospices, could additionally be affordable options to think about in patients with superior heart failure. Optimization of quantity standing should be a precedence for all sufferers with advanced heart failure, with recognition that worsening azotemia and hypotension in response to diuretic remedy are fairly frequent in this group.
Uroxatral 10mg without prescriptionStrategies for extending remission duration in indolent B-cell lymphoma with out considerably growing toxicity are eagerly sought androgen hormone supplements uroxatral 10 mg without a prescription. A variety of investigators have evaluated totally different schedules of maintenance therapy in recent times (Table 70 define androgen hormone buy cheap uroxatral 10mg on line. Further investigations of rituximab maintenance prostate fusion biopsy cheap uroxatral 10 mg without a prescription, including its security and efficacy and optimal length of remedy and mixture with new agents mens health getting abs pdf buy uroxatral 10 mg cheap, are underway in potential randomized trials. These include a examine in first-line indolent lymphoma evaluating 2 versus four 12 months rituximab maintenance therapy (ClinicalTrials. Rituximab was properly tolerated with the incidence of late toxicity in patients evaluable beyond 1 year being solely 7% in both treatment arms [150]. Maintenance therapy was administered according to a schedule of 4 once-weekly doses at six-monthly intervals for a maximum of 4 programs or until illness progression. Rituximab therapy was nicely tolerated and rituximab maintenance was not associated with any grade 3/4 toxicity. No cumulative or late toxicity was observed and there have been no opportunistic infections [89, 152] (Table 70. Both therapy arms had been well tolerated and there were no treatment-related hospitalizations or patient discontinuations due to therapy-related adverse effects. In complete, 462 sufferers had been randomized to either watchful waiting (arm A, n = 186), weekly rituximab for 4 weeks (arm B, n = eighty four (this arm was discontinued early)), or weekly rituximab for four weeks followed by rituximab maintenance each 2 months for two years (arm C, n = 192). The estimated median time to initiation of recent remedy in the watchful waiting arm was 33 months and comparable with earlier research [91, 161]. The time to initiation of latest therapy was significantly longer in each rituximab arms versus watchful ready (p < zero. Longer follow-up knowledge are wanted to assess the position of rituximab upkeep therapy versus retreatment in this study (Table 70. The examine additional investigated whether or not rituximab maintenance remedy in responders would provide illness control superior to rituximab retreatment at progression. Two hundred and seventy-four patients that responded to induction remedy (weekly rituximab for 4 cycles) have been randomized to rituximab upkeep every three months (n = 140) or to retreatment with rituximab at progression (weekly rituximab for 4 cycles, n = 134). Updated results with a median follow-up time of more than four years had been reported in 2009 and confirmed the results reported in 2005 [156]. Neutropenia occurred more typically within the rituximab maintenance arm (11 vs 6% within the remark arm), which can have contributed to the increased grade 3/4 an infection rate of 9. The median response length after rituximab maintenance therapy was considerably longer than after remark only in 157 evaluable patients 70. Five hundred and five sufferers had been handled with rituximab upkeep given every 2 months for 2 years and compared with 513 sufferers in the observation arm. The profitable use of rituximab in patients with indolent B-cell lymphoma prompted its further evaluation in aggressive B-cell lymphoma. Rituximab has subsequently been evaluated with a quantity of completely different treatment regimens both in beforehand untreated (Table 70. The median age of survivors was seventy eight years with the oldest patient being ninety one years of age [186, 187]. It was recognized that the second randomization may have confounded interpretation of the impact of induction therapy and secondary (``weighted') analyses have been due to this fact carried out. No significant differences in survival were seen in accordance with induction or maintenance therapy. Rituximab upkeep remedy was additionally well 1952 70 Rituximab (RituxanΩ tolerated, though granulocytopenia was significantly greater in patients receiving maintenance rituximab compared with these being noticed (p = zero. The first interim evaluation of this trial occurred in November 2003 and included 326 evaluable patients. As this was considerably lower than the crucial threshold for alpha-spending for 97 occasions (0. The 6 12 months total survival price was higher when rituximab was added to chemotherapy (90. Adverse events were generally extra frequent after eight cycles of remedy than six cycles of therapy; the incidence of peripheral neuropathy was 14 and 8% after eight and 6 cycles, respectively. Further follow-up is required to elucidate the impact of this combination on long-term outcomes. Gemcitabine-based regimens have proven promise in B-cell lymphoma and the addition of rituximab to such regimens has been investigated. For such sufferers, rituximab monotherapy could also be an applicable treatment option several studies have demonstrated antitumor activity and a great tolerability profile (Table 70. The median age of the sufferers enrolled in the prospective study (59% ladies; 41% men) was 30 years (range, 19͵2). The two remaining sufferers obtained radiotherapy and have been disease-free at follow-up as well. Further studies are underway to outline the function of rituximab in these highly aggressive hematological malignancies. The Nordic Lymphoma Group identified 258 patients with Burkitt lymphoma in a retrospective examine. As anticipated, hematological toxicity was distinguished and neutropenic fever occurred after 15% of therapy programs, with three deaths due to neutropenic sepsis. There had been no main opposed results throughout rituximab maintenance therapy [235, 236]. Hematological toxicities and alopecia have been less frequent in the R-bendamustine arm [74]. Rituximab monotherapy can thus be thought-about an acceptable remedy for patients unsuitable for extra aggressive interventions. Infusion-related and hematological toxicity charges had been higher with concurrent than sequential therapy, but infectious toxicities Table 70. The investigators lately reported the impact of genetic prognostic elements on outcomes in trial patients for whom cryopreserved cells have been available [271]. Minor infections had been reported in 10% of treatment programs and main infections (including pneumonia and septicemia) in 2. Grade 3/4 neutropenia occurred in 57% of patients and 48% patients had grade 3/4 nonhematological toxicity (most generally nausea or vomiting). As within the first-line setting, myelosuppression was the most typical toxicity, with grade 3/4 neutropenia occurring in 62% of assessable treatment courses and main infections noted in 16% of handled sufferers [257]. However this routine was extremely myelosuppressive with almost all patients experiencing at least one episode of grade 3/4 neutropenia and infections occurring in 26% of sufferers. The routine was described as being properly tolerated with the principal toxicity being myelosuppression [258]. The major toxicity was myelosuppression (59% of all documented courses) and 22% of patients developed infections. There was a reduction in self-reported fatigue symptoms in two-thirds of the sufferers studied. The regimen was very properly tolerated, with grade 3/4 neutropenia and thrombocytopenia occurring in only 4 and 2% of patients, respectively. Lenalidomide was added to rituximab remedy on day 9 of cycle one at 10 mg orally and administered day by day continuously.
Uroxatral: 10 mg
Uroxatral 10 mg lowest priceThese studies can be conducted as stand-alone mens health cover discount 10 mg uroxatral amex, single- or repeat-dose animal studies androgen hormone meaning generic 10mg uroxatral mastercard. Blood samples are collected at prespecified time intervals for evaluation of the mAb focus in serum prostate 4k test cost 10mg uroxatral sale. When mAbs are administered intravenously prostate oncology key discount 10mg uroxatral amex, they usually display a biphasic elimination profile, consisting of a fast distribution section and a protracted elimination part in which antibody recycling and catabolism occur [62]. To help later part clinical trials and licensure of any potential therapeutic product, additional nonclinical research are performed that characterize dangers relating to chronic dosing, human fertility, reproduction, embryo-fetal improvement, and carcinogenicity. Because of inherent difficulties with conducting animal studies using mAbs, some or all of those research will not be feasible. The highest dose used ought to be the upper of those two options: (i) a dose that gives the maximum meant pharmacological impact within the given species; or (ii) a dose that provides an roughly 10-fold exposure multiple over the maximum exposure estimated to be achieved clinically [54]. These knowledge could embody results from in vitro organic assays utilizing human cells. Recovery (non-dosing) periods following the therapy section are used to look at reversibility of pharmacological and toxicological effects. This situation occurs when an excess of mAb is current and combines with the circulating goal, resulting in the deposition of anti-mAb:mAb complexes in the vasculature and subsequent activation of inflammatory pathways. Poorly designed assays most often impede product growth and will lead to post-marketing dedication research upon licensure. Specifically for mAb products, assays detecting anti-product antibodies are sophisticated by the fact that antibodies are normally the detection reagents, the product, and the goal of the assay. Thus, the presence of the product mAb in blood samples from the check animals can intrude with the result of the assay. Mire-Sluis and colleagues [67] present detailed recommendations for optimizing such immunoassays. The level of immunogenicity for any given product varies relying on the indication and concomitant medications. These include the patient inhabitants (immunosuppressed, autoimmune), intercurrent illnesses which will disrupt the distribution of the mAbs, the presence of preexisting antibodies (rheumatoid factor might react with some IgGs), concomitant medications (chemotherapy or immunosuppressive drugs), increases in the dose and/or frequency of administration, and the route of administration. The subcutaneous and intramuscular routes of administration are generally discovered to be more immunogenic than the intravenous route. Thus, the potential exists to choose mAbs with unusual structures that might be immunogenic or that cross-react with autoantigens. This may end up in product interference in the assays, as nicely as the potential interference of rheumatoid elements and nonspecific preexisting antibodies, for instance, anti-N-glycolylneuraminic acid [72, 73] and anti-IgG hinge regions [74]. There are additionally no information at this time addressing the potential immunogenicity of Fc-engineered mAbs that comprise particular mutations. Different IgG1 allotypes are used in licensed mAbs [75], however only a few studies have looked for and never detected anti-allotypic antibodies [76, 77]. Research continues with the goal of understanding illness pathways and figuring out novel targets for mAb remedy. Regulators depend on a versatile, case-by-case, science-based method to the security evaluation needed to help clinical growth and advertising authorization. While the regulatory pathway is complex, an early understanding of the regulatory course of and cautious product and preclinical characterization will improve the possibilities of success. Antibodies in infectious illnesses: polyclonals, monoclonals and area of interest biotechnology. Food and Drug Administration (1997) Points to Consider in the Manufacture and Testing of Monoclonal Antibody Products for Human Use. Food and Drug Administration (1998) Guidance for Industry Q5D Derivation and Characterization of Cell Substrates Used for the Production of Biotechnological/Biological Products. Food and Drug Administration (1995) Points to Consider within the Manufacture and Testing of Therapeutic Products for Human Use Derived From Transgenic Animals. Food and Drug Administration (2002) Guidance for Industry: Drugs, Biologics, and Medical Devices Derived from Bioengineered Plants for Use in Humans and Animals (Draft). Food and Drug Administration (2012) Guidance for Industry: Pyrogen and Endotoxins Testing: Questions and Answers. Food and Drug Administration (2008) Submission of high quality data for biotechnology merchandise in the office of biotechnology merchandise; discover of pilot program. In current years, the number of successfully authorized medicines have plateaued or are at best rising modestly, taking into account the disproportion of accelerating efforts and budgets spent in drug improvement [1]. Since its discovery in 1975, the product class of monoclonal antibodies (mAbs) has always been seen as a singular source of innovation because it may theoretically deliver an endless number of novel compounds for a limiteless number of therapeutic targets. Meanwhile, the know-how has matured permitting the design of hightech compounds corresponding to totally human antibodies, fusion proteins, fragments, bi-, tri-, oligo-specifics, polyclonals, antibodyΤrug conjugates, or synthetic antibodies. During 1996Ͳ005, most of the accredited mAbs have been developed in the same indications as certain therapeutic areas such as Rheumatoid Arthritis have been thought of highly profitable. When exploring the reasons for the hesitation to tackle novel targets, we discover that this is attributable to the growing difficulty in figuring out novel blockbusters due to the number and success of the existing medicinal merchandise. Other important elements are growth failures, specifically because of rejection by regulatory authorities, at the marketing authorization approval stage. These rejections are virtually completely caused by major gaps within the scientific knowledge package both by way of Handbook of Therapeutic Antibodies, Second Edition. Agencies dedicate a big proportion of their capability to the assist of scientific advice. Considering the deep shift the pharmaceutical business faces with the previously talked about lack of revolutionary compounds, you will want to understand what can be done to avoid failures within the selection of novel compounds for growth on one hand and within the strategic and scientific definition of scientific development programs and studies on the other. We will also explore the typical post-marketing activities surrounding mAb growth. These studies are large enough to acquire perception into product-specific safety indicators, a few of which may be important, and assist to additional strengthen the target product profile. General developments in clinical improvement of mAbs mirror these at present observed for novel chemical entities as the medical growth program is increasingly designed in a approach to set up early choice factors. Another way to make the scientific improvement extra efficient is to carry out the pre-pivotal trials using product derived from smaller scale batches quite than ready for a totally validated manufacturing process. This method adds further complexity to the development, as it requires a sequential comparability program in parallel to the clinical program. Because the efficiency assay and maybe a spectrum of legitimate practical assays reflect the various elements of the mode of motion and particular exercise of the mAb, these are so necessary for the efficiency of the comparability exercise. These assays need to be out there and validated in the early levels of development to confirm their performance and their suitability to demonstrate clinical exercise or surrogate medical exercise. This demonstrates that one of many unique features of the clinical development of a mAb is the want to continuously link the strategic issues of the medical pivotal study design, similar to initiation, period, total size, design, pattern measurement, inclusion standards, country selection, and so forth, to the manufacturing course of to be able to have a fully established course of at the time the pivotal trial begins. Development of a stable and particle-free formulation of a mAb and the identification of the first packaging of the drug product is challenging and time consuming. The choice on whether the pivotal trial is planned with a vial or prefilled-syringe requires totally different planning situations. Whether the modifications within the pharmaceutical type require a scientific study or not is a case-by-case problem. For the above causes, companies often resolve to tighten the label to a more limited or even area of interest indication. A very important factor for the acceleration of mAb improvement is thus the involvement of experts with regulatory expertise in the medical target indication of the mAb beneath improvement.
Order 10mg uroxatral fast deliveryFor many of these sufferers or other patients requiring excessive present outputs prostate 7 price uroxatral 10 mg, the transcutaneously rechargeable Medtronic system (which recharges through a radiofrequency field) is chosen to avoid frequent battery replacements androgen hormone x organic uroxatral 10mg on-line. The impedance at typical operating frequencies for individual electrode contacts can vary from 600 to 1800 ohms man health women news p90x results buy uroxatral 10mg overnight delivery. In addition to the three main adjustable parameters for the cost balanced pulses (pulse width man health 3rd buy 10 mg uroxatral overnight delivery, software frequency, and the applied voltage) the identification of the contacts used to transmit the pulses (either between two of the quadripolar-lead contacts-referred to as bipolar stimulation, or between one contact and the heartbeat generator case-referred to as monopolar stimulation) can also be varied permitting the programmer to alter the form of the electrical area surrounding the distal end of the device. Monopolar stimulation sometimes leads to larger unfold of the activation present, whereas bipolar stimulation results in a tighter current profile. Initial programming is probably best done with the patient skipping the morning dose of medication. Subsequent programming then includes an evaluation of each contact because the voltage is stepwise elevated to seek the brink of either scientific efficacy or unwanted aspect effects (Volkmann et al. It could additionally be possible to improve the applied stimulation voltage range as time increases after implantation because of fading unwanted effects. These unwanted effects could include voice alterations, paresthesias, dyskinesias, and, often, mood alterations (Krack et al. Because of this, many facilities modify the initial stimulation depth to 1015% under the level at which nontransient unwanted facet effects occur. The depth can then be decreased at interval visits till the dystonic signs recur providing the clinician with a useful vary of stimulation intensities (Kupsch et al. The neural elements which have the bottom response threshold to externally applied electrical fields are myelinated axons and axon initial segments (McIntyre et al. Human brain tissue has variable electrical characteristics and represents a medium with nonisotropic electrical conductivity. The efferent axonal buildings of the goal neurons, nonetheless, are excited at the identical time and may be unaffected by these upstream inhibitory synaptic effects. This might result in overall increased output from the goal structure due to the activation of efferent axons and could also end in "stimulation-induced modulation of pathological network exercise" (McIntyre et al. In a study utilizing blinded evaluations of 18 patients at 10-year follow-up (out of an unique 46 patient cohort during which eleven were misplaced to follow-up and 12 have been deceased) it was noted that this decrease in improvement with stimulation grew to become more evident after 5 years. More prominently, there was continued deterioration in axial indicators together with speech, posture, gait, and postural stability at 10 years. The lead is inserted via burr holes positioned just anterior to the coronal suture whereas the affected person is awake to assess desired and potential opposed stimulation effects. Microelectrode recording is used before the actual lead placement to better refine the goal and the medical efficacy and unwanted effects of the stimulation. There are a number of business stereotactic frames and even frameless stereotactic systems obtainable for this process. The lateral plane of the goal in Vim may be estimated as mendacity between the inner capsule and the T2 intense medial dorsal nucleus of the thalamus (Burchiel 1995). In our establishment, a map is made to the same scale as a set of transparent atlas maps from the sagittal sections of the Schaltenbrand and Bailey atlas (Schaltenbrand and Walker 1982; Schaltenbrand and Bailey 1959). Direct concentrating on may be carried out with atlas maps of the neuroanatomy overlaid onto the imaging slice. Operative Procedure the affected person is taken to the working room and positioned on a regular adjustable operative table in a seated however reclined place with the stereotactic body rigidly connected to the operative table utilizing a Mayfield adaptor. A warm blanket wrap and foam bolsters are positioned behind the neck and upper back to provide some aid from cervical muscle pressure through the operation. Blood stress is monitored with a cuff with a aim of systolic blood stress at or below one hundred forty mm Hg. Once the affected person is positioned and cozy, the scalp is clipper shaved, and prepped and draped appropriately for the bilateral pores and skin incisions. The middle of the posterior border of the anterior commissure and the center of the anterior border of the posterior commissure are used for atlas-based empirical focusing on strategies (Schaltenbrand and Bailey 1959). The software reformats the images so that a single axial aircraft incorporates the intercommissural line. An entry level is then selected in the center of a gyrus, if potential, to avoid vascular constructions. Ventricular crossings are also averted when planning due to the risk of damaging ependymal veins and causing intraventricular hemorrhage. In the working room, a sterile clear plastic drape is positioned over the prepped scalp and base body and secured to the arm of the fluoroscope. Light intravenous sedation may be used to lower patient anxiety because the burr gap is created, but many patients tolerate the process with out sedation. Two parallel pores and skin incisions are made just in front of and straddling the coronal suture bilaterally. The pericranium is swept apart with a periosteal elevator, and a small self-retaining retractor is positioned to hold the scalp open. The calculated X, Y, and Z coordinates are then set on the body system along with the arc and ring angle, to enable for exact cranium placement of the burr holes. Self-locking plastic lead fixation rings are then hooked up to the outer surface of the burr holes. The dura is opened in cruciate style and concurrently coagulated to assist with retraction. If discovered, large cortical veins can usually be gently moved aside; smaller veins could be coagulated. Microelectrode recordings then start from this depth and continue to 45 mm beneath the target area. Physiologic testing can be performed during these recordings to look for kinesthetic cellular responses or cutaneous sensory responses (see below). Commercial microelectrode recording techniques also permit for stimulation through contacts near the microelectrode tip, to seek stimulation-induced results on tremor or tone, and to test for stimulation-induced unwanted facet effects. Further testing of the inserted lead is then typically carried out with a battery-powered hand-held check stimulator, to again search for unwanted effects and scientific efficacy. The lead-locking system previously positioned in the burr gap is then clipped shut and capped to maintain the lead in place. Neuronal responses to passive and active movements, as well as spontaneous activity of multiunit spike trains, are examined. High impedance microelectrodes for physiologic monitoring and recording are designed to isolate single neuron motion potentials (Lenz et al. This process is often carried out under general anesthesia due to the painful subcutaneous tunneling involved. The distal lead cabling is first uncovered at the scalp site after which tunneled beneath the skin to the periauricular incision. Extension lead cables are then tunneled from the subclavicular incision to the periauricular incision. The connection fixture is sutured to the underlying fascia and periosteum to inhibit migration. Redundant extension lead cabling is placed to the sides and behind the heartbeat generator, but not on high of the gadget. The medical therapy of many of these disorders is kind of restricted and may become ineffective over years (Jankovic et al. Advances in our understanding of the anatomy and physiology of subcortical nuclei and their involvement in movement issues is increasing rapidly and has assisted in guiding therapeutic target selection.
Uroxatral 10 mg saleSpironolactone and eplerenone are thus mineralocorticoid receptor blockers more than merely aldosterone receptor blockers mens health zinc generic uroxatral 10mg with visa. This notion probably led to some initial lack of curiosity in aldosterone receptor inhibitors for the treatment of systolic heart failure man health 6 health purchase 10 mg uroxatral with visa. There was a 30% reduction in mortality in sufferers randomized to spironolactone in comparability with mens health 8 hour diet buy 10 mg uroxatral fast delivery sufferers within the placebo group man health magazine desktop test buy uroxatral 10 mg low price. Spironolactone62 and eplerenone63 are now widely used to treat continual systolic coronary heart failure and postmyocardial infarction heart failure. Careful follow-up of sufferers and frequent measurement of renal operate and serum potassium are essential to ensure security when using aldosterone receptor blocking drugs. The notion is that regulation of salt and water retention is adaptive, maybe by protecting intravascular volume, blood strain and perfusion to vital organs. Blockade of aldosterone membrane receptors is a widely accepted form of therapy for systolic coronary heart failure. Postmyocardial infarction heart failure can be improved by mineralocorticoid receptor blockers. Spironolactone and Eplerenone in Chronic Heart Failure the mechanism of action of spironolactone is complicated, as aldosterone mineralocorticoid modulates many features of the heart failure syndrome. Spironolactone is an old drug that was primarily used in giant doses to treat ascites, edema and refractory hypertension. Excessive mineralocorticoid, widespread in sufferers with heart failure, promotes sodium retention, lack of magnesium and potassium, sympathetic nervous system activation, parasympathetic nervous system inhibition, myocardial and vascular fibrosis, baroreceptor dysfunction, and impaired arterial compliance. Death from progressive heart failure and sudden demise had been each reduced by spironolactone. Today, aldosterone mineralocorticoid antagonists are broadly used to deal with advanced coronary heart failure and selected patients with acute myocardial infarction. However, less than one-third of eligible sufferers hospitalized for coronary heart failure are receiving guidelinerecommended aldosterone receptor blocking drugs. Nevertheless, aldosterone receptor blockers are efficient and safe when properly prescribed and monitored, and their indications are seemingly expanding. Visual disturbances and priapism have additionally been noticed with this class of drugs. A small case series (3 patients) has recently implied that a mix of sildenafil and nitrates can be utilized in sufferers with heart failure and pulmonary hypertension,77 though clearly extra sturdy clinical trials are wanted. Nevertheless, medicine similar to sildenafil and tadalafil that selectively restore right ventricular contractility, limit right ventricular hypertrophy and reduce pulmonary artery transforming are intriguing as potential therapy for proper coronary heart failure due to disproportionately increased pulmonary artery stress. More studies are needed, and use of those drugs for the therapy of heart failure remains investigational for now. The drug is usually began as doses of 10 µg/min, and steadily titrated as much as no more than 400 µg/min, as wanted to control hemodynamic abnormalities and symptoms. Some clinicians give nitroprusside based on body weight, with the typical dose starting at 1020 µg/kg/min. Our in depth expertise with nitroprusside suggests that with low dose infusion charges (<3 µg/kg/min) used for lower than 72 hours, toxicity is almost by no means noticed. Invasive monitoring with a pulmonary artery catheter and an arterial catheter can be useful if the patient has marginal blood strain. Persistent 26 CardiaC medication or severe hypotension will nearly always dissipate as quickly as nitroprusside is stopped. Thiocyanate toxicity can hardly ever happen, and thiocyanate ranges must be monitored, notably if the affected person has received a high dose for a chronic time period. Measurement of thiocyanate is a straightforward, inexpensive colorimetric take a look at, normal levels being lower than 10 mg/mL. Metabolic acidosis, anuria, and a protracted high dose of nitroprusside (>400 µg/min) can predispose to thiocyanate toxicity, prompting measurement of thiocyanate levels. When thiocyanate toxicity does happen, the patient might present with confusion, hyperreflexia and convulsions. Nevertheless, nitroprusside has been used successfully in this setting when given in the subacute part. Patients with extreme mitral regurgitations or aortic regurgitation may show dramatic scientific improvement with nitroprusside. It can be used to stabilize acute coronary heart failure in patients who reveal a ruptured interventricular septum following acute myocardial infarction. Recent observational information indicate that in patients hospitalized with advanced, low-output heart failure, these Vasodilators and Neurohormone Modulators 27 stabilized in the hospital with nitroprusside might have a more favorable long-term scientific outcome. The infusion rate is usually initiated at 1020 µg/min with gradual titration to 200400 µg/min as needed to control signs and enhance hemodynamic parameters. Intravenous nitroglycerin is endothelium dependent, and unlike nitroprusside, it has extra effect on the venous circulation than on the arterial circulation. However, higher doses of intravenous nitroglycerin have arteriolar dilating properties and should decrease afterload. There are few information out there on the results of intravenous nitroglycerin on coronary circulation in sufferers with coronary heart failure. This suggests that each the epicardial conductance vessels and the coronary arteriolar resistance vessels are favorably influenced by intravenous nitroglycerin. Limitations of Intravenous Nitroglycerin in the Treatment of Patients with Heart Failure Intravenous nitroglycerin causes headaches in about 20% of sufferers, and when extreme, may require cessation of the infusion. Some patients are relatively immune to intravenous nitroglycerin and seemingly require very large doses to afford a hemodynamic effect. When infused intravenously into the 28 CardiaC medicine circulation of sufferers with heart failure, the mean terminal elimination half-life of nesiritide is about 18 minutes. The effects of nesiritide on renal perform are variable, but typically only a modest or impartial renal impact is noticed, although worsening renal perform has been reported. Therefore, the usage of nesiritide for sufferers with acute decompensated heart failure has additional waned over the years, while cheaper intravenous vasodilators continue to be employed. However, an excessively lively sympathetic nervous system has repeatedly been shown to be basically toxic to myocardial cells in both animals and people. The significance of dysfunctional adrenergic activation in heart failure was first elucidated by work of Braunwald and colleagues at the National Institutes of Health within the Nineteen Sixties. Such organic conduct means that blocking the receptors pharmacologically may defend the guts. The first use of b-adrenergic blockers to treat sufferers with coronary heart failure was the product of a series of rigorously written case stories from Gцteborg, Sweden. Today b-adrenergic blockers are widely used all through the world to deal with patients with systolic heart failure. The continuation of b-blocker remedy in patients hospitalized with acute decompensated systolic coronary heart failure is related to decrease post-discharge mortality risk and improved remedy rates. One possibility is that practical enchancment from b-blockers could additionally be related to adjustments in myocardial contractile protein gene expression,126 which may differ from patient to patient.
Rewandchini (Rhubarb). Uroxatral. - Are there any interactions with medications?
- What is Rhubarb?
- What other names is Rhubarb known by?
- How does Rhubarb work?
- Are there safety concerns?
- Cold sores, in combination with sage (Salvia officinalis).
- Indigestion, stomach inflammation, hemorrhoids, constipation, diarrhea, or bleeding from the stomach and colon (bowels), and other conditions.
- Dosing considerations for Rhubarb.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96247
Discount uroxatral 10 mg onlineCases diagnosed as "Gleason grade four" could be thought of as both Gleason rating 2 2 four or Gleason score 4 four 8 prostate psa uroxatral 10mg otc. The glands are uniform in their measurement and form with barely more variation in pattern 2 than pattern 1 prostate cancer update buy uroxatral 10 mg lowest price. Consequently prostate cancer screening guidelines 10mg uroxatral free shipping, a lot of the lesions that appear to be very low-grade on needle biopsies are identified by urologic pathologists as Gleason score 3 2 5 or three three 6 prostate kidney stones buy 10 mg uroxatral with mastercard. Studies have proven a dramatic lower within the incidence of diagnosing Gleason rating 2 to four on needle biopsy over the last decade. In one research, 24% of pathologists rendered a analysis of Gleason score of two to four on biopsy in 1991, which decreased to 2. Typically, both Gleason sample 1 and Gleason pattern 2 carcinomas have ample pale eosinophilic cytoplasm. The presence of a few poorly formed glands at high power, which might symbolize a tangential part off of small well-formed glands, remains to be according to Gleason sample three tumor. Gleason pattern 3 glands are both (a) infiltrative between benign glands, (b) extra variably sized, or (c) smaller than Gleason patterns 1 and a pair of. Some pathologists might not really feel snug assigning both a primary and secondary sample three to very small foci of carcinoma on biopsy. A main point of divergence from the unique Gleason system is with project of grade to cribriform glands. The consensus conference proposed extremely stringent standards for cribriform Gleason pattern three. However, Gleason by no means particularly revealed the prognostic distinction between what he known as cribriform Gleason sample 3 compared to cribriform Gleason sample 4. Probably, the commonest state of affairs the place Gleason pattern 3 is overgraded as Gleason sample 4 is when a couple of tangentially sectioned small glands of sample three are present and seen at larger magnification. Glands that artifactually appear poorly formed because of crush artifact should be distinguished from Gleason sample 4. Similarly, the delicate ingrowth of fibrous tissue seen with mucinous fibroplasia (collagenous micronodules) can lead to glands appearing to be fused resembling cribriform buildings, though the underlying structure is really that of individual discrete rounded glands invested by free collagen. In addition, the consensus conference reported that ill-defined glands with poorly shaped glandular lumina also warrant the diagnosis of Gleason pattern 4. Cribriform glands in a single research had been related to the next threat of postradical prostatectomy failure as in comparability with fused glands. There are some difficulties in distinguishing higher developed cribriform glands of sample 4 from poorly fashioned cribriform glands with barely identifiable acini which might be finest characterized as pattern 5 (see Gleason pattern 5 in the following discussion). They are characterised by dilated glands containing intraluminal cribriform constructions with a single point of attachment, resembling a renal glomerulus. On prostate biopsy, glomeruloid glands are completely associated with carcinoma and not related to benign mimickers. A examine from Hopkins subsequent to the consensus conference indicated that glomerulations have been overwhelmingly related to concurrent Gleason sample 4 or greater grade carcinoma. These information recommend that glomerulations represent an early stage of cribriform pattern four cancer and are finest graded as Gleason sample four. In addition to cribriform glands, the other major morphologies of Gleason sample 4 are poorly formed and fused glands. In other circumstances, ill-defined glands with poorly formed glandular lumina are accompanied by fused glands. There is a tendency for basic pathologists to underdiagnose Gleason sample 5 on needle biopsy. Of the various morphologies of Gleason pattern 5, the one state of affairs the place it was extra routinely recognized was with stable sheets as the primary pattern. Most circumstances of Gleason score 9 and 10 are pretty intensive on needle biopsy, though uncommonly, only a small focus of such high-grade cancer is current on biopsy. Although the majority of cases with Gleason sample 5 are both Gleason rating 9 or 10, some circumstances are Gleason score three 5 eight or 5 3 eight. One must be stringent as to the definition of comedonecrosis, requiring intraluminal necrotic cells and/or karyorrhexis, particularly within the setting of cribriform glands. Other less widespread morphologies seen with Gleason pattern 5 are small nests and cords of cells. The nested progress could additionally be confused with urothelial carcinoma, whereas cords are patterns not seen in urothelial carcinoma. Foamy Gland Carcinoma One ought to ignore the foamy cytoplasm and grade the tumor solely based mostly on the underlying architecture. An uncommon variant of foamy gland consists of broadly separated foamy glands associated with a very outstanding desmoplastic stroma. These tumors are most likely to be extensive, aggressive cancers and sometimes are excessive grade regardless of the relative paucity of malignant glands. In the uncommon case where a few of the glands with pseudohyperplastic features have cribriform morphology, a Gleason pattern 4 ought to be assigned. Assume a case with Gleason rating four 4 eight on one core with pattern 3 (3 three 6, three four 7, or 4 3 7) on other cores. The "world" score for the complete case, averaging all concerned needle biopsies collectively as in the event that they had been one lengthy constructive core, could be four three 7 or 3 4 7, relying on whether or not sample four or 3 predominated. Several studies have demonstrated that in instances with totally different cores having completely different grades, the very best Gleason rating on a given core correlates better with stage and Gleason score at radical prostatectomy than the common or most frequent grade among the many cores. Whether the highest grade per core or the general rating is used impacts a big number of cases. As a consequence, the core with the best grade tumor may be selected by the clinician as the grade of the entire case to decide treatment. In the setting of multiple undesignated cores with cancer per container, some urologic pathologists still grade each core separately with the remaining experts in the field giving an general grade for the specimen container. On the other hand, assigning a Gleason score to each core even when there are multiple constructive cores in a given jar offers essentially the most accurate info for patient care. For example, diagnosing Gleason rating four four eight on a tiny tissue fragment where there are other fragments with a higher amount of Gleason pattern 3 could possibly be in error; if the cores had been intact and the tumor was all on one core, it might be assigned a Gleason rating three 4 7. Tertiary Gleason Patterns On needle biopsies with patterns three, four, and 5, both the primary pattern and the highest grade ought to be recorded, which is a departure from the original Gleason grading system. Reporting Secondary Patterns of Lower Grade When Present to a Limited Extent In all specimens, in the setting of high-grade cancer, one ought to ignore decrease grade patterns in the event that they occupy less than 5% of the realm of the tumor. For example, tumor composed of 98% Gleason sample 4 and 2% Gleason pattern 3 must be graded as Gleason score four four 8. In the setting of very limited cancer on needle biopsy, the few glands of pattern three usually occupy over 5% of the world of the tumor focus, resulting in a Gleason rating 4 3 7. Within the literature, upgrading from Gleason rating 6 on needle biopsy to radical prostatectomy was seen in 4,614 out of 13,163 (35%) of the cases, just about the same as with our own experience. Explanations for Grading Discrepancies One supply of grading discrepancy between needle and radical prostatectomy grade is that the variations between different Gleason patterns are on a continuum. For example, it can be subjective whether or not there are small glands of sample 3 or poorly fashioned glands of pattern four. Similarly, it may be a judgment name whether there are very poorly shaped glands of pattern 4 as opposed to sample 5 with barely considerable glandular differentiation.
Buy 10 mg uroxatral overnight deliveryIn three studies prostate young living purchase uroxatral 10mg without a prescription, circumstances signed out as atypical by common pathologists had been identified as benign in 5% to 17% of cases prostate jewelry buy 10 mg uroxatral fast delivery, and as carcinoma in 2% to 20% of circumstances when reviewed by a genitourinary pathologist prostate cancer 5 year survival rate uk uroxatral 10 mg free shipping. Of the 204 circumstances signed out as atypical by the skin pathologist prostate growth purchase uroxatral 10mg with visa, 45% had been definitively recognized as cancer upon professional evaluate with 16% identified as benign. Only three studies report the median time to rebiopsy with a median of approximately 9 months. Approximately 90% of cancers shall be found on the preliminary repeat biopsy after an atypical analysis. We have seen such instances where upon review of the initial biopsy, it was diagnostic of most cancers. If the pathologist is sufficiently worried with the preliminary biopsy to subject the affected person to a surgical process. It remains to be studied whether or not and what quantity of occasions these men want extra tissue sampling. It is subsequently logical that in order to maximize the detection of cancer following an atypical diagnosis, one would need to concentrate the repeat biopsy sampling in the space of the atypical focus. Five research have reported that following an atypical prognosis, the likelihood of most cancers being current in similar sextant web site as the preliminary atypical focus is 48% to 76%. It is critical for urologists to submit needle biopsy specimens in a manner where the sextant location of each core could be decided so that pathologists can specify the sextant site containing the atypical focus. Case was despatched in for consultation, whereby we diagnosed the focus as benign despite the immunohistochemical stains. There are only a few glands on the edge of the core they usually lack prominent cytologic atypia, insufficient to definitively diagnose carcinoma. When certain features more typical of most cancers, corresponding to blue-tinged or dense pink mucinous secretions, are present but the atypical findings are minimal, a analysis of atypical glands suspicious for most cancers is rendered. Furthermore, the diploma of cytologic atypia current in the small atypical glands is significantly greater than the adjoining benign glands although both are uncovered to the same inflammatory milieu. Even if the glands are unfavorable for basal cell markers in a small focus, the lesion might nonetheless be adenosis because basal cell stains may be very patchy in adenosis. Although not often carcinomas may be inflamed, inflammation tends to preferentially localize away from malignant glands. In areas of intense chronic inflammation, prostatic acini seem atrophic with a high nuclear to cytoplasmic ratio. Streaming of basophilic epithelium in areas of intense persistent inflammation resembles transitional cell metaplasia. The distinction of those inflammatory atypias from carcinoma first relies on the popularity that the atypical glands are situated in an area of intense inflammation. The excessive nuclear to cytoplasmic ratio seen in infected glands is predominantly seen in only the extra poorly differentiated prostatic carcinomas that lack good gland formation. Careful examination of these basophilic glands may also show the discovering of a basal cell layer in most cases. Another situation the place benign glands are recognized as atypical is when their basal cells contain prominent nucleoli. Diffuse adenosis of the peripheral zone is a diagnostically challenging mimicker of prostate most cancers seen in prostate needle biopsies from typically youthful sufferers. It is a threat factor for prostate cancer and patients with this discovering should be followed intently and rebiopsied. Atypical small acinar proliferation suspicious for malignancy in prostate needle biopsies: clinical significance in 33 cases. What info are urologists extracting from prostate needle biopsy stories and what do they need for medical administration of prostate cancer? Prostate cancer detection in males with prior high grade prostatic intraepithelial neoplasia or atypical prostate biopsy. The focus of "atypical glands, suspicious for malignancy" in prostatic needle biopsy specimens: incidence, histologic options, and clinical follow-up of cases diagnosed in a neighborhood follow. Practice patterns of clinicians following isolated diagnoses of atypical small acinar proliferation on prostate biopsy specimens. Prostate cancer diagnosed after preliminary biopsy with atypical small acinar proliferation suspicious for malignancy is similar to cancer discovered on preliminary biopsy. Clinicopathological characteristics of prostatic adenocarcinoma in men with atypical prostate needle biopsies. Current apply of analysis and reporting of prostate most cancers on needle biopsy among genitourinary pathologists. Significance of atypical and suspicious small acinar proliferations, and excessive grade prostatic intraepithelial neoplasia on prostate biopsy: implications for most cancers detection and biopsy technique. Is there any scientific parameter in a position to predict prostate cancer after initial analysis of atypical small acinar proliferation? Prostate adenocarcinoma detected after high-grade prostatic intraepithelial neoplasia or atypical small acinar proliferation. Lesions predictive for prostate cancer in a screened population: first and second screening round findings. Repeat biopsy strategy in sufferers with atypical small acinar proliferation or high grade prostatic intraepithelial neoplasia on preliminary prostate needle biopsy. Prognostic significance of high grade prostatic intraepithelial neoplasia and atypical small acinar proliferation within the contemporary period. Clinicopathological features of prostate cancers detected after an preliminary prognosis of "atypical glands suspicious for cancer. Initial atypical diagnosis with carcinoma on subsequent prostate needle biopsy: findings at radical prostatectomy. Diffuse adenosis of the peripheral zone in prostate needle biopsy and prostatectomy specimens. High-grade prostatic intraepithelial neoplasia with adjacent atypia is associated with a better incidence of cancer on subsequent needle biopsy than high-grade prostatic intraepithelial neoplasia alone. High-grade prostatic intraepithelial neoplasia with adjacent small atypical glands on prostate biopsy. When prostatic duct adenocarcinomas arise in massive major periurethral prostatic ducts, they might grow as exophytic lesions into the urethra, mostly in and around the verumontanum. Tumors arising within the extra peripheral prostatic ducts may or could not have a urethral component and could additionally be palpable on rectal examination. They are characterized by tall pseudostratified epithelial cells with plentiful, usually amphophilic cytoplasm, in contrast to the cuboidal to columnar single cell layer of epithelium seen with acinar prostatic carcinomas. Uncommonly, benign glands can show papillary hyperplasia, which is distinguished from ductal adenocarcinoma by the presence of bland cuboidal epithelium. The cribriform sample of prostatic duct adenocarcinomas is more commonly seen deeper throughout the tissue, though it may also be famous (text continues on p. The cribriform sample is fashioned by back-to-back giant glands with intraglandular epithelial bridging ensuing within the formation of slit-like lumens.
Best 10 mg uroxatralAs many as 40% of splenectomies are carried out on account of iatrogenic splenic injury prostate cancer quiz uroxatral 10mg line. The standard use of laparoscopic procedures may decrease the danger of splenic injury by providing higher visualisation mens health july 2012 uroxatral 10 mg online, software of less traction prostate reduction discount uroxatral 10 mg, improved instrumentation for perisplenic dissection prostate 600 buy 10 mg uroxatral fast delivery, and better control of capsular haemorrhage by the stress of the pneumoperitoneum. Haemostatic brokers similar to microfibrillar collagen, microporous polysaccharide hemispheres or injectable haemostatic matrices may be utilized to aid haemostasis. Ligation of chosen arteries within the hilum may assist control bleeding however probably result in a necessity for partial splenectomy. Splenorrhaphy and partial splenectomy have been described for splenic trauma; nevertheless, Holubar et al. If platelet 166 the spleen counts drop after splenectomy, peripheral blood smears may show absence of nuclear inclusions. Mild to reasonable levels of thrombocytopenia without signs of purpura or bleeding postsplenectomy could also be observed with out resuming medical therapy. Many delicate cases require no therapy; nonetheless, if greater than 90% of cells are affected anaemia, is substantive, and splenectomy must be thought-about. Thallassaemias Genetic abnormalities leading to abnormal haemoglobin construction, similar to thalassaemias, might require splenectomy. Defective alpha chains and beta chains within the haemoglobin tetramer result in alpha thalassaemia and beta thalassaemia, respectively. The alpha chains precipitate within the absence of the beta chains and create the more extreme beta thalassaemia. Blood transfusions and chelation remedy are the mainstays of therapy; nonetheless, stem cell transplantation is taking part in a greater function within the administration of this disease. Thalassaemia sufferers are at increased risk of infective issues postoperatively. Evans syndrome Evans syndrome is characterised by autoimmune haemolytic anaemia and autoimmune thrombocytopenia. Splenectomy may be healing in as a lot as 40% of patients and enhance the state of affairs in as a lot as 60%; nevertheless, failures are frequent. The illness is characterised by extravascular destruction of purple cells, notably in the spleen. Major indications for splenectomy are recurrent acute splenic sequestration disaster, hypersplenism, splenic abscess and big splenic infarction. Guidelines from the General Haematology Task Force of the British Committee for Standards in Haematology state that patients with extreme illness presenting in childhood require splenectomy. Otherwise, sufferers should be chosen for splenectomy based on scientific signs and related complications similar to gallstones. Cholecystectomy ought to be performed if gallstones are current at the time of splenectomy. Failure of medical remedy or need for highdose steroids should prompt consideration of splenectomy. Several teams have reported the usage of subtotal splenectomy for the remedy of hereditary spherocytosis and demonstrated amelioration of anaemia and maintenance of immune operate. Mild to average haemolysis, however, may persist and gallstone formation and aplastic crises still developed in some patients. Similarly, systemic therapy has replaced splenectomy as the first remedy of furry cell leukaemia, reserving splenectomy for refractory disease. This could result in symptomatic splenomegaly, thrombocytopenia, hypercatabolic state with resultant excessive output coronary heart failure, and forward circulate portal hypertension. Mortality charges are high as a outcome of severe bleeding complications, coronary heart failure and superior stage of underlying illness at the time of splenectomy. Parasitic cysts are usually echinococcal in origin and the analysis is usually confirmed by serological research. Splenic conserving techniques may be appropriate for early disease or disease situated at the perimeter of the spleen. Portal hypertension Sinistral (left-sided) portal hypertension secondary to splenic vein thrombosis might result in bleeding gastric varices. This is a state of affairs the place preoperative splenic artery embolisation should be considered to lower venous pressure in the splenic collaterals, thereby rising the protection of surgery. Embolisation may be carried out underneath the identical anaesthesia because the splenectomy, since splenic embolisation is extremely painful to the patient. Patients present with severe belly ache and a proper lower quadrant mass, sometimes occurring intermittently. A viable spleen must be returned to the left higher quadrant and glued in place using a mesh sac tacked to the diaphragm. Preparation for splenectomy Preoperative preparation for splenectomy, as for different procedures, is designed to prevent or minimise problems. Splenectomy carries the similar old danger of other abdominal operations and, relying on the disease, increased dangers similar to bleeding, coagulopathies including disseminated intravascular coagulation, an infection (both quick and delayed) and altered cardiovascular efficiency. Efforts ought to be made to right all coagulopathies and optimise blood counts preoperatively if possible. If platelets are to be given in damaging or consumptive states, transfusion ought to be withheld if potential till the splenic artery is ligated to prevent the fast breakdown of the transfused platelets. Patients with large splenomegaly secondary to major myelofibrosis might have hypertrophied cardiac dysfunction, pulmonary hypertension, ascites and pleural effusions. Appropriate preoperative antibiotics should be given to scale back the chance of an infection, particularly in immunocompromised states. Cysts Cystic lesions of the spleen are sometimes categorised as parasitic or non-parasitic. Cysts larger than 5 cm in diameter are at potentially greater risk of rupture, so intervention could also be indicated both by laparoscopic deroofing or resection. Percutaneous drainage and alcohol ablation have additionally been used with unreliable results. Our choice is for an higher midline approach, which can be prolonged within the case of huge splenomegaly. Once packs are removed sequentially and bleeding controlled, the spleen is mobilised from its lateral attachments. Haemostasis is ensured, particularly by inspecting the ligated quick gastric vessels. Alternatively, early entrance to the lesser sac and ligation of the splenic hilum facilitates platelet transfusions as necessary, in addition to management of bleeding because the spleen is additional mobilised. Hilar vessels are divided between clamps and ligated or divided with a linear stapler when appropropriate. Accessory spleens must be sought and removed if surgical procedure is designed to right a damaging or sequestration state.
References - Small TN, Leung L, Stiles J, et al. Disseminated toxoplasmosis following T cell-depleted related and unrelated bone marrow transplantation. Bone Marrow Transplant. 2000;25(9):969-973.
- Royse CF, Royse AG, Soeding PF: Routine immediate extubation after cardiac operation: A review of our first 100 patients, Ann Thorac Surg 68:1326, 1999.
- Machold KP, Smolen JS. Early (rheumatoid) arthritis. In: Hochberg MC, et al., eds., Rheumatoid Arthritis, 1st edition. Philadelphia: Mosby 2009:73-81.
- Greco R, Tassorelli C, Sandrini G, et al: Role of calcitonin gene-related peptide and substance P in different models of pain, Cephalalgia 28:114n126, 2008.
|